
Abstract
Introduction
Recovery-oriented care is central to community mental health. Among psychiatric home-visit nurses in Japan, prior psychiatric hospital experience or recovery-related training is commonly required; however, their relationship with recovery-oriented attitudes remains unclear.
Objective
To examine the association between years of psychiatric hospital work experience and recovery-oriented attitudes and knowledge among psychiatric home-visit nurses.
Methods
In this nationwide cross-sectional web survey of nurses from 1,500 randomly selected agencies, data from 237 registered nurses were analyzed after excluding licensed practical nurses and cases with missing or implausible values. Recovery attitudes and knowledge were assessed using the Japanese 7-item Recovery Attitudes Questionnaire (RAQ) and the Japanese 16-item Recovery Knowledge Inventory (RKI-16). Linear regressions examined associations between years of psychiatric hospital experience and recovery attitudes and knowledge, adjusting for age, sex, home-visit nursing experience, adequacy of agency education, and academic background. An exploratory subgroup analysis compared psychiatric-specialized and general agencies.
Results
Years of hospital experience were not associated with recovery attitudes or knowledge in the fully adjusted models (RAQ: B = 0.04, p = 0.232; RKI-16: B = −0.09, p = 0.176). Hospital experience was positively associated with RAQ Beliefs score (B = 0.05, p = 0.029), although the effect size was modest. Exploratory analyses showed higher RAQ but lower RKI-16 scores in psychiatric-specialized versus general agencies.
Conclusion
Inpatient experience may reinforce belief in recovery, whereas psychiatric hospital tenure alone may be insufficient to explain the broader recovery-oriented attitudes or recovery knowledge.
Keywords
Introduction
The Japanese mental health policy has shifted from “hospital-centered care” to “community life-centered care” since the creation of the Vision for Reform of Mental Health and Welfare (Ministry of Health, Labour and Welfare, 2006). In the early 2000s, when the current generation of mid-career nurses commenced their careers, hospital-based nursing in Japan placed significant emphasis on ensuring safety and providing protective care (Aoki, 2005). Following the 2017 governmental review on the future of mental health and welfare services (Ministry of Health, Labour and Welfare, 2017), the construction of a community-based integrated care system for people with mental disorders has been promoted. Psychiatric home-visit nursing is an indispensable component of this system. Institutionalized in 1986 with coverage under national health insurance, psychiatric home-visit nursing has expanded substantially with service users increasing from 13,532 in 2007 to 52,203 in 2015 (Kayama et al., 2020).
To claim the basic fee for psychiatric home-visit nursing, nurses must meet at least one of four criteria: (1) at least one year of work experience in a psychiatric hospital ward or psychiatric outpatient department of a designated medical institution; (2) at least one year of experience providing home-visit nursing to individuals with mental disorders; (3) at least one year of experience in mental health-related services at a mental health center or public health center; or (4) completion of a training program in mental health care organized by national or prefectural authorities or relevant professional bodies. Thus, either psychiatric hospital experience or completion of relevant training is required. However, not all nurses have prior hospital employment.
Review of Literature
Recovery in mental health is a key concept encompassing empowerment, self-management, and social inclusion (Potter, 2010). Rather than focusing solely on the disability, the recovery perspective emphasizes the possibility of living well while experiencing mental health problems (Slade & Longden, 2015).
Borkin et al. (2000) defined recovery orientation as the stance that people can recover from mental illness. A review of studies up to 2022 reported that recovery-oriented practice in community mental health is effective in preventing social isolation, reducing stigma, supporting employment, and promoting self-management (Mousavizadeh & Jandaghian Bidgoli, 2023). Recovery-oriented care aimed at facilitating discharge and transition to community living has therefore become increasingly important. Among mental health professionals, internal work motivation and the experience of discharging patients after a lengthy hospitalization were significantly and positively associated with recovery attitudes (Chiba et al., 2020). Working at community facilities and being young were significantly and weakly correlated with recovery knowledge. Participation in self-help groups was positively associated with both recovery knowledge and recovery attitudes, whereas formal education showed positive but weak associations (Chiba et al., 2020). Nurses working in high-security forensic psychiatric units showed more positive attitudes toward patients, lower social distance, greater trust, greater willingness to treat, and a lower tendency to perceive patients as threatening compared to nurses in general inpatient settings (Kılıç-Demir & Kızılpınar, 2024). Nurses play a central role in delivering community-based, recovery-oriented mental health services. As key coordinators, community health nurses bridge service users, family caregivers, and providers to support self-management, continuity of care, and community inclusion (Mousavizadeh & Jandaghian Bidgoli, 2023). Among Japanese nurses, those with prior work experience in general healthcare had significantly lower recovery-oriented attitudes than those without, and greater personal stigma was associated with lower recovery-oriented attitudes (Nakanishi et al., 2025).
Despite the policy emphasis on recovery-oriented community care, few studies have examined recovery-oriented attitudes among psychiatric home-visit nurses in Japan. Particularly, it remains unclear how psychiatric hospital work experience influences recovery orientation among these nurses. Clarifying this association is important for informing educational content and improving the quality of recovery-oriented practice in community settings.
Objective
Japan’s psychiatric home-visit nursing requirements present a paradox: while psychiatric hospital experience is prioritized as a primary qualification, the “protective care” models prevalent when many mid-career nurses trained may not foster recovery-oriented attitudes. Consequently, relying on such clinical tenure as a proxy for community competence may be insufficient. Examining this association is essential to evaluate current professional requirements and inform future educational strategies. This study aimed to examine the association between psychiatric hospital work experience and recovery-oriented attitudes among psychiatric home-visit nurses in Japan. It was hypothesized that years of psychiatric hospital experience would be positively associated with both recovery-oriented attitudes and recovery knowledge. The findings are intended to inform future educational strategies and enhance clinical practice quality in community-based mental health care.
Methods
Design
This study used a nationwide cross-sectional web survey design.
Research Questions
1) What are the levels of recovery-oriented attitudes and knowledge among psychiatric home-visit nurses? 2) Are these associated with years of psychiatric hospital experience? 3) Do they differ between psychiatric-specialized and general agencies?
Sample
A total of 1,500 nursing agencies were randomly selected from the national registry of home-visit nursing agencies designated under the Self-Support Medical Care program for psychiatric outpatient care. Managers selected agencies were invited to distribute a flyer with a Quick Response code to up to three eligible nurses; only agencies that consented proceeded to staff distribution; nurse participation was voluntary and anonymous.
Inclusion/Exclusion Criteria
Eligible respondents for the revised analytic sample were registered nurses; licensed practical nurses who responded were excluded from the main analysis. A web-based questionnaire was administered over a one-month period between January and February 2024.
The questionnaire collected data on sociodemographic characteristics and years of psychiatric hospital experience. Perceived adequacy of agency-based education was rated on a 5-point, equal-interval Likert scale (1 = not at all sufficient to 5 = very sufficient). Recovery-oriented attitudes and knowledge were assessed using the Japanese 7-item Recovery Attitudes Questionnaire (RAQ) and the Japanese 16-item Recovery Knowledge Inventory (RKI-16), respectively.
Multiple instruments have been developed to measure recovery-related constructs. Bedregal et al. (2006) developed the RKI to assess staff knowledge about recovery, and Borkin et al. (2000) developed the RAQ to assess recovery-oriented attitudes. These tools have been used to evaluate psychoeducational programs and the effects of recovery-oriented training (Bullock et al., 2000; Crowe et al., 2006; Young et al., 2005). They have also been translated and culturally adapted for use in different contexts, including Japan (Chiba et al., 2016, 2017). In Japan, the RAQ has been used to explore factors influencing recovery-oriented attitudes among mental health professionals (Chiba et al., 2016) and to survey nursing directors of psychiatric hospitals (Matsui et al., 2024). It has also been used in developing a scale to assess the recovery-oriented attitudes of nurses engaged in dementia care (Furuno et al., 2023).
RAQ: Japanese 7-Item Version
The RAQ is a self-report measure originally developed by Borkin and colleagues to assess attitudes toward mental health recovery and is applicable to professionals, service users, family members, and the public. This study used the validated Japanese 7-item short form developed by Chiba et al. (2016). The Japanese short form comprises seven items with a two-factor structure (Beliefs and Difficulties), rated on a 5-point Likert scale; total scores range from 7 to 35, with higher scores indicating more recovery-oriented attitudes. The Japanese version has demonstrated reasonable concurrent validity; however, internal consistency has been reported as modest (Cronbach’s α = 0.64 for the total score), and test–retest reliability has been described as unsatisfactory to modest (intraclass correlation coefficient = 0.68).
RKI: Japanese 16-Item Version
Recovery-related knowledge was measured with the Japanese 16-item RKI (Chiba et al., 2017). Items are rated on a 5-point Likert scale, with higher scores reflecting greater knowledge of recovery principles. The Japanese 16-item RKI has shown reasonable factorial validity and good convergent validity, with acceptable internal consistency for the total score (Cronbach’s α = 0.77); however, domain-level reliability varies (Chiba et al., 2017).
Subgroup Analysis by Agency Specialization
To explore the potential role of organizational context, an exploratory subgroup analysis compared recovery-oriented attitudes and knowledge between psychiatric-specialized and general agencies. An agency-type variable was derived from respondents’ self-reported proportion of psychiatric home-visit nursing in daily practice. Agencies were classified as psychiatric-specialized if ≥ 60% of visits were psychiatry-related (i.e.,categories 61–80% or 81–100%), and as general if <60% (0–20%, 21–40%, 41–60%). Group mean scores for RAQ Beliefs, RAQ Difficulties, RAQ total, and RKI-16 were compared using independent-samples t tests. When homogeneity of variance was violated (Levene’s test), Welch’s t was reported. Effect sizes (Cohen’s d) and 95% confidence intervals were computed. Tests were two-sided with α= .05. Given the exploratory nature and multiple outcomes, no adjustment for multiplicity was made, the comparisons were interpreted as hypothesis-generating. Descriptive group statistics are shown below.
Institutional Review Board Approval, Informed Consent, and Animal/Human Subjects’ Rights
Ethics Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
Participants viewed an online information sheet describing the study aims, voluntary participation, anonymity, data handling, and contact information, and provided informed consent before responding to the questionnaire.
Statistical Analysis
Cases with missing or implausible values were excluded. Linear regression analyses were conducted, with years of psychiatric hospital experience as the independent variable and RAQ total, RAQ subscale, and RKI-16 scores as dependent variables. Three models were estimated:
Model 1 (unadjusted): hospital experience only.
Model 2 (age/sex-adjusted): adjusted for age and sex.
Model 3 (fully adjusted): further adjusted for years of psychiatric home-visit nursing experience, perceived adequacy of agency-based education (5-point Likert, 1–5), and academic background (analyzed as a three-category variable: university/graduate school, junior college/vocational school, and high school). All tests were two-sided with α = 0.05. Analyses were performed using JMP version 17 (SAS Institute Inc.). Reporting adhered to the STROBE guidelines.
Results
Sample Characteristics
Characteristics of Study Participants

Note. N= 237. Values are presented as M (SD) or n (%). RAQ = Recovery Attitudes Questionnaire; RKI-16 = 16-item Recovery Knowledge Inventory.
Research Question Results
Regression Results (RAQ/RKI-16)
RAQ total: In simple regression, years of psychiatric hospital experience were not associated with total RAQ scores (Model 1: B = 0.051, p = 0.101). The association remained non-significant after adjustment for age/sex (Model 2: B = 0.061, p = 0.087) and after further adjustment for years of home-visit nursing experience, perceived adequacy of agency education, and academic background (Model 3: B = 0.044, p = 0.232).
Multiple Regression Analysis of Factors Associated With RAQ and RKI-16 Scores
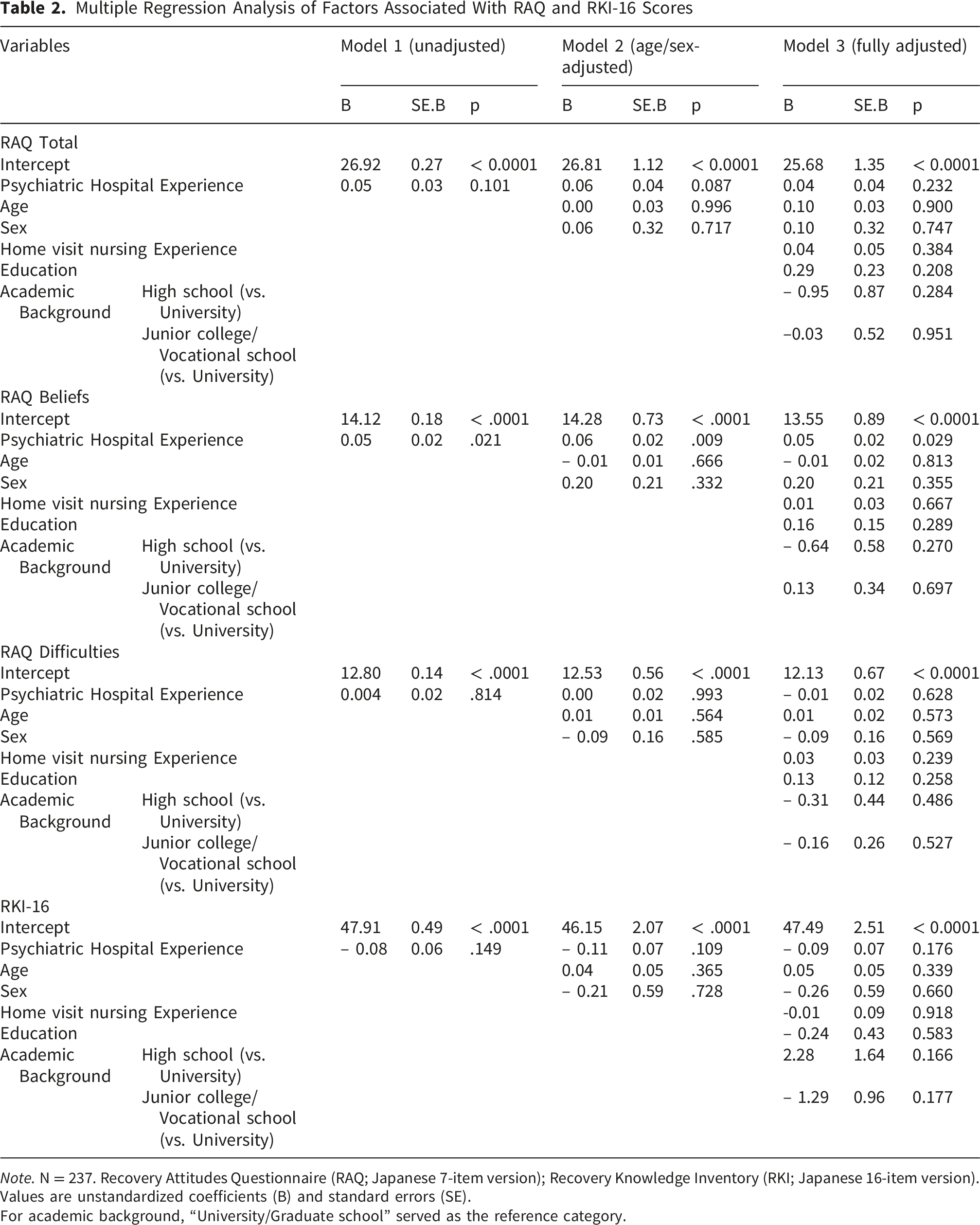
Note. N = 237. Recovery Attitudes Questionnaire (RAQ; Japanese 7-item version); Recovery Knowledge Inventory (RKI; Japanese 16-item version). Values are unstandardized coefficients (B) and standard errors (SE).
For academic background, “University/Graduate school” served as the reference category.
RKI-16
Years of hospital experience were not significantly associated with recovery knowledge in simple or adjusted models (Model 1: B = -0.082, p = 0.149; similarly, non-significant in Models 2–3) (Table 2).
Group Comparisons by Agency Type
Group Comparisons of Recovery-Oriented Attitudes and Knowledge Between Psychiatric-Specialized and General Home-Visit Nursing Agencies
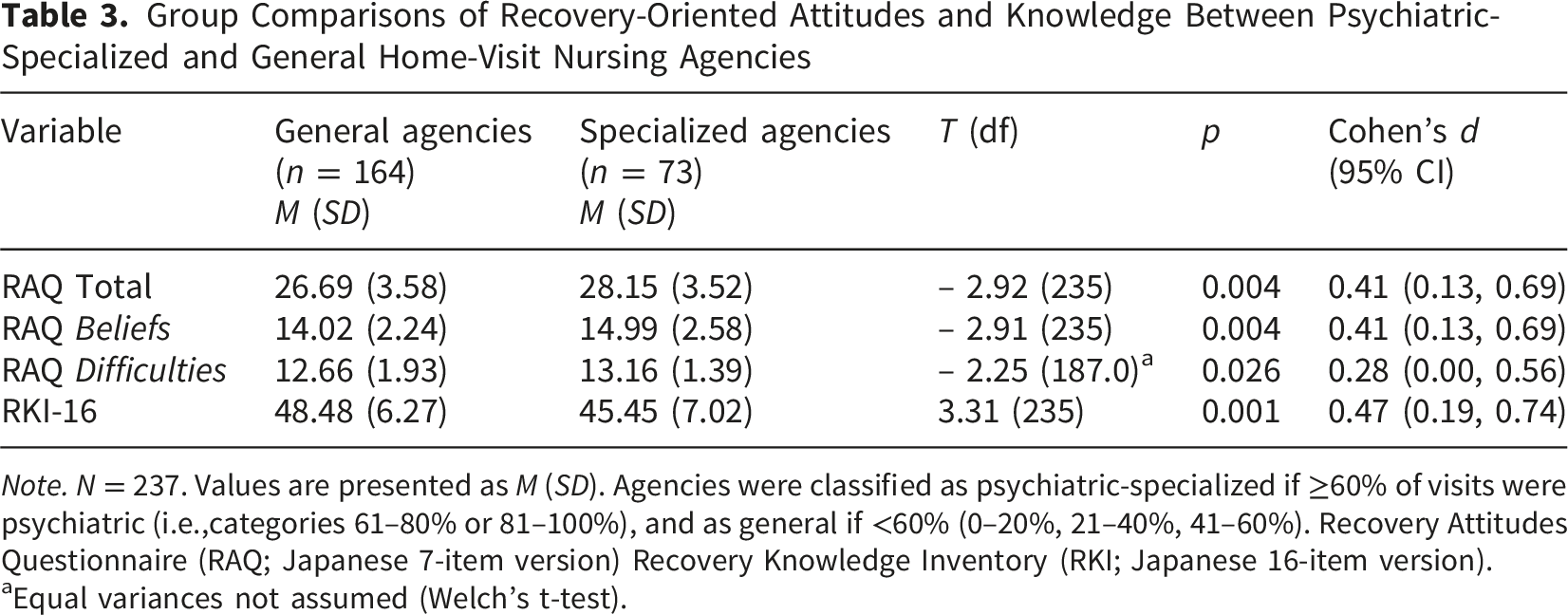
Note. N = 237. Values are presented as M (SD). Agencies were classified as psychiatric-specialized if ≥60% of visits were psychiatric (i.e.,categories 61–80% or 81–100%), and as general if <60% (0–20%, 21–40%, 41–60%). Recovery Attitudes Questionnaire (RAQ; Japanese 7-item version) Recovery Knowledge Inventory (RKI; Japanese 16-item version).
aEqual variances not assumed (Welch’s t-test).
Discussion
Principal Findings
In this nationwide sample of psychiatric home-visit nurses, years of prior psychiatric hospital work was not associated with overall recovery-oriented attitudes (RAQ total) or recovery knowledge (RKI-16). Psychiatric hospital experience was positively associated only with the RAQ Beliefs subscale.
Interpretation
The findings suggest that clinical exposure may influence distinct facets of recovery-oriented attitudes. The fact that only the RAQ Beliefs subscale was associated with inpatient experience indicates a limited, domain-specific association. Although this association was positive, its practical magnitude was modest, suggesting that even a decade of experience would correspond to an increase of only approximately 0.5 points on the subscale. Inpatient experience may be related to endorsement of certain recovery-related beliefs; however, the mechanisms underlying this association cannot be determined from the present data. It is plausible that repeated contact with patient recovery trajectories in inpatient care (e.g. seeing patients stabilize and move toward discharge) helps instill hope and belief in recovery outcomes. Consistent with this idea, a prior study in Japan found that mental health professionals who had experience facilitating the discharge of long-term psychiatric inpatients held more positive recovery attitudes (Chiba et al., 2020). In contrast, broader recovery-oriented attitudes and recovery knowledge may require factors beyond tenure alone, such as the quality of recovery-oriented education, organizational culture, and opportunities for reflective learning. Simply accumulating years in traditional settings may not guarantee broader recovery-oriented thinking; indeed, one survey of psychiatric nursing directors reported that greater length of service was associated with more traditional (less recovery-oriented) attitudes unless accompanied by higher recovery-related knowledge (Matsui et al., 2024). This underscores the need to examine specific educational and organizational factors that may shape recovery-oriented attitudes and knowledge.
Organizational Context
An exploratory subgroup analysis showed an attitude–knowledge divergence across agency types: nurses in psychiatric-specialized agencies demonstrated higher recovery-oriented attitudes (RAQ), yet lower recovery-related knowledge (RKI-16). This suggests that psychiatric specialization does not necessarily correspond to stronger conceptual knowledge of recovery principles. This pattern may reflect differences in workplace learning opportunities or exposure to formal recovery-oriented education. However, because these comparisons were exploratory, the interpretations remain tentative. Nationwide findings indicating heterogeneity across home-visit nursing stations are broadly consistent with this possibility (Kido et al., 2023; Setoya et al., 2023).
Practice & Education (Individual Level)
Although the present study highlights a potential divergence between clinical exposure and recovery knowledge, the specific content, timing, provider, dose, or impact of prior training was not assessed. Consequently, the precise educational mechanisms underlying this divergence remain unclear.
Although the present study does not support recommending specific curricula, the observed gap warrants further investigation into whether education targeting conceptual elements of recovery (e.g., non-linear recovery processes and positive risk-taking) is associated with improvements in recovery knowledge. Prior studies have reported improvements in staff recovery knowledge and/or attitudes following structured recovery training programs (Meehan & Glover, 2009; Walsh et al., 2017), and a review has summarized recovery-focused educational programs for mental health nurses (Hawsawi et al., 2021). In the Japanese context, recovery knowledge and recovery-oriented attitudes have also been discussed as related constructs (Matsui et al., 2024). Future research should directly measure training characteristics and evaluate their associations with both recovery attitudes and recovery knowledge.
Organization (Team/System Level)
To bridge the observed attitude–knowledge divergence between specialized and general agencies, cross-training and exchange programs may be helpful so that staff in “attitude-rich” settings gain up-to-date knowledge, while those in “knowledge-rich” settings absorb recovery values. Peer support and structured team reflection may help normalize recovery-oriented practice, brief, recurring training sessions may help sustain gains (Roth et al., 2021). Evidence that experience in delivering recovery-oriented support, alongside structured education, strengthens recovery beliefs further underscores the need for organizational investment in a strong training culture (Wilrycx et al., 2012). Ensuring equitable access to recovery-centered learning across agency types, along with leadership that champions these values, may help close the attitude–knowledge gap and better equip nurses to deliver recovery-oriented community care.
Strengths and Limitations
A key strength is the nationwide sampling frame of community mental health nurses and the concurrent assessment of attitudes (using RAQ) and knowledge (using RKI), which provides a more granular view of recovery orientation than either measure alone.
Several limitations should be noted. First, the cross-sectional design precludes causal inference. Second, the overall response rate was low (5.6%), and recruitment involved a two-stage opt-in (agency managers consenting to distribute the survey and individual nurses choosing to respond), which may have favored more recovery-interested or better-resourced participants and inflated means while attenuated variability. Since within-agency sampling frames were unknown, stage-specific response rates could not be computed, nonresponse weights could not be applied, and standard errors were not adjusted for clustering by agency.
Third, all measures were self-reported, introducing potential common method bias and reliance on participants’ honesty and insight. In particular, the RAQ was a brief 7-item scale that, while convenient, has known psychometric constraints. Prior studies have found the RAQ-7 to have only moderate internal consistency (Cronbach’s α on the order of 0.6) and suboptimal test–retest reliability (Chiba et al., 2016). Such measurement limitations may have attenuated detectable associations in this study (i.e., some true relationships might not have been captured because of scale imprecision). Finally, residual confounding from unmeasured factors cannot be excluded. Variables such as nurses’ caseload mix, exposure to specific recovery training programs, or the leadership climate of their organizations could plausibly affect both work experiences and recovery orientation. The analyses adjusted for several observable factors; however, unmeasured influences remain possible.
Agency education was measured by a single self-rated adequacy item; the presence, content, provider, timing, or dosage of recovery-oriented training was not assessed. Future research should use more objective measures to evaluate the specific impact of structured recovery education. longitudinal or intervention-based studies are also needed to determine whether structured recovery-oriented education can mediate the relationship between clinical experience and the development of comprehensive recovery knowledge.
Implications for Practice
Given Japan’s reimbursement rules requiring prior hospital experience or approved training, these findings suggest that such qualification pathways alone may be insufficient indicators of recovery-oriented practice in psychiatric home-visit nursing. Home-visit nursing agencies may need to evaluate whether staff development and workplace learning adequately support broader recovery-oriented attitudes in community mental health care.
Conclusion
In this nationwide cross-sectional study of psychiatric home-visit nurses (N = 237), prior psychiatric hospital experience was not associated with overall recovery-oriented attitudes (RAQ total) or recovery knowledge (RKI-16), although it showed a small positive association with the RAQ Beliefs subscale. Exploratory comparisons indicated that nurses in psychiatric-specialized agencies reported higher RAQ scores (total and subscales) but lower RKI-16 than those in general agencies, suggesting a potential attitude–knowledge divergence by organizational context.
Supplemental Material
Supplemental Material - Hospital Experience and Recovery Orientation Among Psychiatric Home-Visit Nurses: A Cross-Sectional Study
Supplemental Material for Hospital Experience and Recovery Orientation Among Psychiatric Home-Visit Nurses: A Cross-Sectional Study by Yoshiyuki Takashima, RN, PhD, Maiko Matsumura, RN, MSN, Ryu Suzuki, RN, MSN, Takemasa Ishikawa, RN, PhD in Sage Open Nursing
Footnotes
Acknowledgments
The authors are grateful to all the study participants for their valuable contributions.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. This study was approved by the Research Ethics Committee of Baika Women’s University (2023-0245).
Consent to Participate
Participants viewed an online information sheet describing the study aims, voluntary nature of participation, anonymity, data handling, and contact information, and provided informed consent before responding to the questionnaire.
Consent for Publication
Not applicable, as the study did not include any individual person’s data in any form (including individual details, images, or videos).
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Nana-r home-visit nursing research grant project (grant number 05010)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.