
Abstract
Objective
Pressure injuries (PIs) are common complications among orthopedic patients. This study aimed to compare the effectiveness of aloe vera gel, rosemary oil, and their combination with a control intervention in preventing PIs.
Methods
A triple-blind randomized four arm parallel clinical trial was conducted among 160 orthopedic patients assigned to four groups: aloe vera–rosemary combination, rosemary oil, aloe vera gel, or control (n=40 each). The assigned spray was applied twice daily for 10 days to pressure-prone areas. Outcomes included PI incidence, skin temperature, and pain intensity.
Results
The aloe vera–rosemary group demonstrated the lowest incidence of sacral, hip, heel, and total PIs compared with the other groups (p = 0.02, 0.03, 0.03, and 0.009, respectively). Significant reductions in pain intensity were also observed across pressure-prone areas over time (all p < 0.001). Additionally, skin temperature decreased significantly in the intervention groups compared with the control group during follow-up (all p < 0.05).
Conclusion
The rosemary oil and aloe vera-rosemary oil combination showed positive effectiveness in preventing PIs; it is recommended for use in the prevention of PIs among orthopedic patients.
Introduction
Pressure injuries (PIs) remain a major global healthcare problem and a key nursing concern. They are defined as localized damage to the skin or underlying tissue over bony prominences, resulting from pressure or shear (Anker-Hansen et al., 2024; Hammad et al., 2025). Despite being largely preventable, PIs are among the leading causes of patient harm worldwide and are associated with increased morbidity, prolonged hospital stay, and higher healthcare costs (Li et al., 2020; Miraj et al., 2020).
In orthopedic wards, 8.4–34.2% of patients face higher PIs risk ((Kathirvel et al., 2021), due to prolonged immobility, surgical positioning, and reduced tissue perfusion (Jiao et al., 2022; Suh et al., 2021). Sustained pressure during and after surgery reduces soft tissue circulation, contributing to ischemia and tissue damage (Mervis & Phillips, 2019; Yap et al., 2021). As a result, PIs commonly occur in areas such as the sacrum, hips, and heels.
Although standard preventive measures such as repositioning, pressure-relieving devices, and skin care are widely implemented, the incidence of PIs remains considerable (Tervo-Heikkinen et al., 2022). Therefore, there is increasing interest in complementary, low-cost interventions, including herbal topical agents.
Aloe vera and rosemary oil have demonstrated anti-inflammatory, analgesic, and wound-healing properties (de Macedo et al., 2020; Safdari et al., 2021). However, evidence regarding their effectiveness in PI prevention remains limited and inconsistent (Fallahi et al., 2022; Hekmatpou et al., 2018), and no clinical trials have evaluated their combined use in orthopedic patients.
Therefore, this study aimed to evaluate the effectiveness of an aloe vera–rosemary combination compared with aloe vera alone, rosemary oil alone, and standard care in preventing PIs among orthopedic patients.
Literature Review
Pressure injuries are associated with substantial clinical and economic burdens, including pain, reduced quality of life, prolonged hospitalization, and increased mortality risk (Appiah et al., 2023; Sen & Kilic, 2024). Effective prevention is therefore essential, and nurses play a central role through risk assessment, early detection, and implementation of preventive strategies (Arıburnu & Korkmaz, 2024; Källman et al., 2022; Kunimitsu et al., 2024).
Accurate staging is essential for PI assessment and management, with the six-category system widely used (Haesler, 2014). Stage 1 presents as non-blanchable erythema and may progress to full-thickness tissue loss in Stage 4, while slough, eschar, or deep discoloration may obscure staging (ALFadhalah et al., 2024). Standard prevention includes pressure-redistributing surfaces, regular repositioning, mobilization, moisture control, and nutritional support (Källman et al., 2022; Tervo-Heikkinen et al., 2022). However, prevalence in acute care remains high (6–18.5%), indicating the need for more effective complementary strategies (Dube et al., 2022; Mervis & Phillips, 2019).
Recently, herbal compounds have gained attention in PI management due to their effectiveness and low side-effect profile. Studies have evaluated various agents for prevention, including aloe vera, plant-based oils, and topical gels (Babamohamadi et al., 2019; Fallahi et al., 2022; Hekmatpou et al., 2018; Sadeghi et al., 2023), while others have focused on treatment using agents such as Calendula officinalis, aloe vera, and rosemary (Avijgan et al., 2016; Esmaili et al., 2008; Parizi et al., 2021). Evidence on aloe vera remains inconsistent, with some studies demonstrating preventive benefits and others reporting no significant effect when used alone (Fallahi et al., 2022; Hekmatpou et al., 2018).
Rosemary has been widely used in dermatological and therapeutic applications due to its anti-inflammatory, vasodilatory, and antioxidant properties (de Macedo et al., 2020). It has been shown to be an inexpensive, simple, available, and low-risk option that supports PIs healing and prevents grade 1 PIs progression in ICU patients (Parizi et al., 2021). Moreover, rosemary essential oil nanoparticles incorporated into gel showed greater capability to hydrate and increase skin elasticity than those without essential oils (Montenegro et al., 2017). However, its role in PI prevention remains underexplored.
Both aloe vera and rosemary oil have mechanisms relevant to PI prevention. Rosemary oil has anti-inflammatory, analgesic, and vasodilatory effects that improve microcirculation and tissue perfusion, and its components—camphor and p-cymene—modulate inflammatory cytokines and reduce pain (de Santana et al., 2015; Keshavarzian & Shahgholian, 2017). Aloe vera contains polysaccharides and antioxidants that provide anti-inflammatory, antibacterial, and wound-healing benefits by promoting collagen synthesis, fibroblast activity, moisture retention, and skin elasticity (Safdari et al., 2021; Sánchez et al., 2020). Both agents may be more effective together; aloe vera with oil performed better than aloe alone (Fallahi et al., 2022), and rosemary with gel improved absorption (Akbari et al., 2015).
Most studies used high concentrations of aloe gel (pure vs. 94%) and rosemary cream, which may be difficult to apply to large areas, costly (administer 10-15 mL twice daily or three times daily for prevention) and more likely to cause allergies, whereas lower concentrations improved wound healing and may be more cost-effective (Grundmann, 2012; Moghbel et al., 2007). Although rosemary–aloe combinations appear in scalp care products (Shakeena et al., 2021), no studies have evaluated them for skin care. Therefore, combining aloe vera gel with rosemary oil is expected to yield superior PI prevention compared to using either agent alone.
Aloe vera and rosemary oil have complementary mechanisms relevant to PIs prevention and fit within nursing roles for maintaining skin integrity. Despite these promising properties, no clinical studies have evaluated the combined use of aloe vera and rosemary oil for PI prevention, particularly among orthopedic patients. This gap highlights the need for further investigation of this combination as a potential nursing intervention.
Materials & Method
Design, Participants, and Setting
This triple-blind, randomized, four-arm parallel clinical trial used a 1:1:1:1 allocation ratio and was powered for the prespecified primary comparison of the combined aloe vera–rosemary group versus the control group (superiority, two-sided). Participants were recruited from the orthopedic units at Mansoura University Hospital between November 2022 and April 2023. This trial was conducted and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 guidelines.
Sample size was determined using the GIGA Power & Sample Size Calculator (https://www.gigacalculator.com/calculators/power-sample-size-calculator.php) and informed by prior randomized controlled trials (Fallahi et al., 2022; Hekmatpou et al., 2018). Control-group pressure injury (PI) incidence was set at 31%, representing the midpoint of the range (21.1%–36.7%) reported in prior RCTs. This strategy was adopted to minimize the risk of underpowering the study due to an underestimated event rate while avoiding inflation of the required sample size based on an extreme value.
The sample size calculation was explicitly based on the prespecified primary outcome of stage I PI incidence. The calculation targeted detection of a minimum detectable absolute difference (MDE) of 30.2 percentage points in PI incidence. Statistical power was set at 80% (1−β = 0.80). To account for multiple comparisons across the three intervention arms sharing a common control, a two-sided Type I error rate of 2.5% (α = 0.025) was specified, with multi-arm adjustments implemented by the calculator for comparisons versus a shared control.
For binary outcomes in a multi-arm superiority trial comparing

where
Evidence from Hekmatpou et al., (2018) demonstrated a moderate association between intervention and PI incidence (Cramer’s V = 0.302; χ2 = 7.001; N = 77), which supported the plausibility of the anticipated effect magnitude. Accordingly, the assumed absolute difference of 30.2 percentage points was derived from effect estimates reported in prior randomized trials of comparable preventive interventions and was selected as a clinically meaningful superiority margin for the prespecified primary comparison rather than an optimistic effect assumption. Importantly, the observed between-group difference in total PI incidence in the present trial was consistent with this assumption, supporting the adequacy of the original sample size calculation. The trial was powered for the prespecified primary comparison (aloe vera–rosemary combination versus control) rather than for detecting smaller effects across all secondary comparisons. In addition, a post hoc power analysis based on the observed primary outcome effect size (Cramer’s V = 0.28) indicated achieved power of 82.7%, further supporting adequate statistical power for the primary endpoint.
Of 200 participants assessed for eligibility, 160 met the inclusion criteria and were randomized. All randomized participants received their allocated intervention. During follow-up, 12 participants were not included in the final analysis due to post-randomization attrition: three withdrew consent and nine were discharged early before completing the 10-day follow-up period. Therefore, 148 participants completed follow-up and were included in the final (per-protocol) analysis. Participant flow is presented in the CONSORT diagram (Figure 1). Consort flow chart of the study enrolment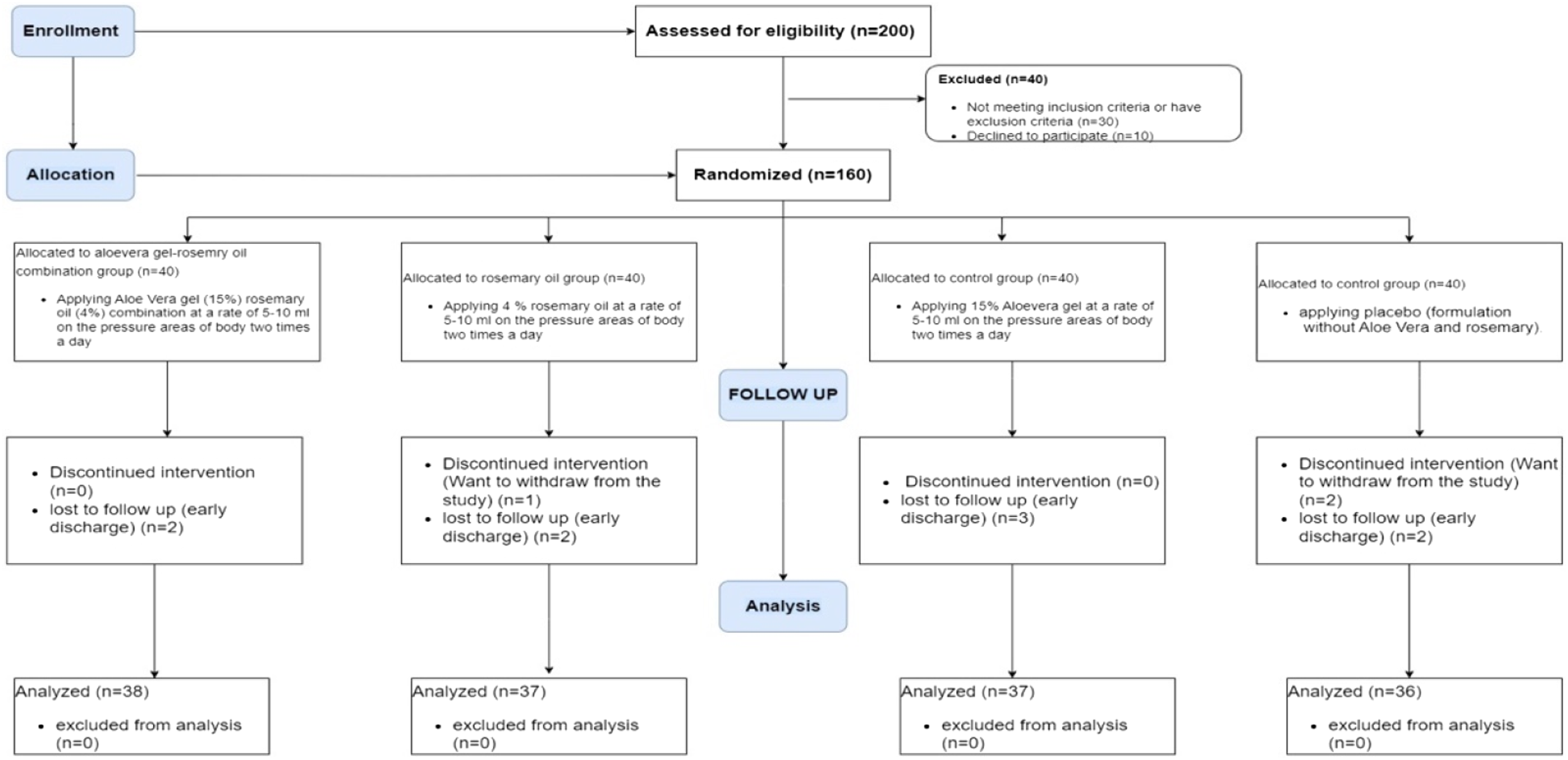
Eligible participants were adults aged 18–60 years who consented to join the study, a range chosen to avoid age-related skin changes and chronic disease confounding. They had no skin conditions (e.g., fungal infections, psoriasis, freckles), were at moderate to severe PIs risk based on nursing diagnosis and a Braden score below 13–14, and had no PIs on admission. Participants were therefore free of PIs at baseline and were monitored daily for the development of Stage I PIs during the 10-day follow-up period. They were expected to stay more than 10 days based on surgery type and predicted recovery time. Patients had to be admitted within the previous 24 hours and have no prior recent hospitalizations. Exclusion criteria included withdrawal from the study, a drop in hemoglobin to <12 mg/dL in males or <10 mg/dL in females, fever above 38.8 °C during the study, or sensitivity to aloe vera or rosemary.
Randomization and Blinding
Block randomization with a fixed block size of 16 was used to allocate 160 patients equally into four groups: aloe vera–rosemary (n = 40), rosemary (n = 40), aloe vera (n = 40), and control (n = 40) in a 1:1:1:1 ratio. A block size of 16 was selected because it is a multiple of the four study arms and ensured balanced allocation within each block throughout the enrollment period while minimizing temporal imbalance.
The randomization sequence was computer-generated by an independent researcher who was not involved in participant recruitment, intervention administration, or outcome assessment, using Sealed Envelope software (https://www.sealedenvelope.com/simple-randomiser/v1/lists). Allocation concealment was maintained using sequentially numbered, opaque, sealed envelopes, each signed across the seal and stored securely. Envelopes were opened sequentially only after written consent and completion of baseline assessment, and the allocation codes were concealed from all investigators until the intervention. The first enrolled participant received envelope number one, and subsequent participants followed the sequence accordingly. Group assignments corresponded to pre-coded, identical bottles labelled with letters, ensuring allocation to the aloe vera–rosemary combination, rosemary, aloe vera, or control groups. To maintain triple blinding, neither the trained nurse administering the interventions, the patients, the outcome assessors, nor the statistician analyzing the data were aware of group assignments and the bottle contents (aloe vera gel, rosemary oil, aloe vera–rosemary combination, or placebo). To assess blinding integrity, outcome assessors were asked at the end of the study to guess group allocation. Correct identification did not exceed the 25% expected by chance in a four-arm trial, supporting preservation of assessor blinding.
Outcomes
The prespecified primary outcome was the incidence of stage I PIs within 10 days of follow-up, assessed using the NPUAP staging system at days 3, 7, and 10. Secondary outcomes included daily changes in skin temperature at pressure-prone areas and pain intensity measured using a 100-mm Visual Analog Scale (VAS). All outcomes were prespecified in the registered clinical trial protocol (https://ClinicalTrials.gov Identifier: NCT05578638; registered on 13 October 2022).
Tools
Four tools were utilized in the present study to evaluate outcomes, including:
Demographic and clinical information sheet: Developed by researchers based on the literature, including age, gender, BMI, and type of orthopedic surgery. Reviewed by three medical-surgical nursing experts with a content validity index of 0.91.
Braden scale: Assesses key factors related to PIs occurrence, including sensory perception, moisture, activity, mobility, nutrition, friction, and shear (Amirifar et al., 2014; Cooper, 2013;
National pressure ulcer advisory panel (NPUAP) staging scale: It includes four main stages plus categories for deep tissue injury and unstageable PIs. In this study, non-blanchable redness under finger pressure was classified as Stage I (Edsberg et al., 2016). Reliability studies showed 65% agreement among nurses and specialists (Kappa = 0.514). Expert evaluations using 56 photographs demonstrated higher agreement (94.5%; multirater Kappa = 0.80) (Babamohamadi et al., 2019).
A daily record checklist was used to monitor pain intensity and skin temperature at the sacrum, hip, and heel pressure points for 10 days. Pain intensity was assessed using a 100 mm Visual Analog Scale (VAS), and patients rated pain daily at each site. Skin temperature at the same regions was measured using a non-contact infrared thermometer (NC 150, Microlife AG, Widnau, Switzerland). The device allows hygienic, non-invasive temperature measurement without direct contact with the skin and is widely used in clinical settings. PI development was assessed according to the National Pressure Ulcer Advisory Panel (NPUAP) staging guidelines (Edsberg et al., 2016; Haesler, 2019). Assessments were performed at consistent times each day. A trained nurse and a specialist collected all outcome data, with periodic cross-checks to ensure consistency and minimize observer bias.
Materials of the Study
Plant Material and Chemicals
The leaves of Rosmarinus officinalis were collected from the Faculty of Pharmacy farm, Mansoura University in Egypt. Associate Prof. Dr Mahmoud Makram Qassem from the Vegetables and Floriculture Department at the Faculty of Agriculture affiliated with Mansoura University in Egypt. Aloe vera green gel (Aloe barbadensis Miller) was purchased from a standardized commercial source (Patanjali Ayurved, Haridwar, India) with a mucilage content of 13.22%, determined by gravimetric assay. Absolute ethanol (ETOH), tween 80 (T80), and benzyl alcohol (BZA) were obtained from El-Gomhoreyah Company for Trading Chemicals and Medical Appliances, Cairo, Egypt.
Essential Oil Isolation
A total of 1 kg of fresh rosemary leaves was subjected to hydrodistillation for approximately 6 hours using a Clevenger-type apparatus, with distilled water used to extract the hydrophobic essential oils (Fagbemi et al., 2021). During distillation, the hydrated plant material was heated to evaporate volatile compounds, which were subsequently condensed and collected. The oil phase was separated from the aqueous phase using a separating funnel. The extraction process was repeated three times to maximize oil recovery. The obtained essential oil was dried over anhydrous sodium sulfate to remove residual moisture and stored in dark glass vials at 4 °C till tested.
Identification of the Rosemary Essential Oil Constituents
The analysis of the essential oil from Rosmarinus officinalis leaves and the identification of its constituents were performed utilizing retention indices, data stored on the mass spectral database NIST/CHEMStation, and/or mass spectral fragmentation patterns. The GC-MS analysis identified 30 constituents representing 100% of the total oil composition Table S1 and Figure S1). The non-oxygenated fraction percentage of the oil was 52.13%. Monoterpene hydrocarbons (45.85%) were the most prevalent non-oxygenated constituents, and p-Cymene (15.98%) was the fundamental component, followed by iso-camphane (8.33%), iso-terpinolene (7.78%), and γ-Terpinene (4.40%), in addition to other minor monoterpene hydrocarbons. β-Caryophyllene (4.83%) was found to be the major sesquiterpene hydrocarbon. The oxygenated fraction represented about 47.89 %, in which alcohols were the major (21.76%), followed by ketones (13,04%), esters (7.48%), epoxides (4.72%), acids (0.56%), and aldehydes (0.33%) in a descending order. Camphor (11.03%) was the dominant ketonic component, followed by α- α-α-α-Terpineol (10.40%), Linalool (5.80%), and γ-Terpineol (4.75%) as the major alcohols, while Eucalyptol (4.26%) was the major oxide present. In addition, the most abundant ester was Borneol acetate (4.61%).
Method of Preparation of Emollient Spray
The composition of 15% (w/w) aloe vera (ALV) and 4.0% (w/w) rosemary oil (RSM) is shown in Table S2. The rosemary oil concentration (4%) was selected within the range commonly used for topical essential oil formulations (Hadizadeh-Talasaz et al., 2022; Parizi et al., 2021). Four different spray formulations, namely PS (plain formulation without ALV or RSM oil), ALVS (with ALV gel only), RSMS (with RSM oil only), and ALV/RSMS (with both ALV gel and RSM oil), were prepared. The spray was prepared by adding the ALV and T80 in deionized water (DW) and ETOH with constant stirring at moderate speed (100 rpm) for 1 h to complete homogenization, and the other components were added. The total weight was adjusted to 100.0 grams with DW. All formulations were prepared under hygienic laboratory conditions and transferred into clean containers to maintain product stability. All formulations (PS, ALVS, RSMS, and ALV/RSMS) were dispensed into identical amber spray bottles that were indistinguishable in appearance, smell, and color. The placebo spray consisted of deionized water, ethanol, Tween-80, and benzyl alcohol, formulated to match the viscosity, color, and odor of the active sprays. The hydrodistillation process used to extract rosemary oil yields a final volatile oil free of hydrophilic residues. As the aqueous distillate contains no detectable non-volatile compounds, incorporating hydrodistillation by-products into the placebo would not be chemically meaningful. Therefore, the placebo was formulated to mimic the sensory characteristics (color, viscosity, odor) of the active sprays while avoiding the addition of volatile constituents that could exert independent biological effects.
The bottles were labeled only with the letters A, B, C, or D according to a random coding scheme. To maintain blinding, neither the trained nurse administering the interventions, the patients, nor the statistician analyzing the data were aware of the contents of the bottles (aloe vera gel, rosemary oil, aloe vera–rosemary combination, or placebo). The study supervisors and pharmacists were the only individuals with access to the allocation code, which was disclosed only after data analysis was completed. All sprays were prepared fresh weekly, stored at 4 °C, and used within 7 days. No visible degradation or phase separation was observed during the trial. To enhance reproducibility, all formulations were prepared using the same standardized protocol, ingredient ratios, and preparation procedures for each batch. Batch preparation was performed under controlled laboratory conditions, and no visible instability or phase separation was observed during the study period. Potential variability in intervention delivery was minimized through standardized nurse training, protocolized twice-daily application, and documented intervention logs to ensure consistency in application technique.
Implementation
After obtaining informed consent from the patient on the first day of hospitalization, pre-test data were collected using tool I, which included demographic information and past medical history, prior to the intervention. The Braden Scale (Tool II) was used to evaluate the risk of PI development in four patient groups. Then, at day 0, before applying sprays, patients were also assessed for PIs using tool III, skin temperature, and pain level using tool IV. Patients meeting the inclusion criteria were randomly assigned to four groups.
Nurses in orthopedic wards received standardized training on applying the sprays. Prior to enrollment, sensitivity to aloe vera or rosemary was tested on a 2 × 2 cm area of the patient’s forearm, and swelling, warmth, or redness were assessed after 30 minutes. In all four groups, 10 mL of the designated spray was applied twice daily during routine skin care to areas at risk for PI development (sacrum, hip, and heel). The application continued for 10 days; patients discharged before day 10 were excluded. The intervention was applied only to intact skin at pressure-prone areas. If a PI developed during follow-up, the intervention was discontinued at the affected site and the patient received standard wound care according to institutional clinical protocols. In accordance with the protocol term “rubbing,” the sprayed solution was gently spread over the skin using light, superficial strokes solely to ensure even distribution, without applying pressure, circular movements, or deep massage. This gentle spreading did not generate friction or shear forces that might predispose to PI. After even distribution, the spray was allowed to dry naturally. Group 1 received the aloe vera–rosemary combination spray; group 2 received rosemary oil spray; group 3 received aloe vera gel spray; and group 4 received the placebo. All groups also received routine PI prevention care, including skin hygiene monitoring, adequate nutrition, scheduled repositioning, pressure-relief mattresses, and skin-damage prevention. Environmental and clinical care conditions were standardized across all groups. All participants were admitted to the same orthopedic wards, received care from the same nursing staff, and were managed according to identical institutional PI prevention protocols, including scheduled repositioning, pressure-relief mattresses, nutritional monitoring, and skin hygiene practices. Room temperature and ward conditions were consistent across study groups. In addition, potential clinical confounders such as comorbidities, medication use, and analgesic administration were expected to be balanced across groups through randomization. Randomization was expected to balance any remaining unmeasured environmental factors between groups.
Adherence to the twice-daily application protocol was ensured through direct administration by trained ward nurses during routine inpatient skin care. Each application was documented in a standardized intervention log. Missed doses were recorded; no scheduled applications were missed among participants who remained hospitalized during the 10-day follow-up period.
Before spray application, two observers, a trained nurse and a specialist, assessed the patients at 9:00 am daily for 10 days to monitor the PIs’ development using tools III and IV. Observers were unaware of the patient group and evaluated the high-risk areas every day before applying the spray. The same nurse and specialist conducted all daily assessments to ensure consistency.
Statistical Analysis
Data were analyzed using IBM SPSS v. 27.0. Prior to inferential analyses, data were screened for statistical assumptions. Normality was evaluated across the four study groups using skewness and kurtosis statistics, standardized z-scores (±3.29), and visual inspection of histograms and Q–Q plots. No substantial departures from normality or extreme outliers were observed, supporting the use of parametric analyses. Descriptive statistics were presented as means ± SD, frequencies, and percentages. Chi-square tests, Fisher’s exact test, one-way ANOVA, repeated measures ANOVA, and Bonferroni-adjusted post hoc comparisons were used for inferential analyses. Bonferroni correction was applied to exploratory post hoc pairwise comparisons following repeated-measures ANOVA (Table 2). For PI incidence outcomes (Table 3), analyses were prespecified rather than exploratory multiple testing, with total PI incidence designated as the primary endpoint and site-specific outcomes interpreted as supportive secondary outcomes; therefore, no additional multiplicity adjustment was applied. The primary endpoint remained statistically significant under a conservative Bonferroni-adjusted threshold for four comparisons (α = 0.0125; p = .009). Univariable logistic regression was first performed to examine associations between candidate predictors and PI occurrence. Variables considered clinically relevant or associated with the outcome in univariable analyses were then entered into a multivariable logistic regression model to identify independent predictors while adjusting for potential confounding. Group allocation was retained in the adjusted model irrespective of statistical significance because it represented the prespecified primary intervention variable of interest. In addition, an intention-to-treat sensitivity analysis for the primary outcome was conducted using multiple imputation (20 imputations), alongside the primary per-protocol analysis.
Ethics Approval and Consent to Participate
Approval (number. P.0270) was acquired from the Institutional Review Board of the Faculty of Nursing affiliated with Mansoura University, Egypt. Written informed consent was secured, and participants were assured of voluntary participation and the right to withdraw without affecting their care. The study adhered to the Declaration of Helsinki. Collection and use of Rosmarinus officinalis complied with institutional, national, and international guidelines; a qualified botanist verified plant identification, and necessary permissions were obtained according to local regulations.
Results
Comparing Demographic and Clinical Variables of the Four Groups
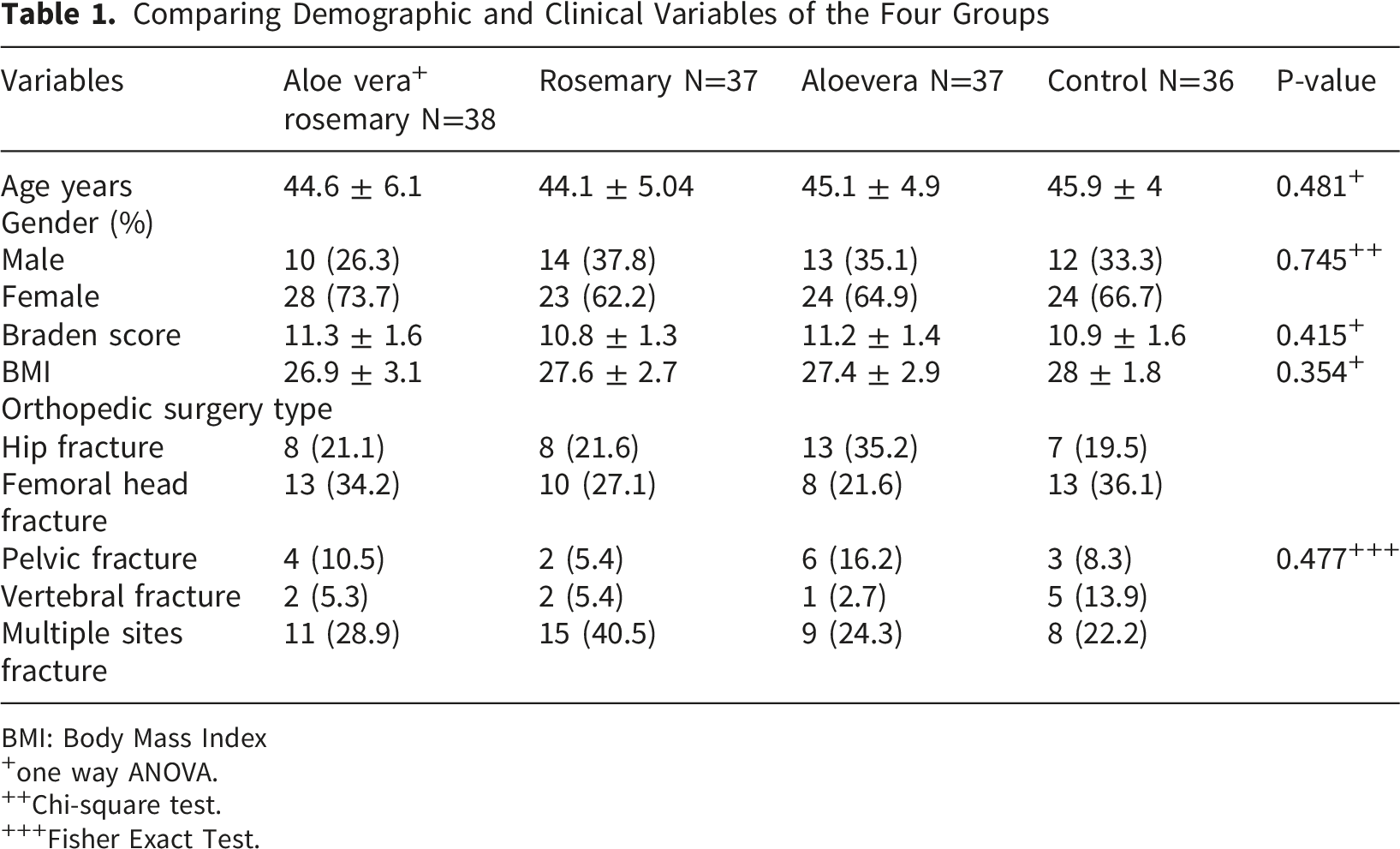
BMI: Body Mass Index
+one way ANOVA.
++Chi-square test.
+++Fisher Exact Test.
Main Effects of Time and Group and Interaction Effects on Pain and Temperature
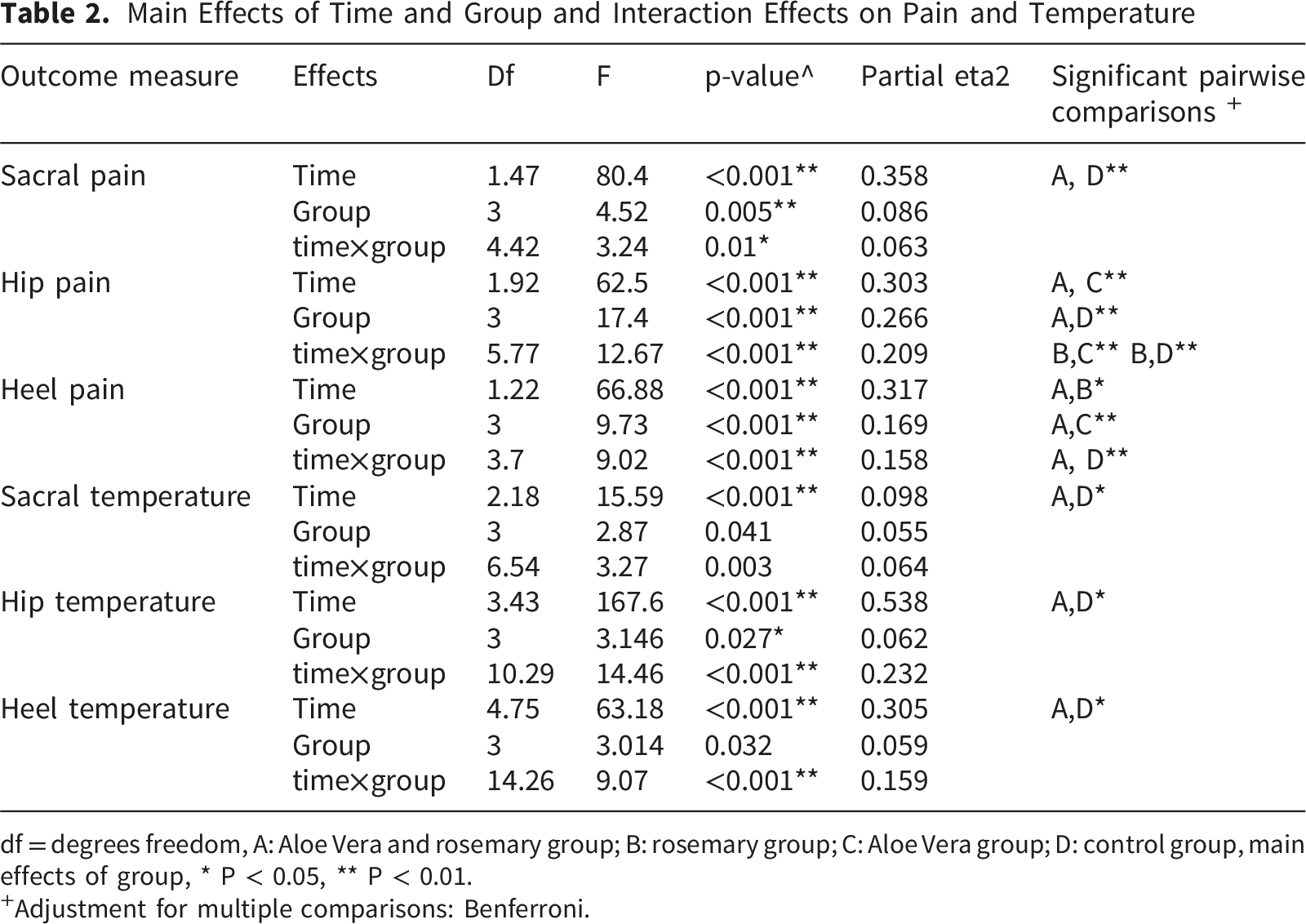
df = degrees freedom, A: Aloe Vera and rosemary group; B: rosemary group; C: Aloe Vera group; D: control group, main effects of group, * P < 0.05, ** P < 0.01.
+Adjustment for multiple comparisons: Benferroni.
Because PIs typically develop at specific anatomical pressure points, pain intensity and skin temperature were analyzed separately for the sacrum, hip, and heel to detect localized tissue changes. Table 2 also shows the partial ETA2 values for sacral, hip, and heel pain levels. According to these values, 6.3% of the variance in sacral pain, 20.9% in hip pain, and 15.8% in heel pain were accounted for by the time × group interaction. For temperature, the time-by-group interaction was also significant for sacral (p 0.003), hip (p < 0.001), and heel (p < 0.001), indicating a positive effect of the aloe vera-rosemary combination in decreasing temperature over time compared to other groups, as further clarified by pairwise comparisons. According to partial ETA2 values, 6.4% of the variance in sacral temperature, 23.2% in hip temperature, and 15.9% in heel temperature were accounted for by the time × group interaction. Detailed descriptive statistics for daily pain intensity and skin temperature across study groups from Day 0 to Day 10 are presented in Table S4.
Comparing PIs Frequency Across Study groups +

Primary comparison: RR = 0.17 (95% CI 0.04–0.72). FET: Fisher Exact Test. RR = risk ratio; CI = confidence interval; χ2 = chi-square test. Results shown are based on per-protocol analyses.
* P < 0.05, ** P < 0.01.
+not mutually exclusive.
The effect size for total PIs was small (Cramer’s V = 0.279). Compared with the control group, the aloe vera–rosemary combination significantly reduced the risk of PI (RR = 0.17, 95% CI 0.04–0.72). Sacral PIs first appeared on the eighth day in the aloe vera-rosemary group, the seventh day in the rosemary and aloe vera groups, and the fifth day in the control group. No heel or hip PIs were observed in the aloe vera-rosemary group.
Univariable, Multivariable, and Intention-To-Treat Sensitivity Logistic Regression Analyses of Pressure Injury

Note. SE = standard error; OR = odds ratio; CI = confidence interval. Panel B presents pooled estimates from multiple imputation (20 imputations) including all randomized participants. Intention-to-treat sensitivity analysis was conducted for the prespecified primary outcome only.
* P < 0.05, ** P < 0.01
Harms
No adverse events or intervention-related harms were observed during the study. Participants were monitored daily by clinical staff through direct observation and self-report for potential adverse reactions, including skin irritation, redness, swelling, or allergic responses. No participants discontinued the intervention due to adverse effects, and all participants tolerated the sprays without complications. A summary of adverse events across study groups is presented in Table S3.
Discussion
Pressure injuries are highly prevalent in orthopedic settings, making effective nursing prevention essential, particularly through continuous skin assessment for early signs such as non-blanchable erythema, temperature changes, and pain (Kottner et al., 2019; UK, 2014).
A temperature differences either warmer or cooler than surrounding tissue are key indicators of stage 1 PIs (Kottner et al., 2020). In this study, higher sacral, hip, and heel temperatures in the control group compared with the aloe vera–rosemary group reflected the combination’s effectiveness in reducing temperature changes, consistent with lower PI incidence. Warm areas indicate inflammation caused by tissue loading (Gefen et al., 2022; Kottner et al., 2020), and increased temperature is widely reported as an early sign of PI development (Sae-Sia et al., 2005; Yoshimura et al., 2015; Yusuf et al., 2015). In orthopedic patients, elevated sacral and hip temperatures, and lower heel temperature, have been associated with stage 1 PIs (Hekmatpou et al., 2018). However, ICU studies report lower sacral temperature as a predictor (Jiang et al., 2020). while others found no significant differences (Yilmaz & Günes, 2019). This variation is explained by guidelines indicating that both increased and decreased temperature may signal stage 1 PIs, depending on whether tissue is inflamed (warm) or progressing to ischemia and necrosis (cool) (Farid et al., 2012; Gefen et al., 2022; Kottner et al., 2020). Additional factors, including hypotension, hyperglycemia, and older age, may further influence temperature patterns and PI development (Aloweni et al., 2019; Jiang et al., 2020).
Pain is also an important indicator of early PI development, and was higher in the control group than in the intervention groups, particularly the aloe vera–rosemary group, with reductions also observed in the rosemary group at specific sites. These findings align with previous evidence linking pain to early PI development (Williams et al., 2024; Wilson et al., 2021). The greater reduction in the combination group may reflect synergistic anti-inflammatory and analgesic effects. Rosemary has established analgesic properties, mediated by inhibition of inflammatory mediators (Keshavarzian & Shahgholian, 2017; Kopustinskiene et al., 2022; Rahbardar & Hosseinzadeh, 2020). In the rosemary oil analysis conducted in this study, p-cymene and camphor were the main constituents of rosemary oil, with strong anti-inflammatory, anti-hyperalgesic, anesthetic, antimicrobial, and skin-protective effects, with evidence of reducing musculoskeletal pain (de Santana et al., 2015; Duda-Madej et al., 2024; Keshavarzian & Shahgholian, 2017). Aloe vera also exhibits anti-inflammatory and analgesic effects, with evidence of pain reduction in PI and orthopedic settings (García Sánchez & Mudarra García, 2024; Hekmatpou et al., 2018; Malek Hosseini et al., 2024; Safdari et al., 2021). However, In the present study, aloe vera alone did not significantly reduce pain across all sites, while rosemary alone reduced hip pain; similarly, some studies have reported increased pain with aloe vera use in certain contexts (Hoopfer et al., 2015).
This discrepancy may be explained by several factors. Orthopedic pain, which is primarily nociceptive and procedural, may not respond optimally to the aloe vera concentration used, as its analgesic effects are more evident in inflammatory or superficial skin pain. Fixed assessment timing may have missed short-term effects, and the relatively low Aloe vera concentration (15%) in spray form may have limited efficacy compared with higher concentrations or occlusive dressings used in previous studies (Hekmatpou et al., 2018; Malek Hosseini et al., 2024). Variations in aloe vera species, bioactive compound stability, and preparation methods may further influence efficacy and contribute to inconsistent findings (Fallahi et al., 2022).
The PI damage cascade involves tissue deformation, inflammation, and ischemia, and prevention strategies focus on leave-on products that enhance tissue tolerance (Gefen, 2018; Gefen et al., 2022). In this study, the aloe vera–rosemary group showed the lowest PI incidence (5%) compared with rosemary (8%), aloe vera (13.5%), and control (30.6%), with significant effects for the combination and rosemary groups but not aloe vera alone. Previous studies similarly report inconsistent findings for aloe vera, with no benefit in ICU or cancer settings but some effectiveness in orthopedic patients (Ahmadloo et al., 2017; Fallahi et al., 2022; Hekmatpou et al., 2018). The limited effect of aloe vera alone may be due to its short skin retention time and rapid evaporation (Fallahi et al., 2022).
The greasy nature of rosemary oil helps retain skin moisture and increase hydration. Combining rosemary with aloe vera appears to enhance aloe vera’s properties and create a formulation that lasts longer on the skin. Rosemary-based gels have shown superior hydration and elasticity, and rosemary has demonstrated effectiveness in accelerating healing, preventing PI progression, promoting vasodilation, and improving wound healing outcomes (de Macedo et al., 2020; Montenegro et al., 2017; Parizi et al., 2021; von Schoen-Angerer et al., 2018; Hadizadeh-Talasaz et al., 2022).
The superior effectiveness of the aloe vera–rosemary combination likely reflects synergistic mechanisms. Oils enhance absorption and retention, while aloe vera maintains hydration and skin integrity and rosemary improves microcirculation and reduces inflammation. These combined effects may reduce oxidative stress and inflammatory responses, explaining the lower pain, temperature, and PI incidence observed. Such combinations are already used in dermatologic products, supporting their complementary actions (Akbari et al., 2015; Fallahi et al., 2022; Shakeena et al., 2021).
Given the burden of PI prevention in nursing practice, the aloe vera–rosemary combination appears to be a practical, cost-effective adjunct that may improve patient outcomes and support community health.
Strengths and Limitations
This study has several strengths, including its triple-blind randomized controlled design, four-arm active comparator structure, clinically relevant primary outcome, and the addition of an intention-to-treat sensitivity analysis that supported the robustness of the findings. In addition, the intervention was standardized and delivered under controlled clinical conditions, enhancing internal validity.
This study also has limitations. First, few comparable randomized controlled trials were available, as most prior studies examined aloe vera alone, used traditional controls, or did not evaluate rosemary oil or the aloe vera–rosemary combination, particularly in orthopedic patients. Second, follow-up was limited to 10 days; therefore, delayed PIs after discharge may not have been captured, potentially underestimating incidence. However, this period was selected to reflect the highest-risk postoperative hospitalization period and the prespecified early-stage PI endpoint. Third, although the primary analysis was conducted per protocol, an intention-to-treat sensitivity analysis using multiple imputation yielded consistent findings, reducing concern regarding attrition bias. Fourth, the sample included only adults aged 18–60 years and patients at moderate to severe risk, limiting generalizability to pediatric, older adult, or lower-risk populations. Fifth, pain intensity was self-reported and may be subject to variability or reporting bias. Sixth, the study was conducted in orthopedic wards only, which may limit transferability to other clinical settings such as intensive care or geriatric units. Finally, skin hydration and inflammatory biomarkers were not measured due to resource constraints. Although clinical indicators such as skin temperature, pain intensity, and PI incidence provide meaningful evidence of preventive effects, they do not directly reflect underlying physiological mechanisms. Objective measures such as inflammatory cytokines, microcirculatory markers, transepidermal water loss, and skin hydration indices could provide deeper mechanistic insight into how aloe vera and rosemary oil influence tissue integrity, perfusion, and early PI development. Future studies should incorporate biomarker assessments, larger samples, longer follow-up, and broader clinical settings to strengthen mechanistic understanding and generalizability.
Implications for Nursing Practice
Findings from this trial suggest that nurse-applied aloe vera–rosemary spray, and rosemary oil alone, may serve as low-cost adjuncts to support PI prevention in at-risk orthopedic patients. As a nurse-delivered topical intervention, the formulation may complement routine care such as repositioning, pressure-relieving surfaces, skin assessment, and moisture management. Its potential to reduce early PI occurrence, pain, and localized temperature changes may help preserve skin integrity postoperatively.
These findings highlight the potential role of evidence-informed herbal adjuncts within preventive skin care protocols, particularly in resource-limited settings. Such interventions may expand nurses’ options for early prevention; however, broader implementation requires confirmation from larger multicenter trials and longer-term follow-up.
Conclusion
The study shows that rosemary oil and the aloe vera–rosemary combination effectively prevent PIs in orthopedic surgery patients. Based on these benefits, the combination is recommended as an adjunct to standard PI prevention measures such as repositioning and pressure-relieving surfaces. Incorporating these herbal agents into care may improve outcomes and reduce the healthcare costs of PI management. Future studies should include larger samples and diverse clinical settings, particularly high-risk areas such as intensive care, geriatric, and rehabilitation units. Further research is also needed to evaluate the therapeutic potential of these compounds for treating existing PIs.
Supplemental Material
Supplemental Material - Effect of Nurse-Applied Aloe Vera and Rosemary Oil Combination on Pressure Injury Prevention in Orthopaedic Surgery: A Triple-Blind Randomized Trial
Supplemental Material for Effect of Nurse-Applied Aloe Vera and Rosemary Oil Combination on Pressure Injury Prevention in Orthopaedic Surgery: A Triple-Blind Randomized Trial by Mohamed E.H Elzeky, Awatef abdelhamid, Basma Salameh, Noha F.M. Shahine, Amal F. Soliman, Amgad E. Salem, Barakat Sayed Elalfy, Rasha Hafez Ramadan El-Shaboury in Sage Open Nursing
Supplemental Material
Supplemental Material - Effect of Nurse-Applied Aloe Vera and Rosemary Oil Combination on Pressure Injury Prevention in Orthopaedic Surgery: A Triple-Blind Randomized Trial
Supplemental Material for Effect of Nurse-Applied Aloe Vera and Rosemary Oil Combination on Pressure Injury Prevention in Orthopaedic Surgery: A Triple-Blind Randomized Trial by Mohamed E.H Elzeky, Awatef abdelhamid, Basma Salameh, Noha F.M. Shahine, Amal F. Soliman, Amgad E. Salem, Barakat Sayed Elalfy, Rasha Hafez Ramadan El-Shaboury in Sage Open Nursing
Footnotes
Acknowledgment
We thank all subjects, nursing staff at the Mansoura university hospital who participated in the study.
Ethical Considerations
Approval (number. P.0270) was acquired from the Institutional Review Board of the Faculty of Nursing affiliated with Mansoura University, Egypt. All participant rights were preserved, and informed written consent was obtained. They were assured that their participation is voluntary and that they can withdraw at any time, with no effect on their hospital treatment plan. During our study, the Declaration of Helsinki ethical principles were followed. The collection and use of plant materials (Rosmarinus officinalis) complied with institutional, national, and international guidelines. A qualified botanist conducted plant identification, and appropriate permissions were obtained in line with local regulations.
Authors’ contributions
M.E.H.E designed the study. A.A, B.S.E, H.R collected the data. M.E.H.E, A.A, N.F.M.S, A.F.S, A.E.S analyzed the data. M.E.H.E, A.A, B.S, N.F.M.S, A.F.S, A.E.S, B.S.E, H.R prepared the manuscript. M.E.H.E, A.A, B.S, N.F.M.S, A.F.S, A.E.S, B.S.E, H.R approved the final version for submission
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Researchers declares no conflict of interest with any organization regarding the materials discussed in this paper.
Data Availability Statement
The data utilized to support the results of the research are accessible to the corresponding author upon request.
Trial Registration
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.