
Abstract
Background
Non-reassuring fetal heart rate patterns refer to specific alterations in the fetal heartbeat during labor or pregnancy, suggesting that the baby may not be receiving adequate oxygen. Globally, non-reassuring fetal heart rate patterns during labor contribute to maternal and neonatal mortality. In this study, the prevalence of non-reassuring fetal heart rate patterns and their related key risk factors among laboring mothers were examined.
Methods
A cross-sectional, facility-based study was conducted between April 15 and June 15, 2024, at the West Guji Hospital, Oromia, Ethiopia. Data were collected from 361 women in labor who were systematically selected. Both bivariable and multivariable logistic regression analyses were used to identify statistically significant variables associated with the outcome. A p-value less than 0.05, a adjusted odds ratio, and 95% confidence intervals were used to declare statistically significant variables.
Results
The study found that the prevalence of non-reassuring fetal heart rate patterns among laboring women was 21.6% (n = 78; 95% CI: 17.5-26.2). Key risk factors significantly linked to non-reassuring fetal heart rate patterns were women referred from other facilities (AOR = 5.19, 95% CI = 2.27-11.90), blood-stained amniotic fluid (AOR = 3.55, 95% CI = 1.44-8.68), meconium-stained amniotic fluid (AOR = 3.87, 95% CI = 1.68-8.89), women undergoing labor augmentation (AOR = 2.26, 95% CI = 1.06-4.83), and women experiencing prolonged labor (AOR = 2.73, 95% CI = 1.17-6.38).
Conclusion
Despite the use of intermittent auscultation for fetal heart rate assessment, the prevalence of non-reassuring patterns was notably higher than that reported in previous studies. Factors significantly associated with these patterns included being a referred case, the presence of blood-stained or meconium-stained amniotic fluid, labor augmentation, and prolonged labor. This study highlights the importance of closely monitoring and timely intervention in women with these risk factors.
Background
A non-reassuring fetal heart rate pattern is a term used to describe fetal hypoxia secondary to inadequate oxygen supply to the fetus. The concept of the fetus as a patient is fundamental to current obstetric practice (Purandare, 2024). Considering an abnormal fetal heart rate as a single parameter to identify fetal distress alone leads to improper management, which is why the concept of non-reassuring fetal heart rate patterns has been introduced (Borovitz et al., 2024).
Although neonatal mortality has declined since 1990, progress has been slow. In 2024, 2.3 million newborns died, a rate of 17.2 per 1,000 live births accounting for 47% of all under-five mortality (UNICEF, 2026b). Intrapartum-related events, such as birth asphyxia and trauma, account for 21% of all deaths.
If current trends persist, an estimated 13 million neonatal deaths will occur between 2025 and 2030 (UNICEF, 2026a). Currently, non-reassuring fetal heart rate patterns are the most common and tend to increase the rates of Cesarean sections and operative vaginal deliveries more than those recommended by the World Health Organization (Chuwa & Nganga, 2026).
The practice of continuous electronic fetal monitoring is less common in sub-Saharan Africa and South Asia (Mwakawanga et al., 2025). Some of the health risks caused by non-reassuring fetal heart rate patterns include hypoxia, varying degrees of intellectual disability and/or seizures, cerebral palsy, motion impairment, visual and hearing impairment, learning disabilities, and stillbirths (Ayebare et al., 2021). Mothers also face additional risks such as cesarean section, blood loss, long hospital stays, infection, and possible birth injuries (Gul et al., 2025).
A common reason for a neonate’s admission to the neonatal intensive care unit (NICU) and death during the neonatal period is a non-reassuring fetal heart rate pattern (Suciu et al., 2021). Although Ethiopia’s neonatal mortality rate has declined from 49 to 25 deaths per 1,000 live births between 2000 and 2025, it remains a persistent public health challenge. Significant resource limitations for essential intrapartum fetal monitoring (ESS and ICF, 2025. EDHS 2024–25) exacerbate this burden.
Literature Review
Prevalence of Non-reassuring Fetal Heart Rate Patterns
A prospective observational study conducted in the tertiary hospital of Xiamen University of China found that the prevalence of non-reassuring fetal heart rate patterns was 11.5% among 44 cases from 384 pregnant women who were admitted for induction of labor, in which 19 cases underwent emergency C/S and 25 cases underwent instrumental deliveries (Lu et al., 2021).
In a retrospective cohort study conducted in a tertiary hospital in Nigeria, the prevalence of non-reassuring fetal heart rate patterns was 23.1% (Olumodeji et al., 2025). In Ethiopia, the prevalence of non-reassuring fetal heart rate patterns has been reported to range from 19.2% to 41.5% (Abasimel et al., 2025; Asnake et al., 2026; Fiseha et al., 2026; Yilak et al., 2026).
Factors Associated With Non-reassuring Fetal Heart Rate Patterns
A retrospective observational study conducted in China at the General Hospital of the Northern Theater Command of the Chinese People’s Liberation Army showed that maternal age was significantly associated with a non-reassuring fetal heart rate pattern (Shen et al., 2022). A retrospective cohort study conducted at the University Hospital in Helsinki, Finland, found that male fetal sex, nulliparity, and post-term pregnancy were significantly associated with non-reassuring fetal heart rate patterns (Tarvonen et al., 2021).
An institution-based cross-sectional study conducted in public hospitals in South Omo, Southern Ethiopia, showed that drinking alcohol, having obstetric complications, having no antenatal follow-up, having meconium-stained amniotic fluid, mothers who were not referred, and having a nuchal cord were significantly associated with a non-reassuring fetal heart rate pattern (Asnake et al., 2026).
A facility-based cross-sectional study conducted in public hospitals in the Woliata Zone, southern Ethiopia, showed that labor augmentation, referral from other healthcare facilities, primigravida status, and meconium-stained amniotic fluid were significantly associated with a non-reassuring fetal heart rate pattern (Fiseha et al., 2026). In a study conducted in the Southern part of Ethiopia in Hadiya Zone public hospitals, factors such as a gestational age of less than 34 weeks, Apgar score at five minutes and one minute, and multiparity were associated with non-reassuring fetal heart rate patterns (Meskele et al., 2021).
This study assessed the associations of other variables, such as blood-stained amniotic fluid, with non-reassuring fetal heart rate patterns in addition to those assessed in other studies. Even in cases of non-reassuring fetal heart rate patterns, few studies have been conducted in our country, and no research evidence has been reported in the study area.
In Ethiopia, the true prevalence and contributing factors of non-reassuring fetal heart rate patterns during labor are poorly understood, with limited local research available. Recognizing the crucial role of this knowledge in preventing NRFHRP and its complications, this study aimed to determine the prevalence of NRFHRP and identify the associated factors among women in labor in public hospitals.
Methods and Materials
Study Area, Period, and Design
A facility-based cross-sectional study was conducted at the West Guji Hospital in the Oromia Region of Southern Ethiopia. The West Guji zone is located in the southern Oromia region. The capital city of the West Guji zone is Bule Hora, located 467 km from Addis Ababa. It is located at 5°35′ N latitude and 38°15′ E longitude, at an altitude of 1716 m above sea level. The zone has one teaching hospital, two primary hospitals, 42 health centers, and 166 health posts. The zone has a total population of 1,428,109, of whom 712,627 are men and 715,482 are women. The total number of pregnant women in the zone is 4,955 (West Guji Zone Health Bureau, 2022). The study was conducted from April 15 to June 15, 2024.
Population
The source population included all laboring women admitted to West Guji hospitals, whereas the study population included laboring women admitted to West Guji hospitals during the study period.
Inclusion Criteria and Exclusion Criteria
All laboring women who were admitted to West Guji hospitals with living fetuses were included in the study, while those who were mentally and critically ill were excluded from the study.
Sample Size Determination
The sample size was calculated using Epi Info software 7.2.2.6 by considering the double population proportion formula with the following parameters: 95% CI, power 80%, odds ratio 2.72, ratio 1, and percentage of the unexposed group among primigravida was 8.1% (Kassahun et al., 2020). After assuming a 10% non-response rate, the final sample size was 361 participants.
Sampling Procedure
All hospitals in the West Guji Zone were included in this study. The hospitals were Teaching Hospital, Kercha Primary Hospital, and Melka Soda Primary Hospital. First, the average number of laboring women admitted over the past two months in all hospitals was estimated based on six months of records from the registration book.
The study participants were proportionally distributed among the three hospitals based on two-month labor averages: 271 for Teaching Hospital, 48 for Kercha Hospital, and 42 for Melka Soda Primary Hospital. Systematic sampling was conducted using a k-interval of two. After selecting the first participant by lottery, every second woman was enrolled until the target sample size was reached.
Data Collection Techniques and Instruments
Data were collected through face-to-face interviews by three bachelor’s degree nurses using structured, pretested, and adapted questionnaires (Meskele et al., 2021). Before data collection, two-day training was provided by the principal investigator to the data collectors, highlighting the study objectives, information confidentiality, and data collection protocols. All interviews were conducted in Afan Oromo and translated by language experts. The tools included sociodemographic, obstetric, and other factors. Diagnoses and other necessary investigations were collected from chart reviews using a checklist. The principal investigator supervised the data collection. We collected data during the postpartum period in a private setting, once the mother was stable.
Study Variables
Dependent Variables
Non-reassuring fetal heart rate patterns.
Independent Variables
Operational Definition
Data Quality Control
The questionnaire was developed in English, translated into Afan Oromo, and back-translated into English by language experts to maintain consistency. Before the study, data collectors and supervisors underwent one day of intensive training on the research protocol and standardized fetal heart rate diagnostic criteria. A pre-test was conducted on 5% of the sample outside the study area. Based on the results, the tool was refined by adding variables (onset of labor), modifying skip patterns, and improving the overall layout to align with observer interpretations.
To minimize inter-observer variability, the clinical variables were recorded using objective operational definitions. The principal investigator and supervisors performed daily audits of the completed forms to ensure accuracy. Any identified errors, ambiguities, or missing data were discussed and resolved through daily debriefings.
Data Processing and Analysis
Data quality was ensured through rigorous checks for completeness, consistency, and accuracy before being entered into Epi-Data version 4.6. All subsequent cleaning and statistical analyses were conducted using IBM SPSS version 25. Descriptive statistics, including frequencies, percentages, and medians with interquartile ranges (IQR), were used to summarize the study population. A two-stage logistic regression approach was used to identify factors associated with non-reassuring fetal heart rate patterns. Initially, bivariable analysis was performed to screen candidate variables; those with a p-value of less than 0.25 were then included in the multivariable logistic regression model.
In addition to the evidence from the prior literature, covariates were chosen based on their potential biological impact. Factors such as meconium-stained amniotic fluid and labor augmentation were considered.
The strength of the associations was quantified using crude and adjusted odds ratios (AOR) with 95% confidence intervals (CI). Prior to the final multivariable analysis, multicollinearity was assessed using the Variance Inflation Factor (VIF), with all values remaining below 4, indicating no significant correlation between the independent variables. The goodness of fit of the model was confirmed using the Hosmer-Lemeshow test (p > 0.05). Statistical significance was set at p < 0.05, and the findings are presented through a combination of text, tables, and figures.
Results
Sociodemographic Characteristics of Laboring Women
A total of 361 women in labor were included in this study, with a 100% response rate. Among the total sample, 210 (58.2%) were in the 15–25-year age group. The median age of the study participants was 25 (+6 interquartile range [IQR]) years.
Socio-Demographic Profile of Participants, West Guji, Southern Ethiopia

*- Others: Divorced, Widowed.
Antepartum Characteristics of the Respondents
Obstetric Profiles of Participants in West Guji, Southern Ethiopia
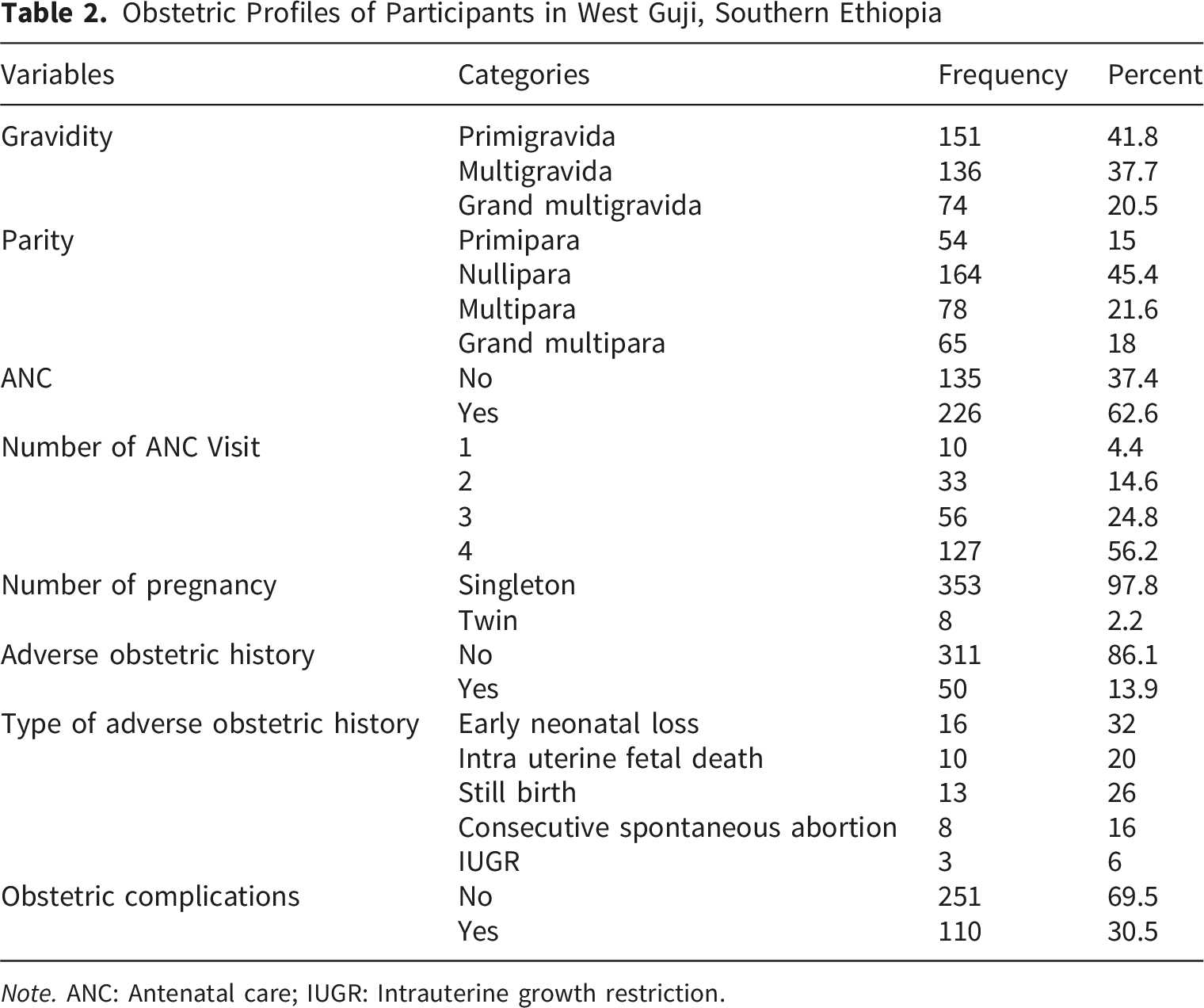
Note. ANC: Antenatal care; IUGR: Intrauterine growth restriction.
Type of Obstetric Complications
Approximately 42 (38.2%) of the laboring women had premature rupture of membranes, and 28 (25.5%) had oligohydramnios (Figure 1). Obstetric complications among laboring women in West Guji, Southern Ethiopia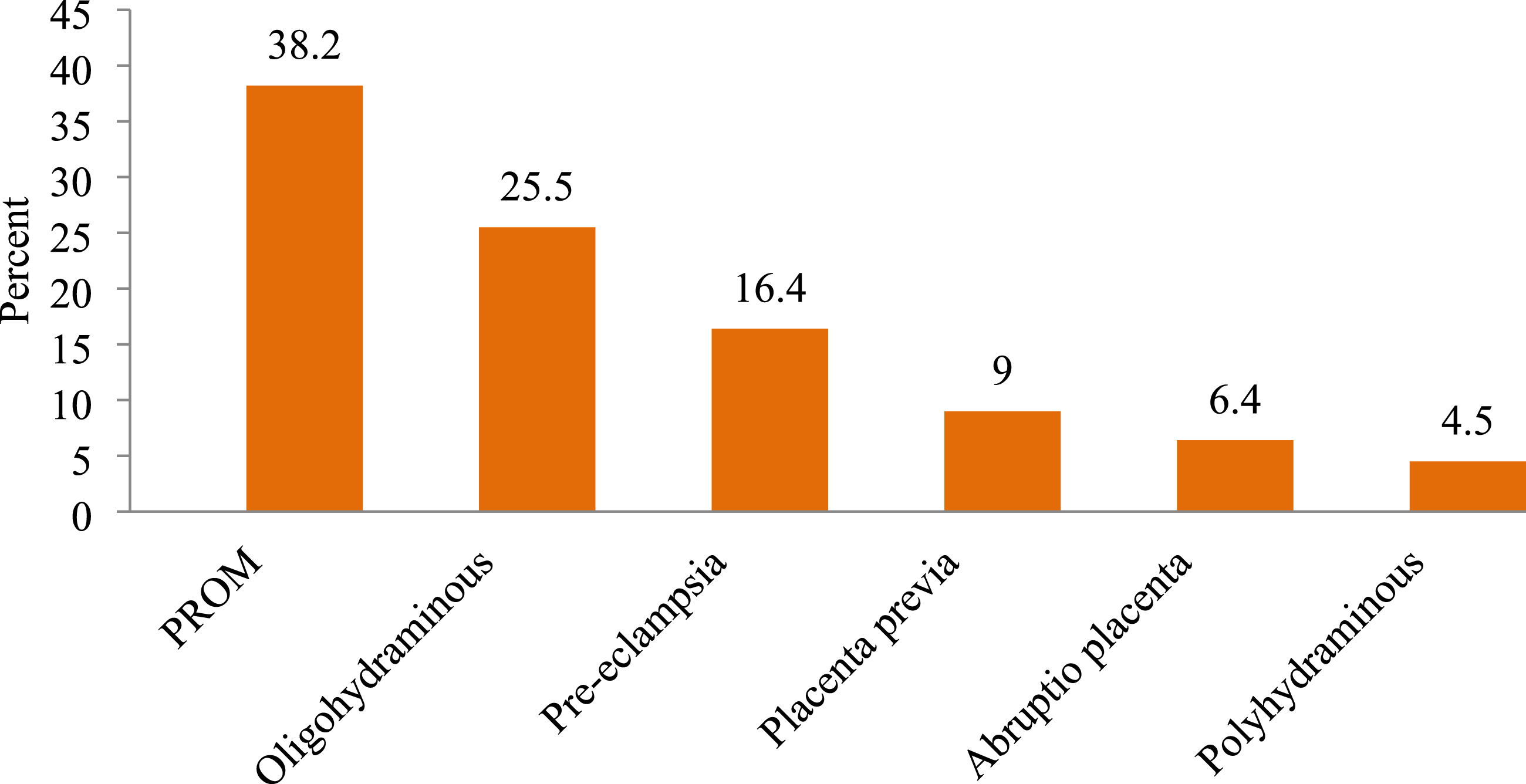
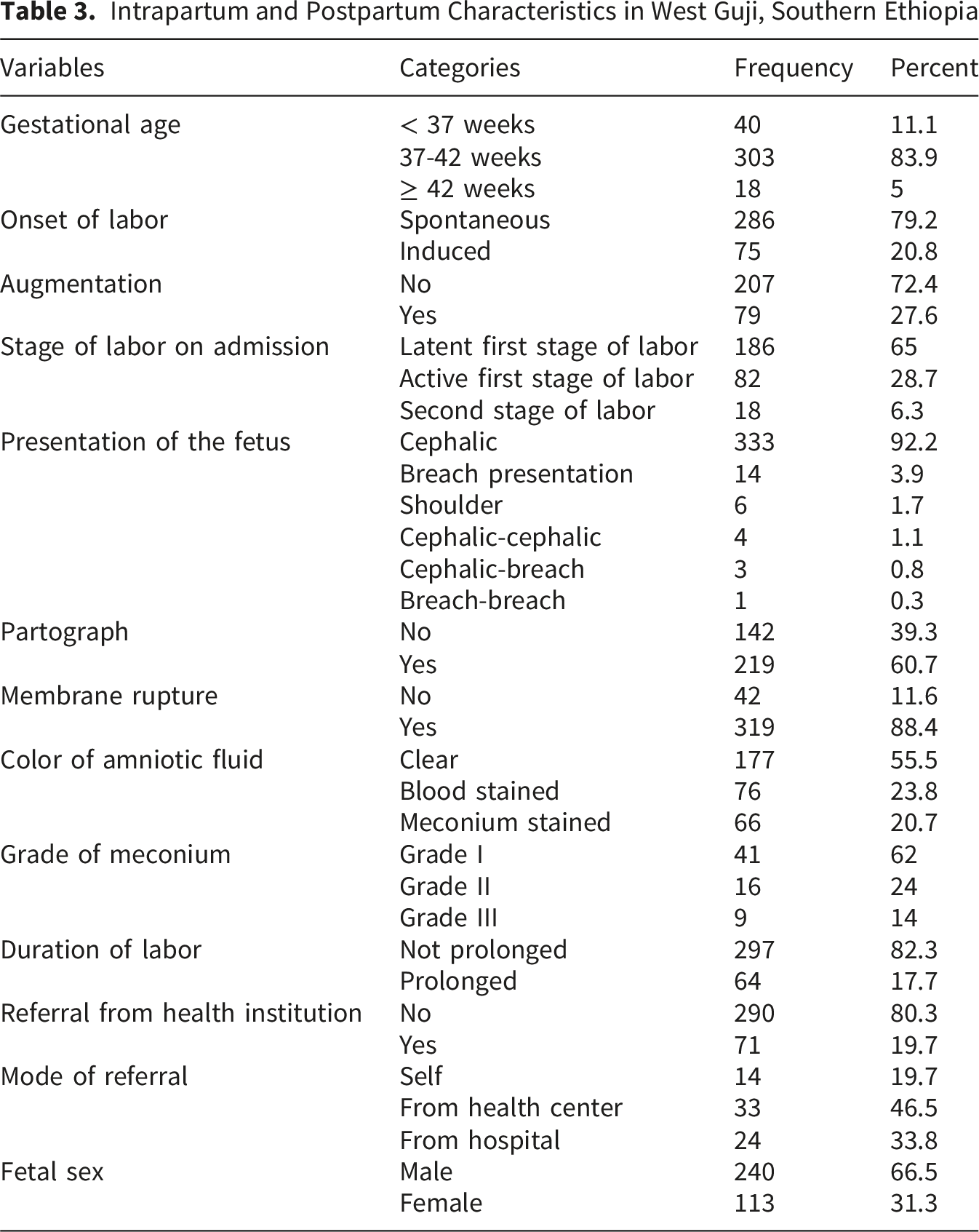
Intrapartum and Postpartum Characteristics of Laboring Women
The majority of women (83.9%) were at term. Most labors (79.2%) began spontaneously, whereas a smaller proportion (27.6%) were augmented. Nearly two-thirds of the women (65%) were admitted during the latent first stage of labor. The vast majority of women (92.2%) were admitted with cephalic presentation.
Intrapartum and Postpartum Characteristics in West Guji, Southern Ethiopia
Proportion of Non-reassuring Fetal Heart Rate Patterns
According to this study, the proportion of NRFHRP was 78 (21.6%, 95% CI=17.5–26.2). The most common non-reassuring fetal heart rate patterns detected were bradycardia (51, 65.4%) and tachycardia (27, 34.6%).
Factors Associated With the Non-reassuring Fetal Heart Rate Patterns
The bivariable analysis identified several factors as candidates for multivariable logistic regression, including the onset and duration of labor, referrals from other health facilities, obstetric complications, color of amniotic fluid, use of a partograph, labor augmentation, antenatal follow-up, gravidity, parity, educational status, and medical illnesses, with a p-value of less than 0.25.
Multivariate analysis revealed that referral from other health facilities, blood-stained amniotic fluid, meconium-stained amniotic fluid, augmentation, and prolonged labor were significantly associated with non-reassuring fetal heart rate patterns (p < 0.05). Multivariable analysis revealed that referrals from other health facilities were significantly associated with non-reassuring fetal heart rate patterns.
The odds of non-reassuring fetal heart rate patterns were 5.19 times greater among laboring women referred from other health facilities than among women who were directly admitted to the facility (AOR = 5.19, 95% CI: 2.27-11.90).
This study revealed that blood- and meconium-stained amniotic fluid was significantly associated with non-reassuring fetal heart rate patterns. Women with blood-stained and meconium-stained amniotic fluid were 3.55 and 3.87 times more likely to develop a non-reassuring fetal heart pattern than their counterparts (AOR = 3.55, 95% CI: 1.45-8.68 and AOR = 3.87, 95% CI: 1.68-8.89), respectively. Similarly, undergoing labor augmentation and experiencing prolonged labor were both significantly associated with non-reassuring fetal heart rate patterns.
Logistic Regression Analysis of Factors Associated With Non-reassuring Fetal Heart Rate Patterns in West Guji, Southern Ethiopia
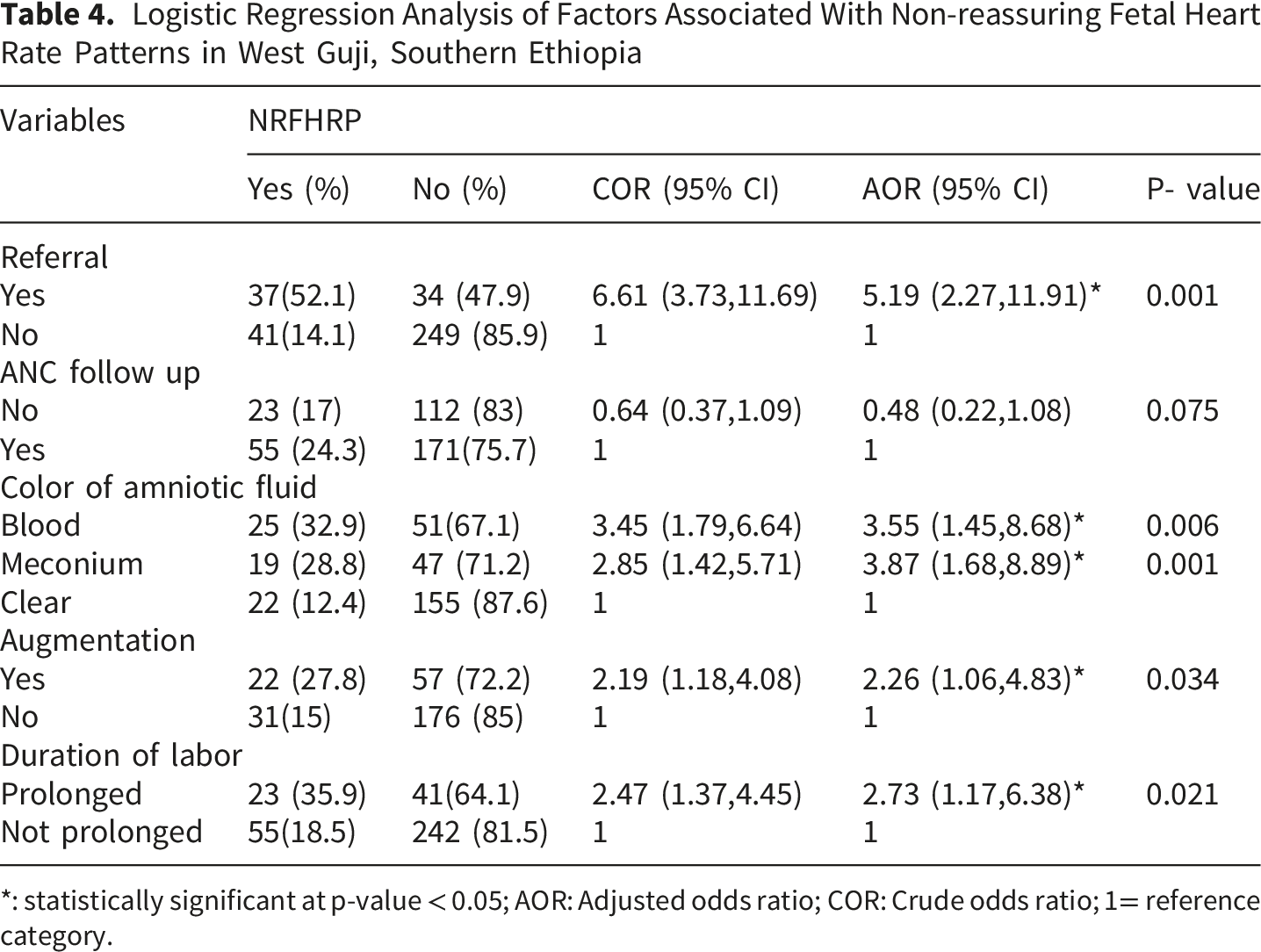
*: statistically significant at p-value < 0.05; AOR: Adjusted odds ratio; COR: Crude odds ratio; 1= reference category.
Discussion
This study was conducted to assess the prevalence of non-reassuring fetal heart rate patterns and associated factors among laboring women admitted to West Guji public hospitals. The findings from the current study revealed that the prevalence of non-reassuring fetal heart rate patterns was 78 (21.6%; 95% CI = 17.5-26.2). These findings align closely with other cross-sectional studies from similar clinical settings in Ethiopia, which reported comparable prevalence rates: 24.6% in Northwest Ethiopia (Abate et al., 2021), 22.4% in Jigjiga Public Hospitals (Abasimel et al., 2025), and 19.2% in Wolaita Zone, Southern Ethiopia (Fiseha et al., 2026).
The current findings are greater than those of studies performed in China (11.5%) (Lu et al., 2021) and southern public hospitals in Ethiopia (41.5%) (Asnake et al., 2026). This disparity might be explained by differences in sociodemographic characteristics, accessibility of health services, and study settings.
Our analysis identified a statistically significant link between the occurrence of non-reassuring fetal heart rate patterns and several factors, including facility referral, amniotic fluid staining (blood or meconium), augmentation, and prolonged labor.
Referrals from other healthcare facilities were significantly associated with non-reassuring fetal heart rate patterns. This finding is aligned with recent research conducted in the Wolaita Zone of Southern Ethiopia (Fiseha et al., 2026). The Ethiopian Ministry of Health has developed and implemented a referral system to establish a network of primary healthcare facilities. Research in Ethiopia’s agrarian regions reveals that 95% of referral cases lack pre-referral communication. Consequently, laborers often arrive at health facilities without confirming the availability of services, leading to further delays that may contribute to non-reassuring fetal heart rate patterns (Hailemichael et al., 2021).
Meconium-stained amniotic fluid significantly increased the odds of non-reassuring fetal heart rate patterns compared to clear amniotic fluid. This finding agrees with the findings in Ethiopia (Abasimel et al., 2025, and Asnake et al., 2026). This might be because fetal heart rate abnormalities often signal hypoxia, which increases intestinal activity and relaxes the anal sphincter, leading to meconium passage. As a foreign substance, meconium can inflame fetal lung tissue, the chorionic plate, and umbilical vessels, further contributing to fetal heart rate abnormalities and potential complications during labor and delivery (Mwaihabi et al., 2026).
The odds of exhibiting non-reassuring fetal heart rate patterns were significantly higher among mothers who underwent labor augmentation than among those who did not. This finding is consistent with that of a study conducted in West Gojjam, Ethiopia (Kassahun et al., 2020). Augmentation is the artificial stimulation of uterine contractions using oxytocin. Oxytocin causes uterine hyperstimulation, resulting in alterations in uteroplacental perfusion. A decrease in blood flow to the fetus leads to hypoxemia and disturbance of the fetal heart rate (Sciscione, 2020). This may also be due to maternal psychological disturbance as her labor was stimulated artificially by medication and the drop rate was not correctly adjusted.
Mothers who experienced prolonged labor were significantly more likely to manifest non-reassuring fetal heart rate patterns than those with normal labor durations. Prolonged labor is an intrapartum obstetric complication that arises when the combined duration of the first and second stages of labor exceeds 18 h. This may be due to malpresentation/malposition, cephalopelvic disproportion, and inadequate uterine contractions. This causes compression of the presenting part of the fetus against the lower uterine segment, resulting in utero-placental insufficiency. This leads to non-reassuring fetal heart rate patterns (Purandare, 2024).
In this study, blood-stained amniotic fluid was significantly associated with non-reassuring fetal heart rate patterns. Blood-stained amniotic fluid following rupture of membranes is a critical indicator of fetal compromise, often reflecting underlying placental abnormalities such as premature separation or abnormal attachment. These conditions lead to uteroplacental insufficiency, which triggers fetal distress. Notably, in cases of retroplacental abruption, blood-stained fluid may serve as the sole clinical sign of placental separation in the absence of other overt symptoms (Purandare, 2024). The inability to differentiate blood-stained amniotic fluid from a bloody show early on results in non-reassuring fetal heart rate patterns, as blood-stained amniotic fluid requires intervention.
Limitations of the Study
This study had several limitations. First, its hospital-based scope may overlook different patterns in lower-level facilities or home deliveries, which limits generalizability of the findings. Methodologically, reliance on intermittent auscultation rather than continuous CTG monitoring may have resulted in missed non-reassuring heart rate patterns and introduced subjective measurement variability. Finally, the cross-sectional design precluded the establishment of definitive cause-and-effect relationships.
Nursing Implications for Practice
This study provides valuable insights for maternal and child health policymakers. Close feto-maternal monitoring during labor is vital for mitigating non-reassuring fetal heart rate patterns, as all laboring mothers are at high risk. Nurses/midwives must note the amniotic fluid color and document/report the findings.
Conclusion
The findings of this study indicate that the prevalence of non-reassuring fetal heart rate patterns was somewhat higher than that in other local studies. Obstetric and other factors were associated with non-reassuring fetal heart rate patterns. Referrals from other health facilities, blood-stained amniotic fluid, meconium-stained amniotic fluid, augmentation, and prolonged labor were associated with non-reassuring fetal heart rate patterns.
Supplemental Material
Supplemental material -Non-Reassuring Fetal Heart Rate Patterns and Key Contributing Factors in West Guji Zone, Southern Ethiopia: Facility-Based Cross-Sectional Study
Supplemental material for Non-Reassuring Fetal Heart Rate Patterns and Key Contributing Factors in West Guji Zone, Southern Ethiopia: Facility-Based Cross-Sectional Study by Ahmedteyib Jemalo Mohammed, Girma Tufa Melesse, Geroma Morka, Belda Negesa Beyene in Sage Open Nursing
Footnotes
Ethical Considerations
Ethics approval was obtained from the institutional review board (IRB) of Bule Hora University (Ref. no.: BHU/RDP/799/2014). Permission was obtained from all hospitals' chief executive officers. The goals, procedures, risks, and benefits of the study were explained to the participants. Prior to the interview, the selected participants confirmed their desire to participate in the study by providing their informed written consent. Names were left out of the written questionnaire to maintain confidentiality. In addition, the research participants were guaranteed that their choice to withdraw from the study or withhold consent would not carry any repercussions.
Authors Contribution
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors affirm that the data supporting the findings of this study are available in the article and its supplementary material.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.