
Abstract
Background
Digital health technologies are increasingly embedded in Neonatal Intensive Care Units (NICUs), yet the role of nurse-led governance in shaping safe, sustainable implementation for high-risk neonates remains underexplored. This review synthesized evidence on nursing leadership and digital health integration in NICUs.
Methods
Following PRISMA 2020, six databases were searched (January 2013–January 2025), supplemented by grey literature, reference-list screening, and forward citation tracking. The protocol was prospectively registered with PROSPERO. Eligible empirical studies (n = 18) addressed formal nurse-led governance, operational governance enactment by nurses, or leadership-relevant determinants. Risk of bias was appraised with design-specific tools (Cochrane RoB 2, ROBINS-I, JBI, MMAT); synthesis combined structured narrative and reflexive thematic analysis.
Results
Findings are presented as associations, not causal effects. Favorable signals included a 60% reduction in high-stage device-related pressure injuries in one quality-improvement initiative; 30-day readmission rates of 13.8% among enrolled versus 30.9% among non-enrolled caregivers in a nurse-led post-discharge telehealth intervention; and an approximately 12-day shorter length of stay favoring the intervention in one randomized trial of nurse-led developmental care. Using conservative, author-reported coding, organizational/leadership support (17/18; 94%) and structured training (8/18; 44%) were most frequently documented; funding/IT (22%) and clinical champions (17%) less so. Nurse-led governance could not be statistically separated from co-occurring implementation activities.
Conclusion
Across a predominantly observational, low-to-moderate-certainty evidence base, nurse-led governance was consistently associated with stronger implementation processes and selected family- and clinical-level signals when embedded in coordinated training, workflow redesign, and audit-and-feedback. Findings are hypothesis-generating. Comparative-effectiveness and economic evaluations decomposing leadership from co-occurring implementation components are needed.
Introduction
Neonatal deaths remain stubbornly high, at approximately 2.3 million annually, and now comprise nearly half of global under-five mortality (Lawn et al., 2023). Although under-five mortality has fallen, neonatal mortality has declined more slowly, from 37 to 17 per 1,000 live births between 1990 and 2023 (Huang et al., 2025; Çeri et al., 2025). Risk is concentrated among NICU-admitted infants with prematurity, congenital anomalies, and critical illness, where care complexity, rapid physiological change (Enyew et al., 2025), and time-critical decisions demand both advanced technology and strong organizational leadership (Tan et al., 2025). As the largest continuous-care workforce in NICUs, nurses integrate physiologic data, device outputs, and family-centered care at the bedside, positioning nursing leadership as a fulcrum for translating technology into outcomes (Hu et al., 2025).
Digital NICU capabilities now span telehealth/telemedicine, electronic health records (EHRs) with clinical decision support, artificial intelligence/machine learning (AI/ML) for predictive analytics, remote monitoring, and neuromonitoring (aEEG, NIRS, cEEG) (Duci et al., 2025; Meeus et al., 2024). AI/ML can forecast conditions such as sepsis and necrotizing enterocolitis days before onset (Fang & Chuo, 2021); telemedicine extends subspecialty expertise and reduces avoidable transfers (Jagarapu & Savani, 2021); neuromonitoring enables real-time cerebral assessment (Jagarapu & Savani, 2021); and tele-ophthalmology programs, often with nurse-performed imaging, expand retinopathy of prematurity (ROP) screening (Luo et al., 2025). Yet technical deployment alone is insufficient: high-fidelity, sustained integration depends on leadership that establishes evidence-based protocols, builds competence through structured training, aligns workflows, secures infrastructure and policy support, and cultivates a safety-first innovation culture (Wei et al., 2025).
Leadership approaches central to digital transformation include transformational leadership, shared governance, and dyadic leadership models that link medical and nursing co-leads (Conte et al., 2023; Ramadan et al., 2024). Operational levers include appointing clinical champions, conducting audits and providing feedback, redesigning workflows, establishing clear standard operating procedures, and implementing iterative Plan-Do-Study-Act cycles (Sinha, 2024). Qualitative evidence shows that nurses perceive AI as enhancing clinical judgment (93.9%) when paired with human validation, with success contingent on infrastructure (97.0%), training (90.9%), and policy clarity (84.8%) (Alruwaili et al., 2025b). Persistent barriers, technical failures, alert fatigue, EHR integration gaps, staffing constraints, and culture-based resistance underscore the leadership mandate to balance innovation with safety, efficiency, and workforce well-being (van Houwelingen et al., 2024).
Despite rapid digitization, the core research problem is that NICUs lack consolidated, evidence-informed guidance on which nursing leadership models and actions most reliably support the safe, equitable, and sustainable implementation of digital technologies. Existing evidence on how nursing leadership shapes implementation fidelity, adoption, and sustainability, and how leadership functions interact with co-occurring implementation activities to translate digital investments into clinical, family, and workforce outcomes, remains fragmented across disciplines and technologies (Laakkonen et al., 2024). This gap is consequential because poorly governed digital change can amplify workload, alert fatigue, and safety risks, while widening inequities in access and family engagement. Broader literature from other high-stakes healthcare contexts similarly highlights the importance of leadership competencies and ethical governance for complex system change (Alruwaili et al., 2025a; Fischer et al., 2024; Grimell & Nilsson, 2020; Malterud et al., 2016; Ramadan, Aldousari, et al., 2025; Ramadan, Alshammari, et al., 2025).
This review addressed that gap by: (1) identifying nursing leadership models, strategies, and actions used to integrate digital health in NICUs; (2) cataloging implemented technologies and workflow integration approaches; (3) mapping implementation frameworks and evidence-based strategies; (4) examining associations between leadership approaches and implementation, clinical, and family/workforce outcomes; and (5) distilling facilitators, barriers, and best practices for nursing-led digital transformation in neonatal intensive care. Practically, the review was intended to provide nurse leaders, NICU managers, educators, and policymakers with actionable levers for planning, staffing, training, and evaluating digital NICU transformation.
Methods
Search Strategy and Selection Criteria
This review followed the PRISMA 2020 guidelines, and the protocol was registered with PROSPERO prior to data extraction (CRD420251161936). The review question was framed using PICO: in NICUs caring for high-risk neonates (i.e., neonates requiring Level II–IV NICU care such as preterm and/or very low birthweight infants and those with significant respiratory, cardiovascular, neurologic, surgical, or infectious morbidity), which nursing leadership models or strategies, compared with usual practice or standard governance where applicable, are associated with digital health implementation and clinical/family outcomes?
Search Strategy Overview by Database
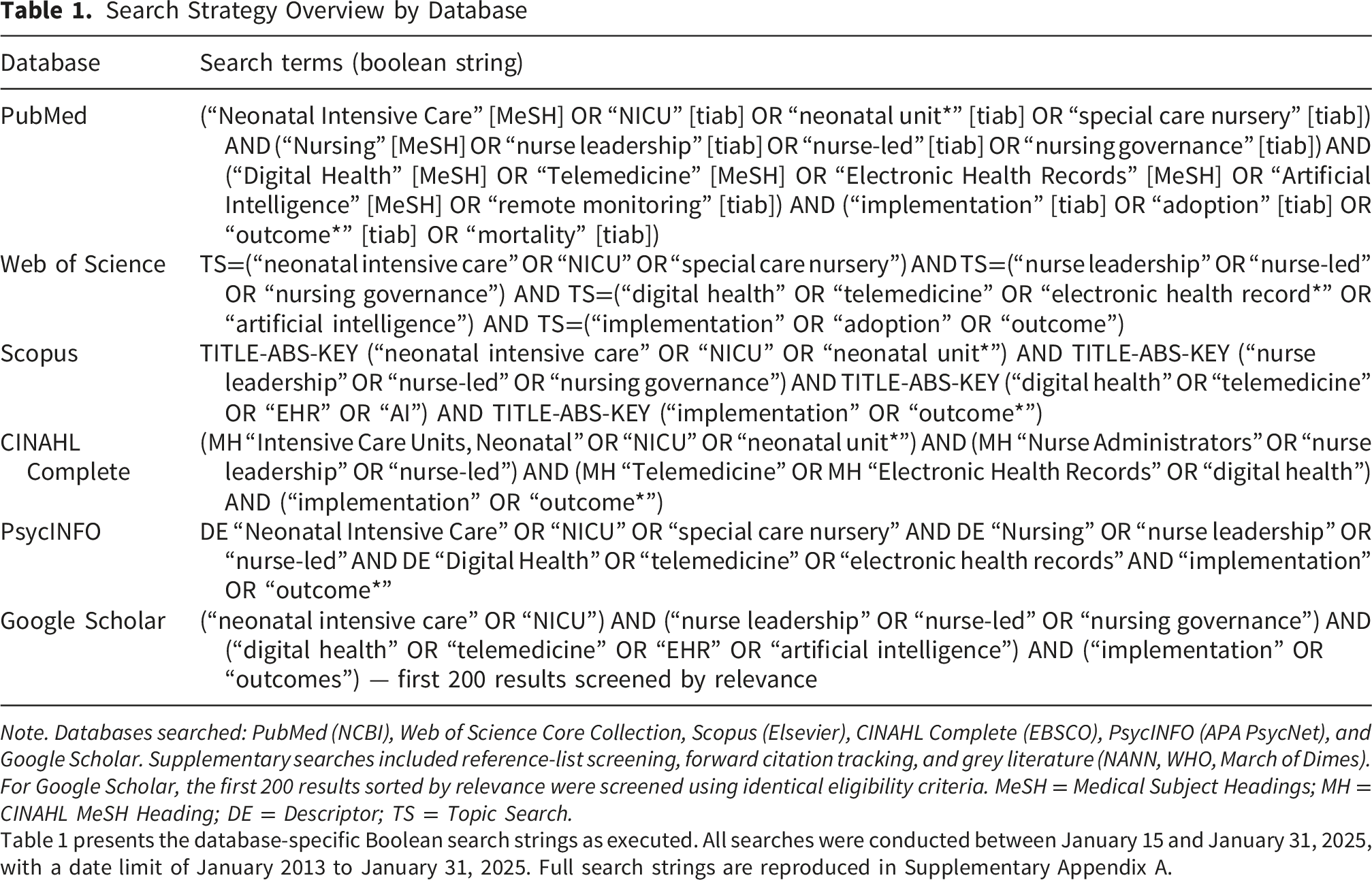
Note. Databases searched: PubMed (NCBI), Web of Science Core Collection, Scopus (Elsevier), CINAHL Complete (EBSCO), PsycINFO (APA PsycNet), and Google Scholar. Supplementary searches included reference-list screening, forward citation tracking, and grey literature (NANN, WHO, March of Dimes). For Google Scholar, the first 200 results sorted by relevance were screened using identical eligibility criteria. MeSH = Medical Subject Headings; MH = CINAHL MeSH Heading; DE = Descriptor; TS = Topic Search.
Table 1 presents the database-specific Boolean search strings as executed. All searches were conducted between January 15 and January 31, 2025, with a date limit of January 2013 to January 31, 2025. Full search strings are reproduced in Supplementary Appendix A.
Eligibility Criteria
Eligible studies were original empirical research (quantitative, qualitative, or mixed-methods) conducted in Level II–IV NICUs. Studies were included if they involved neonates (<28 days) or NICU-treated infants beyond 28 days, with the sample remaining NICU-specific and high-acuity. For this review, “high-risk neonates” were operationalized as neonates (<28 days) or NICU-treated infants requiring intensive care because of prematurity and/or low birthweight, need for respiratory/cardiovascular support, or significant medical/surgical conditions (e.g., sepsis, necrotizing enterocolitis, hypoxic-ischemic encephalopathy, major congenital anomalies). Eligible studies were further required to satisfy at least one of three prespecified leadership/governance tiers: Tier 1: formal nurse-led governance structures (e.g., shared-governance councils, nursing informatics governance committees, nursing leadership dyads, advanced practice nurse-led services); Tier 2: operational governance enactment, defined as discrete, authority-bearing leadership actions undertaken by nurses with primary or co-primary decision authority over implementation (e.g., nurse-led champion programs, nurse-led training and competency systems, nurse-led workflow redesign with formal sign-off, nurse-led protocol development with audit-and-feedback); or Tier 3: leadership-relevant determinants with direct implications for nurse-led governance and digital implementation (e.g., NICU work environment and manager support as predictors of safety attitudes, e-health literacy, AI readiness, digital competence, and organizational culture). In addition, eligible studies (i) involved clinically integrated technologies (e.g., EHR/clinical decision support, telehealth, AI/ML, remote monitoring, digital assessment tools) and (ii) reported at least one implementation outcome (e.g., adoption, fidelity, acceptability, sustainability), clinical outcome (e.g., mortality, morbidity, length of stay, complications), or family/workforce outcome (e.g., satisfaction, stress/burnout, engagement).
Studies were required to be published in English, available in full text, and published between January 2013 and January 31, 2025. Studies were excluded when limited to adult populations or non-NICU pediatric ICUs without NICU-specific data; focused on administrative-only technologies without clinical integration; or lacked either an explicit nursing leadership/governance component (Tier 1 or 2) or a clearly articulated leadership-relevant determinant (Tier 3) with direct implications for nurse-led implementation and governance in NICU digital transformation.
Operational Definition of Nurse-Led Governance
For the purposes of this review, nurse-led governance was operationalized through a three-tier framework that explicitly distinguishes formal governance structures, operational governance enactment, and leadership-relevant determinants. Tier 1: Formal nurse-led governance structures: standing authority arrangements in which nurses hold or co-hold chartered responsibility for digital implementation decisions (e.g., shared-governance councils, nursing informatics governance committees, nursing leadership dyads, advanced practice nurse-led service models) formally.
Tier 2: Operational governance enactment: discrete, authority-bearing leadership actions that constitute governance in action when undertaken by nurses with primary or co-primary decision authority (e.g., designation and support of clinical champions, delivery of structured training programs, workflow redesign through nursing-led processes with formal sign-off, protocol development and monitoring, and systematic audit-and-feedback). Tier 3: Leadership-relevant determinants: empirically measured constructs that nurse leaders are accountable for shaping when planning and resourcing digital implementations (e.g., NICU work environment, manager support, e-health literacy, AI readiness). The distinction between Tier 2 and broader implementation activities is operationalized as decision authority: governance is coded only when nurses held primary or co-primary authority over implementation decisions (planning, sequencing, escalation, and sustainability), not merely when nurses delivered or participated in a particular activity. Each included study was tier-classified by two independent reviewers; the inclusion-justification matrix is reported in Supplemental Table B2.
Study Selection Summary
Two reviewers independently screened titles and abstracts, then full texts, using prespecified criteria. Disagreements were resolved through discussion, with adjudication by a third reviewer when consensus could not be reached. In accordance with PRISMA 2020, 3,847 records were identified from databases (no registers). After duplicate removal (n=987), 2,860 records were screened by title/abstract, and 2,482 were excluded. Full texts were retrieved for 378 reports and assessed for eligibility; 360 were excluded for prespecified reasons (wrong population, n=152; no nursing leadership/governance component or leadership-relevant determinant, n=98; wrong intervention, n=73; wrong outcomes, n=37). Eighteen studies met the inclusion criteria and were retained for synthesis (Figure 1). Included studies were Asturias et al. (2022), Ayed et al. (2025), Bilodeau et al. (2024), Gross et al. (2020), Jalali et al. (2022), Kilcullen et al. (2020), Mousavi et al. (2025), Moyer et al. (2022), Olgun et al. (2024), Öz et al. (2024), Ramadan, Elsharkawy, et al. (2025), Rezende et al. (2016), Sarik et al. (2022), Shade et al. (2017), Unver and Isik (2024), Vazquez and Bell (2024), Willard et al. (2018), and Wong (2013). PRISMA flow diagram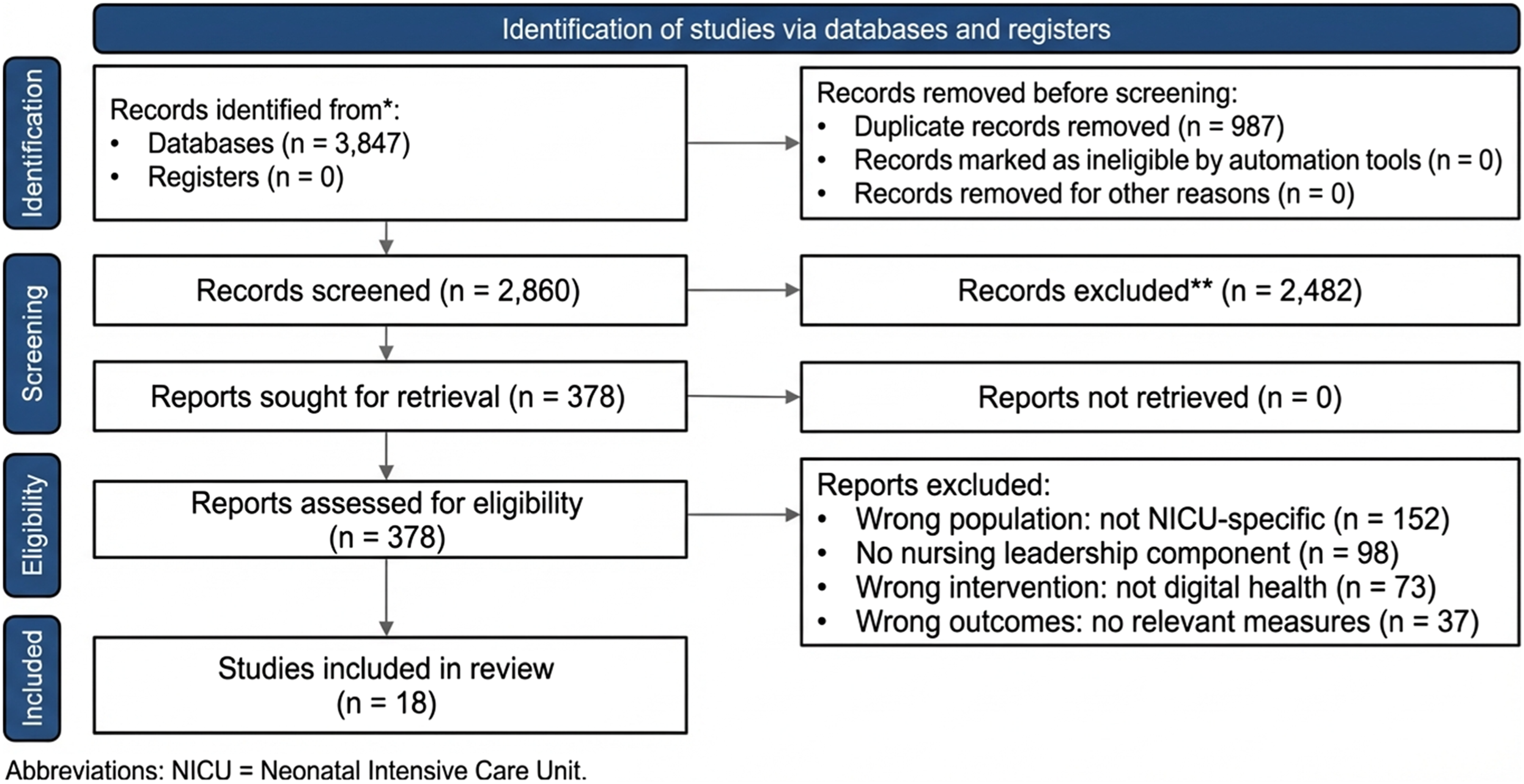
Data Extraction Process
Two independent reviewers performed systematic data extraction using a standardized template, which was piloted on three studies. Discrepancies were resolved through discussion, with consultation of a third reviewer when consensus proved elusive. The extraction framework encompassed eight domains:
Quality Assessment
Methodological quality was assessed using design-specific tools. RCTs were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool across five domains: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting. Quasi-experimental studies were evaluated using ROBINS-I across seven domains: confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and selective reporting. Cross-sectional studies were assessed using the JBI Critical Appraisal Checklist, focusing on sampling/setting clarity, measurement validity and reliability, confounding identification/management, and analytic appropriateness. Mixed-methods studies were assessed using the Mixed Methods Appraisal Tool (MMAT), focusing on the mixed-methods rationale, integration quality, interpretation of convergence/divergence, and component-level methodological rigor. Two reviewers independently appraised each study; initial inter-rater agreement before consensus discussion was 82%, and all disagreements were resolved through structured consensus using prespecified decision rules prior to analysis. Studies were categorized as low, moderate, or high/serious risk of bias, and these ratings informed the interpretation of findings.
Data Analysis
Narrative Synthesis
Meta-analysis was infeasible due to heterogeneity in interventions, populations, and outcomes. Instead, a structured narrative synthesis, following Popay’s framework, was used to systematically compare findings. Quantitative outcomes were tabulated alongside intervention characteristics, sample sizes, effect estimates (with 95% CIs where available), and statistical significance. To convey directionality transparently, each quantitative outcome was coded as favorable, unfavorable, or null based on the authors’ reported comparisons, and these patterns were summarised within the Results narrative.
Thematic Analysis
Qualitative and mixed-methods findings underwent reflexive thematic analysis using Braun and Clarke’s six-phase approach: familiarization through iterative reading; systematic feature coding; code collation into potential themes; theme review against coded extracts and the complete dataset; theme definition and scope refinement; and synthesis with exemplar quotes. Initial coding generated 127 codes, subsequently organized into 15 sub-themes within four overarching themes: (1) leadership as change catalyst (vision-setting, culture transformation, stakeholder engagement); (2) technology–workflow integration challenges (alert fatigue, documentation burden, system interoperability); (3) workforce readiness (digital literacy, training adequacy, role evolution); and (4) sustainability factors (resource allocation, policy support, continuous improvement cycles).
Integration
A convergent-segregated approach enabled independent quantitative and qualitative syntheses before interpretive integration. Qualitative themes contextualized quantitative outcomes, elucidating mechanisms of intervention success and failure. Discordant findings between effect sizes and experiential data were explicitly examined to capture implementation complexity. Throughout the synthesis, the tier classification (Tier 1/2/3) was used to differentiate findings ascribable to formal nurse-led governance arrangements (Tier 1) from those embedded within broader nurse-engaged implementation processes (Tier 2) and from associations between leadership-relevant determinants and outcomes (Tier 3). This integrative approach revealed that quantitative improvements often co-existed with qualitative challenges, while some interventions that showed null effects generated substantial qualitative benefits through unmeasured pathways.
Results
Risk of Bias
Risk of bias was assessed for the 18 included studies (Figure 2) using design-appropriate tools. Randomized controlled trials (RCTs) were appraised using Cochrane RoB 2 across five domains (randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting). ROBINS-I was used for quasi-experimental studies (confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and selective reporting). The JBI critical appraisal was applied to cross-sectional surveys (sampling/setting clarity, exposure and outcome measurement validity, confounding identification/management, and analytic appropriateness). MMAT was used for mixed-methods studies, emphasizing the strength of the mixed-methods rationale and the quality of integration and interpretation of convergence/divergence. Risk of bias assessment
Across the three RCTs, Olgun et al. (2024) and Bilodeau et al. (2024) were judged to be at low risk of bias, whereas Mousavi et al. (2025) raised some concerns, primarily related to missing outcome data, resulting in a moderate overall judgment. Among the six quasi-experimental studies, the overall risk was variable: Moyer et al. (2022) was judged low risk, while several pre–post/non-randomized evaluations were judged moderate risk, driven mainly by residual confounding and outcome measurement limitations. Asturias et al. (2022) could not be rated confidently overall because incomplete screening/coverage and missing-data concerns provided insufficient information to support a stable judgment. Cross-sectional surveys showed predictable observational limitations; the appraisal supported a low risk for Ayed et al. (2025) and moderate risk for the remaining surveys due to selection and/or measurement limitations. A mixed-methods appraisal showed the greatest variability: Kilcullen et al. (2020) and Rezende et al. (2016) were judged to be high risk due to weaknesses in methodological rigor and/or integration quality. Overall, Figure 2 summarizes the distribution as 22% low risk (n=4), 61% moderate risk (n=11), 11% high risk (n=2), and 6% insufficient information (n=1).
Certainty of evidence (GRADE): Given substantial heterogeneity in technologies, outcomes, and study designs, the certainty of evidence was judged overall as low for most clinical and implementation outcomes (primarily quasi-experimental and observational studies with moderate risk of bias). For selected family and training outcomes supported by randomized designs, certainty was judged as moderate, but imprecision and limited replication prevented high-certainty conclusions.
Main Outcomes
Study Characteristics, Tier Classification, and Key Findings (Streamlined Summary)
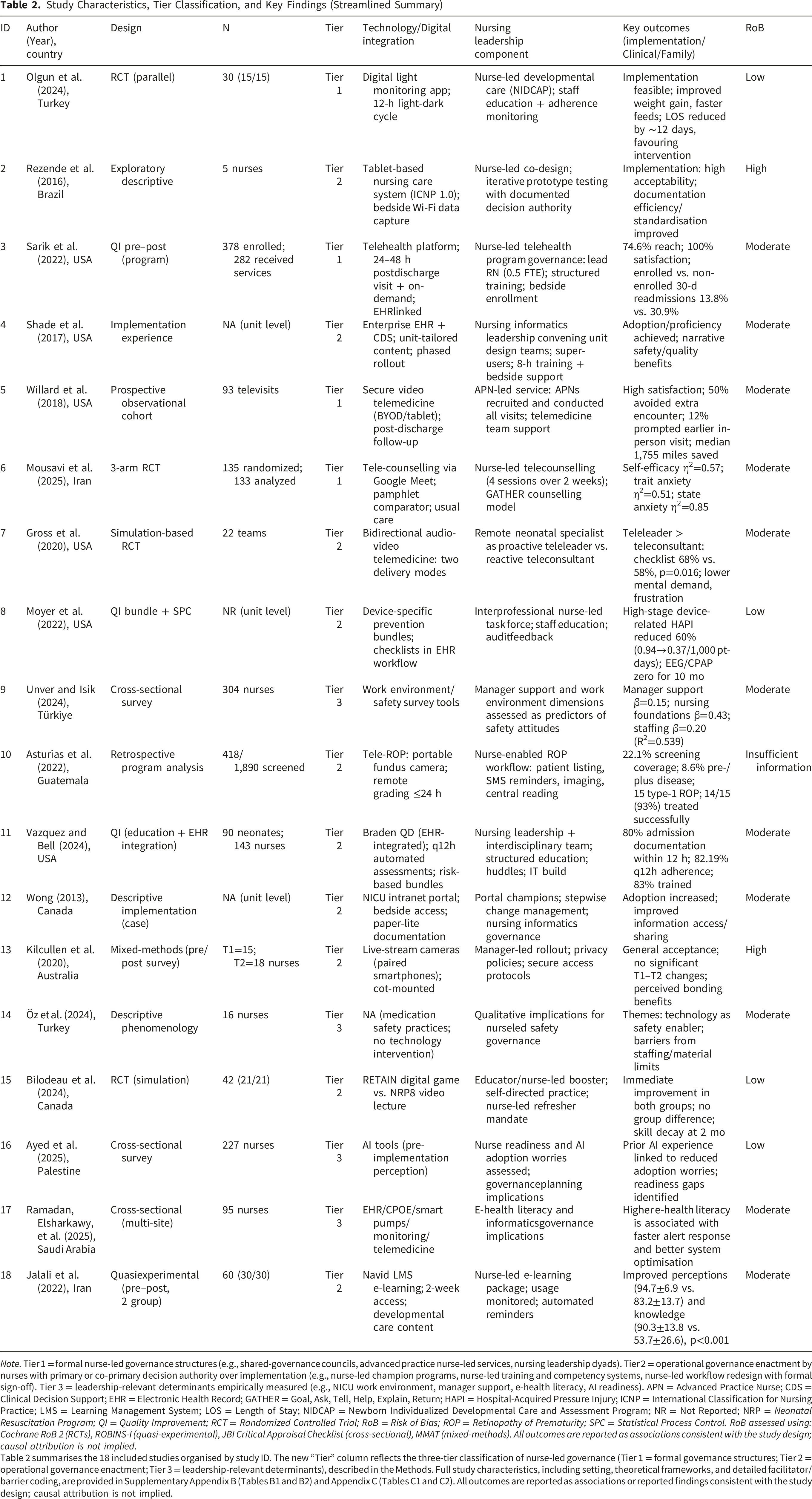
Note. Tier 1 = formal nurse-led governance structures (e.g., shared-governance councils, advanced practice nurse-led services, nursing leadership dyads). Tier 2 = operational governance enactment by nurses with primary or co-primary decision authority over implementation (e.g., nurse-led champion programs, nurse-led training and competency systems, nurse-led workflow redesign with formal sign-off). Tier 3 = leadership-relevant determinants empirically measured (e.g., NICU work environment, manager support, e-health literacy, AI readiness). APN = Advanced Practice Nurse; CDS = Clinical Decision Support; EHR = Electronic Health Record; GATHER = Goal, Ask, Tell, Help, Explain, Return; HAPI = Hospital-Acquired Pressure Injury; ICNP = International Classification for Nursing Practice; LMS = Learning Management System; LOS = Length of Stay; NIDCAP = Newborn Individualized Developmental Care and Assessment Program; NR = Not Reported; NRP = Neonatal Resuscitation Program; QI = Quality Improvement; RCT = Randomized Controlled Trial; RoB = Risk of Bias; ROP = Retinopathy of Prematurity; SPC = Statistical Process Control. RoB assessed using: Cochrane RoB 2 (RCTs), ROBINS-I (quasi-experimental), JBI Critical Appraisal Checklist (cross-sectional), MMAT (mixed-methods). All outcomes are reported as associations consistent with the study design; causal attribution is not implied.
Table 2 summarises the 18 included studies organised by study ID. The new “Tier” column reflects the three-tier classification of nurse-led governance (Tier 1 = formal governance structures; Tier 2 = operational governance enactment; Tier 3 = leadership-relevant determinants), described in the Methods. Full study characteristics, including setting, theoretical frameworks, and detailed facilitator/barrier coding, are provided in Supplementary Appendix B (Tables B1 and B2) and Appendix C (Tables C1 and C2). All outcomes are reported as associations or reported findings consistent with the study design; causal attribution is not implied.
Theme 1: Nurse-Led Governance Models and Digital Transformation
Four studies (22%) contributed Tier-1 evidence on formal nurse-led governance structures, and an additional six studies (33%) contributed Tier-2 evidence on operational governance enactment with documented decision authority within nurse-led implementation. In a nurse-led post-discharge telehealth program with a dedicated lead RN (0.5 FTE) and formal program governance (Tier 1), visit completion was reported at 74.6% (282/378), family satisfaction at 100%, and a contemporaneous comparison showed 30-day readmissions of 13.8% among enrolled versus 30.9% among non-enrolled caregivers (p<0.01); ED use within one month was also lower among enrolled families (Sarik et al., 2022). In an advanced practice nurse-led post-discharge telemedicine service (Tier 1; 93 visits), 78 issues were identified (medication 13%, respiratory 19%, feeding 33%, surgical 35%); 50% of caregivers were documented to have avoided an extra encounter and 12% to have received earlier intervention, with a median 1,755 miles saved per family (Willard et al., 2018). In a randomized trial of a nurse-led developmental care model using digital light monitoring (Tier 1), the intervention group showed greater daily weight gain (7.34±1.89 vs. 3.50±0.92 g/day; t=2.273, p=0.03), shorter time to full enteral nutrition (8.47±3.36 vs. 13.80±7.63 days; t=−2.479, p=0.023) and to oral feeding (28.93±11.00 vs. 37.86±7.91 days; t=4.257, p=0.001), and a length of stay reduced by approximately 12 days favoring intervention (t=4.52, p=0.01), without compromising comfort, pain, or vital signs (Olgun et al., 2024). Collectively, studies that combined formal nurse-led governance with structured implementation activities reported higher implementation fidelity and favorable family- and clinical-level signals; however, the design of these studies (predominantly pre and post and observational) does not permit isolation of a leadership-specific effect, and estimates should be interpreted as associations with the bundled governance-plus-implementation package.
Theme 2: Technology–Workflow Integration Through Operational Governance Enactment
Eight studies (44%) emphasized workflow redesign and bedside enablement, predominantly through the enactment of Tier-2 operational governance by nurses with documented decision authority. In a Level II NICU EHR rollout, nursing informatics leaders convened unit design teams to map workflows, define requirements, project future states, test, and provide super-user training (8-hour sessions with bedside support) (Shade et al., 2017). With nursing leadership and interdisciplinary collaboration, implementation of the Braden QD tool was associated with 80% admission documentation compliance (41/51 within 12 hours), 82.19% adherence to q12h assessments (466/567), and 83% staff training completion (119/143) (Vazquez & Bell, 2024). A nurse-led, tablet-based classification system (ICNP 1.0; 143 diagnoses, 130 interventions) was reported to improve documentation agility, standardization, information retrieval, and space efficiency, although some users reported informatics skill gaps (Rezende et al., 2016). These process indicators reflect the contribution of operational governance embedded within broader interprofessional implementation processes; the relative contribution of nurse-led governance to the observed compliance metrics, as distinct from training, IT build, or audit-and-feedback, cannot be quantified from these designs.
Theme 3: Implementation Facilitators and Barriers
Using the conservative, explicit-only coding rule documented in Supplemental Table C2, the most frequently reported facilitator by authors was organizational/leadership support (17/18 studies; 94%). Structured training was explicitly named as a facilitator in 8/18 studies (44%); dedicated funding/IT infrastructure in 4/18 (22%); and clinical champions in 3/18 (17%). The full row-level coding, including studies in which a determinant was implied but not explicitly stated, is reported in Table C2; we deliberately reported only explicitly named determinants in the abstract and the present narrative to avoid over-counting and to align with Reviewer 3’s request for greater internal consistency. In a three-arm trial of tele-counseling versus pamphlet versus usual care (n=135 mothers; 32–36 weeks gestation), accessible expert support was associated with large effects on self-efficacy [F (2,127)=86.02, p<0.001, η2=0.57; means 77.12±1.01 vs. 68.28±1.10 vs. 57.43±1.07], trait anxiety [F (2,127)=67.26, p<0.001, η2=0.51; 30.22±1.10 vs. 40.36±1.14 vs. 48.09±1.11], and state anxiety [F (2,127)=76.46, p<0.001, η2=0.85; 28.16±1.17 vs. 39.89±1.21 vs. 48.04±1.18] (Mousavi et al., 2025). Barriers most frequently named explicitly by study authors comprised combined infrastructure/workload limitations (15/18; 83%), digital literacy gaps (4/18; 22%), and resistance to change (3/18; 17%). For example, nurses acknowledged the benefits of livestream cameras for bonding but flagged privacy and cybersecurity concerns, as well as workload concerns; pre/post surveys showed no significant changes in perceived security, familiarity, or parent time in the NICU (Kilcullen et al., 2020).
Theme 4: Clinical and Safety Outcomes
Fourteen studies (78%) reported clinical/safety outcomes. In one quality-improvement initiative combining a nurse-led interprofessional task force with structured training and audit-and-feedback (Tier 2), high-stage device-related hospital-acquired pressure injuries (HAPIs) were reduced by 60% (0.94→0.37 per 1,000 patient-days), with EEG- and CPAP-related high-stage HAPI rates reaching zero for 10 consecutive months (Moyer et al., 2022). In a rural tele-ROP program operationalized with a dedicated ROP nurse (Tier 2), 418/1,890 eligible infants (22.1%) were screened; 8.6% had pre-/plus disease, 15 had type 1 ROP, and 14/15 (93%) were treated successfully (Asturias et al., 2022). In simulated neonatal resuscitation, proactive “teleleader” support outperformed reactive “teleconsultant” support [checklist median 68% (IQR 66–69) vs. 58% (42–62), p=0.016], with lower mental demand (14.1±4.7 vs. 17.0±1.9, p=0.044) and frustration (7.9±5.5 vs. 14.7±3.5, p=0.047); inter-rater reliability κ=0.789 (p<0.001) (Gross et al., 2020). Among 304 NICU nurses, work-environment factors (Tier 3), nursing foundations for quality (β=0.43, p<0.001), manager leadership/support (β=0.15, p=0.033), staffing/resource adequacy (β=0.20, p<0.001), and nurse–physician relations (β=0.14, p=0.002), were associated with patient-safety attitudes (R2=0.539) (Unver & Isik, 2024). Pre–post and observational designs in this theme do not allow the leadership component to be statistically separated from concurrent training, EHR build, and audit-and-feedback; reported reductions are interpreted as associations with the integrated implementation package.
Theme 5: Family-Centered Outcomes and Engagement
Eleven studies (61%) evaluated family outcomes. A three-arm tele-counseling intervention reported improvements in maternal self-efficacy and reductions in anxiety, with large between-group effects (Mousavi et al., 2025). Nurse-led post-discharge telehealth (Tier 1) was associated with 100% family satisfaction and high uptake (74.6%; 282/378), and a contemporaneous comparison showed lower 30-day readmission rates among enrolled (13.8%) versus non-enrolled (30.9%) caregivers (Sarik et al., 2022). APN-led post-surgical telemedicine follow-up was associated with reduced caregiver burden (median 1,755 travel miles saved), avoidance of unnecessary encounters (50%), and earlier care when indicated (12%) (Willard et al., 2018). Despite implementation frictions, nurses perceived livestream video as supportive of bonding for families constrained by distance or work (Kilcullen et al., 2020).
Theme 6: Workforce Development and Professional Evolution
Eight studies (44%) addressed workforce development. A nurse-led e-learning intervention was associated with improved developmental-care perceptions (94.7±6.9 vs 83.2±13.7, p<0.001) and knowledge (90.3±13.8 vs 53.7±26.6, p<0.001) (Jalali et al., 2022). Higher e-health literacy (Tier 3) was associated with faster alert responses, better EHR navigation, and more effective use of decision support (Ayed et al., 2025; Ramadan, Elsharkawy, et al., 2025). Prior AI exposure tempered displacement concerns and increased acceptance, although infrastructure and ethics issues persisted (Ramadan, Elsharkawy, et al., 2025). Simulation-based resuscitation training was associated with initial skill improvement, but significant decay by two months underscored the need for regular refreshers in high-acuity, low-frequency domains (Bilodeau et al., 2024). Overall, sustained digital integration was linked to continuous education, skills maintenance, and broad-based digital literacy within the nursing workforce.
Discussion
This systematic review synthesized evidence on the relationship between nursing leadership and digital health integration in neonatal intensive care units (NICUs). Across 18 studies, classified as Tier 1 (formal nurse-led governance), Tier 2 (operational governance enactment), or Tier 3 (leadership-relevant determinants)- formal and operational nurse-led governance and key leadership-relevant determinants were consistently associated with stronger implementation processes and selected clinical and family-centered outcomes. However, the evidence base was predominantly observational and methodologically heterogeneous; the findings are best interpreted as associations rather than causal effects of leadership in isolation. Overall, the synthesis suggests that digital transformation in NICUs depends less on technology in isolation and more on how nursing expertise is mobilized, alongside training, workflow redesign, and audit-and-feedback, to align digital tools with clinical workflows, safety priorities, and family needs.
Theoretical Implications for Implementation Science
Three implementation-relevant insights emerged from the synthesis. First, the recurrent use of distributed and nurse-led leadership structures highlighted the limits of purely hierarchical adoption models. Frequently reported facilitators, organizational support, structured training, and clinical champions, underscore that implementation success often operates through social and organizational mechanisms (readiness, influence, credibility, and local problem-solving) rather than technological determinism. This is consistent with complexity-informed perspectives that emphasize adaptive coordination and local fit in high-acuity environments (Barnes et al., 2024).
Second, the findings emphasized capability-building as an implementation pathway. Several studies suggested that digital competence (e-health literacy, informatics confidence, and role clarity) may strengthen professional agency, while supported exposure to technology can reduce uncertainty and normalize new practices. Rather than proposing a new construct, these results are best interpreted as evidence that competence and agency may co-evolve during digital change, particularly when leaders create psychological safety, role support, and structured learning opportunities (Tsapnidou et al., 2024).
Third, the prominence of workflow integration reframed implementation from “adoption” to “adaptation.” Studies describing nursing informatics leadership and interdisciplinary workflow redesign consistently reported stronger process indicators (e.g., documentation timeliness, assessment adherence, training completion) than studies emphasizing technology deployment alone. Importantly, the high protocol-compliance figures reported in the Braden QD implementation study (Vazquez & Bell, 2024) should be interpreted as implementation-process metrics that emerged from coordinated interprofessional redesign with nursing leadership engagement, rather than as outcomes attributable to any single leadership component.
Distinguishing Leadership Signals From Implementation Co-Interventions
A central methodological caution that emerged from this synthesis concerns the difficulty of isolating a leadership-specific effect from the bundle of co-occurring implementation activities with which leadership is typically deployed. In most included studies, formal nurse-led governance (Tier 1) or operational governance enactment (Tier 2) was implemented alongside structured training, workflow redesign, EHR build, audit-and-feedback, and stakeholder engagement; the available pre- and post-observational designs do not permit decomposition of these components. As a result, the consistent association of nurse-led governance with favorable implementation indicators is hypothesis-generating rather than confirmatory. Tier-3 evidence (e.g., Ayed et al., 2025; Ramadan, Elsharkawy, et al., 2025; Unver & Isik, 2024) further supports the plausibility that leadership-relevant workforce and organizational determinants shape digital implementation, but it does not establish a causal pathway from leadership to clinical outcomes. Future research designs that could begin to decompose these effects include comparative-effectiveness studies of leadership models (e.g., shared governance vs dyad vs APN-led), stepped-wedge designs with leadership-component decomposition, sequential multiple-assignment randomized trials (SMART) of leadership intensification, and embedded qualitative process evaluations that document the specific decision authority arrangements in operation. Until such evidence accumulates, recommendations to invest in nursing leadership capacity should be framed as prioritized alongside, and not in place of, the implementation infrastructure with which leadership co-acts.
Interpreting Outcome Signals With Appropriate Caution
Several studies have reported sizable clinical and family-centered improvements, but the magnitude of the effects should be interpreted conservatively. Quality-improvement initiatives in NICU/PICU contexts (e.g., pressure-injury prevention) often use pre–post designs that are vulnerable to confounding from concurrent service changes, secular trends, staffing variation, and documentation effects (Moyer et al., 2022). Likewise, telemedicine-based ROP screening programs have demonstrated feasibility and encouraging performance in real-world rollouts, yet many evaluations are programmatic or observational, so the strongest defensible inferences are plausibility and association rather than causality (Al Amro et al., 2022). Family-centered outcomes were generally favorable: randomized and quasi-experimental studies of tele-counseling/telenursing after NICU discharge reported improvements in maternal self-efficacy and reductions in anxiety, supporting the premise that nursing-led delivery models can shape how digital tools translate into outcomes that families value (Mousavi et al., 2025).
Human-Centered Leadership as a Critical Capability
A consistent message across the evidence is that sophisticated digital systems do not diminish the need for skilled leadership; they intensify it. The review suggests that NICU digital transformation tends to be most effective when nursing leaders actively curate the conditions for safe use, workflow fit, role clarity, competency reinforcement, and ongoing troubleshooting, so that digital tools extend rather than replace clinical judgment (El-Bassal et al., 2025). This carries practical workforce implications: investments in leadership capacity, implementation support, and informatics competence may yield more durable benefits when paired with sustained investment in training, workflow integration, and IT infrastructure, rather than in any one component alone (Berardinelli et al., 2024; Leask & Macleod, 2023).
Strengths and Limitations
This review had several noteworthy strengths. Adherence to PRISMA 2020 guidelines, prospective PROSPERO registration, and a broad six-database search with supplementary grey literature screening ensured methodological rigor and search comprehensiveness. Dual-reviewer screening, extraction, and quality appraisal with design-specific tools (Cochrane RoB 2, ROBINS-I, JBI, MMAT) enhanced transparency and reduced subjective bias. The integration of quantitative and qualitative evidence through a convergent-segregated approach enabled a nuanced understanding of both outcome effects and implementation mechanisms across diverse technologies, settings, and leadership models.
Limitations should temper interpretation. First, the predominance of moderate-risk-of-bias observational and pre–post designs reflects typical constraints in real-world implementation evaluations, where randomization and blinding are often infeasible (Laukka et al., 2020). Second, the bundling of nurse-led governance with co-occurring training, workflow redesign, and audit-and-feedback in most included studies precludes statistical decomposition of a leadership-specific effect; the available evidence supports plausibility and association rather than causal inference. Third, although the broadly consistent direction of findings across diverse technologies supports the plausibility of nurse-led governance as a determinant of implementation, generalizability remains constrained by the concentration of studies in high-resource settings, despite the disproportionate burden of neonatal mortality in low- and middle-income countries (Olgun et al., 2024; Öz et al., 2024). The single included study from Guatemala (Asturias et al., 2022) demonstrates feasibility but cannot represent the range of infrastructure, staffing, connectivity, regulatory environments, and cultural contexts that shape implementation. Fourth, the absence of economic evaluations is a notable gap given finite resources and competing priorities. Future evaluations should explicitly address digital-divide constraints (connectivity, device access, interoperability, and informatics workforce capacity) and test scalable nurse-led models that remain functional under variable infrastructure and policy conditions (Yew et al., 2025).
Several research priorities follow. Comparative-effectiveness studies that directly contrast nursing leadership models would clarify the optimal governance structures for specific digital technologies and organizational contexts. Implementation research in resource-limited settings must address culturally responsive adaptations and minimum viable infrastructure requirements. Mixed-methods investigations examining unintended consequences, including algorithmic bias, moral distress, and risks of depersonalization, would provide a balanced perspective on the human costs of digital transformation. Economic evaluations incorporating direct costs, indirect benefits, and long-term neurodevelopmental outcomes would strengthen the evidence base for leadership investment decisions. Studies exploring the intersection of digital nursing leadership and health equity could identify strategies to reduce, rather than exacerbate, existing disparities. Research on optimal human–AI collaboration models in neonatal care would inform next-generation implementation strategies as artificial intelligence capabilities continue to expand. Finally, future evaluations should examine ethics-informed, crisis-ready digital governance and training models in NICUs, including how bioethical education and disaster-management competencies translate into safer, more resilient digital implementations.
Implications for Practice and Policy
For practice, the evidence supports three actionable directions, framed cautiously given the predominantly observational evidence base. First, organizations should formalize nursing informatics governance by establishing documented decision-making authority (clear scope, responsibilities, and escalation pathways) rather than relying on ad hoc committees. Second, implementation should be structured around workflow redesign plus competency reinforcement, with training models that include bedside coaching, super-users, and iterative competency assessment, particularly in environments where skill retention is vulnerable. Third, organizations should adopt implementation measurement plans that track both process indicators (fidelity, training coverage, documentation timeliness) and patient/family outcomes to avoid mistaking early adoption for sustained integration.
For policy, frameworks should recognize nursing informatics and digital leadership as competency-based functions that require workforce planning, protected time, and defined professional development pathways. Reimbursement and quality models should be aligned with the observed associations of nursing-led digital interventions with favorable outcomes (e.g., family satisfaction and reduced unplanned utilization), with the caveat that the underlying evidence does not establish causal effects of leadership in isolation, and policy levers should therefore co-invest in the broader implementation infrastructure (training, IT build, audit-and-feedback) with which leadership co-acts.
Conclusions
This systematic review identified nurse-led governance, encompassing formal governance structures, operational governance enactment, and leadership-relevant determinants, as a consistent and plausible determinant of successful digital health integration in NICUs, warranting prospective evaluation. The evidence challenges narrowly technology-deterministic approaches and suggests that digital transformation tends to succeed through the strategic mobilization of nursing expertise, embedded within coordinated training, workflow redesign, and audit-and-feedback, to bridge technical possibilities with clinical realities. As artificial intelligence and advanced monitoring technologies proliferate, investment in nursing leadership capacity should keep pace with the development of technological infrastructure and be paired with sustained investment in implementation systems. The path to improved neonatal outcomes lies not in technological sophistication alone but in recognizing and empowering nurses as architects of sociotechnical transformation, while continuing to test these propositions through comparative-effectiveness, stepped-wedge, and economic evaluations that can decompose leadership components from co-occurring implementation activities.
Supplemental Material
Supplemental Material - Nursing Leadership for Digital NICU Transformation: A Systematic Review of Strategies, Digital Health Integration, and Outcomes in High-Risk Neonates
Supplemental Material for Nursing Leadership for Digital NICU Transformation: A Systematic Review of Strategies, Digital Health Integration, and Outcomes in High-Risk Neonates by Osama Mohamed Elsayed Ramadan in Sage Open Nursing.
Footnotes
Ethical Considerations
Registration: This review was prospectively registered with PROSPERO (CRD420251161936). The review followed PRISMA 2020 reporting guidance.
Author Contributions
O.M.E.R. conceptualization; methodology and search design; screening and selection; data extraction and curation; risk-of-bias appraisal; formal analysis and synthesis; writing—original draft; writing—review & editing; project administration. The author approved the final manuscript and agrees to be accountable for all aspects of the work.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All search strategies, screening forms, and extraction templates are described in the manuscript. De-identified review materials (full database search strings, EndNote/Covidence export of screened records, data-extraction sheets, and risk-of-bias matrices) are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.