
Abstract
Background
Pregnancy-related anxiety is a significant public health concern, yet evidence on its prevalence and associated factors remains limited in Cameroon. This study aimed to estimate the prevalence of pregnancy-related anxiety and identify associated factors among women attending antenatal care service in Cameroon.
Methods
A cross-sectional study was conducted among pregnant women attending their first antenatal care visit for the current pregnancy. A total of 316 participants were enrolled after providing informed consent. Data were collected using Pregnancy-related Anxiety Questionnaire-Revised 2. Bivariate and multivariate logistic regression analyses were performed to identify factors associated with pregnancy-related anxiety.
Results
The prevalence of PRA was 23.4% (95% CI: 19.1% - 28.4%), with common concerns including fear of giving birth (25.0%), concerns about having a child with health problems or disability (22.15%), and concern about one’s appearance (21.20%). Multivariate analysis identified significant factors associated with pregnancy-related anxiety, including younger maternal age (OR = 0.94, 95% CI: 0.89 - 0.98, p= 0.015), being a victim of intimate partner violence (OR = 5.23, 95% CI: 1.15 - 23.79, p= 0.002), being primigravida (OR = 6.18, 95% CI: 1.86 - 44.55, p= 0.026), and having a history of stillbirth (OR = 12.4, 95% CI: 1.21 - 26.7, p= 0.034).
Conclusion
Nearly one in four pregnant women in this study experienced pregnancy-related anxiety. Younger maternal age, intimate partner violence, primigravidity, and a history of stillbirth were significant risk factors. These findings highlight the need for targeted screening and interventions in antenatal care to address pregnancy-related anxiety and improve maternal mental health outcomes.
Introduction
The Pregnancy Related Anxiety (PRA) is commonly conceptualized as an emotional state involving a combination of concerns about one’s pregnancy, baby, self, hospital and healthcare, childbirth, and future parenting (Dryer & Brunton, 2021). PRA has been linked to adverse maternal and fetal outcomes, including preterm birth, low birth weight, and postpartum depression (Grigoriadis et al., 2018). The prevalence of PRA varies globally, influenced by population characteristics and the tools used for measurement. A systematic review by Bayrampour et al. (2016) found that PRA prevalence ranges from 11% to 54%, with higher rates observed in low- and middle-income countries (LMICs), particularly in sub-Saharan Africa (Bayrampour et al., 2016).
In sub-Saharan Africa, the prevalence of PRA remains high due to factors such as limited access to healthcare, high maternal mortality rates, and socioeconomic stressors. Dadi et al. (2020) reported that the pooled prevalence of antenatal anxiety in sub-Saharan Africa was approximately 26.3%, with significant country-to-country variation, ranging from 8.3% to 78.2% (Dadi et al., 2020). Mental health issues during pregnancy in this region are often underdiagnosed and undertreated, primarily due to limited healthcare access, cultural beliefs, stigma, and a lack of awareness and training among healthcare providers (Frayne et al., 2023; Sawyer et al., 2010). This gap is particularly concerning, as untreated PRA can lead to long-term consequences for both mothers and their children, perpetuating cycles of poor health and socioeconomic disadvantage (Biaggi et al., 2016).
Despite the few studies available, there is limited data on PRA in sub-Saharan Africa (World Health Organization, 2023), that emphasizes the need for localized studies to inform policy and practice. This study aims to fill this gap by determining the prevalence of PRA and exploring its associated factors among pregnant women at the largest antenatal care facility in Cameroon. By doing so, it seeks to contribute to the growing body of evidence on maternal mental health in LMICs and advocate for the integration of mental health services into routine antenatal care.
Review of Literature
Pregnancy is a period marked by profound physical, emotional, and social transitions, during which women may experience heightened vulnerability to psychological distress. Pregnancy-related anxiety (PRA), often defined as worry or fear specifically linked to pregnancy, fetal health, childbirth, and maternal role transition (Dryer & Brunton, 2021), has been increasingly recognized as a distinct construct from general anxiety or depression. Evidence indicates that PRA is associated with adverse maternal and fetal outcomes, including preterm birth, low birth weight, and postpartum depression (Grigoriadis et al., 2018). Despite its clinical significance, the prevalence of PRA varies widely, influenced by population characteristics, measurement tools, and contextual factors. A concept analysis by Bayrampour et al. (2016) documented global prevalence estimates ranging from 11% to 54%, with notably higher rates observed in low- and middle-income countries (LMICs) (Bayrampour et al., 2016).
Studies from sub-Saharan Africa consistently report elevated levels of antenatal psychological distress. A systematic review by (Dadi et al., 2020) estimated a pooled antenatal anxiety prevalence of 26.3% across the region, with substantial heterogeneity between countries. This elevated burden reflects broader structural and sociocultural challenges, including limited access to mental health services, high maternal mortality rates, socioeconomic instability, and the influence of cultural norms that discourage the disclosure of emotional difficulties (Frayne et al., 2023; Sawyer et al., 2010). These constraints contribute to the under-recognition and under treatment of perinatal mental health conditions and may compound the severity of PRA in many African contexts.
Multiple determinants of PRA have been identified in the literature. A systematic review by Biaggi et al. (2016) highlighted lack of social support, intimate partner violence, personal or family history of mental illness, unplanned pregnancy, previous pregnancy complications, and high levels of perceived stress as salient predictors of antenatal anxiety. These findings underscore the importance of a socioecological understanding of PRA, which situates psychological risk within individual, interpersonal, and structural domains (Biaggi et al., 2016).
Evidence from Cameroon suggests a similar pattern of psychosocial risk. Although few studies have specifically examined PRA, existing research points to substantial burdens of antenatal psychological morbidity. For instance, Dingana et al. (2022) reported a 31.8% prevalence of depression among pregnant women in rural Cameroon, with gender-based violence and financial stress emerging as significant predictors (Dingana et al., 2022). These findings reflect broader gaps in antenatal mental health support within the country, where services continue to prioritize physical health despite increasing recognition of the role of psychological wellbeing in maternal and newborn outcomes (Bongajum et al., 2021).
Method
Study Design
A hospital-based cross-sectional study was conducted among sampled pregnant women attending their first antenatal visit, regardless of their gestational age at the time of data collection. A structured questionnaire was administered to the individuals who accepted to participate in the study by trained interviewers. The primary outcome was the prevalence of pregnancy-related anxiety, defined as a score at or above the 75th percentile on the PRAQ-R2 total score.
Study Setting and Period
This study was conducted from January to March 2024 at the ANC unit of a faith-based hospital in Yaounde. Based on the national data reporting system (DHIS2), the hospital ANC unit receives the highest number of pregnant women for antenatal visits in the country (averagely 413 monthly). The unit delivers routine ANC, high-risk pregnancy follow-up, counseling, and obstetric triage.
Study Variables
The dependent variable in this study was pregnancy-related anxiety (PRA), that was evaluated using the French version of Pregnancy-related anxiety questionnaire-revised (PRAQ-R2). This version was translated from the English version and the validation done by Reymond et al., on 160 pregnant women showed a good internal consistency (α > .80), and a convergent validity (Reymond et al., 2020). The PRAQ-R2 is a psychometric tool designed to assess anxiety specific to pregnancy. This version, an updated form of the original Pregnancy-Related Anxiety Questionnaire (PRAQ), is made of 10 items divided in 3 categories: fear of childbirth (3 items), baby health concerns (4 items) and body image changes (3 items). The PRAQ-R2 is a commonly used tool for assessing and identifying pregnancy-related anxiety in all pregnant women, regardless of parity (Huizink et al., 2016). Each item of the questionnaire was measured on a 5-point Likert scale: absolutely not relevant, hardly relevant, sometimes relevant, reasonably relevant, and very relevant, coded as “0”, “1”, “2”, “3”, and “4”, respectively. Previous studies have demonstrated that PRAQ-R2 has a satisfactory internal consistency (Cronbach’s alpha >0.8) (Huizink et al., 2016), and that the tool is an accurate indicator of pregnancy-specific anxiety in several settings including low- and middle-income countries (LMICs) (Fraga et al., 2024; Sinesi et al., 2019).
The total score for each participant was the sum of score of each question. The PRA score was then dichotomized based on the 75th percentile, marking a cutoff of 18 for the overall pregnancy-related anxiety and cutoffs of 8.5, 7 and 6 for subscales fear of giving birth, concerns about having a child with health problems or disability and concern about one’s appearance respectively. The use of the 75th percentile as a cutoff is consistent with prior studies employing the PRAQ-R2 in the absence of an established clinical threshold (Fraga et al., 2024; Sinesi et al., 2019). Currently, no universally accepted diagnostic cutoff exists for this instrument. Therefore, this approach allows identification of women with relatively elevated pregnancy-related anxiety within the study population. However, this method is sample-dependent and may influence prevalence estimates.
In accordance with the socioecological model, independent factors were stratified across three levels: individual (e.g., age, education, substance use), interpersonal (e.g., marital status, partner characteristics, reproductive history), and community (e.g., intimate partner violence).
The questionnaire (sociodemographic and PRAQ-R2 items) was pretested among 20 pregnant women attending ANC to assess clarity, cultural appropriateness, and comprehension. Necessary adjustments were made before data collection commenced. Data of the women involved in the pretesting were not included in the analysis.
Sampling and Sample Size
A consecutive sampling strategy was used, whereby all pregnant women presenting for their first antenatal care visit during the study period and meeting eligibility criteria were approached for participation until the minimum sample size was achieved. While consecutive sampling may introduce selection bias, it was the most feasible method to achieve the required sample size within the study period. We selected women at their first antenatal visit to ensure a uniform entry point into the study. In our setting, first visits occur across the first and second trimesters. All eligible women were included regardless of gestational age, and gestational age was adjusted for in the regression models. Women attending ANC with a pregnancy-related complication (including active bleeding, severe pre-eclampsia, placenta previa, suspected ectopic pregnancy, or any condition requiring immediate obstetric intervention) were excluded from the study.
The minimum sample size was calculated using the formula n=Z2P(1−P)/d2. For a precision of 5%, the level of confidence of 95% and assuming the prevalence of PRA in the population is 26.3% (Dadi et al., 2020), the minimum of 298 pregnant women were required for the study.
Data Collection and Analysis
Data were collected through face-to-face interviews conducted by trained research assistants in a private consultation room, using a structured questionnaire. Prior data collection, administrative authorization from the study facility and ethical clearance were obtained.
Collected data were keyed directly in a CSPro-built database and analyzed in Stata/SE 18.0 statistical package. In the descriptive analysis that was first done, categorical variables were presented in frequencies and percentages, while continuous variables were presented as mean and standard deviation.
Bivariate analyses were performed using chi-square tests to compare the association between pregnancy-related anxiety (dependent variable) and independent variables (sociodemographic related variables, psycho-social factors, pregnancy-related factors, previous obstetrics factors and substance use-related factors). All factors in the bivariate analysis with a p-value<0.2 were subsequently entered in the multivariate analysis. All regression models were adjusted for gestational age (categorized by trimester: first, second, and third) to account for potential confounding effects and considered statistically significant when p-values were <0.05.
We assessed the model performance and goodness-of-fit using the Hosmer–Lemeshow test. Additionally, we computed the area under the receiver operating characteristic (ROC) curve (AUC) to determine the model’s discriminatory ability. We assessed multicollinearity using variance inflation factors (VIF). To account for multiple comparisons, the Benjamini-Hochberg procedure was applied, maintaining a false discovery rate of 5%.
Results
During the study period, a total of 758 pregnant women visited the hospital’s antenatal care unit. Of these, 341 (45.0%) were eligible (i.e.,this was their first antenatal care visit for the current pregnancy), and 316 (92.7%) provided their consent to participate in the study and were therefore enrolled.
The mean age of the participants was 27.5 years (SD: 6.2). The mean gestational age of the participants was 15.4 weeks (SD: 5.8). Most participants (61.6%) were in the second trimester, while 89 (27.1%) and 37 (11.3%) were in the first and third trimesters, respectively. A total of 36 (11.5%) participants reported experiencing Intimate Partner Violence (IPV).
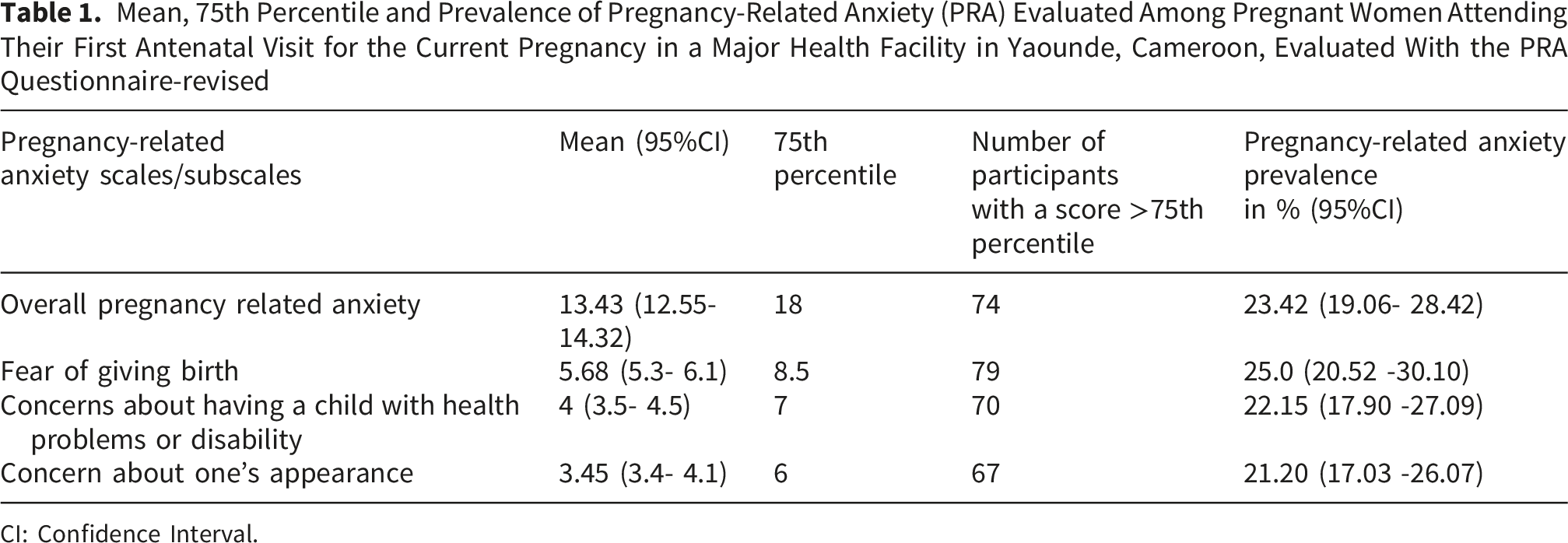
Figure 1 presents the mean scores of the three PRAQ-R2 subscales with their 95% confidence intervals. Fear of giving birth showed the highest mean score (5.68), followed by concerns about having a child with health problems or disability (4.00) and concern about one’s appearance (3.45). The overall mean pregnancy-related anxiety (PRA) score was 13.43 (SD: 8.0), with the 75th percentile set at 18, which was considered the cutoff for estimating PRA prevalence in this study. The overall prevalence of PRA was 23.4% (95%CI: 19.1% - 28.4%) as presented in Table 1. Pregnancy-related anxiety subdomains mean scores and confidence intervals among women attending ANC in Cameroon Mean, 75th Percentile and Prevalence of Pregnancy-Related Anxiety (PRA) Evaluated Among Pregnant Women Attending Their First Antenatal Visit for the Current Pregnancy in a Major Health Facility in Yaounde, Cameroon, Evaluated With the PRA Questionnaire-revised CI: Confidence Interval.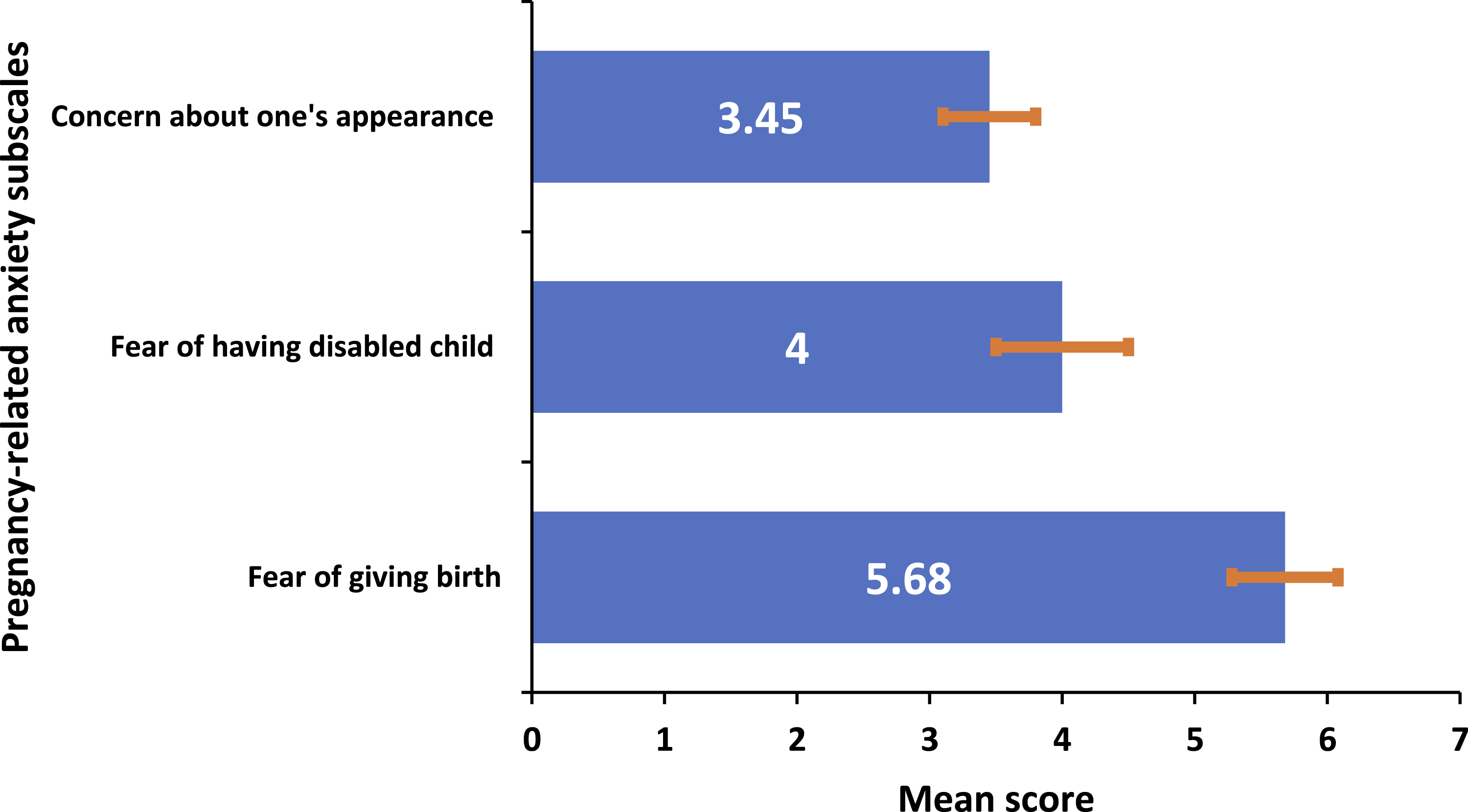
Bivariate and Multivariate Binary Logistic Regression Analysis Showing the Association Between Pregnancy-Related Anxiety and Socio-Demographic, Medical Variables Among Pregnant Women Attending Antenatal Care Initial Visit at a Major Health Facility in Yaounde, Cameroon, 2024 (N = 316)
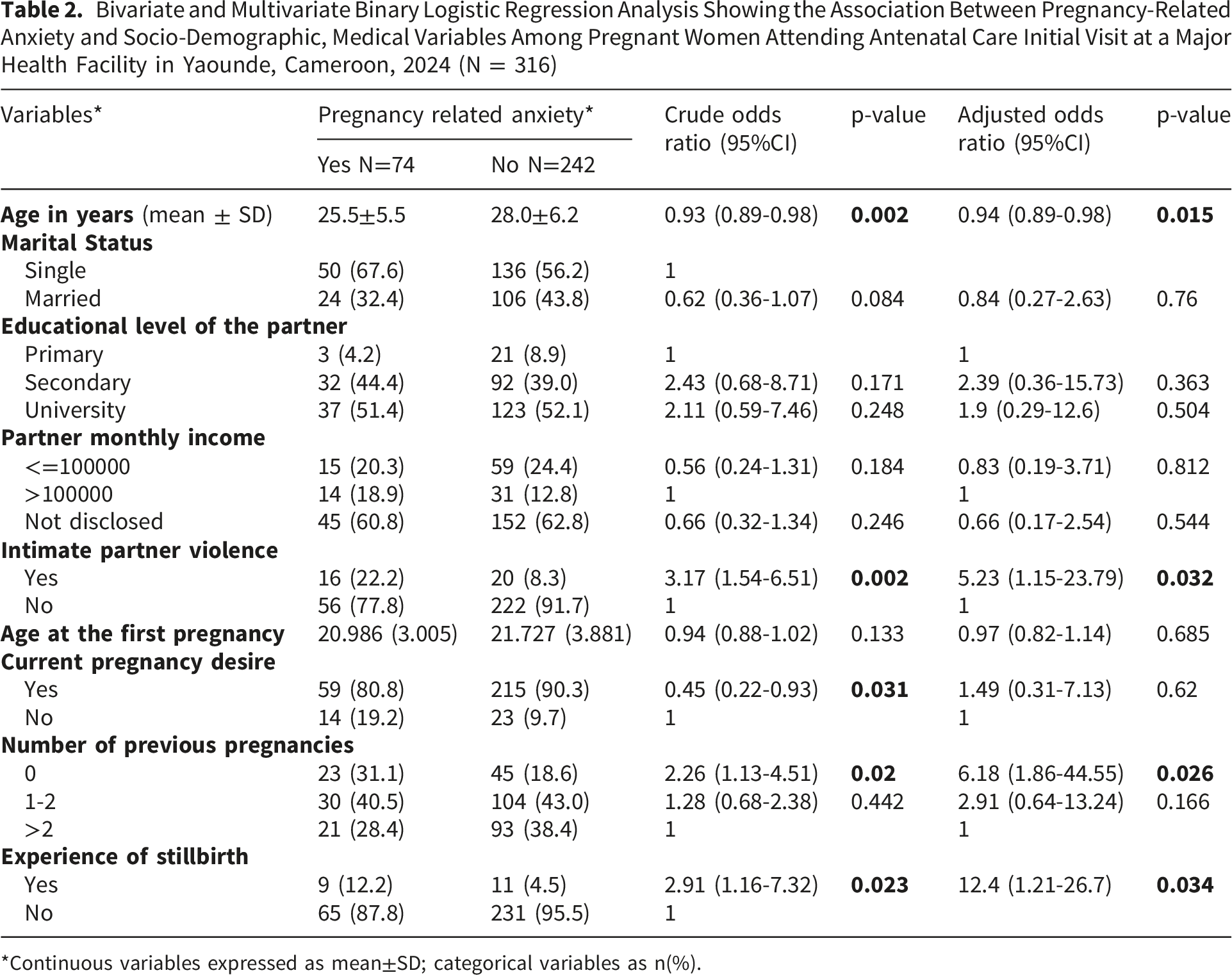
*Continuous variables expressed as mean±SD; categorical variables as n(%).
In the multivariate analysis, the following factors remained significantly associated with PRA: participant’s age (OR = 0.94, 95%CI: 0.89 - 0.98, p= .015), being a victim of intimate partner violence (OR = 5.23, 95%CI: 1.15 - 23.79, p= .002), being primigravida (OR = 6.18, 95%CI: 1.86 - 44.55, p= .026), and having a history of stillbirth (OR = 12.4, 95%CI: 1.21 - 26.7, p= .034). While being a victim of intimate partner violence and history of stillbirth showed a very strong association, the confidence interval was wide, indicating some statistical imprecision likely due to the small number of women in the sample victim of IPV and those in the sample with a stillbirth history. Application of the Benjamini-Hochberg procedure to account for multiple comparisons did not change the statistical significance of the variables retained in the final multivariate model. The ROC curve (Figure 2) demonstrated that the logistic regression model had good discriminatory ability, with an area under the curve (AUC) of 0.77. Receiver Operating Characteristic (ROC) Curve for the Logistic Regression Model Predicting Pregnancy-Related Anxiety in women attending antenatal care in Yaounde, Cameroon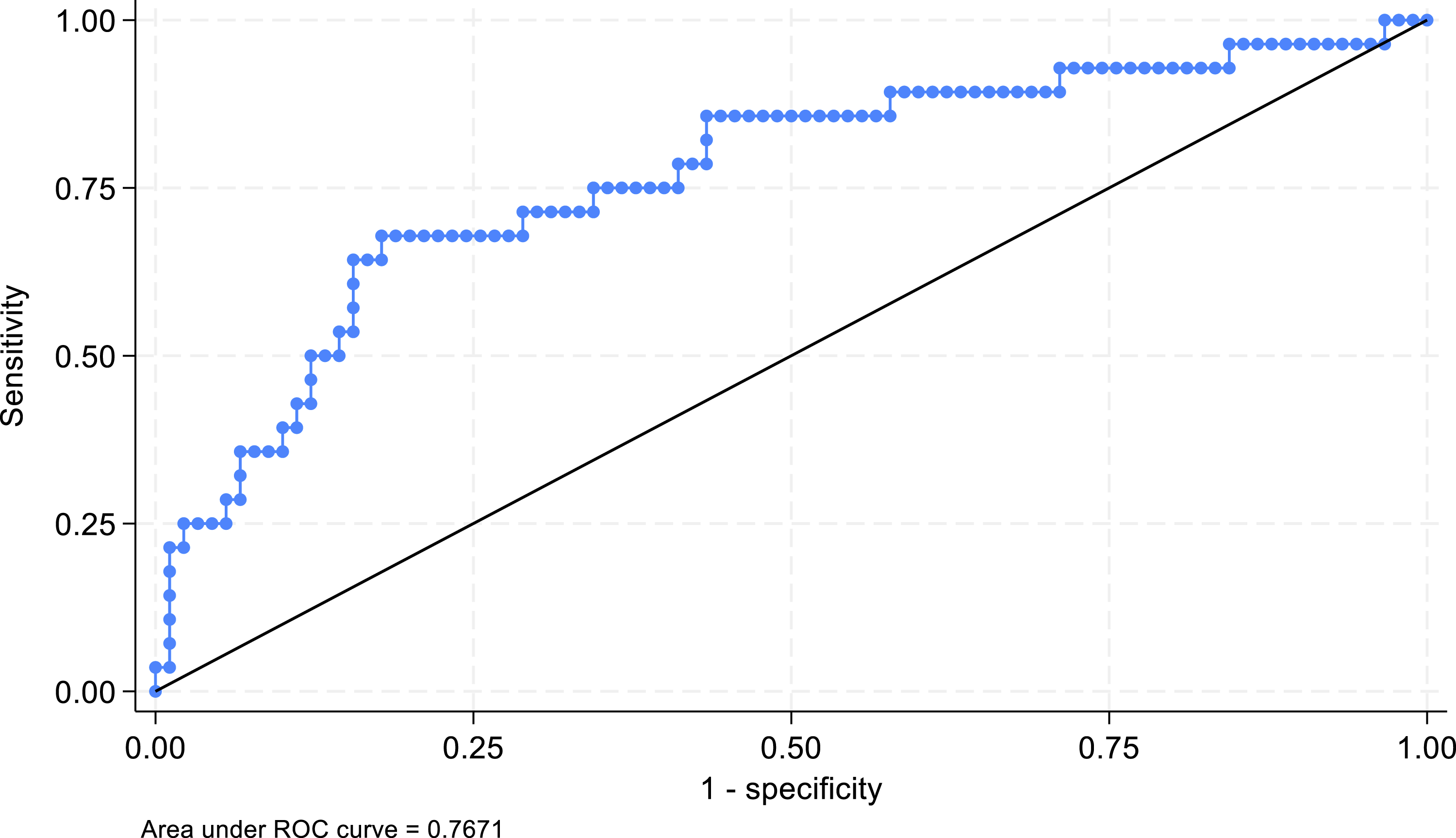
Discussion
The findings revealed that PRA was prevalent among 23.4% of the participants, and that younger maternal age, first-time pregnancy (primigravida status), history of stillbirth, and intimate partner violence were associated with PRA. These findings are consistent with what was reported in previous studies worldwide. A meta-analysis conducted by Dennis et al. (2017) showed that the prevalence of PRA ranges from 17% to 42% (Dennis et al., 2017), and a systematic review by Biaggi et al. (2016) highlighted young age, primiparity, history of domestic violence, unplanned or unwanted pregnancy, past or present pregnancy complications, and pregnancy loss as factors associated with PRA (Biaggi et al., 2016).
The large variability in the prevalence of PRA observed in the literature can be explained by several parameters, including, but not limited to, study settings, characteristics of the studied population, gestational age at the time of the interview, the tool used for estimation, and the data collection method (self-reported vs. clinical diagnosis). A meta-analysis conducted by Dennis et al. (2017) showed a significantly higher PRA prevalence in low-to middle-income countries (34.4%, 95% CI 25.0–43.8) compared to high-income countries (19.4%, 95% CI 17.0–21.8) (Dennis et al., 2017). The relatively higher prevalence observed in our study, as well as in other low-income countries, may be partially explained by socioeconomic and cultural contexts, where limited access to healthcare, financial constraints, and poor pregnancy outcomes (such as high maternal and infant mortality rates) may exacerbate anxiety among pregnant women. Additionally, the lack of mental health integration into antenatal care in resource-limited settings may contribute to the underdiagnosis and undertreatment of PRA, leading to higher reported prevalence when assessed systematically. Considering that the high prevalence of PRA has been associated with maternal and child health (Dadi et al., 2025; Wei et al., 2023), actions need to be taken to reduce PRA at every stage of the pregnancy.
The use of the Pregnancy-Related Anxiety Questionnaire-Revised 2 (PRAQ-R2) in this study is a strength, as it is a validated tool specifically designed to assess PRA regardless of parity (Huizink et al., 2016) and has been validated and used on several settings, including low- or middle-income countries (Fraga et al., 2024; Hadfield et al., 2022). However, the variability in PRA prevalence across studies may be partly attributed to differences in assessment tools and cutoff points. For instance, studies using other tools, such as the State-Trait Anxiety Inventory (STAI), often report lower prevalence rates due to differences in the constructs measured (Dennis et al., 2017). The PRAQ-R2 focuses specifically on fears and worries related to pregnancy, childbirth, and fetal health, which may capture a broader spectrum of anxiety symptoms compared to general anxiety tools. This specificity likely contributed to the relatively higher prevalence observed in our study. The high prevalence of PRA and its documented adverse effects on pregnancy outcomes (Grigoriadis et al., 2018) in resource-limited settings suggest the need to identify and address factors associated with anxiety during pregnancy.
Women with a prior stillbirth had approximately 12-fold higher odds of elevated anxiety. Although this estimate is large, it is statistically imprecise and should be interpreted cautiously. The finding is consistent with evidence showing that adverse pregnancy outcomes increase the risk of anxiety in subsequent pregnancies (Donegan et al., 2023). The loss of a baby can intensify fears about recurrence and evoke guilt or self-blame. In sub-Saharan Africa, where stillbirth rates remain high, the psychological burden may be compounded by cultural interpretations and stigma related to pregnancy loss (Hug et al., 2021). These findings underscore the importance of compassionate, trauma-informed antenatal care and accessible psychological support for women with prior loss.
Primigravidae had 6.18 times higher odds of PRA compared with multigravidae. First-time mothers often report greater uncertainty regarding pregnancy, childbirth, and parenting, which may heighten anxiety (Huizink et al., 2016). In resource-limited settings such as Cameroon, limited access to structured antenatal education may further amplify fears of complications. Tailored antenatal counseling and childbirth education for first-time mothers may therefore help reduce anxiety and strengthen maternal confidence.
Intimate partner violence (IPV) was also strongly associated with PRA. Women reporting IPV had 5.23 times higher odds of anxiety, though this relatively large estimate is imprecise and warrants cautious interpretation. Over one-third of affected women had not disclosed their experience, underscoring the hidden nature of violence. This association aligns with evidence linking IPV to adverse antenatal mental health outcomes, including anxiety and depression (Biaggi et al., 2016). In sub-Saharan Africa, IPV remains highly prevalent among reproductive-age women (Tadesse et al., 2025). Routine screening, confidential disclosure pathways, and referral mechanisms within antenatal care are critical to mitigate psychological harm.
Younger maternal age was associated with higher PRA, consistent with prior evidence indicating increased vulnerability to anxiety among younger pregnant women (Biaggi et al., 2016). Contributing factors may include limited social and economic resources (Bajaria et al., 2025), stigma related to early pregnancy, and constrained access to youth-friendly mental health services (Gelaye et al., 2016; Mutahi et al., 2022). Targeted, age-appropriate antenatal education and peer support interventions may help address this vulnerability.
Cultural factors in Cameroon may also contribute to the elevated levels of pregnancy-related anxiety observed in this study. Pregnancy is widely regarded as a central marker of womanhood, and strong societal expectations for women to carry a healthy pregnancy to term can intensify fears related to childbirth and fetal wellbeing. Limited culturally acceptable avenues for emotional disclosure, together with norms that prioritize resilience over vulnerability, may also reduce opportunities for women to seek support. These cultural pressures, combined with existing socioeconomic and health system challenges, likely interact to compound pregnancy-related fears and may contribute to the high prevalence of PRA in this setting.
Strengths and Limitations
This study has several strengths. The use of the Pregnancy-Related Anxiety Questionnaire-Revised 2 (PRAQ-R2), a validated tool specifically designed to measure pregnancy-related anxiety, allowed for focused assessment of pregnancy-specific concerns. Recruiting women at their first antenatal care visit provided a standardized point of assessment early in pregnancy and reduced variability related to gestational timing. In addition, the study contributes context-specific evidence from a high-volume antenatal care setting in Cameroon, addressing a recognized gap in maternal mental health research in low-resource settings.
Some limitations should be noted. The cross-sectional design limits causal inference. As a single-center, facility-based study, the findings may not be generalizable beyond similar antenatal care settings. The use of consecutive sampling may have introduced selection bias. Some confidence intervals were wide, reflecting small subgroup sizes for certain exposures, such as intimate partner violence and history of stillbirth. These findings should therefore be interpreted cautiously and warrant confirmation in larger multicenter studies with greater statistical power.
Implications for Clinical Practice
The findings of this study highlight important implications for antenatal care practice in Cameroon, particularly for nurses and midwives who serve as the primary point of contact for pregnant women. Given the observed prevalence of pregnancy-related anxiety and its associated factors, routine screening for pregnancy-related anxiety during antenatal visits is warranted. Nurses and midwives are well positioned to administer brief, validated tools such as the PRAQ-R2, provide empathetic communication, and identify women who may benefit from additional psychosocial support. The strong association between pregnancy-related anxiety and intimate partner violence further underscores the need for nurses to incorporate confidential, trauma-informed IPV assessment into routine antenatal care layering, alongside clear referral pathways to psychosocial and protective services. Strengthening nursing capacity through targeted training in perinatal mental health, basic counseling skills, and referral processes may facilitate early identification and management of anxiety, particularly in resource-limited settings where specialist mental health services are scarce. Integrating these practices into routine antenatal care may contribute to improved maternal wellbeing and more comprehensive, person-centered maternity care.
Conclusion
This study found a high prevalence of PRA and identified younger age, primigravidity, IPV, and prior stillbirth as key associated factors. These findings underscore the need to integrate routine mental health screening and tailored support into antenatal care in Cameroon.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.