
Abstract
Introduction
Adherence to secondary prevention is important for patients with coronary artery disease. Healthcare providers must identify the factors that affect secondary coronary artery disease prevention to formulate and execute strategies aimed at enhancing patient adherence.
Objective
To assess healthy lifestyle behaviors among patients with coronary artery disease and examine associations among individual characteristics, cardiac self-efficacy, social support, and healthy lifestyle adherence.
Methods
A correlational, cross-sectional design was employed. Two hundred and nineteen patients with coronary artery disease were selected as a convenience sample from the cardiac clinics of three large Jordanian hospitals. Descriptive and multivariate linear regression analyses were employed.
Results
Coronary artery disease patients reported a moderate cardiac self-efficacy level, a high perceived social support level, and moderate adherence to healthy lifestyle behaviors. Multiple regression analysis indicated that smokers demonstrated significantly lower adherence to healthy lifestyle behaviors compared with non-smokers. (β = −0.21, p < .01). Meanwhile, patients with comorbidities (β = 0.18, p < .01), had received coronary care education (β = 0.20, p < .01), perceived more social support (β = 0.15, p < .05), and had a higher level of perceived cardiac self-efficacy (β = 0.41, p < .001) were significantly associated with healthy lifestyle adherence.
Conclusion
Further research into intervention strategies is necessary to enhance patients’ understanding of coronary care, boost their self-efficacy, and strengthen social support, ultimately leading to improved adherence behaviors among individuals with coronary artery disease.
Introduction
One of the major causes of death worldwide is coronary artery disease (CAD), accounting for more than eight million deaths globally each year (WHO, 2021). Currently, both high-income and low-to middle-income countries are experiencing a rise in the disease burden linked to cardiovascular disease morbidity and mortality (Wu et al., 2024). As per the most recent WHO data released in 2020, deaths from CAD in Jordan amounted to 4,856, constituting 18.60% of overall deaths. Unhealthy diet, Lack of physical activity, smoking, overweight or obesity, diabetes, hypertension, and hyperlipidemia are the main risk factors of CAD (WHO, 2021). CAD is widely acknowledged as a preventable condition, primarily because it has been demonstrated that modifiable risk factors contribute to over 90% of the overall risk associated with CAD (Kaminsky et al., 2022). Prevention of CAD includes pharmacological treatment and non-pharmacological approaches such as engagement of healthy lifestyle behaviors, which encompass weight management, dietary modification, exercise, and smoking cessation. Adherence to secondary prevention is important for patients with CAD (Jung & Yang, 2021).
Review of Literature
Adherence is described as “the extent to which patients comply with the prescribed medication, dietary, and lifestyle modifications recommended by healthcare providers,” which is crucial for achieving good treatment outcomes (Zolnierek & Dimatteo, 2009). Adherence to healthy lifestyle behavior has been demonstrated to correlate with a decreased likelihood of a significant coronary incident and enhance the efficacy of any administered treatment and surgical procedure (Wu et al., 2024). However, a survey conducted across 17 countries worldwide revealed that only a small percentage of patients, specifically 4.3%, have adopted these health-promoting behaviors (Teo et al., 2013). A review of 12 studies revealed low adherence among Arab people with CAD (Alomari et al., 2022). Determining a patient’s degree of adherence to a healthy lifestyle may enhance their quality of life, lower their chance of experiencing another cardiac episode, and lower their readmission rates to hospitals (Ghandour et al., 2019). Therefore, healthcare providers must identify the factors that affect secondary coronary artery disease prevention to formulate and execute strategies aimed at enhancing patient adherence (Ammouri et al., 2018).
According to the World Health Organization (WHO, 2003), factors related to socioeconomic status, health systems, therapy, and individual patients influence adherence. Some individual-related factors include self-efficacy and social support. A major determinant of positive health outcomes among people with CAD is social support, and patients with CAD frequently depend on support from their family and friends to begin and sustain healthy behaviors (Graven & Grant, 2014). Rashidi and colleagues (2020) in their systematic review, revealed that in order to enhance adherence to treatment regimens for chronic diseases, social support plays a crucial role. Meanwhile, according to a thorough worldwide systematic review, it was determined that those with low social health had a 30% higher risk of having CAD (Freak-Poli et al., 2022).
Cardiac self-efficacy is an important part of health behavior regulation and management, as well as the development of health behavior that is associated with CAD (Brouwer-Goossensen et al., 2018). Heart self-efficacy (CSE) creates a desire and readiness to adopt such practices, which in turn encourages people to make appropriate lifestyle choices about their CAD (Breaux-Shropshire et al., 2012). Patients with CAD who have high self-efficacy are more likely to take an active role in managing their disease, maintain better health, and practice self-care (Alizadeh et al., 2018). Previous studies have reported that inadequate self-care practices are significantly associated with low self-efficacy level (Almeida et al., 2022).
Cardiac nurses are in a unique position to assess patients’ lifestyle practices, identify barriers to adherence, provide tailored education, and promote behavioral change through ongoing counseling and follow-up. In addition to providing disease-specific education, nurses have an important role in bolstering the patients’ self-efficacy and activating social support resources, both of which are critical in maintaining long-term lifestyle changes. There is evidence that nurse-led interventions can improve patients’ engagement in physical activity, dietary adherence, smoking cessation, medication management, and general self-care behaviors, leading to improved cardiovascular outcomes and reduced hospital readmissions (Rashidi et al., 2020; Tawalbeh & Ahmad, 2014). Therefore, understanding factors associated with adherence to a healthy lifestyle in nursing practice is of great importance, as it provides evidence for the development of targeted culturally appropriate interventions in patients with CAD.
This study was based on Pender’s Health Promotion Model (HPM), which is a holistic model that enables the identification of various determinants that affect health behaviors (Pender et al., 2015). According to HPM, health behaviors are affected by individual experiences and behavior-specific cognitions related to specific actions, including self-efficacy and interpersonal influence, such as social support (Pender et al., 2015). Self-efficacy is considered to be among the major predictors of health behavior, because individuals who believe that they are capable of performing particular actions are more likely to do them. Cardiac self-efficacy can help patients diagnosed with CAD follow recommendations concerning healthy eating, physical activities, stress management, and medication use (Shrestha et al., 2020). Social support coming from one’s family, friends, and other members of the healthcare team also serves as one of the important interpersonal influences that contribute to the performance of positive health behaviors due to the provision of encouragement, help, and motivation for lifestyle changes (Tawalbeh et al., 2015). Therefore, HMP provides an ideal framework for understanding healthy lifestyle adherence among patients with CAD.
While adherence to a healthy lifestyle in patients with CAD has been extensively studied, significant knowledge gaps remain. Most of the current research has focused on the psychosocial determinants in isolation, with limited attention to the simultaneous contribution of cardiac self-efficacy and perceived social support. Moreover, there is no evidence available for Arab and Middle Eastern populations, despite the cultural features that may influence adherence behavior such as family-centered support structures, smoking practices, and healthcare access. Recent systematic reviews have underscored the role of psychosocial factors in the management of cardiovascular disease, while also emphasizing the necessity for context-specific explorations in various populations (Wu et al., 2024). Such knowledge about these relationships among Jordanian populations may provide valuable evidence for the development of culturally appropriate nursing interventions to improve secondary prevention outcomes among patients with CAD. Consequently, this study was conducted to address this gap. This study aims to assess healthy lifestyle behaviors among patients with coronary artery disease and examine associations among individual characteristics, cardiac self-efficacy, social support, and healthy lifestyle adherence.
Methods
Design
A correlational, cross-sectional design was used to examine associations among individual characteristics, cardiac self-efficacy, social support, and healthy lifestyle adherence.
Sample and Setting
Using a convenient sampling technique, all patients diagnosed with CADs referred to outpatient cardiac clinics were possible participants for the current study. Patients were enrolled in the study if they met the following inclusion criteria: outpatients with CAD (angina or myocardial infarction), older than 18 years, capable of reading and comprehending the study information to complete the questionnaire, willing to sign the consent form, and diagnosed with CAD at least six months ago. Patients who have mental and neurological disorders (e.g., stroke), admitted to hospital wards, underwent CABG surgery were excluded. Patients who had undergone CABG were excluded because postoperative recovery, participation in rehabilitation, and procedure-specific lifestyle recommendations may significantly affect adherence behaviors and self-efficacy levels, thereby introducing clinical heterogeneity into the sample. For statistical testing, linear multiple regression was used based on a G* power calculation (F test); approximately 187 participants were required to obtain a power of .80, an effect size of 0.15, an alpha of .05, and a total of 7 tested predictors.
The study was carried out at two private hospitals and cardiac clinics at a university-affiliated hospital. The three hospitals were selected for this study because they provide both coronary care and intensive care (with readily available cardiac laboratories) as well as cardiac disease outpatient care. Within the campus of a governmental university, the university-affiliated hospital is located in the northern region of Jordan. It is a teaching hospital that offers training for nursing, medicine, and other health-related fields. It contains a surgical and medical department with 552 beds. The hospital is regarded as a referral hospital that provides specialized health care for referred patients from other hospitals in the northern area of Jordan. Every month, over 1400 patients are treated at the outpatient cardiac clinics by cardiologist doctors and cardiac nurses.
The two private hospitals are located in the capital city Amman with a bed capacity between 220 and 250. The two hospitals provided their services in various branches of medicine and surgery. These hospitals are considered among the largest private hospitals in Jordan. In addition, outpatient’s cardiac clinics in the two private hospitals offer treatment for several cardiac outpatients from cardiologist doctors and cardiac nurses. The outpatient cardiac clinics in the two hospitals receive about 40-80 patients daily.
Data Collection
Following permission by the two private hospitals where the study was carried out and the Institutional Review Boards of a governmental university. Data was gathered in 2022 between April and June.
All participants were recruited at the cardiac clinics of the three hospitals. The hospital offers comprehensive healthcare services for patients admitted. All patients with CADs regularly attend the outpatient clinics. The outpatient cardiac clinics gave the research team access to patient medical records. All physicians received invitation letters with information about this study for potential participants to circulate to patients with CADs. The research team approached patients with CADs, who expressed interest in participating in this study, to confirm that they met the eligibility criteria. Data for this study were collected via a self-reporting questionnaire.
Instrument
The self-administered questionnaire was developed and consisted of four sections that included sociodemographic and health variables, cardiac self-efficacy, social support, and lifestyle adherence. To collect data on particular sociodemographic, health variables, and disease-specific characteristics of the participants, a sociodemographic sheet was developed. These characteristics were: age, gender, education level, marital status, health insurance, employment status, and disease-specific characteristics (CAD-specific education, smoking status, and comorbidity). In this study, normal weight, overweight, and obesity were evaluated using body mass index. Body mass index, which is calculated by dividing weight in kilos by the square of height in meters, calculates body fat (weight/height2 (kg/m2)). (WHO, 2022). A BMI of less than 18.5 was considered underweight; 18.5 to 24.9 kg/m2 was considered normal weight; 25 to 29.9 kg/m2 was considered overweight; and more than 30 kg/m2 was considered obese (The study questionnaire is provided in Supplementary File).
To measure social support indicators, the Personal Resource Questionnaire (PRQ-2000) developed by Weinert (2000) was used. Fifteen items on a 7-point Likert scale make up the self-administered questionnaire. Responses to the item fall between 1 (strongly disagree) and 7 (strongly agree). In order to obtain the overall score of social support indicators, the 15 items were calibrated. Higher scores indicate greater amounts of perceived social support; possible scores ranged between 15 and 105. The instrument’s alpha coefficient ranged from 0.87 to 0.94, indicating a excellent level of internal consistency (Weinert, 2000). The PRQ-2000 Arabic version questionnaire was utilized (Tawalbeh et al., 2015). The Cronbach’s α coefficient in this study was 0.95.
The Cardiac Self-Efficacy (CSE) questionnaire, developed by Sullivan and colleagues (1998), was used to measure cardiac self-efficacy. The 16 items CSE questionnaire has three subscales that include “control of symptoms” subscale (eight items), “maintenance of function” subscale (five items), and “maintaining healthy life style” subscale (three items) (Sullivan et al., 1998). An ordinal 5-point Likert-type scale ranging from 0 (strongly disagree) to 4 (strongly agree) was used to score the items. A higher score indicates a higher level of cardiac self-efficacy; scores ranged from 0 to 64. Sarkar and colleagues (2009) indicated that the CSE Scale has been used widely in patients with CAD. The CSE is a reliable and valid questionnaire; according to Sullivan et al. (1998), internal consistency reliability is 0.90. Arabic version of the CSE (Shajrawi et al., 2020) was used. Overall, the reliability and validity scores of the Arabic version of the CSEQ were comparable to those of the original form (Shajrawi et al., 2020). The Cronbach’s α coefficient in this study was 0.91.
The Adherence Scale, which was a 0-9 ordinal scale developed by Alm-Roijer and colleagues (2004), was used to assess participants’ levels of adherence to healthy lifestyle behaviors. Responses ranged from 0 (“I have not made any lifestyle changes”) to 9 (“I have made a lot of lifestyle changes”) for the 11 items that were used. The average score for each item was calculated to obtain the final total score. Higher scores indicate a greater degree of lifestyle modifications adherence; the total possible score ranges from 0 to 9. Internal consistency reliability for items was assessed using Cronbach’s α coefficient. A previous study found the Cronbach’s α coefficient to be approximately 0.73 (Alm-Roijer et al., 2004). Tawalbeh and colleagues’ (2015) Arabic version of the Adherence Scale was used in this study. The Cronbach’s α coefficient in this study for the Arabic version was 0.78.
Ethical Consideration
This study was approved by the Institutional Review Board of a governmental university and the two hospitals where the study was carried out. The IRB approval date is March 2, 2022. The study participants were given an explanation of the study’s significance and goal. The researcher clarified that participation in the study is entirely optional and that there are no consequences if individuals decide to leave at any point. The questionnaires were coded, and confidentiality was assured. All participants were informed that only the researcher would have access to the data and that it would only be utilized and shared for research purposes.
Data Analysis
SPSS version 21 (SPSS, Chicago, Illinois) was used to analyze data. A 0.05 criteria was applied to the statistical significance analyses. All study variables were analyzed using descriptive statistics, such as mean, standard deviations, frequency, and percentages. To examine associations among individual characteristics, cardiac self-efficacy, social support, and healthy lifestyle behaviors, multiple regression statistical analyses were used. All independent variables were entered simultaneously using the enter method. Categorical variables were dummy coded with appropriate reference categories prior to analysis. All assumptions were tested before the multiple linear regression analysis to ascertain whether the assumptions were satisfied. The multicollinearity assumptions were established using collinearity diagnostics by calculating the tolerance value and the variance inflation factor (VIF), with all the VIF being below 10. Regression assumptions were also tested based on the residuals plot analysis in order to determine linearity, normality, homogeneity, and independence of error. Based on the results from the assumptions test, it can be concluded that all the assumptions for multiple linear regression have been satisfied.
Results
Participants’ Characteristics
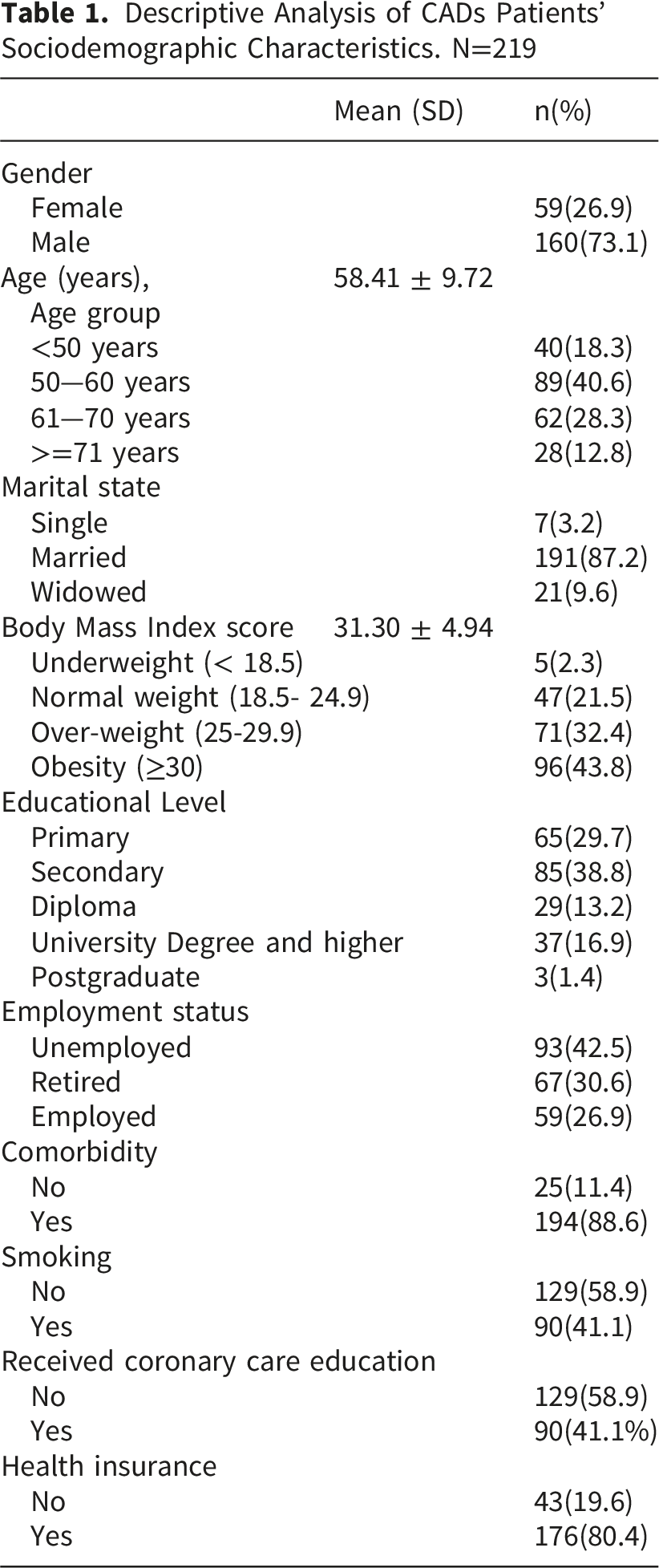
Descriptive Analysis of CADs Patients’ Sociodemographic Characteristics. N=219
Perceived Cardiac Self-Efficacy, Social Support, and Healthy Lifestyle Behaviors Adherence
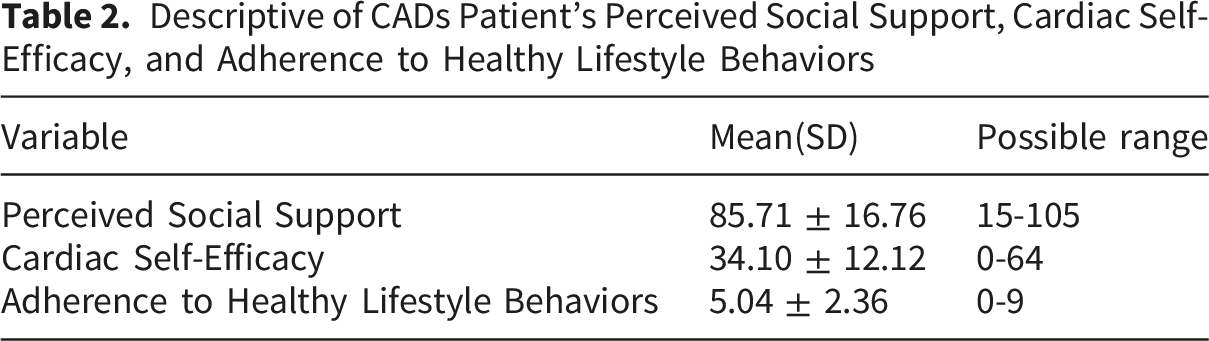
Descriptive of CADs Patient’s Perceived Social Support, Cardiac Self-Efficacy, and Adherence to Healthy Lifestyle Behaviors
Predictors of Healthy Lifestyle Behaviors
Multiple Regression Analysis of Individual Characteristics Perceived Social Support, Cardiac Self-Efficacy on Adherence to Healthy Lifestyle Behaviors
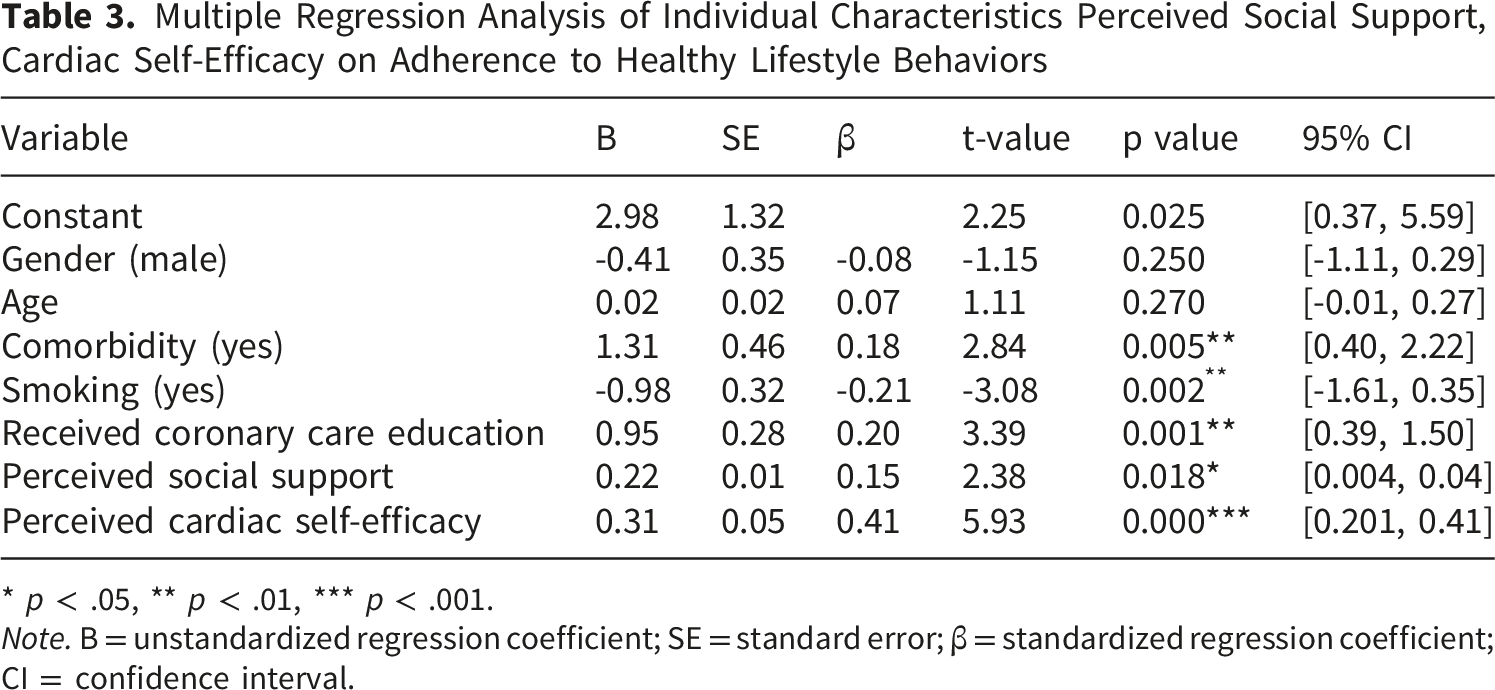
* p < .05, ** p < .01, *** p < .001.
Note. B = unstandardized regression coefficient; SE = standard error; β = standardized regression coefficient; CI = confidence interval.
Discussion
The aim of this study was to assess healthy lifestyle behaviors among patients with CAD and examine associations among individual characteristics, cardiac self-efficacy, social support, and healthy lifestyle behaviors. For individuals with CAD, adhering to healthy lifestyle behaviors is essential, and numerous factors, particularly social support and self-efficacy, have been acknowledged as significant contributors. In the present study, there was high social support. In addition, 92.7% of the patients have said that they have someone to take care of them. This result was consistent with previous studies (Freeborne et al., 2019; Malak et al., 2023). The collectivist culture widespread in the Jordanian and Arab communities may elucidate this phenomenon, as social support plays a crucial role and serves as a protective factor against the challenges posed by stressful life events (Baqutayan, 2011). In addition, the result showed moderate CSE perceived by patients with CAD. This result was consistent with previous studies (Mazar et al., 2020; Wantiyah et al., 2020).
The level of healthy lifestyle behaviors adherence score was moderate. The result was consistent with Al-Zaru et al. (2022), who demonstrated that 41.0% of CAD participants did not follow healthy lifestyle practices. Among patients with CAD, medication adherence was the most common healthy lifestyle practice. Patients with CAD may place greater emphasis on the therapeutic outcomes of their medication, which in turn may enhance their adherence to the prescribed treatment regimen (Chen et al., 2022). Meanwhile, the least adherence to healthy lifestyle behaviors was found in the areas of exercise participation, weight management, and diet. These findings aligned with those of Alomari et al. (2022), who discovered that Arab patients with CAD follow food and exercise guidelines less frequently than those from other ethnic groups. They gave an explanation of this in terms of the social customs that Arabs share in common. These customs dictate that guests should consume everything that is offered to them, and it is traditional for the host to request that they eat more. Because of this, people frequently overeat to please the host. (Akhu-Zaheya & Shiyab, 2017; Alomari et al., 2022; Ammouri, 2008).
This study’s results indicated that smoking has a negative significant association with healthy lifestyle behaviors’ adherence. CAD smokers were less adherent to healthy lifestyle behaviors compared to those patients who were non-smokers. This study’s results were consistent with Celebi and colleagues (2021) who explained that reduction in functional abilities impacts smokers in various ways, resulting in constraints on daily activities and a decline in work productivity.
In addition, patients who received coronary care education from a health care provider had significantly higher adherence to healthy lifestyle behaviors compared to those who had been received coronary care education. In a mixed-method review conducted by Alomari et al. (2022), which examined healthy lifestyle adherence recommendations among CAD Arab patients, it was found that nine studies identified key predictors of adherence. One significant predictor was receiving recommendations and regular advice from the health care professionals. Tawalbeh and Ahmad (2014) conducted a study to evaluate the impact of a cardiac education program on the degree of healthy lifestyle adherence among patients with CAD in Jordan. They concluded that patients with CAD benefit from the implementation of cardiac education programs in terms of improved understanding and adherence to healthy lifestyles.
In addition, patients who had other comorbidity had a significantly higher level of healthy lifestyle behaviors adherence. Ndualem and colleagues (2020) attributed this to the existence of additional co-morbidities and their associated challenges may encourage patients to alter their lifestyle in accordance with the provided recommendations. Furthermore, implementing lifestyle changes is generally more financially feasible than purchasing medication, which can be costly.
This study’s results supported that patients with CAD who perceived more social support were associated with more adherence to healthy lifestyle behaviors, consistent with previous findings (Freak-Poli et al., 2022; Rashidi et al., 2020). The findings showed a strong positive association between social support and the adoption of healthy lifestyle practices, suggesting that promoting adherence in people with CAD may require strengthening social support (Zhou et al., 2022).When individuals receive support, direction, and encouragement from friends, family, and medical experts, they are far more likely to adopt behavioral patterns that are beneficial to their health. These peoples contribute significantly to the patient’s dedication to the treatment by acting as influential influences (Babygeetha & Devineni, 2024).
This study’s findings are in line with earlier research that found self-efficacy to be a crucial factor in association with heart-healthy lifestyle adherence (Almeida et al., 2022; Wantiyah et al., 2020). Nuraeni and colleagues (2023) concluded that interventions, including increasing awareness of the disease, altering health behaviors, and conducting prompt screenings, can enhance patients’ self-efficacy. Furthermore, accurate diagnosis and continuous treatment are essential for improving self-efficacy and outcomes in CAD care.
In addition to psychosocial determinants, anatomical characteristics may also contribute to differences in symptom perception and subsequent health behaviors in patients with cardiovascular disease. There is mounting evidence that the conformation of the chest wall, especially a concave thorax, might influence perception and awareness of cardiovascular symptoms. For example, a recent study of patients with atrial fibrillation undergoing electrical cardioversion showed that a higher modified Haller index, indicating a greater concavity of the chest wall, was associated with an increased symptom perception and lower odds of asymptomatic status (Sonaglioni et al., 2024). Although these results were discovered in a different cardiovascular population and were not directly related to adherence behaviors, they suggest the possibility for individual anatomical factors to play a role in differences in symptom perception and disease experience. Future studies in patients with coronary artery disease might explore the combined effects of anatomical and psychosocial factors on self-management and adherence to recommended lifestyle behaviors.
The results of this study should be evaluated in light of the larger sociocultural environment that affects coronary artery disease (CAD) patients’ adherence to health-promoting practices. Adherence to suggested lifestyle changes may be restrained by factors such low health literacy, cultural acceptance of smoking, gender-related obligations, and obstacles to receiving healthcare services (Alrasheeday et al., 2024; Magnani et al., 2018). The culture within the Middle East is such that smoking is a socially acceptable practice, especially among males, with women struggling with care-giving duties and physical activities as a result of social and cultural as well as gender barriers (Chaabane et al., 2021; Osabi et al., 2023). The importance of culturally sensitive nursing interventions has been brought out by this evidence. Nurses are central in this case by ensuring assessment of health literacy levels, educating the patient, helping in smoking cessation, involving family members in the care plan, and accessing community and cardiac rehabilitation services (Qiu, 2024). These evidenced-based practices are known to improve self-management and adherence to healthy lifestyles in CVD patients (Qiu, 2024).
Strengths and Limitations
The study has several strengths that make its findings more credible and relevant. The study has contributed to a comprehensive understanding of psychosocial factors related to adherence to healthy lifestyles as it simultaneously investigated cardiac self-efficacy, perceived social support, and compliance to healthy lifestyle behaviors of patients with CAD. The study has bridged an important gap in the literature. This study also adds valuable evidence from the Middle Eastern context where research on the psychosocial determinants of healthy lifestyle adherence among patients with CAD is still limited and will help to expand the global evidence base and inform culturally sensitive nursing interventions.
The results must be interpreted within the context of certain limitations. The cross-sectional design of the research does not allow drawing causal conclusions about relations among different variables. In addition, the data was collected using self-reports and, thus, is subject to recall bias and social desirability bias. Moreover, convenience sampling may have introduced a selection bias and reduced the representativeness of the sample. Furthermore, recruitment took place in only a few healthcare institutions, which could have affected the generalizability of the results. Lastly, medication adherence behaviors depend on various contextual variables, such as health literacy and access to healthcare services. Further longitudinal studies are required to investigate these links (WHO, 2023).
Implications for Practice
The outcomes of this research hold considerable significance for practice in nursing. Understanding the roles of cardiac self-efficacy, social support, and adherence is crucial for nurses and other healthcare professionals. This knowledge can be integrated into various health education initiatives and shared with healthcare providers. Nurses and other healthcare providers can be empowered by the results to recognize the challenges patients with CAD confront. Consequently, they can develop cardiac education and follow-up programs that address the psychosocial aspects of these patients, facilitating the acquisition of new behaviors through modeling or the modification of existing maladaptive behaviors. These programs are designed to increase patients’ understanding of the cardiac disease process and risk factors; enhance their cardiac self-efficacy; strengthening their social connectedness; and commit to healthy lifestyle behaviors.
This study’s findings have important implications for cardiovascular nursing practice. Nurses are well-placed to identify psychosocial barriers that may impact on adherence to healthy lifestyle behaviors in patients with CAD. Routine assessment of cardiac self-efficacy and perceived social support may promote early identification of patients at risk for poor adherence. Evidence suggests that educational interventions by nurses, motivational interviewing, and family-centered counseling can enhance self-management behaviors and adherence outcomes in patients with cardiovascular disease (Tawalbeh & Ahmad, 2014; Zolnierek & Dimatteo, 2009). Therefore, nursing interventions should not only involve education on the disease but also strategies that enhance confidence in self-management and bolster support systems.
Conclusion
By increasing awareness of the disease, nurses are crucial in evaluating the lifestyle choices of patients with CAD and the importance of adopting healthy lifestyle behaviors. This study demonstrates that Jordanian patients with CAD reported moderate healthy lifestyle behaviors adherence. Meanwhile, adherence to healthy living practices was significantly associated with coronary care knowledge, strong self-efficacy, and greater social support. In order to improve adherence behaviors among people with coronary artery disease, more research into intervention strategies is required to improve patients’ comprehension of coronary treatment, increase their self-efficacy, and fortify social support.
Supplemental Material
Supplemental material - Cardiac Self-Efficacy, Social Support, and Adherence to Healthy Lifestyle Behaviors Among Patients With Coronary Artery Disease
Supplemental material for Cardiac Self-Efficacy, Social Support, and Adherence to Healthy Lifestyle Behaviors Among Patients With Coronary Artery Disease by Ibtisam M. Al-Zaru, Ali A. Ammouri, Audai A. Hayajneh, Ayat M. Zyout in Sage Open Nursing
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Jordan University of Science & Technology (Approval no. 45/147/-2022).
Consent to Participate
All the patients provided informed consent. Copies of the consent forms are available upon request.
Authors Contribution
A.I: Conceptualization; methodology; formal analysis; writing—review and editing; investigation. A.A: Methodology; formal analysis; writing—review and editing. H.A: Conceptualization; methodology; formal analysis; writing. Ayat A.M: Conceptualization; methodology; formal analysis; writing; investigation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.