
Abstract
Background
Emergency nurses in Palestinian hospitals operate under chronic stress related to political instability, resource constraints, and high trauma exposure. These conditions may affect both psychological resilience and Advanced Life Support (ALS) competency, yet the evidence base remains unclear. This scoping review sought to map the available body of literature about psychological resilience and ALS competency among emergency nurses in Palestine, identify gaps in research, and determine the relationship between psychological resilience and ALS competency, which is the core focus of this review.
Methods
Following PRISMA-ScR guidelines and JBI scoping review methodology, a comprehensive search of seven electronic databases and grey literature was conducted for studies published between January 2000 and January 2026. Two reviewers independently screened studies and extracted data using a standardized, pilot-tested charting form. Findings were synthesized descriptively using narrative synthesis organized around the review objectives.
Results
From 1,292 records identified, 18 studies met inclusion criteria. Most studies were descriptive or correlational (94.4%). Burnout prevalence among emergency nurses ranged from 64% to 72.9%, and substantial gaps in ALS/BLS knowledge were reported, including low accuracy in resuscitation sequence identification (26.6%). Only one intervention study was identified, evaluating simulation-based BLS training. No studies were found that assessed resilience-based or comprehensive programs which address psychological wellbeing and clinical competency issues. There were no studies that specifically analyzed the connection between psychological resilience and competency in ALS.
Conclusion
The existing literature on Palestinian emergency nurses is dominated by descriptive studies, with a marked absence of intervention research. Despite documented psychological distress and clinical competency gaps, no studies have evaluated psychological resilience-focused or integrated interventions. This review highlights critical evidence gaps and provides a foundation for future intervention-oriented research.
Keywords
Introduction
The Context of Emergency Nursing in Palestine
The Palestinian healthcare system faces a challenging political environment, transforming emergency nursing into a daily challenge (WHO, 2023). Amidst ongoing conflict, constant uncertainty, and limited resources, hospital emergency departments bear a significant workload, with nurses experiencing stress that influences their professional practice and societal expectations (Giacaman et al., 2009).
Political instability manifests in multiple dimensions, creating unpredictable working conditions where emergency nurses must adapt rapidly to fluctuating patient volumes, varying acuity levels, and disrupted supply chains (Truppa et al., 2024). Movement restrictions further impede coherent care delivery and professional development, compounding the operational challenges nurses face.
Resource limitations represent a pervasive challenge, with chronic scarcity of medical supplies, equipment, and medications forcing nurses to adapt their practice (Mataria et al., 2009). Infrastructure deficits, including unreliable electricity and water shortages, further complicate emergency care delivery.
The high workload burden reflects both the intensity of trauma cases and staffing shortages. Emergency nurses routinely manage high-acuity conflict-related injuries alongside typical medical emergencies (Barbisch & Koenig, 2006). Trauma exposure is particularly significant: regular exposure to severe injury and suffering creates conditions conducive to secondary traumatic stress, compassion fatigue, and burnout, while limited access to mental health services elevates the risk of psychological distress (Hamdan & Hamra, 2017). Within this environment, chronic stressors function as a dual burden: they deplete the psychological resilience of emergency nurses while simultaneously erecting barriers to the acquisition, practice, and retention of life-saving Advanced Life Support competencies.
The Imperative of Psychological Resilience
Psychological resilience, defined as the capacity to preserve psychological well-being and adapt positively amid adversity, is crucial for professional longevity and therapeutic efficacy in high-stress contexts (Fletcher & Sarkar, 2013). In Palestinian emergency nursing, psychological resilience involves both individual psychological resources and organizational support mechanisms (Hammad & Tribe, 2021).
Chronic stress exposure severely impairs well-being and organizational effectiveness. The association between chronic stress and burnout syndrome is well-documented, with emergency nursing regarded as particularly high-risk (Adriaenssens et al., 2015). Burnout, characterized by emotional exhaustion, depersonalization, and diminished personal accomplishment, undermines both nurse well-being and patient care quality (Maslach & Leiter, 2016). In resource-limited settings such as Palestinian hospitals, the departure of experienced staff further threatens consistent care quality (Hamdan & Hamra, 2017).
The Criticality of Advanced Life Support Competency
Advanced Life Support competency is an essential prerequisite for emergency nursing practice, incorporating the requisite knowledge, skills, and clinical judgment to deliver life-saving measures (Perkins et al., 2021). Maintaining high ALS competency is especially critical in Palestinian emergency departments due to the high volume of severe trauma cases and limited specialist medical care (Aldabbour et al., 2025). ALS expertise encompasses domains such as cardiac rhythm detection, advanced airway management, pharmacological treatment, and resuscitation team coordination (Soar et al., 2021). Due to the complexity of ALS protocols, continuous practice and education are necessary for maintaining competency after initial training (Abu-Rmeileh et al., 2012).
Emergency nurses confident in their clinical skills handle high-acuity situations more effectively, make rapid clinical decisions under duress, and remain composed under pressure (Hunziker et al., 2011). Conversely, perceived deficiencies in clinical skill can lead to elevated stress and decreased job satisfaction (Chesak et al., 2019), underscoring the inextricable link between competency support and mitigation of workplace stressors.
The Potential Interplay: Bridging Resilience and Competency
The connection between psychological resilience and clinical competency represents an emerging area of interest, with growing acknowledgment that these domains may be interconnected (Arrogante & Aparicio-Zaldivar, 2017). We propose a conceptual framework for this context, positing a dynamic, bidirectional relationship between nurse psychological resilience and ALS competency, moderated by the chronic contextual stressors of the Palestinian setting. It is important to emphasize, however, that this framework is theoretical in nature; the available evidence does not yet provide direct empirical support for this proposed bidirectional relationship, and this review was conducted, in part, to map what evidence does and does not exist in this area.
Theoretical models suggest psychological well-being may affect clinical performance through decision-making, attentiveness, and professional self-confidence (Wetzel et al., 2006). Cognitive load theory provides one framework for understanding this connection, positing that high psychological discomfort consumes cognitive resources otherwise available for clinical decision-making and skill execution (Sweller, 1988). Self-efficacy theory offers another lens, suggesting that confidence in one’s capacity to perform effectively influences both motivation and persistence in the face of difficulty (Bandura, 1997). Higher psychological resilience may support emergency nurses’ professional self-efficacy, potentially facilitating better performance under pressure, though this relationship remains empirically unexamined in this population (Malak et al., 2025). Conversely, nurses who feel well-equipped to manage emergency circumstances may experience lower anxiety and higher job satisfaction, which may in turn enhance psychological resilience (Yu et al., 2019). While theoretically plausible, this reciprocal relationship has not been empirically investigated in this population, and the present review was designed to determine the current state of such evidence.
Rationale and Objectives
Rationale
A scoping review represents the most appropriate methodology to map the broad, heterogeneous, and emerging evidence at the intersection of psychological resilience and clinical competency in Palestinian emergency nursing (Arksey & O'Malley, 2005). Unlike a systematic review, which is designed to answer a focused clinical question about effectiveness using a homogeneous evidence base, a scoping review is suited to mapping the extent and nature of an emerging field, clarifying key concepts, and identifying research gaps across heterogeneous study designs (Munn et al., 2018). The present question, mapping what is known about psychological resilience and ALS competency in a specific conflict-affected context, is exploratory rather than evaluative, making a scoping approach methodologically appropriate. Furthermore, given this theoretical yet empirically underexamined interplay, a structured mapping of the available evidence is warranted before more focused synthesis can be undertaken.
Objectives
The objectives of this scoping review are to: • Systematically identify and map available literature on psychological resilience and ALS competency among emergency nurses in Palestinian hospitals. • Catalog and describe characteristics of any identified resilience-building or competency-training interventions. • Examine reported relationships, whether explicit or implied, between psychological well-being and clinical performance in this population. • Identify key characteristics, trends, and evidence gaps in existing literature, with specific attention to studies linking interventions across both domains. • Provide actionable recommendations for future clinical practice, policy development, and primary research.
Review Question
The primary research question guiding this scoping review is: What is the nature and extent of available literature regarding resilience-building interventions and their potential association with Advanced Life Support competency among emergency nurses in Palestinian hospitals?
Methods
Protocol and Registration
This scoping review protocol was registered with the Open Science Framework (OSF) (https://osf.io/ktahd/overview?view_only=64797d2dd59743b0b160b026a8e26496) to ensure transparency and methodological rigor (Nosek et al., 2018). The protocol, including the a priori search strategy, eligibility criteria, data extraction framework, disagreement resolution procedures, and calibration exercises, was established prior to study selection. As PROSPERO does not accept scoping review protocols, OSF registration is consistent with current JBI guidance (Peters et al., 2020).
Review Question and PCC Framework
Population, Concept, Context (PCC) Framework

Eligibility Criteria
Inclusion Criteria
Studies were included if they: (1) involved emergency nurses in Palestinian hospitals; (2) addressed psychological resilience (including well-being, stress, and burnout as proxy constructs) and/or ALS/BLS competency (e.g., knowledge, skills); (3) were set in Palestinian hospitals or emergency departments; (4) used any study design (quantitative, qualitative, mixed-methods, reviews, or grey literature); (5) were published in English or Arabic; and (6) were published between January 2000 and January 2026.
The 2000–2026 timeframe was selected to capture the modern evidence base while reflecting the post-Oslo Accords period, during which the current structure of the Palestinian healthcare system emerged. Studies predating 2000 were considered insufficiently reflective of the contemporary health system context.
Resilience was operationalized broadly to include direct measures (e.g., Connor-Davidson Resilience Scale), as well as related psychological constructs such as burnout, job stress, compassion fatigue, and coping strategies, which the literature treats as proxies for or inversely related to psychological resilience. ALS/BLS competency was operationalized to include studies addressing knowledge, skills, attitudes, or performance related to resuscitation and emergency life support procedures.
Exclusion Criteria
Studies were excluded if they: (1) did not involve Palestinian healthcare settings or nursing populations; (2) focused exclusively on non-emergency nursing specialties without extractable emergency nurse data; (3) examined student nurses or nursing education without a direct connection to practicing emergency nurses; (4) were published before January 2000; or (5) were written in languages other than English or Arabic.
Note: An initial protocol draft included Hebrew-language studies in the eligibility criteria. Following review, this criterion was removed because no Hebrew-language studies meeting the remaining eligibility criteria were identified during the search, and the reviewers did not have the Hebrew-language proficiency required to conduct independent, systematic appraisal of such sources. Retaining this criterion without the capacity to evaluate relevant sources would have undermined methodological transparency. The final eligibility criteria therefore specify English and Arabic only.
Search Strategy
A comprehensive search strategy was developed in consultation with a research librarian and implemented across seven electronic databases (MEDLINE/PubMed, CINAHL, PsycINFO, Embase, Cochrane Library, Web of Science, and IMEMR) and grey literature sources (Palestinian Ministry of Health reports, WHO documents, institutional repositories, and theses) between November 10, 2025 and January 31, 2026. Search terms combined Boolean operators (AND/OR) across three concept groups: (1) Population (e.g., “emergency nurse*,” “Palestinian nurse*,” “Gaza nurse*”); (2) Concept (e.g., “resilience,” “burnout,” “ALS,” “Advanced Life Support,” “Basic Life Support,” “competency,” “well-being”); and (3) Context (e.g., “Palestine,” “Gaza,” “West Bank,” “occupied Palestinian territory”).
An example search string used in MEDLINE/PubMed was: (“emergency nurse*” OR “emergency department nurse*” OR “Palestinian nurse*”) AND (“resilience” OR “burnout” OR “psychological well-being” OR “stress” OR “compassion fatigue”) AND (“Palestine” OR “Gaza” OR “West Bank” OR “occupied Palestinian territory”). Analogous search strings adapted to each database’s controlled vocabulary and syntax are provided in full in the Supplementary File (Appendix A).
Grey literature was searched systematically using the following approach: (1) the WHO EMRO regional publications database was searched using terms “Palestine” AND “nurses” AND “emergency”; (2) the Palestinian Ministry of Health website and document repository were reviewed for relevant reports; (3) two relevant institutional repositories (Arab American University and An-Najah National University) were searched by title keyword; and (4) ProQuest Dissertations and Theses was searched for unpublished theses. All grey literature sources and results are documented in Supplementary File (Appendix A).
(See Supplementary File, Appendix A for complete search strategies for all databases.)
Study Selection Process
A systematic two-stage screening approach was conducted by two independent reviewers using Rayyan software (Ouzzani et al., 2016). First, title/abstract screening was performed by both reviewers independently, followed by full-text review of all records marked as included or uncertain. Prior to the formal screening stage, both reviewers independently screened a calibration set of 20 records and discussed decisions to ensure shared understanding of the eligibility criteria. Inclusion and exclusion decisions were operationalized using a standardized decision guide developed during the calibration phase.
Disagreements at both the title/abstract and full-text stages were resolved through structured discussion between the two reviewers. In cases where consensus could not be reached, a third independent reviewer adjudicated the decision. Inter-rater reliability was formally assessed using Cohen’s kappa at each stage: kappa = 0.837 at the pilot calibration stage, kappa = 0.882 at the title/abstract screening stage, and kappa = 0.877 at the full-text review stage. The value of kappa = 0.81 reported in prior drafts represented a summary approximation; the stage-specific values in Supplementary File (Appendix D) are the definitive reported values, all indicating almost perfect agreement (See Supplementary File, Appendix D for full reliability results.).
Data Extraction
Data extraction was performed using a standardized, pilot-tested charting form developed iteratively by the review team. One reviewer extracted data from all included studies, with a second reviewer independently verifying 20% of studies (n = 4, randomly selected) for accuracy. Discrepancies identified during verification were resolved by consensus between the two reviewers. This partial verification approach is consistent with scoping review practice; however, as a limitation, this means that extraction errors in the unverified 80% of studies cannot be fully excluded, and this should be considered when interpreting findings.
The charting form captured: study identification (author, year, country), study design, sample characteristics (size, setting, population), concept focus (resilience/well-being, ALS/BLS competency, or both), key findings, and methodological quality observations. “Quality notes” refers to the reviewer’s documented observations on methodological features of each included study, such as study design, sampling approach, response rate, and risk of bias indicators, recorded descriptively in the charting form. These observations were used to contextualize the interpretation of findings in the narrative synthesis and to inform the strengths and limitations section. No formal critical appraisal tool was applied (see Section 2.7 for justification). (See Supplementary File, Appendix C for the complete data extraction form and examples.).
Data Analysis and Synthesis
Following established scoping review methodology (Peters et al., 2020), we employed descriptive analysis and narrative synthesis rather than statistical meta-analysis. The decision not to conduct a formal critical appraisal of included studies is consistent with JBI guidance for scoping reviews, which explicitly states that critical appraisal is not mandatory, as the purpose of a scoping review is to map the evidence base rather than to assess the effectiveness or quality of included studies (Munn et al., 2018; Peters et al., 2020). Given the predominantly descriptive and heterogeneous nature of the included studies, formal quality appraisal would not have altered the synthesis approach or the identification of evidence gaps. Methodological observations relevant to interpretation were captured descriptively in the charting form (see “quality notes” above).
Descriptive Analysis
Summarized study characteristics including publication trends, study design, sample size, geographic distribution, and conceptual focus. These descriptive summaries were used to characterize the overall research landscape, identify patterns across studies, and contextualize the evidence gaps informing the narrative synthesis.
Narrative Synthesis
Organized around the five review objectives to describe the evidence base, catalog any interventions, examine relationships between domains, and synthesize gaps. Studies were grouped by conceptual focus (psychological resilience/burnout; ALS/BLS competency; both domains; contextual/descriptive) and then compared within each group in terms of design, population, setting, measurement tools, and findings. Themes and patterns were identified inductively across grouped studies, and interpretations were grounded explicitly in the data rather than in theoretical assumptions. Where discrepant findings were identified across studies, these were highlighted and discussed in relation to methodological differences.
Data Presentation
Combined summary tables, narrative descriptions, and visual displays (PRISMA-ScR flow diagram). These integrated presentation formats were selected to maximize clarity and accessibility, enabling readers to interpret findings across quantitative, qualitative, and mixed-methods studies within a unified framework.
Results
Search Results
The comprehensive search yielded 1,292 records. After removing 312 duplicates, 980 unique records underwent title/abstract screening. Of these, 842 were excluded, leaving 138 for full-text assessment. After full-text review, 18 studies met the inclusion criteria (See Figure 1). PRISMA-ScR flow diagram illustrating the study selection process, from initial identification of records (n = 1,292) to final inclusion (n = 18)
Characteristics of Included Studies
Summary of Key Characteristics of Included Studies (n = 18)
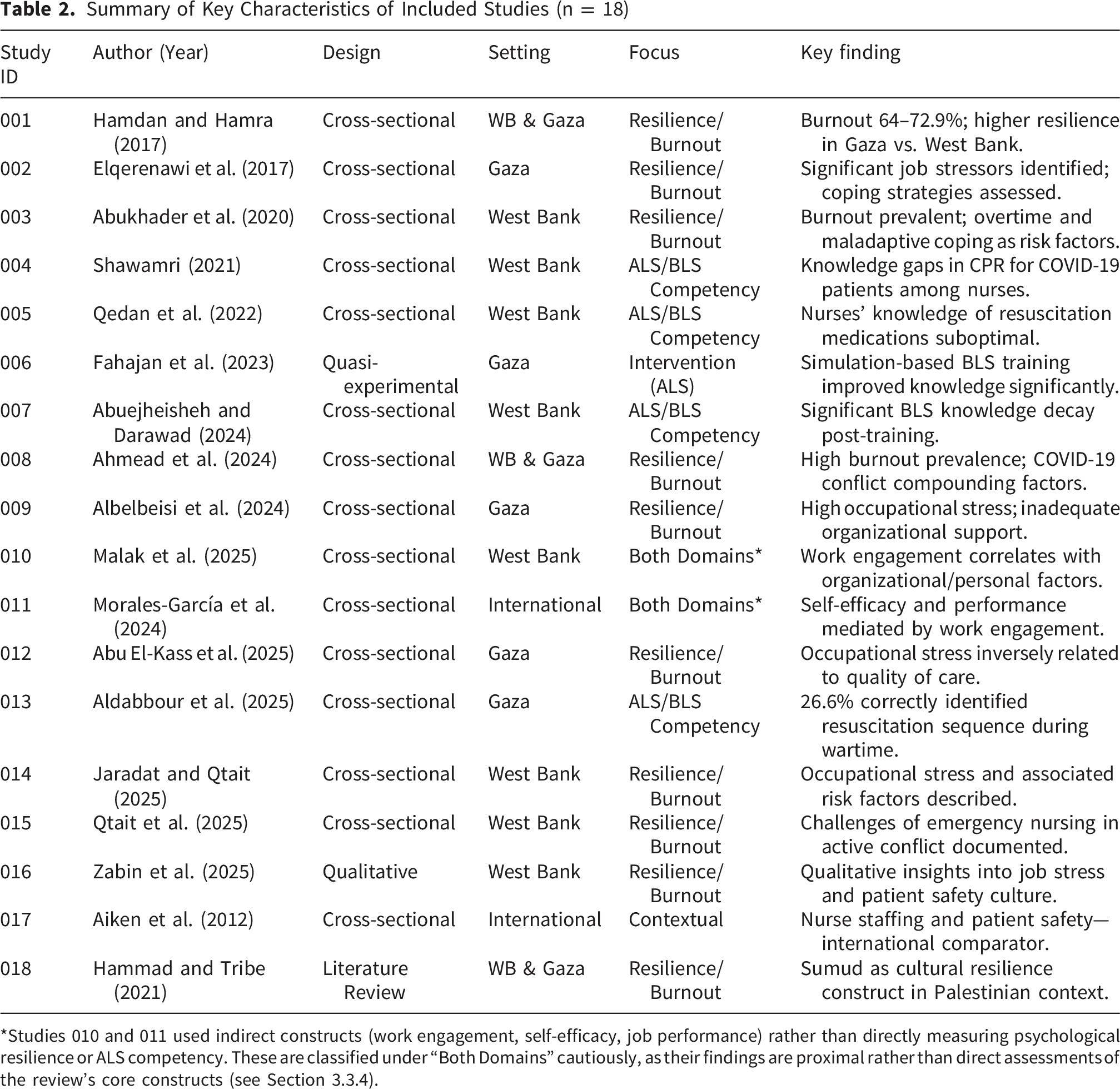
*Studies 010 and 011 used indirect constructs (work engagement, self-efficacy, job performance) rather than directly measuring psychological resilience or ALS competency. These are classified under “Both Domains” cautiously, as their findings are proximal rather than direct assessments of the review’s core constructs (see Section 3.3.4).
Mapping the Core Concepts
Evidence on Psychological Resilience and Burnout
Ten studies assessed psychological well-being, psychological resilience, or burnout. All employed assessment designs; no intervention studies were identified in this domain. Detailed findings from these ten studies are presented in Supplemental Table 1. Collectively, these studies documented high burnout prevalence (64%–72.9%), with one study (Hamdan & Hamra, 2017) reporting a finding of higher resilience among Gaza nurses compared to West Bank nurses. It is important to note that this spatial variation finding derives from a single study; it should not be interpreted as an established pattern but rather as a preliminary finding warranting replication and further investigation. Key protective factors identified across studies included social support and adaptive coping, while risk factors included overtime, insufficient organizational support, and maladaptive coping strategies.
Evidence on ALS/BLS Competency
Five studies assessed ALS/BLS knowledge, skills, or competency. All employed cross-sectional assessment designs; no intervention studies were identified beyond the single quasi-experimental study described in Section 3.3.3. Detailed findings from these five studies are presented in Supplementary Table 2. Critically, these studies used varied measurement instruments (e.g., knowledge-based multiple-choice questionnaires, self-report skill assessments), which limits direct comparability of findings. The predominant use of knowledge-based tests, rather than objective clinical performance assessments, is a methodological limitation across this domain. Notwithstanding, consistent findings included: critical gaps in resuscitation sequence knowledge; significant knowledge decay in the absence of retraining; a positive association between prior training and knowledge retention; and contextual barriers including chaotic environments and medication unavailability.
Evidence on Interventions
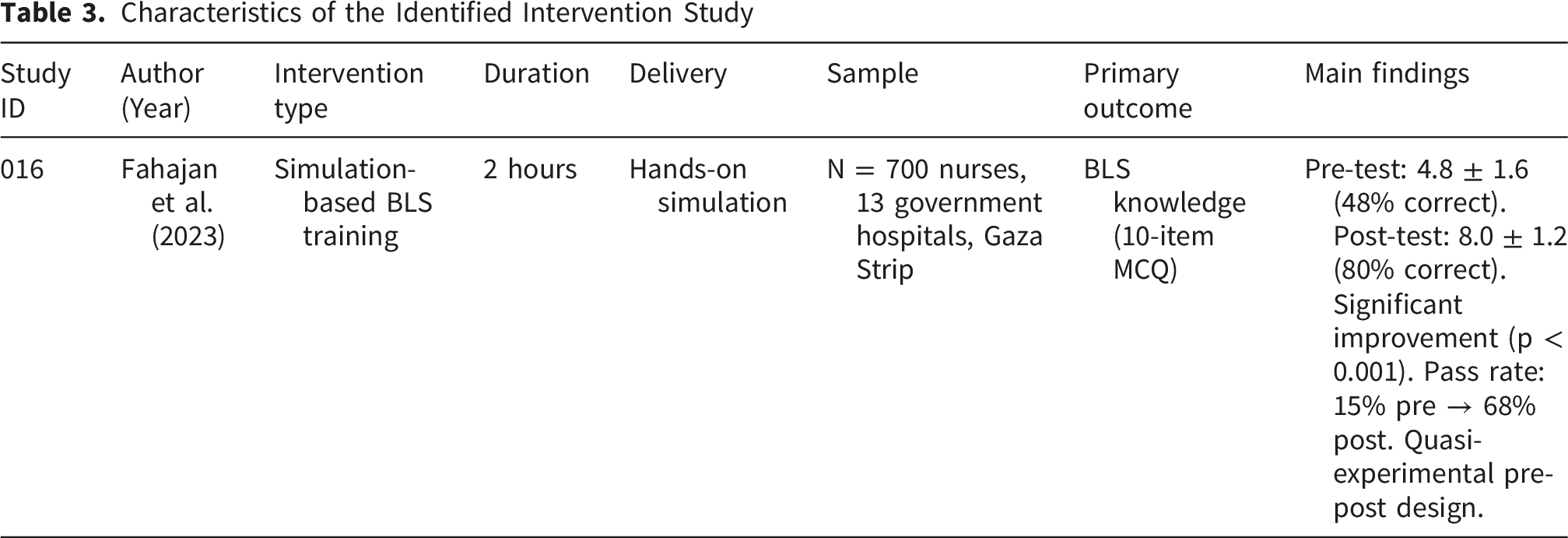
Characteristics of the Identified Intervention Study
Notably, no resilience-focused intervention studies were identified despite documented burnout rates of 64%–72.9% across the included studies. Furthermore, no studies evaluated interventions addressing both psychological well-being and clinical competency simultaneously. This dual absence represents the most significant evidence gap identified by this review.
Evidence on Relationships Between Domains
Only two studies examined relationships between psychological factors and performance-related outcomes: Malak et al. (2025), who investigated factors associated with work engagement among Palestinian emergency nurses during the Gaza conflict; and Morales-García et al. (2024), who examined relationships between self-efficacy, job performance, and life satisfaction in nurses. Both studies used indirect constructs, work engagement and self-efficacy, respectively, rather than directly measuring psychological resilience or objective ALS/BLS competency outcomes. These studies provide proximal, but not direct, evidence relevant to the resilience-competency relationship. Detailed findings from these studies are presented in Supplementary Table 3. No study in the included evidence base directly assessed the association between psychological resilience and objective ALS/BLS competency, confirming this as a critical and unaddressed empirical gap. This conclusion is based on systematic examination of all 18 included full-texts.
Cross-Cutting Methodological Observations
Across all 18 included studies, the predominance of cross-sectional designs represents a significant collective limitation. Cross-sectional studies can document associations and describe prevalence at a single point in time, but they cannot establish causal or temporal relationships. This design limitation is particularly consequential for the central question of whether psychological resilience and ALS competency are related, as cross-sectional data cannot address directionality. The absence of longitudinal, experimental, or quasi-experimental designs in all but one study severely restricts the strength of evidence available from this literature base.
Additionally, the variability in measurement tools used across studies, particularly for burnout (using different subscales of the Maslach Burnout Inventory, or alternate instruments) and competency (ranging from knowledge-based tests to self-report assessments), limits comparability between studies and precludes pooling of findings. Future research should work toward standardized, validated measurement approaches to enable cumulative synthesis.
Figure 2 provides a visual summary of the key evidence gaps identified across the 18 included studies, illustrating the disconnect between documented problems and the absence of intervention and relationship-based research. This visualization underscores the central conclusion of this section: a well-documented clinical and psychological burden exists among Palestinian emergency nurses, yet the evidence base remains overwhelmingly descriptive and offers no intervention studies addressing both domains concurrently. Conceptual Framework and Evidence Gaps in Palestinian Emergency Nursing Research. This visual summary illustrates the proposed bidirectional relationship between psychological resilience and ALS competency among emergency nurses in Palestinian hospitals (theoretical framework from Section 1.4, indicated by the dashed arrow). The left and right columns summarize the documented descriptive evidence for each domain. The bottom panel highlights the three critical evidence gaps identified by this review: (1) no studies directly examining the resilience-competency relationship, (2) no resilience-focused intervention studies, and (3) no integrated interventions addressing both domains simultaneously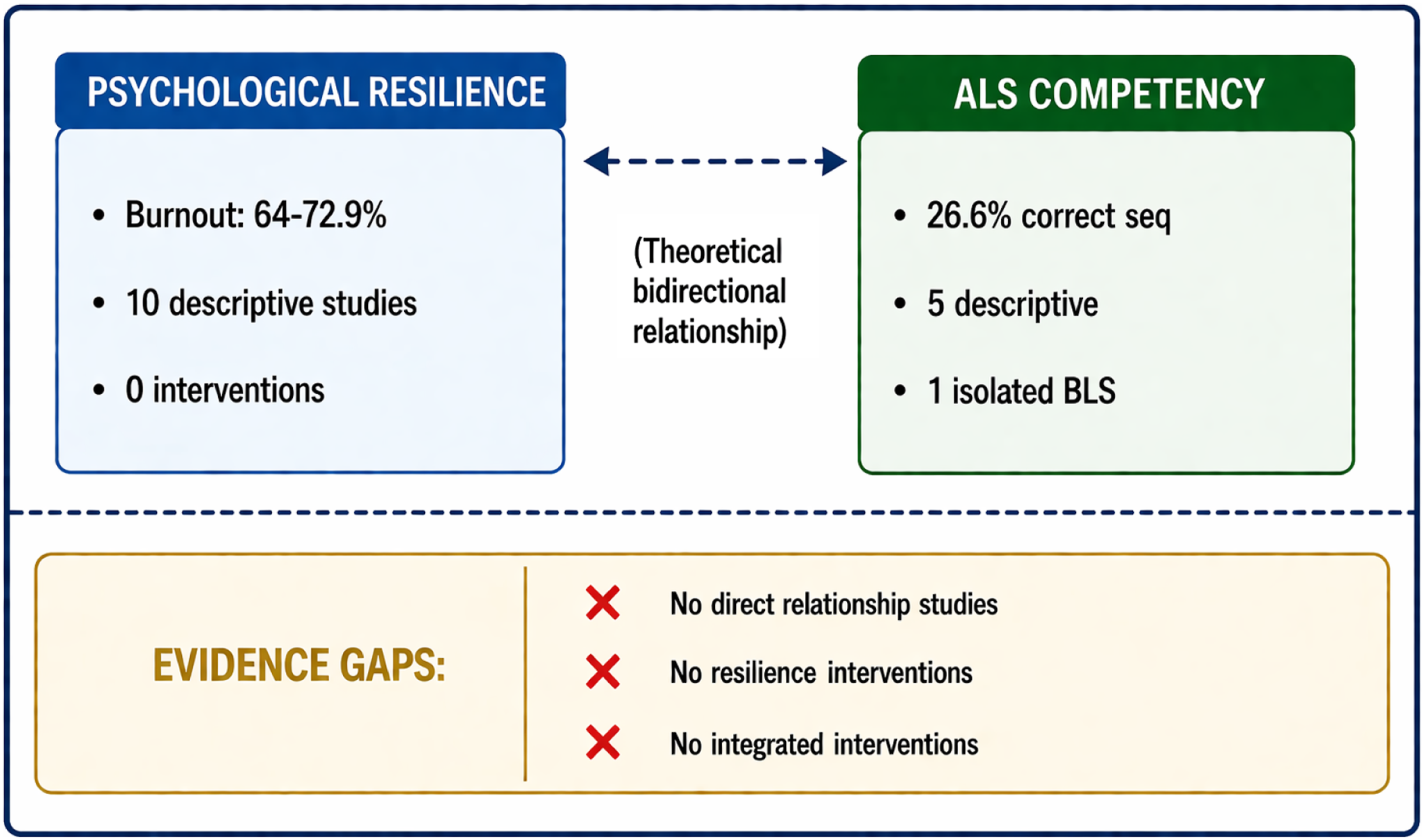
Narrative Synthesis
Finding 1: A Predominantly Descriptive Evidence Base Documenting High Burnout and Notable Competency Gaps
Ninety-four percent (94.4%) of included studies were descriptive or correlational in design, focused on documenting problems rather than testing solutions. Ten studies reveal a high prevalence of burnout (64%–72.9%) among Palestinian emergency healthcare workers. A finding of higher resilience among Gaza nurses compared to West Bank colleagues was reported in one study (Hamdan & Hamra, 2017); this finding is preliminary and derives from a single source, and should be interpreted with caution pending replication. Qualitative investigations provide complementary depth, indicating that organizational support for stress management remains inadequate and is largely left to individual initiative (Zabin et al., 2025).
Concurrently, five studies on ALS/BLS competency consistently document concerning knowledge and skill gaps. Critical deficiencies in resuscitation sequences and compression depth were identified, with only 26.6% of providers correctly identifying the resuscitation sequence during the wartime period (Aldabbour et al., 2025). Significant knowledge decay post-training and contextual barriers further challenge competency maintenance (Abuejheisheh & Darawad, 2024; Qedan et al., 2022). Together, these descriptive studies reveal the scope of a dual challenge: a psychologically distressed workforce attempting to provide high-risk emergency care with significant clinical skill deficits, yet the literature offers limited evidence for effective solutions.
Finding 2: A Near-Total Absence of Intervention Research
Only one intervention study was identified, a quasi-experimental study demonstrating that a two-hour simulation-based BLS training significantly improved knowledge and pass rates among 700 nurses in Gaza (Fahajan et al., 2023). This single study highlights a critical gap: despite burnout rates of 64%–72.9%, no psychological resilience-building intervention has been tested in this population. This represents a meaningful disconnect between documented need and evidence-based solutions. This pattern is consistent with an early-stage research landscape in which the priority has been to establish the scope of the problem through descriptive methods, a necessary but insufficient step toward evidence-based workforce support.
Finding 3: An Unaddressed Empirical Gap Regarding the Resilience-Competency Relationship
Only two studies examined relationships between psychological factors and performance-related outcomes, both using indirect measures (work engagement, self-efficacy) rather than direct assessments of psychological resilience or objective clinical competency (Malak et al., 2025; Morales-García et al., 2024). Systematic review of all 18 included full-texts confirmed that no study has directly assessed the relationship between psychological resilience and objective ALS/BLS competency outcomes, measured the impact of competency training on psychological resilience, or evaluated an integrated intervention targeting both domains simultaneously. While cognitive load theory (Sweller, 1988) and self-efficacy theory (Bandura, 1997) provide theoretical grounds for expecting such a relationship, the complete absence of empirical investigation within this population means that the proposed bidirectional framework introduced in Section 1.4 remains untested and should be treated as a hypothesis rather than an established finding.
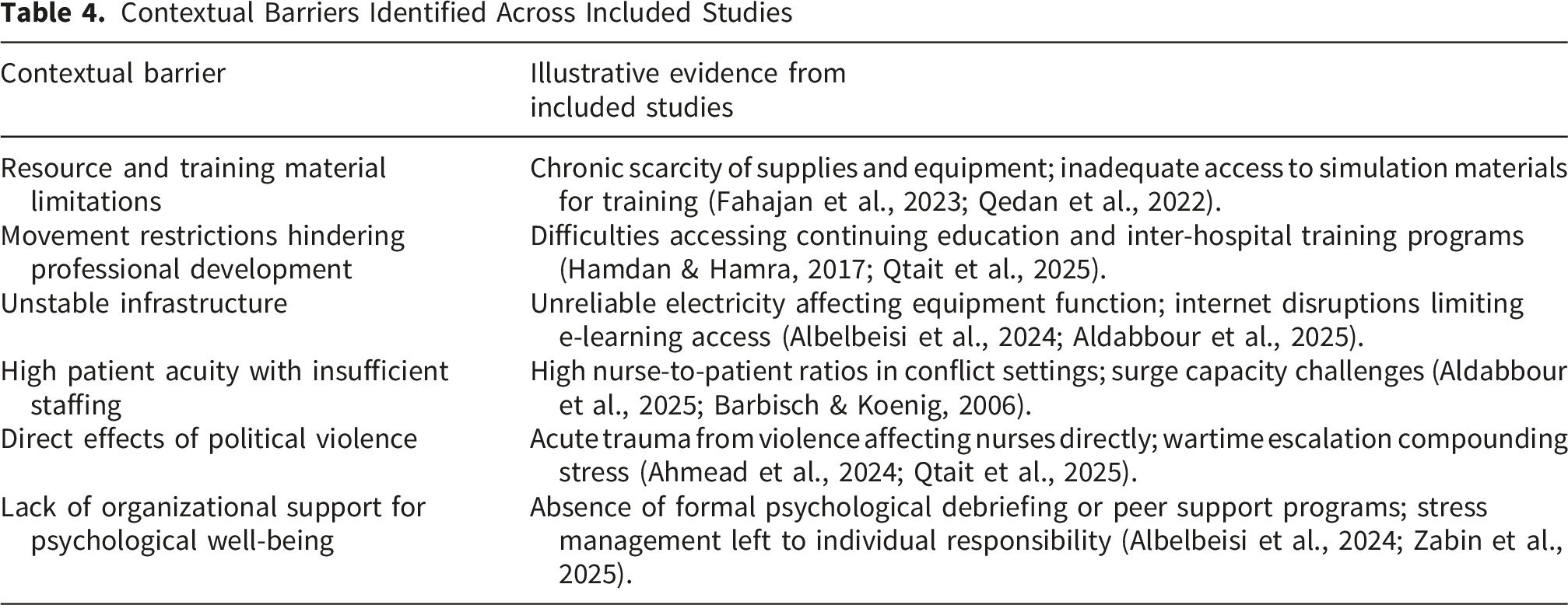
Finding 4: Contextual Challenges as Universal Barriers
Contextual Barriers Identified Across Included Studies
Discussion
This scoping review provides the first comprehensive map of the literature on psychological resilience and Advanced Life Support (ALS) competency among emergency nurses in Palestinian hospitals. The findings reveal a significant imbalance: while the prevalence of psychological distress, with burnout rates ranging from 64% to 72.9%, and critical clinical competency gaps, such as only 26.6% of providers correctly identifying the resuscitation sequence, are extensively documented, 94.4% of the existing literature is descriptive or correlational. No study has evaluated a psychological resilience-building intervention for this workforce, and no study has empirically examined the proposed link between psychological resilience and domain-specific clinical performance. These findings are broadly consistent with the early-stage research landscape observed in other conflict-affected healthcare settings, where documentation of need typically precedes intervention development (Truppa et al., 2024).
The heavy reliance on descriptive, cross-sectional evidence reflects the challenges inherent in conducting intervention research in active conflict settings, where logistical and ethical complexities are substantial (Arksey & O'Malley, 2005). This pattern is not unique to the Palestinian context; similar trajectories have been observed in other fragile and conflict-affected health systems (Truppa et al., 2024). However, the duration of this descriptive phase, spanning more than two decades, suggests that structural barriers to conducting intervention research in this context are significant and may require targeted capacity-building efforts. In contrast, in more stable environments, robust evidence supports the efficacy of various psychological resilience-building interventions, such as mindfulness-based stress reduction, peer support programs, and cognitive-behavioral techniques, in reducing burnout and improving well-being among healthcare workers (Yu et al., 2019). International research grounded in cognitive load (Sweller, 1988) and self-efficacy theories (Bandura, 1997) also robustly demonstrates the interconnectedness of psychological state and clinical performance (Fraser et al., 2014; Wetzel et al., 2006). Whether these theoretical relationships apply in the specific Palestinian context, and to what degree, remains to be empirically determined. The proposed bidirectional framework (Section 1.4) represents a theoretically grounded hypothesis to be tested rather than a conclusion supported by the available evidence.
One notable finding from the included literature is the spatial variation in psychological resilience, with nurses in Gaza demonstrating higher resilience scores than their counterparts in the West Bank, as reported by Hamdan and Hamra (2017). This finding derives from a single study and should be interpreted with considerable caution, as it may reflect measurement differences, sampling variation, or contextual factors specific to the study period rather than a reliable geographic pattern. If replicated in future research, it may suggest complex, non-linear adaptation to long-term adversity and may point to culturally rooted coping mechanisms, including the concept of Sumud (steadfastness) (Hammad & Tribe, 2021). Such possibilities reinforce the need for contextually nuanced, culturally grounded approaches to intervention development that build upon existing community strengths, rather than directly transplanting models from international settings.
The conceptual framework introduced in Section 1.4 posited a dynamic, bidirectional relationship between psychological resilience and ALS competency. The findings of this review demonstrate that this relationship, while theoretically plausible, is entirely empirically unexplored in this population. The complete absence of studies directly linking these two domains, combined with the absence of integrated interventions, means that the framework’s components remain unvalidated in this context. Future research should treat the examination of this relationship as a primary empirical objective.
The predominance of descriptive research, while representing a necessary foundation, creates a situation in which workforce needs are documented but not addressed within the research literature. This pattern warrants attention from research funders and institutions, who may wish to consider whether the current balance of descriptive versus intervention research is adequate given the documented scale of psychological distress and competency deficits in this population. This observation is not intended as a critique of individual researchers, who operate under significant constraints in conflict-affected settings, but rather as a systemic observation about research investment priorities.
Implications for Practice, Policy, and Research
Implications for Practice
The evidence from this review, while primarily descriptive, points toward several evidence-informed directions for practice. It is important to note that these recommendations are informed by the patterns identified in this review and by relevant international evidence; they are not directly supported by Palestinian-specific intervention studies, and should therefore be approached as evidence-informed priorities for piloting and evaluation rather than as established best practices.
Hospital administrators and clinical nurse leaders should consider: (1) prioritizing regular, low-resource, simulation-based BLS and ALS training programs, given the demonstrated effectiveness of even brief hands-on training in this context (Fahajan et al., 2023); (2) piloting integrated in-service programs combining brief, evidence-based psychological strategies with clinical simulation scenarios, and rigorously evaluating their impact; (3) ensuring any support programs are culturally appropriate, incorporating local concepts such as Sumud into program design; and (4) moving toward objective, simulation-based competency assessments (e.g., OSCEs) rather than relying solely on knowledge-based tests.
Implications for Policy
Policy-level implications should be understood in the context of the descriptive evidence base available. The following directions are theoretically informed and reflect evidence gaps rather than direct intervention findings. The Palestinian Ministry of Health and hospital leadership may wish to consider formally integrating psychological support and clinical competency development as components of workforce strategy for emergency departments. Research funding priorities, both local and international, could be rebalanced to support applied intervention research in this setting, with particular attention to studies exploring the resilience-competency link. Addressing macro-level structural barriers, such as movement restrictions for training and unstable supply chains, is a prerequisite for effective workforce support interventions.
Implications for Research
This review establishes a clear agenda for primary research. The highest priority should be given to rigorously designed intervention studies with dual-outcome measures (psychological resilience and ALS competency), developed using participatory methodologies that involve Palestinian emergency nurses as co-designers. Such studies should employ experimental or quasi-experimental designs where feasible, and should assess impact using both validated psychological scales (e.g., Maslach Burnout Inventory, Connor-Davidson Resilience Scale) and objective clinical competency measures (e.g., simulation scores, OSCE performance).
Longitudinal research is needed to track how psychological resilience and competency co-evolve over time. Tool development and validation efforts should create brief, context-appropriate instruments feasible for use in busy, resource-limited clinical settings. Implementation science perspectives will be essential for identifying barriers and facilitators to sustained delivery of interventions in this complex environment.
Strengths and Limitations
This review possesses several key strengths. It employed a comprehensive, multilingual search strategy across seven major databases and grey literature sources in English and Arabic, maximizing capture of relevant studies. It adhered to rigorous, pre-registered scoping review methodology (PRISMA-ScR), with dual independent reviewer screening and calibration prior to formal screening, resulting in high inter-rater reliability at all stages (kappa = 0.837–0.882). The included evidence base is highly current, with 44.4% of studies published in 2024–2025. As the first synthesis to map this specific intersection of psychological resilience and ALS competency in Palestine, its clear identification of the critical intervention gap constitutes a significant contribution to the field.
The review’s findings must be interpreted in light of its limitations. Most importantly, the absence of formal critical appraisal of included studies, justified by JBI scoping review guidance, means that the quality of the underlying evidence cannot be formally evaluated. The predominance of cross-sectional designs (17 of 18 studies) is a significant collective limitation, as these designs cannot establish causal or temporal relationships, which is particularly consequential for the review’s central question about the resilience-competency link. The partial verification of data extraction (20% of studies) introduces a risk of extraction error in the unverified subset. Grey literature may be underrepresented despite systematic efforts, given the challenging information environment of the Palestinian context. As with any review, publication bias may be present, skewing evidence toward statistically significant or problem-focused findings. Finally, the finding that only one intervention study exists, far from being a limitation of the review’s methodology, directly validates the review’s primary conclusion about the state of the evidence.
Future Directions
This review crystallizes several pivotal, unresolved questions for the next generation of research. First, the directionality of effect between psychological resilience and competency remains entirely unknown, and establishing this through longitudinal or experimental research is fundamental. Second, the efficacy of integrated intervention programs must be tested empirically. Third, mechanistic qualitative research is needed to explore the lived experience of the resilience-competency interplay from the nurses’ own perspectives.
Cultural feasibility is paramount: which evidence-based intervention components can be most effectively adapted for the Palestinian context, and how can culturally rooted constructs such as Sumud (steadfastness) be incorporated into intervention design? Finally, implementation science approaches are needed to identify the specific barriers and facilitators to delivering and sustaining integrated interventions within the complex environment of Palestinian hospitals. Addressing these questions requires sustained investment in intervention-oriented research conducted in genuine partnership with Palestinian nurses and institutions.
Conclusion
This scoping review provides the first comprehensive map of the literature concerning psychological resilience and Advanced Life Support competency among emergency nurses in Palestinian hospitals. The mapped evidence reveals a consistent finding: an extensive body of descriptive studies documents a workforce under significant psychological and professional pressure, characterized by high burnout rates and notable clinical skill deficits, while intervention research aimed at addressing these challenges remains almost entirely absent. The central evidence gap identified is the complete absence of studies examining the proposed relationship between psychological resilience and ALS competency, and the absence of integrated interventions targeting both domains simultaneously. This gap reflects the early-stage nature of this research area and the significant challenges of conducting intervention research in conflict-affected settings.
Palestinian emergency nurses, who operate under conditions of profound and ongoing challenge, would benefit from research that moves beyond documentation toward the development and rigorous evaluation of practical support. The findings of this review should inform research investment decisions, encouraging a shift toward feasibility and intervention studies that are co-designed with Palestinian nurses, culturally grounded, and rigorously evaluated. The well-being of this workforce and the safety of the patients they serve are the ultimate justification for this research agenda.
Supplemental Material
Supplemental Material -Resilience-Building Interventions and Advanced Life Support Competency for Emergency Nurses in Palestinian Hospitals: A Scoping Review
Supplemental Material for Resilience-Building Interventions and Advanced Life Support Competency for Emergency Nurses in Palestinian Hospitals: A Scoping Review by Saqr Alkorom, Mei-Chan Chong, Noor Hasliza Che Seman and Ibrahim Aqtam in Sage Open Nursing.
Footnotes
Authors Contributions
SA: Conception, search strategy development, drafting of manuscript. MC, NH, IA: Supervision, critical revision, and intellectual review. SA & IA: Study screening, data extraction, and verification. NH & SA: Corresponding authors, submission management. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
AI Declaration
During the preparation of this work, the authors used AI-assisted tools for language refinement and initial drafting. The authors reviewed, edited, and take full responsibility for the final manuscript.
Statistical Statement
As a scoping review of published literature, this study did not involve primary data collection or statistical analysis.
Nagoya Protocol Compliance
This scoping review utilized only published literature; no biological or genetic resources were accessed.
Patient or Public Contribution
This study did not include patient or public involvement in its design, conduct, or reporting.
Scoping reviews are outside the scope of PROSPERO, which accepts systematic review protocols only. This review was therefore pre-registered on OSF, consistent with current JBI scoping review guidance (Peters et al., 2020). The OSF registration contains the full a priori protocol, including search strategy, eligibility criteria, and data extraction framework, established prior to study selection.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.