
Abstract
Introduction
Workplace violence (WPV) is a major occupational safety concern in emergency departments, where healthcare professionals frequently interact with distressed patients and families under conditions of high workload and crowding. Shorter professional experience and perceived overcrowding may be associated with greater exposure to WPV, while formal reporting of incidents often remains limited.
Aim
This study aimed to examine the prevalence of WPV exposure and formal reporting behavior among emergency healthcare professionals and to assess the association of professional experience and perceived overcrowding with WPV exposure.
Methods
An analytical cross-sectional study was conducted among 300 nurses and physicians working in emergency departments of three tertiary hospitals within a large public healthcare system. A non-probability convenience sampling method was used. Data collection took place between January 2025 and April 2025 using a structured paper-based self-administered questionnaire. Descriptive statistics were used to summarize WPV exposure, perceived risk factors, preventive strategies, and reporting behavior. Multivariable logistic regression was used to examine factors associated with WPV exposure.
Results
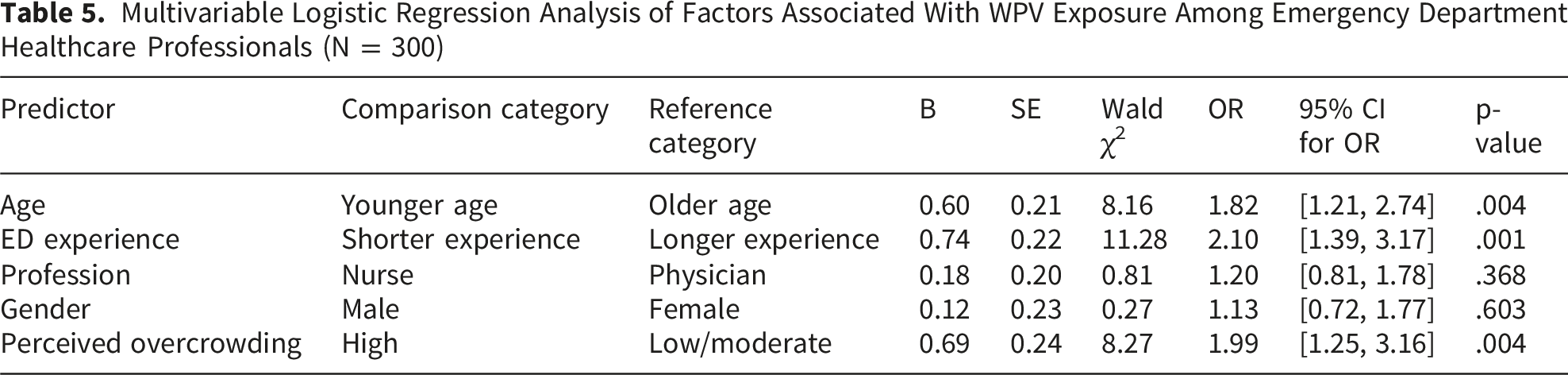
Overall, 71.3% of participants reported exposure to WPV, and only 34.6% of exposed participants formally reported the most recent incident. Shorter emergency department experience was associated with higher odds of WPV exposure (OR = 2.10, 95% CI: 1.39–3.17, p < .001). High perceived overcrowding was also associated with increased odds of WPV exposure (OR = 1.99, 95% CI: 1.25–3.16, p = .004). Profession and gender were not significantly associated with WPV exposure in the multivariable model.
Conclusion
WPV exposure was common among emergency healthcare professionals, whereas formal reporting was low. Shorter professional experience and perceived overcrowding were associated with greater odds of WPV exposure. These findings support the need for organizational strategies that strengthen violence prevention, support less experienced staff, and improve formal reporting systems.
Keywords
Introduction
Workplace violence (WPV) is a major occupational safety concern in healthcare settings, particularly in emergency departments (EDs). WPV refers to incidents in which healthcare workers are physically assaulted, threatened, verbally abused, harassed, intimidated, or exposed to other disruptive behaviors while performing work-related duties (Occupational Safety and Health Administration, nd.). In healthcare environments, WPV may include verbal abuse, threats, bullying, physical assault, and other aggressive behaviors directed toward staff by patients, relatives, visitors, or, less commonly, coworkers.
EDs have perennially emerged as one of the biggest risk areas in the occurrence of WPV because of factors like overcrowding, waiting times, acuity of patients, exposure to distressed patients and their families, and exposure to patients influenced by substance use or acute mental health crises (Alqaissi et al., 2025a; Farajalla, 2025; Phillips, 2016; Qtait, Amro, et al., 2026). Such factors create stress and sources of aggravation for both the patients and the staff members, thus contributing to a heightened risk of WPV occurrence (Dopelt et al., 2022).The impact of exposure to WPV in ED settings has been reported to result in adverse effects on job performance and staff turnover, posing risks to patient safety (Vrablik et al., 2019).
WPV against healthcare professionals is not only an individual safety issue but also an organizational and public health problem. A systematic review and meta-analysis by Liu et al. (2019) reported that WPV is highly prevalent among healthcare workers, with emergency and psychiatric settings among the highest-risk clinical environments. Exposure to WPV has been associated with psychological distress, burnout, reduced job satisfaction, absenteeism, turnover intention, and impaired quality of care (Liu et al., 2019; Vrablik et al., 2019). These consequences are especially concerning in EDs, where staff must maintain rapid decision-making, communication, and clinical vigilance despite high workload and repeated exposure to stressful encounters (Farajalla et al., 2026a).
Emergency department overcrowding has increasingly been recognized as an important organizational factor associated with WPV. Professional experience may also be associated with WPV exposure and reporting behavior. Underreporting of WPV remains another major challenge (Arnetz et al., 2015). Formal reporting systems are essential for identifying patterns of violence, planning preventive measures, allocating security resources, and supporting affected staff. Therefore, reporting behavior should be examined as a distinct outcome rather than assumed from WPV exposure alone.
Although international evidence confirms that WPV is common in EDs, important gaps remain in understanding how workforce characteristics and perceived organizational pressures are associated with exposure and formal reporting. Much of the literature focuses either on prevalence, risk factors, or consequences, while fewer studies examine professional experience, perceived overcrowding, WPV exposure, and reporting behavior within the same study. In addition, local and regional healthcare contexts require further attention because patterns of violence and reporting may be influenced by staffing structures, patient flow, institutional safety culture, security arrangements, public trust, and broader sociopolitical pressures.
Review of the Literature
WPV in EDs has been widely documented as a persistent occupational safety problem affecting healthcare professionals across different health systems. Evidence from systematic reviews indicates that healthcare workers experience multiple forms of WPV, including verbal abuse, threats, bullying, and physical assault, with EDs consistently identified as among the highest-risk clinical settings (Liu et al., 2019). This elevated risk is partly related to the nature of emergency care, where staff provide rapid clinical assessment and treatment under conditions of uncertainty, high emotional distress, acute illness, and frequent interaction with patients and relatives (Farajalla et al., 2026b). However, WPV should not be understood only as a behavioral problem caused by individual aggressors; rather, it is increasingly recognized as a complex occupational and organizational phenomenon shaped by patient-related, staff-related, institutional, and system-level factors (Vrablik et al., 2019; Xie et al., 2025).
International literature shows that verbal abuse is usually the most frequently reported form of WPV, followed by threats and physical violence. In their systematic review and meta-analysis, Liu et al. (2019) found that WPV against healthcare workers was common globally, although prevalence estimates varied substantially across countries, clinical settings, measurement tools, and recall periods. This variation is important because studies that combine different forms of violence into one general outcome may produce high prevalence estimates but provide limited insight into severity, frequency, perpetrators, or prevention priorities (Alqaissi et al., 2025b; Liu et al., 2019). Therefore, when comparing WPV prevalence across studies, differences in definitions, recall windows, sampling methods, and professional groups must be considered rather than assuming that prevalence differences reflect true differences in risk alone. Overcrowding, patient waiting time, heavy workloads, patient dissatisfaction, substance abuse, and inadequately treated mental health issues are found to be the primary risk factors (Dopelt et al., 2022; Farajalla, 2026c; Farajalla et al., 2026d; Phillips, 2016; Qtait et al. 2026; Ramacciati & Morales Palomares, 2025). In a worldwide study, WPV produces alarming consequences, including burnout, anxiety, low job satisfaction, and turnover intentions among healthcare workers such as doctors and nurses (Phillips, 2016; Vrablik et al., 2019).
Regional evidence also supports the significance of WPV in emergency care settings. In Saudi Arabia, Harthi et al. (2020) reported that WPV was prevalent among healthcare workers in public hospital EDs, with verbal abuse being the most common form. The authors emphasized the need to improve awareness of reporting systems and encourage formal reporting of violent incidents. Similarly, Shafran-Tikva et al. (2017), in a mixed-methods study conducted in Israel, showed that violence against physicians and nurses was shaped by interactions among patients, relatives, healthcare professionals, and organizational conditions. Extending this evidence to neighboring regions, Al Smadi (2026) examined WPV in Jordanian hospitals and found that sociodemographic and occupational characteristics influenced violence exposure, with significant effects on perceived quality of care. The study recommended multilevel solutions including policy enforcement and staff support systems. In the European context, Koutsofta et al. (2025) explored emergency nurses’ experiences of WPV in Cyprus, identifying an “empathy gap” between nurses and patients/relatives as a key theme, along with divergent needs that escalate into aggression. These regional findings suggest that WPV in EDs is not only related to individual patient behavior but also to communication difficulties, waiting time, perceived unmet needs, and institutional responses to violence (Al Smadi, 2026; Harthi et al., 2020; Koutsofta et al., 2025; Shafran-Tikva et al., 2017).
Emergency department overcrowding is one of the organizational factors most frequently associated with WPV. Crowding may increase tension through prolonged waiting times, reduced privacy, delayed care, limited staff availability, and dissatisfaction among patients and families. Xie et al. (2025) synthesized evidence on ED crowding and patient-initiated violence against nurses and concluded that crowding contributes to a work environment in which frustration, uncertainty, and perceived neglect may escalate into aggression. Nevertheless, most studies rely on perceived overcrowding rather than objective indicators such as patient-to-staff ratios, waiting time, boarding time, or ED occupancy. This distinction is important because perceived overcrowding may be influenced by previous exposure to violence, workload stress, or organizational climate. Therefore, perceived overcrowding should be interpreted as an important staff-reported organizational stressor, but not as direct evidence that crowding causes violence in cross-sectional research (Xie et al., 2025).
Professional experience is another factor that may shape WPV exposure and reporting behavior. Less experienced healthcare professionals may have fewer opportunities to develop confidence in communication, conflict de-escalation, role negotiation, and recognition of escalating aggression. They may also be more likely to work in high-contact roles or seek assistance less readily when exposed to aggressive behavior. In contrast, more experienced staff may have greater familiarity with ED routines, institutional reporting procedures, and strategies for managing difficult interactions. However, the relationship between experience and WPV should be interpreted cautiously. Cross-sectional studies cannot confirm whether limited experience increases WPV exposure, whether exposure changes staff perceptions, or whether other unmeasured factors, such as shift type, staffing level, patient acuity, or security presence, explain the association. For this reason, professional experience is best described as a factor associated with WPV exposure rather than as a confirmed determinant or protective factor.
Underreporting is a central challenge in WPV research and practice. Formal incident reports are often used by institutions to monitor violence, identify high-risk areas, allocate resources, and develop prevention policies. However, the literature consistently shows that many healthcare workers do not formally report violent incidents. Spencer et al. (2023), in a systematic review, found that nurses’ underreporting of patient- and visitor-perpetrated WPV was influenced by normalization of violence, lack of trust in institutional responses, time pressure, fear of blame, and the belief that reporting would not result in meaningful action. Recent evidence on reporting barriers also emphasizes that underreporting is shaped by organizational culture and the perceived usefulness of reporting systems, not simply by individual staff attitudes (Spencer et al., 2023; Xu et al., 2025).
The literature also suggests that profession may influence both exposure to WPV and reporting practices, although findings are not always consistent. Nurses are often described as highly exposed because of their continuous bedside presence, prolonged contact with patients and relatives, and involvement in emotionally sensitive care situations(Alqaissi et al., 2026; Farajalla et al., 2026e; Mesk et al., 2025; Sbaih et al., 2025). Physicians may also experience WPV, particularly when communicating diagnoses, treatment delays, admission decisions, or discharge plans. Studies that include both nurses and physicians are therefore valuable because they allow comparison across professional groups. However, if profession is not statistically associated with WPV exposure in multivariable analysis, the discussion should avoid portraying nurses as uniquely or independently at higher risk unless supported by subgroup analysis or interaction testing.
Overall, existing literature indicates that WPV in EDs is a multifactorial problem shaped by organizational stressors, workforce characteristics, patient–family interactions, and institutional reporting culture. Nevertheless, several gaps remain. First, many studies focus primarily on prevalence without sufficiently examining reporting behavior as a distinct outcome. Second, overcrowding is often discussed as a major contributor to WPV, but it is frequently measured subjectively rather than through objective ED crowding indicators. Third, professional experience is commonly included as a demographic variable but is less often integrated into a broader explanation of vulnerability, coping, and reporting. Finally, regional and local evidence remains limited compared with international literature. Addressing these gaps, the present study examines WPV exposure and formal reporting behavior among emergency healthcare professionals and assesses the association of professional experience and perceived overcrowding with WPV exposure, while interpreting findings cautiously within the limits of cross-sectional self-reporteddata.
Aim and Objectives
This study aimed to examine WPV exposure and formal reporting behavior among emergency department nurses and physicians and to assess whether professional experience and perceived overcrowding were associated with WPV exposure. Specifically, the study sought to estimate the prevalence of WPV exposure, describe formal reporting behavior among exposed participants, examine the associations of professional experience and perceived overcrowding with WPV exposure, and describe perceived organizational contributors and preventive strategies related to WPV in emergency departments.
Methods
Study Design
This study used an analytical cross-sectional quantitative design. This design was appropriate because the study aimed to estimate the prevalence of WPV exposure and examine associations between selected demographic, professional, and organizational variables and WPV exposure among emergency department healthcare professionals. Cross-sectional studies are suitable for estimating prevalence and identifying associations at a specific time point; however, they cannot establish temporal sequence or causal relationships. Therefore, all findings were interpreted as associations rather than evidence of causation.
Study Period
The study was conducted over a three-month period, from January 2025 to April
Study Setting
The study was conducted in the emergency departments of three tertiary hospitals. These hospitals provide emergency care for large and socio-culturally diverse populations and serve patients with varying levels of clinical acuity. The participating emergency departments operate continuously and are characterized by high patient flow, frequent crowding, time-sensitive clinical decision-making, and direct interaction between healthcare professionals, patients, and family members.
Because perceived overcrowding was a central variable in this study, the setting was described in relation to emergency workload and crowding pressures. The hospitals were tertiary-level emergency care centers within the same public healthcare system. To maintain institutional confidentiality, hospital names were not reported. However, the study included three hospitals to capture variation in emergency department work environments within the same healthcare system. Where available, aggregate contextual information on staffing patterns, patient volume, security arrangements, and shift structure should be reported without identifying the hospitals.
Population and Sampling
The target population consisted of nurses and physicians employed full time in the emergency departments of the participating hospitals. The accessible population included eligible emergency healthcare professionals who were available during the study period and met the inclusion criteria.
The sample size was calculated using the Raosoft® sample size calculator for cross-sectional studies. The calculation was based on a 95% confidence level, a 5% margin of error, and a 50% response distribution. Based on administrative staffing records, the estimated population of full-time nurses and physicians working in the emergency departments of the three participating hospitals was approximately 1,200 healthcare professionals. The minimum required sample size was 291 participants. To compensate for nonresponse and incomplete questionnaires, 360 questionnaires were distributed.
A nonprobability convenience sampling method was used because of rotating shifts, high workload, and the operational demands of emergency departments. Recruitment was conducted across morning, evening, and night shifts to improve inclusion of staff working different schedules and to reduce shift-related recruitment imbalance. However, this approach does not fully eliminate selection bias, and representativeness should be interpreted cautiously.
A total of 313 questionnaires were returned. After excluding 13 questionnaires because they were incomplete or did not meet eligibility requirements, 300 questionnaires were included in the final analysis. The response rate was calculated based on the number of distributed questionnaires, not the total number of all eligible staff in the hospitals; therefore, the response rate was interpreted cautiously.
Eligibility Criteria
Participants were included if they met all of the following criteria: they were registered nurses or physicians; they were employed full time in the emergency department of one of the participating hospitals; they had direct patient contact; they had at least six months of emergency department work experience; and they were available during the study period from January to April 2025.
Participants were excluded if they were students, interns, trainees, administrative staff, non-clinical staff, part-time employees, temporary staff, or on extended leave during the data collection period. Healthcare professionals who participated in the pilot testing phase were also excluded from the final sample to avoid duplication and contamination of responses.
The six-month experience criterion was used to ensure that participants had sufficient exposure to the emergency department work environment and institutional procedures. However, this criterion may have excluded newly employed staff who could have different patterns of WPV exposure and reporting behavior. Similarly, excluding part-time and temporary staff may have limited the ability to capture experiences among healthcare workers with less stable employment arrangements. These issues were acknowledged as limitations.
Instrumentation
Data were collected using a structured, self-administered questionnaire adapted, with permission, from previously used instruments assessing WPV among healthcare professionals in emergency care settings. The questionnaire consisted of three sections. The first section assessed sociodemographic and professional characteristics, including age, gender, profession, marital status, educational level, years of emergency department experience, and exposure to WPV. WPV was operationalized as exposure to any form of workplace-related physical assault, verbal abuse, threats, bullying, harassment, intimidation, or aggressive behavior occurring in the emergency department. Participants were asked whether they had experienced any form of WPV during the study reference period. For this study, WPV exposure referred to incidents experienced during the period covered by the study, from January 2025 to April 2025. WPV exposure was coded as a binary outcome: exposed to WPV or not exposed to WPV.
The first section also assessed formal reporting behavior among participants who reported WPV exposure. Participants were asked whether they formally reported the most recent WPV incident through official hospital reporting channels. Reporting behavior was coded as a binary variable: formally reported or not formally reported. This measure focused on formal reporting only. It did not capture informal reporting to colleagues or supervisors, reasons for nonreporting, satisfaction with institutional response, perceived barriers to reporting, or whether the most recent incident was considered severe enough to require formal reporting.
The second section assessed perceived organizational and environmental risk factors contributing to WPV, including overcrowding, long waiting times, inadequate security, lack of punishment for aggressors, inadequate resources, poor communication, and unrealistic expectations from patients or families. These items were rated on a three-point Likert scale: not important, somewhat important, and very important. Perceived overcrowding was treated as a staff-reported organizational stressor rather than an objective crowding indicator.
The third section assessed participants’ perceptions of the usefulness of preventive strategies, including legislative measures, improved staffing and facilities, availability of diagnostic tests and medications, communication and de-escalation training, security infrastructure, and public and media awareness. These items were rated on a three-point Likert scale: not useful, somewhat useful, and very useful. These responses represented perceived usefulness and were not interpreted as evidence of intervention effectiveness.
Validity and Reliability
The questionnaire underwent content review, translation, pilot testing, and internal consistency assessment for selected domains. Six senior emergency nurses with clinical and academic experience reviewed the questionnaire for clarity, relevance, and alignment with the study objectives. Their comments were used to refine wording and improve the clarity of the items. A formal content validity index was not calculated.
The questionnaire was translated from English into Arabic and Hebrew using a forward–backward translation process to support linguistic and conceptual equivalence. The translated versions were reviewed to ensure that the intended meaning of the items was retained across languages. However, formal measurement equivalence testing across language versions was not conducted.
A pilot study was conducted during the study preparation phase among 25 emergency department healthcare professionals. Participants in the pilot study were excluded from the final analysis. The pilot study assessed readability, clarity, feasibility, and approximate completion time. Participants indicated that the questionnaire was understandable and required approximately 10–15 minutes to complete.
Internal consistency reliability was assessed using Cronbach’s alpha for the perceived risk factor domain and the preventive strategy domain. Cronbach’s alpha values were acceptable for perceived risk factors, α = .81, and preventive strategies, α = .82. Because WPV exposure and formal reporting behavior were measured using single items, internal consistency reliability was not applicable to these outcomes. The study did not conduct construct validity testing, criterion validity testing, test–retest reliability, factor analysis, or formal measurement equivalence testing across Arabic and Hebrew versions. Therefore, the questionnaire was described as a structured adapted instrument that underwent content review, translation, pilot testing, and reliability assessment for selected domains rather than as a fully validated instrument for this specific multilingual emergency department population.
Data Collection Procedure
Data were collected between January 2025 and April 2025. Before data collection, permission was obtained from the participating institutions. Eligible participants were approached during morning, evening, and night shifts to improve coverage of different work schedules. Participants were provided with information about the study purpose, procedures, voluntary nature of participation, confidentiality, and expected time required to complete the questionnaire.
Written informed consent was obtained before questionnaire completion. Questionnaires were completed anonymously in designated private areas within the emergency departments to reduce social desirability bias and workplace pressure. No names, employment numbers, or identifying information were collected. Supervisors were not involved in recruitment, questionnaire completion, or collection, and participants were informed that their decision to participate or decline would not affect their employment status or professional evaluation.
Completed questionnaires were returned in sealed envelopes or placed in a secure collection location. The principal investigator collected the questionnaires regularly and stored them securely. Of the 360 distributed questionnaires, 313 were returned. Thirteen questionnaires were excluded because of substantial missing responses or ineligibility. The final analyzed sample included 300 participants. The handling of incomplete questionnaires was documented before data analysis.
Data Analysis
Data were analyzed using SPSS version 26 after screening for completeness, coding accuracy, outliers, and plausibility. Descriptive statistics summarized demographic variables, WPV exposure, reporting behavior, perceived risk factors, and preventive strategies. Multivariable logistic regression examined factors associated with WPV exposure, reporting adjusted odds ratios, 95% confidence intervals, and p-values. Reporting behavior was analyzed among exposed participants using frequencies and group comparisons. Model fit, multicollinearity, stratified profession analyses, missing data, and significance at p < .05 were assessed.
Ethical Considerations
Ethical approval was obtained from
Written informed consent was obtained from all participants before questionnaire completion. Participation was voluntary, and refusal or withdrawal did not affect employment status, professional evaluation, or relationship with the institution. No personally identifiable information was collected. Questionnaires were coded numerically and stored in a secure location. Electronic data were kept in password-protected files accessible only to the research team. Data were reported in aggregate form to protect participant and institutional confidentiality.
Results
Participant Characteristics
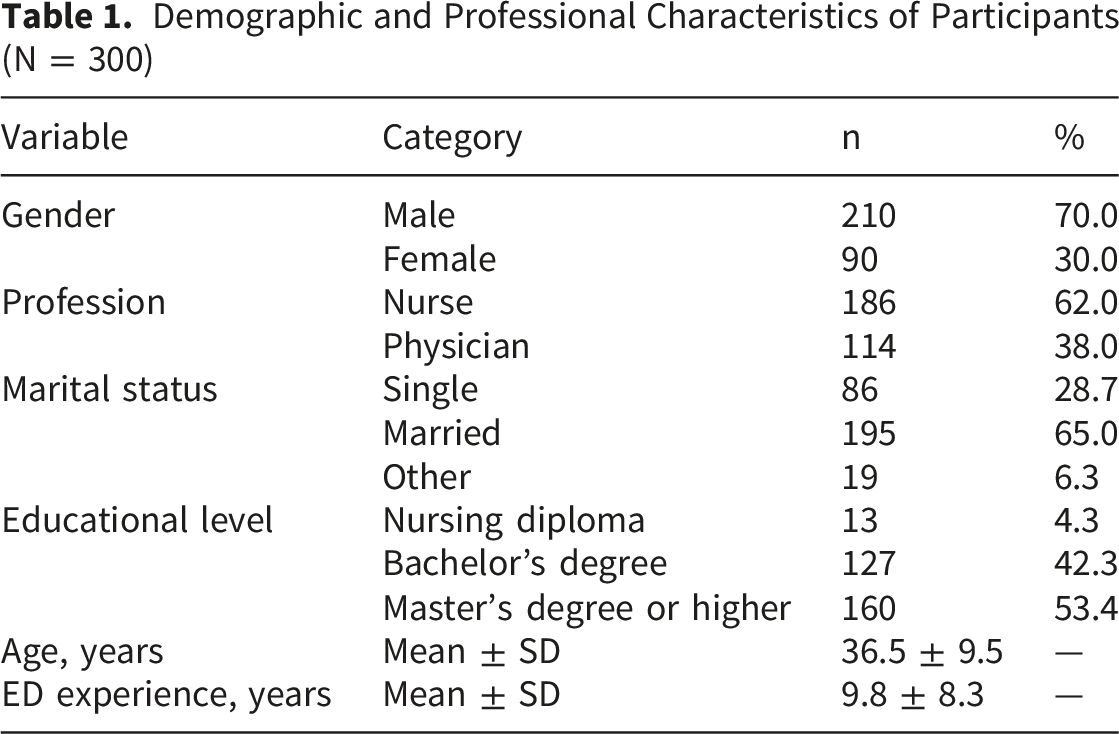
A total of 360 questionnaires were distributed to eligible emergency department healthcare professionals across the three participating tertiary hospitals. Of these, 313 questionnaires were returned, giving a response rate of 86.9% based on distributed questionnaires. Thirteen questionnaires were excluded because they were incomplete or did not meet eligibility criteria. The final analyzed sample included 300 participants.
Demographic and Professional Characteristics of Participants (N = 300)
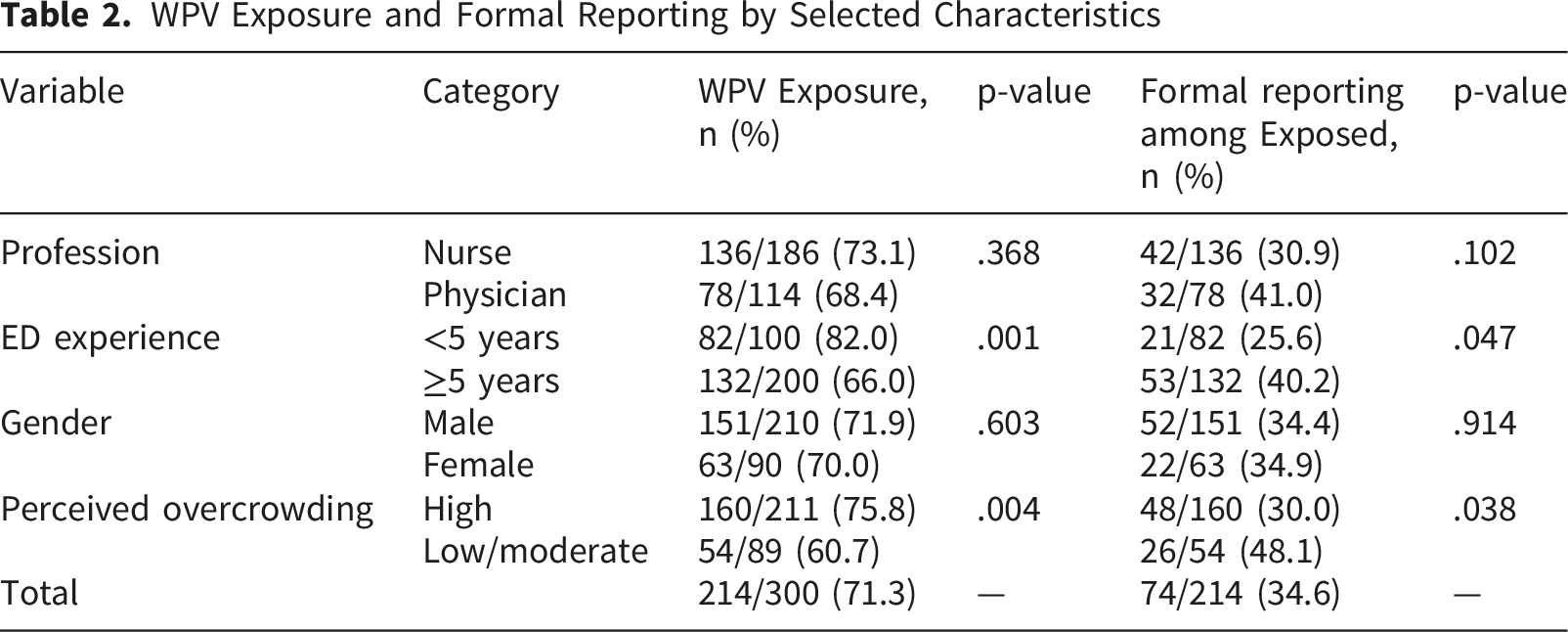
WPV Exposure and Formal Reporting by Selected Characteristics
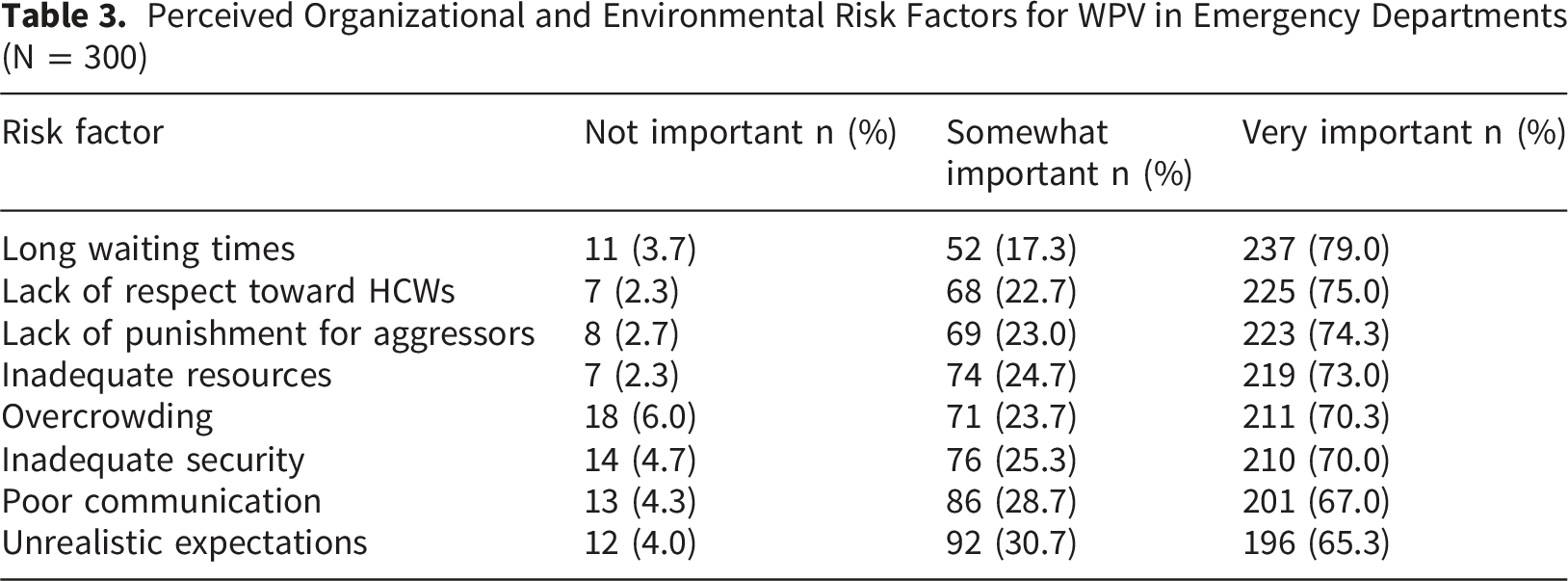
Perceived Organizational and Environmental Risk Factors for WPV in Emergency Departments (N = 300)
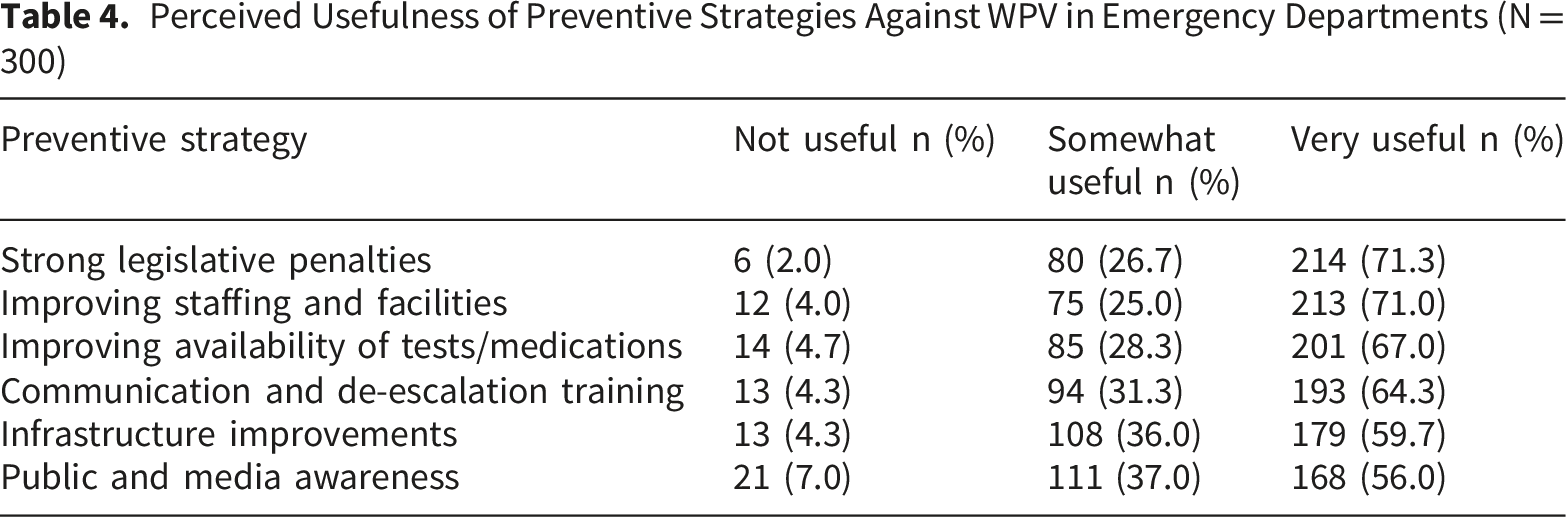
Perceived Usefulness of Preventive Strategies Against WPV in Emergency Departments (N = 300)
Multivariable Logistic Regression Analysis of Factors Associated With WPV Exposure Among Emergency Department Healthcare Professionals (N = 300)
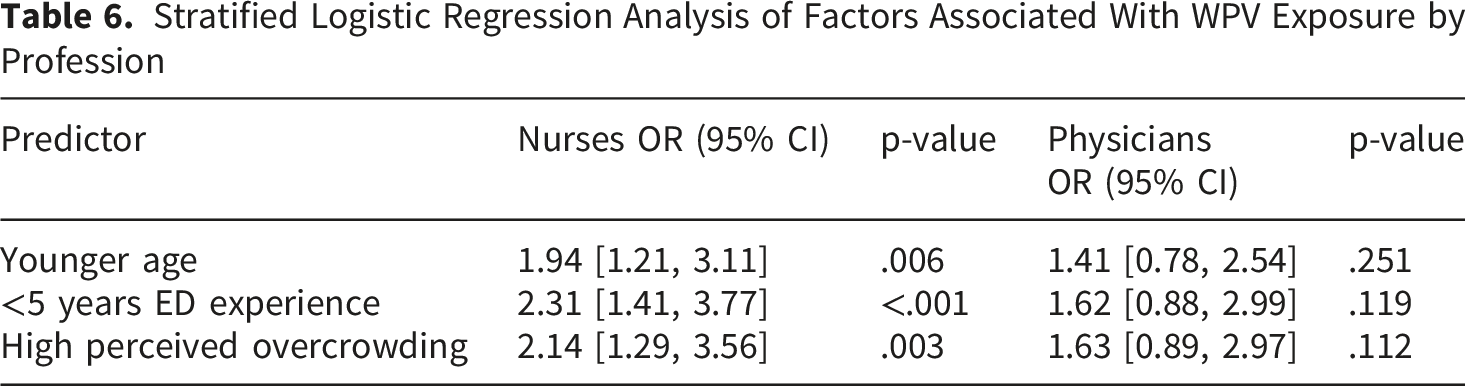
Stratified Logistic Regression Analysis of Factors Associated With WPV Exposure by Profession
Discussion
This study examined WPV exposure and formal reporting behavior among emergency department (ED) healthcare professionals and assessed whether professional experience and perceived overcrowding were associated with WPV exposure. The findings showed that WPV exposure was common, with 71.3% of participants reporting at least one form of violence during the study reference period. Formal reporting was low, as only 34.6% of exposed participants reported the most recent incident through official hospital reporting channels. In the adjusted analysis, shorter ED experience and high perceived overcrowding were significantly associated with WPV exposure, whereas profession and gender were not statistically significant. These findings should be interpreted as associations rather than causal relationships because the study used an analytical cross-sectional design.
The high prevalence of WPV in this study is consistent with recent evidence indicating that EDs remain high-risk clinical environments for violence against healthcare workers. Dopelt et al. (2022), in a cross-sectional study conducted in Israel, reported that WPV against hospital workers remained a significant concern during the COVID-19 pandemic and that ED workers were among the groups with increased exposure. Similarly, Alobaidan et al. (2024), in a study of ED healthcare workers in Saudi Arabia, found that violence in emergency settings remains a growing challenge and includes multiple forms such as verbal abuse, intimidation, and physical aggression. However, comparisons across studies should be made cautiously because prevalence estimates vary according to WPV definitions, recall periods, measurement tools, types of violence included, and professional composition of the sample (Alobaidan et al., 2024; Dopelt et al., 2022).
In the present study, WPV exposure was measured as a combined binary outcome that included different forms of violence, including verbal abuse, threats, bullying, harassment, intimidation, and physical assault. Although this approach provides an overall estimate of exposure, it may obscure differences in severity, frequency, perpetrator type, and clinical context. Recent evidence supports the importance of distinguishing between forms of violence because verbal aggression, threats, and physical assault may have different risk factors and require different preventive responses (Benning et al., 2024). Therefore, the high prevalence observed in this study should be interpreted as evidence of substantial occupational safety concern, but not as an indication that all forms of WPV occurred with the same intensity or consequences.
Shorter ED experience was significantly associated with higher odds of WPV exposure. Staff with less experience may have fewer opportunities to develop familiarity with ED routines, confidence in difficult interactions, and knowledge of institutional safety procedures. Rather, shorter ED experience may represent a marker of professional vulnerability, early role adjustment, or greater exposure to high-contact clinical tasks.
Perceived overcrowding was also significantly associated with WPV exposure. This finding is consistent with recent literature emphasizing crowding as an important organizational stressor in emergency care. Xie et al. (2025), in a literature review on ED crowding and patient-initiated violence against nurses, reported that crowding may contribute to violence through prolonged waiting times, delayed care, frustration, uncertainty, reduced privacy, and increased pressure on staff.
The comparison between nurses and physicians showed that nurses had a slightly higher prevalence of WPV exposure than physicians, but the difference was not statistically significant. Profession was also not independently associated with WPV exposure in the multivariable model. This finding is important because the manuscript should avoid presenting nurses as uniquely affected when the adjusted results do not support a profession-specific association. Although nurses often have continuous bedside contact with patients and families, the present findings suggest that WPV is a broader ED workforce issue affecting both nurses and physicians. The stratified analysis suggested stronger associations among nurses, but these results should be interpreted cautiously because no interaction test was conducted and the physician subgroup may have been underpowered.
Gender was not significantly associated with WPV exposure or formal reporting in this study. This finding suggests that, within this sample, organizational and professional factors may have been more relevant than gender in explaining WPV patterns. However, the absence of statistical significance does not mean that gender is irrelevant. Recent studies indicate that gender-related patterns may vary according to the type of violence examined, the setting, and the professional role of the healthcare worker (Alobaidan et al., 2024; Benning et al., 2024). Because this study used a combined WPV outcome, it may not have captured gender differences in specific forms of violence.
Formal reporting was low in this study, with only 34.6% of exposed participants reporting the most recent incident through official hospital channels. This finding is consistent with recent systematic evidence showing that underreporting remains a persistent challenge in healthcare settings. Spencer et al. (2023) found that nurses’ underreporting of patient- and visitor-perpetrated WPV is shaped by normalization of violence, lack of trust in organizational responses, time pressure, fear of blame, and perceptions that reporting will not lead to meaningful change. Similarly, Xu et al. (2025) reported that barriers to WPV reporting include organizational challenges, cultural and social barriers, and personal or emotional barriers. These findings indicate that underreporting should be understood as a system-level issue rather than only an individual decision.
The present study also found that formal reporting was lower among staff with less than five years of ED experience and among participants who perceived overcrowding as high. This suggests that staff who experience higher exposure may also face greater barriers to reporting. However, reporting behavior was measured using a single item focused only on formal reporting of the most recent incident. The study did not assess informal reporting, reasons for nonreporting, satisfaction with institutional response, reporting barriers, or the severity of the incident. Therefore, the reporting findings should be interpreted cautiously. Future studies should examine reporting behavior as a separate outcome using validated measures that capture both formal and informal reporting pathways.
Participants perceived WPV as strongly linked to organizational and environmental pressures. Long waiting times, lack of respect toward healthcare workers, lack of punishment for aggressors, inadequate resources, overcrowding, inadequate security, poor communication, and unrealistic expectations were frequently rated as very important contributors. This aligns with recent literature indicating that WPV in EDs is influenced by interacting organizational, environmental, and patient-related factors rather than isolated individual behavior (Alobaidan et al., 2024; Xie et al., 2025). Participants also rated several preventive strategies as useful, especially strong legislative penalties, improved staffing and facilities, improved availability of diagnostic tests and medications, communication and de-escalation training, infrastructure improvements, and public awareness. These findings suggest that participants favored multilevel prevention strategies that address institutional, workforce, and policy-level factors. Recent evidence supports the importance of structured organizational responses to WPV, including training, reporting support, and system-level prevention strategies (Benning et al., 2024; Xu et al., 2025).
Several potential confounding variables were not included in the regression model, including staffing level, shift type, patient acuity, ED unit characteristics, security presence, prior WPV training, type of WPV, and hospital-level reporting culture. These factors may influence both WPV exposure and formal reporting behavior. For example, shift type may affect staffing, patient flow, supervision, and security coverage, while different types of WPV may be reported at different rates. In addition, participants were nested within three hospitals, but hospital-level clustering was not adjusted statistically. Therefore, the model’s explanatory power should be interpreted cautiously, even though it was statistically significant.
Overall, this study contributes to the WPV literature by examining exposure, formal reporting behavior, professional experience, and perceived overcrowding within the same ED sample. The findings suggest that WPV prevention should address both workforce vulnerability and organizational pressures. However, the cross-sectional design, convenience sampling, self-reported data, single-item measurement of WPV exposure and reporting, lack of objective crowding indicators, and absence of hospital-level adjustment limit causal interpretation and generalizability. Future research should use longitudinal or multicenter probability-based designs, distinguish between different types and severity of WPV, include objective ED crowding measures, assess reporting barriers in depth, and examine hospital-level factors influencing both WPV exposure and reporting behavior.
Strengths and Weaknesses
This study addresses an important occupational safety issue in emergency departments and includes both nurses and physicians, allowing comparison across professional groups. It also examines WPV exposure together with reporting behavior, professional experience, and perceived overcrowding, which strengthens the practical relevance of the findings.
The cross-sectional design prevents causal interpretation. Convenience sampling may limit representativeness, and WPV exposure was measured as a broad combined outcome. The study also relied on perceived overcrowding rather than objective crowding indicators and did not fully assess WPV type, severity, perpetrator, or detailed barriers to reporting.
Implications
The findings suggest the need for stronger institutional reporting systems, targeted support for less experienced ED staff, and organizational strategies to reduce crowding-related pressures. Emergency departments should consider mentorship, de-escalation training, clear reporting pathways, adequate staffing, security support, and non-punitive responses to reported WPV incidents.
Conclusion
WPV is highly prevalent among emergency healthcare professionals, yet formal reporting remains low. Shorter ED experience and high perceived overcrowding were significantly associated with increased WPV exposure, while profession and gender were not. Participants viewed WPV primarily as a systems-level issue driven by long wait times, inadequate resources, and a lack of consequences for aggressors.
These findings necessitate multi-level interventions. Organizationally, institutions must implement strategies to alleviate overcrowding and address systemic stressors. For the workforce, targeted support—including mentorship and de-escalation training—is essential for less experienced staff. To address underreporting, reporting channels must be streamlined and directly linked to meaningful institutional action to counter the normalization of violence. Broader prevention efforts should integrate legislative penalties, improved staffing and infrastructure, and public awareness.
Future research should utilize longitudinal designs, objective crowding metrics, and distinguish between specific WPV types and severities. Additionally, studies must deeply assess reporting barriers and evaluate the effectiveness of targeted prevention strategies in emergency settings.
Supplemental Material
Supplemental Material - Professional Experience, Perceived Overcrowding, and Workplace Violence Exposure Among Emergency Healthcare Professionals: A Cross-Sectional Study
Supplemental Material for Professional Experience, Perceived Overcrowding, and Workplace Violence Exposure Among Emergency Healthcare Professionals: A Cross-Sectional Study by Ibraheem Abu Ras, Imad Fashafsheh and Nizar B. Said in Sage Open Nursing.
Supplemental Material
Supplemental Material - Professional Experience, Perceived Overcrowding, and Workplace Violence Exposure Among Emergency Healthcare Professionals: A Cross-Sectional Study
Supplemental Material for Professional Experience, Perceived Overcrowding, and Workplace Violence Exposure Among Emergency Healthcare Professionals: A Cross-Sectional Study by Ibraheem Abu Ras, Imad Fashafsheh and Nizar B. Said in Sage Open Nursing.
Footnotes
Acknowledgments
The author thanks the healthcare workers who participated in this study.
Ethical Considerations
Ethical approval for this study was obtained before the commencement of the Arab American University, Jenin, Palestine (Approval No 2023/C/111/N). The research was conducted in line with ethical considerations as outlined in the Declaration of Helsinki. Participants in the research were fully informed of the purposes, processes, risks, and benefits associated with the research activities. Participants signed a written, informed consent process before being selected. The research was conducted on a voluntary basis, with all participants informed of their right to withdraw at any time without being penalized academically or personally. To ensure confidentiality and anonymity, no personally identifiable information was collected. Questionnaires assigned numbers for anonymity and with password-protected computer files not accessible to anyone else aside from the research team, in line with international standards of data protection and research ethics.
Consent to Participate
Written informed consent was secured from all study participants.
Consent for Publication
This manuscript does not contain any individual person’s data in any form (including individual details as name, images, or videos).
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.