
Abstract
There is no “gold-standard” material for the operative management of root caries. The aim of this study was to determine if the clinical performance of Biodentine would be acceptable for the restoration of root caries in older adults. A randomized controlled clinical trial was conducted comparing a calcium silicate cement (Biodentine), a high-viscosity glass ionomer cement (Fuji IX GP Extra), and a resin-modified glass ionomer cement (Fuji II LC). Of the 334 volunteers assessed for eligibility, 249 were excluded. A total of 303 lesions in 85 participants were randomized, with 151 lesions allocated to receive Biodentine, 77 to Fuji IX GP Extra, and 77 to Fuji II LC. Patients were reviewed by a calibrated dentist who was not involved in restoration placement and who was blinded to material allocation. Restorations were assessed according to a modified US Public Health Service criteria. The cumulative survival percentages after 6 mo and 1 y were 58.6% and 47.2% in the Biodentine group, 89.6% and 83.8% in the Fuji IX GP Extra group, and 89.5% and 84.9% in the Fuji II LC group, respectively. There were statistically significant differences (χ2 test, P < 0.001) in restoration failure rates between restoration groups. There was no difference between Fuji IX GP Extra and Fuji II LC, but differences (P < 0.001) were shown between the Fuji II GP Extra group and the Biodentine group and also between the Fuji II LC group and the Biodentine group at both time points. Based on the results of this study, Biodentine cannot be recommended for the operative management of root caries. Fuji IX GP Extra and Fuji II LC displayed similar success rates, and high-viscosity glass ionomer cement and resin-modified glass ionomer cement continue to be the best available option for the restoration of root caries (ClinicalTrials.gov NCT01866059).
Keywords
Introduction
The world population is rapidly aging. Between 2000 and 2050, the proportion of the world’s population older than 60 y will double from about 11% to 22%. Alongside this trend in global aging, there is a concomitant reduction in levels of edentulism in developed countries (Chen et al. 1997; Petersen et al. 2004). An increase in the prevalence of root caries can be expected as it has been shown that older people are at a higher risk of root caries than younger populations due to an increased number of exposed root surfaces (Fejerskov et al. 1991; Chi et al. 2013).
Restoration of these lesions is challenging as the cavities are broad and saucer shaped with ill-defined margins, which can be positioned in enamel as well as dentine (Wefel et al. 1985). A systematic review of the operative management of root caries lesions identified only 5 clinical trials in the literature that compared different restorative materials (Hayes et al. 2014). Most studies included patients with radiation-induced caries, and there is limited information regarding the success of operative treatment for root caries. Failure rates were high across all restorative materials, and at present, there is no “gold-standard” restorative material for this indication.
Calcium silicate–based cements were first introduced to dentistry in 1993 when Torabinejad developed a formula based on ordinary Portland cement (OPC) to produce the mineral trioxide aggregate (Lee et al. 1993). In 2011, a quick-setting calcium silicate–based cement (Biodentine; Septodont, Saint Maur de Fosses, France) was developed as a dentine replacement material. As root carious lesions are often confined to dentine, and Biodentine produces mineral tags in dentinal tubules, it has the potential to offer high micro-leakage resistance (Han and Okiji 2011). This material has many favorable biological properties and encourages dentine bridge formation with no inflammatory pulp response through secretion of transforming growth factor (TGF)–β1 (Laurent and Camps 2012; Nowicka et al. 2013). When it was introduced to the market, it was described as having “similar mechanical properties and mechanical behaviour as human dentin,” and a clinical trial subsequently concluded that Biodentine could be successfully used as a posterior restoration material for up to 6 mo (Koubi et al. 2013). A clinical trial reported in 2015 by Hashem et al. reported promising results on the healing dynamics of periapical tissues when Biodentine was placed as an indirect pulp cap in deep carious lesions in teeth with clinical signs of reversible pulpitis (Hashem et al. 2015). However, review articles published to date have unanimously concluded that a lack of clinical outcome data precludes a definitive conclusion about this novel material (Chen and Jorden 2010; Meshack et al. 2012; Bogen and Chandler 2012; Malkondu et al. 2014; Rajasekharan et al. 2014).
The aim of this study was to determine if the clinical performance of Biodentine would be acceptable for the restoration of root caries lesions in older adults. The null hypothesis of this noninferiority study stated that 1-y survival of Biodentine restorations would be inferior to the combined success rates of a high-viscosity glass ionomer cement (Fuji IX GP Extra; GC Corporation, Tokyo, Japan) and a resin-modified glass ionomer cement (Fuji II LC; GC Corporation) by at least 15% when used to restore root caries in older individuals.
Materials and Methods
Study Design
A 3-arm randomized controlled clinical trial was conducted comparing Biodentine as the test material and glass ionomer cement (GIC; Fuji IX GP Extra) and resin-modified glass ionomer cement (RMGIC; Fuji II LC) as the 2 control groups. This randomized controlled clinical trial was conducted following the CONSORT (Consolidated Standards of Reporting Trials) guidelines. The study protocol was submitted and given full ethical approval by the Clinical Ethics Committee of the Cork Teaching Hospitals (ECM 4 Y 06/12/11). The study was conducted in compliance with the principles of the Declaration of Helsinki, and written informed consent was obtained from each participant. This trial was registered at clinicaltrials.gov as NCT01866059.
Recruitment
Adults older than 65 y with any of their remaining natural dentition were invited to attend Cork University Dental School and Hospital for a free dental examination. Advertisements were placed in local shopping centers, community centers, and the local press. Contact details of the study coordinator were provided, and patients were allocated appointments. All patients recruited to the study were independently living older adults. No financial rewards were offered to patients, but all treatment costs involved in the study were covered. Recruitment commenced in October 2012 and was completed in November 2013.
Inclusion and Exclusion Criteria
The inclusion criteria for entering this study were as follows:
Be aged 65 y or older
Present a minimum of 2 teeth with active (soft on probing with a ball-ended probe) cavitated root caries lesions
Have sufficient cognitive ability to understand consent procedures
The exclusion criteria for this study were as follows:
Medically frail individuals (American Society of Anesthesiologists [ASA] IV)
Individuals with any painful symptomology other than sensitivity
Individuals with severe periodontal disease
Individuals requiring antibiotic prophylaxis for invasive dental treatment
Data Collection
Each participant completed a questionnaire that recorded age, sex, medical history including medications, fluoride exposure, oral and denture hygiene practices, smoking and alcohol consumption, diet information, self-reported oral dryness, and socioeconomic information. Clinical examinations were performed and the data were entered into case report forms. Stimulated saliva samples were taken at a separate appointment as patients had to be advised to avoid eating, drinking, smoking, chewing gum, tooth brushing, or mouthwashes for 1 h prior to sample collection. Saliva was collected over a period of 5 min following 1 min of stimulation by having the participant chew a paraffin pellet. Xerostomia was defined as <0.7 mL saliva/min.
Clinical Examination
The clinical examination comprised a hard tissue charting with separate examination of the coronal tooth structure and the root, visible plaque index, a basic periodontal examination, and removable partial denture contacts. Hard tissue charting was recorded following removal of plaque and calculus deposits. A surface was categorized as in close contact with a partial denture if it was within 3 mm of any denture component. Patients who fulfilled the inclusion criteria for the study were invited to participate and given a unique identifier.
Randomization
A computer-generated randomization scheme was generated using STATA 12.1 (StataCorp LP, College Station, TX, USA) for the 8 strata arising from the stratification variables: denture wearing (yes/no), dry mouth (yes/no), and past root caries experience (i.e., treated plus untreated root caries lesions [3 or less, 4 or more]). The randomization ratio was 2:1:1 (2 Biodentine/1 Fuji IX GP Extra/1 Fuji II LC), and the unit of randomization was the tooth. Interventions were randomized in blocks of 6, with the first intervention assigned to the tooth with the lowest number according to FDI World Dental Federation notation and so on. Restorative materials were allocated to root surfaces without any specific pairing scheme for teeth applied. Allocation was concealed from the clinical operator until the time of restoration placement, at which time the research nurse opened a sealed opaque envelope.
Power Calculation
A sample size calculation was performed to demonstrate noninferiority of Biodentine restoration survival rate relative to conventional treatment (GIC and RMGIC) at 1 y, using the tooth as the statistical unit of assessment. The survival of the conventional treatments was estimated to be 85% based on previous studies (McComb et al. 2002; Lo et al. 2006; De Moor et al. 2011). GIC and RMGIC were applied in a ratio of 1:1 in the control group. In determining the sample size, a difference in restoration survival rate of 15% or more was regarded as clinically significant. Using an 80% power and a 5% statistical significance level, we found that 71 restorations per group would be necessary (i.e., 71 Biodentine and 71 control). In anticipation of a 15% dropout rate, this was increased to 82. The sample size was then increased by a factor of 1.5 in an attempt to correct for a lack of independence. Therefore, a total of 123 restorations per group were required at baseline, with an achieved sample of 107 restorations per group (i.e., 107 Biodentine, 107 combined GIC and RMGIC) at 1 y required for adequate power.
Operative Care
All of the operative caries management was completed by a single operator. As in similar studies, the study was not operator blinded because of the different appearance of the materials and the different operative procedures required for placement. Local anesthesia was provided if the patient requested it or if the operator felt it would be necessary. Cavity preparation was carried out with low-speed rotary instruments and hand instruments for the removal of soft carious tissue. Following the principles of modern, minimally invasive caries removal (Banerjee and Watson 2011), only caries-infected dentine was removed. Caries-affected dentine was not removed unless needed for cavity margin seal. Moisture control was achieved with the use of cotton wool rolls and a saliva ejector. Cavities receiving either of the control materials (GIC or RMGIC) were conditioned with a polyacrylic acid (GC Dentin Conditioner; GC Corporation) for 20 s. Both the GIC and RMGIC used were encapsulated versions. In the case of RMGIC, the material was light-cured for 20 s.
For the Biodentine group, cavities were not conditioned. In accordance with the manufacturer’s instructions, 5 drops of liquid were added to the single capsule of powder. All mixing was completed by 1 research assistant who had been provided with training by the manufacturer. After mixing for 30 s at 4,000 to 4,200 rpm, the Biodentine was applied and allowed to set untouched for 12 min. The final restorations in all groups were then coated with a varnish (G-coat plus; GC Corporation).
Evaluation of Restorations
Patients were reviewed 6 mo and 1 y after the restorations had been placed by a calibrated clinician who was not involved in restoration placement and who was blinded to material allocation. Restorations were assessed according to modified US Public Health Service criteria (van Dijken 1986). In this study, failure was defined as complete loss of the restoration, fracture of the restoration exposing the base of the cavity, the presence of recurrent caries, replacement of the restoration with another restoration, patient experiencing pain in the tooth, or loss of the tooth. Failed restorations were replaced by the evaluating dentist on the day of review.
Statistical Analysis
All data were entered into SPSS (version 22; SPSS, Inc., an IBM Company, Chicago, IL, USA) software. Cumulative survival proportions at 6 mo and 1 y were defined as the number of restorations still in situ or with acceptable marginal defects or wear at that time point, divided by the total number of restorations assessed in that group.
A logistic regression model with survival of the restoration at 1 y as the outcome variable was fitted using Stata. The explanatory variables included were age, sex, restorative material, proximity of restoration to gingival margin (supragingival or within 1 mm of gingival margin/subgingival) tooth location (anterior or posterior), root surface restored (buccal, mesial, distal, palatal, or lingual), xerostomia, past root caries experience, and partial denture contact.
Individual restorations could not be assumed to be independent as each participant received at least 2 restorations, and the usual method of calculating the standard errors of the logistic regression parameters could not be used. Thus, these parameters were estimated based on 5,000 bootstrap samples from 81 participants. The tests of significance of the logistic regression parameters were based on these bootstrap estimates of the standard errors. A 1-y success rate of 85% with a noninferiority limit of 15% meant that a success rate of at least 70% would be acceptable to consider further trials of the Biodentine material for root caries. Thus, the lower limit of the odds ratio for the restorative material in this trial was set at 0.41. This implied that the lower limit of a 1-sided 95% confidence interval (CI) (or 2-sided 90% CI) should be greater than 0.41 for inferiority to be rejected.
Results
The CONSORT flow diagram is illustrated in the Figure. In total, 334 adults attended for examination after receiving information about the study. Of these, 249 were excluded: 247 did not fulfill the criteria, and upon receiving further information about the treatment randomization in the study, 2 individuals declined to participate and were excluded. Eighty-five individuals with 305 root caries lesions participated in the study. In total, 151 lesions were assigned to receive Biodentine, 77 lesions to Fuji IX GP Extra, and 77 to Fuji II LC. Of the 85 participants, 1 patient was lost to follow-up at 6 mo and 4 were lost to follow-up at 1 y. Two of these patients were unwell, and a further 2 could not be contacted by telephone and did not respond to letters sent to their addresses. Therefore, 303 restorations in 84 participants were assessed at 6 mo posttreatment, and 291 restorations in 81 participants were assessed at 1 y posttreatment.
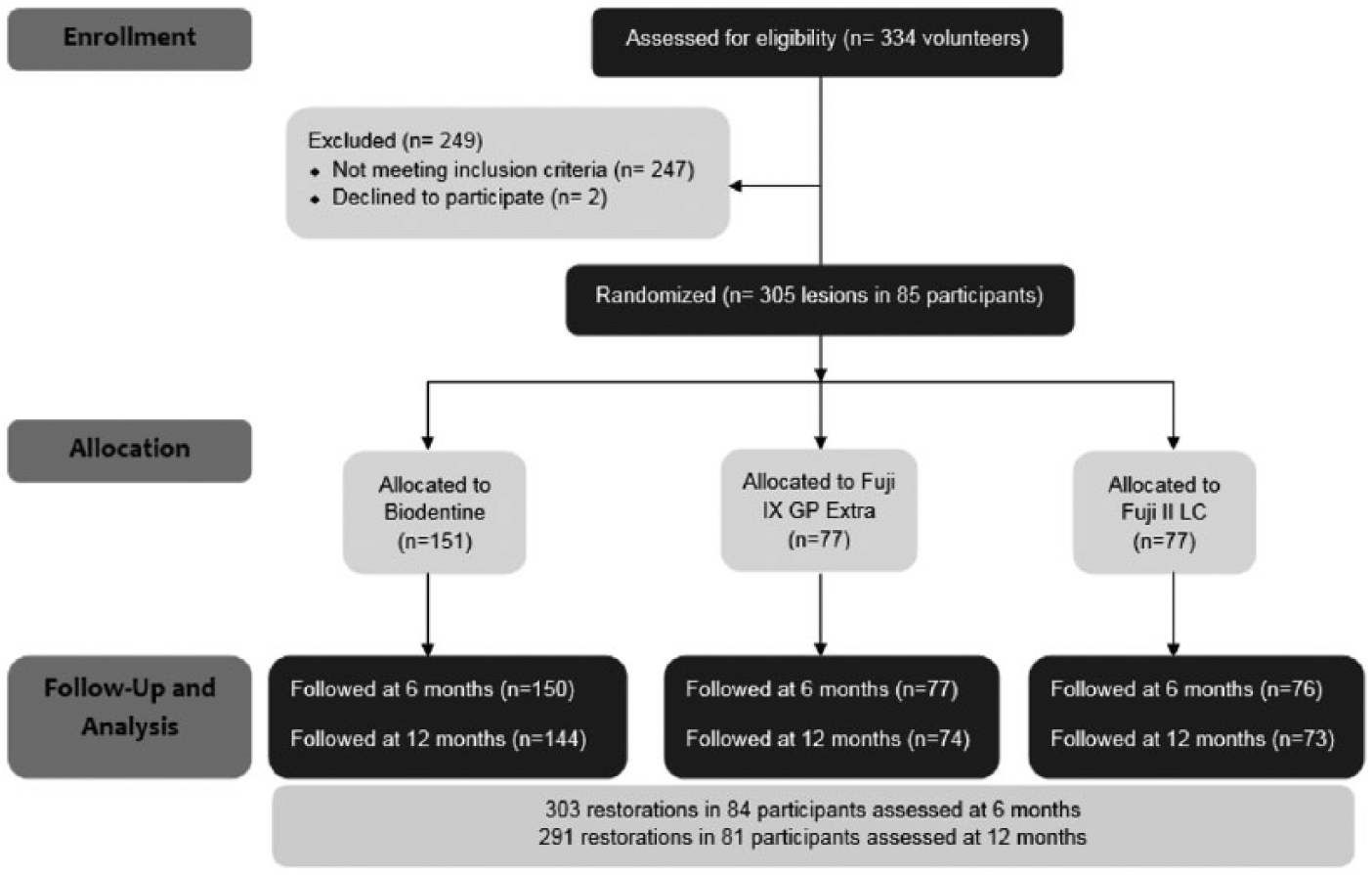
CONSORT flow diagram.
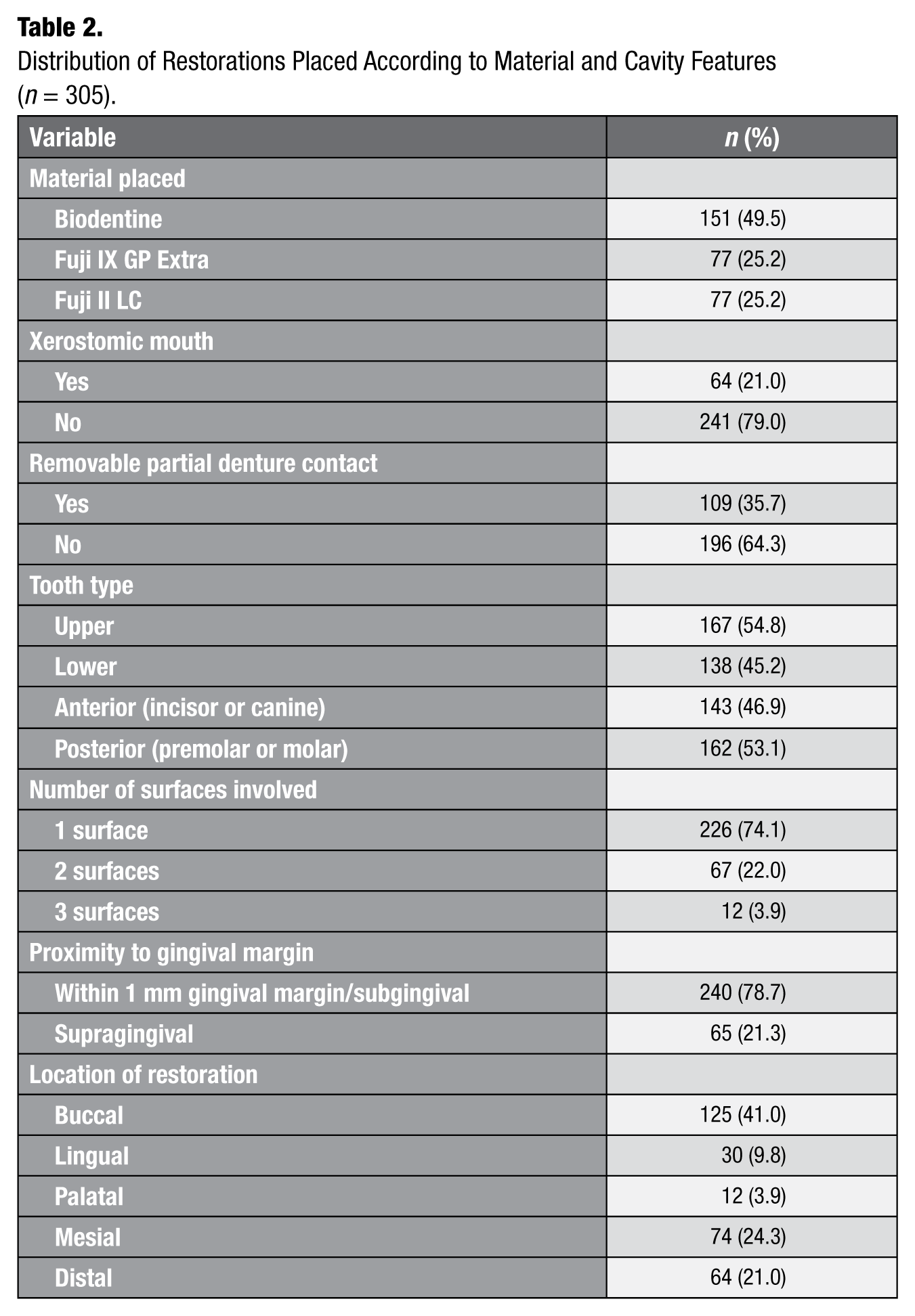
Table 1 illustrates the baseline demographics of the study participants, and Table 2 describes the characteristics of each cavity that was restored. Fifty-four male participants and 31 female participants with a mean (SD) age of 71.9 (4.9) y were included in this study. Most participants (35%) received 2 restorations, and 78% of participants received 4 restorations or fewer. Most of the cavities restored were confined to 1 root surface (74.1%) and were located on the buccal (41%) or proximal surfaces (45.3%). Of the cavities, 78.7% were within 1 mm of the gingival margin or extended subgingivally.
Baseline Demographic and Clinical Characteristics of Participants (n = 85).
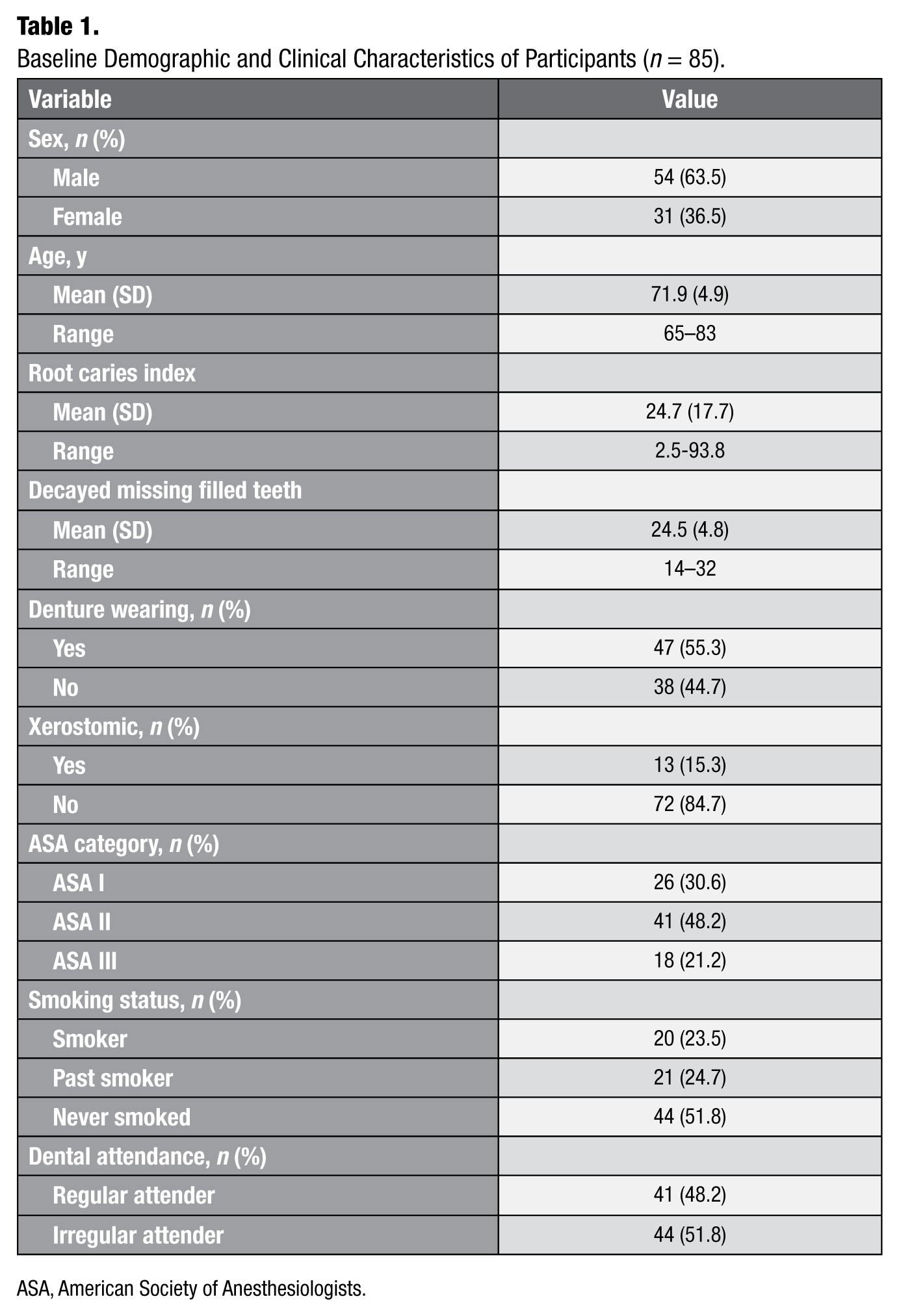
ASA, American Society of Anesthesiologists.
Distribution of Restorations Placed According to Material and Cavity Features (n = 305).
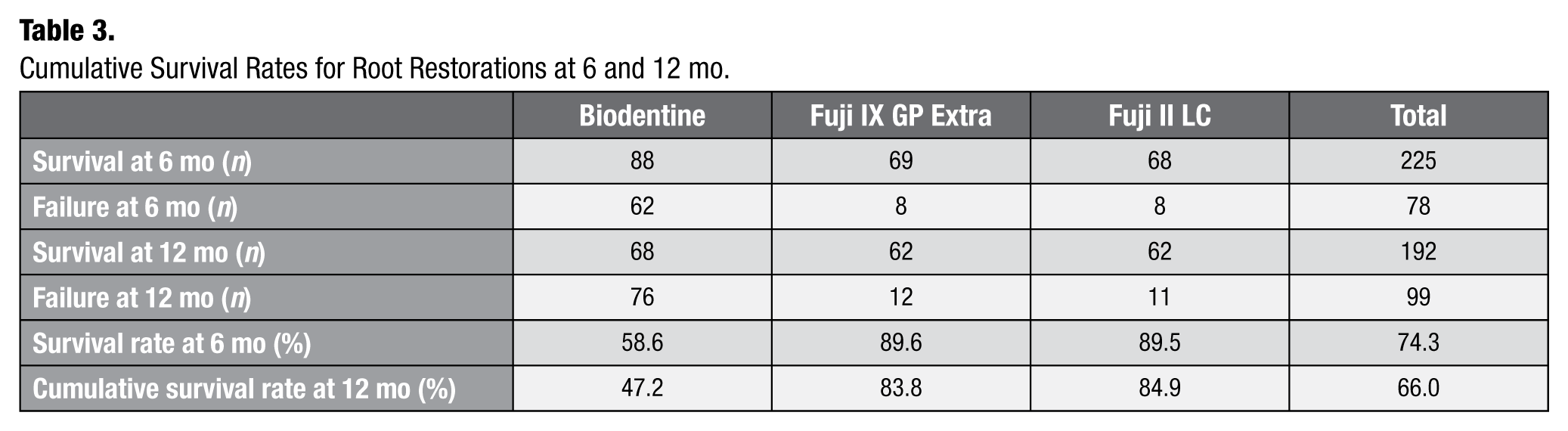
At 6 mo, 88 (58.6%) of Biodentine restorations were assessed as being clinically acceptable, and at 1 y, 68 (47.2%) of Biodentine restorations were clinically acceptable (Table 3). Of the 76 restorations that failed over the 12-mo period, 11 had developed recurrent caries and 65 were completely or partly missing. Most failures occurred within the first 6 mo of placement. Of the Fuji IX GP Extra restorations, 89.6% were clinically acceptable at 6 mo, and 83.8% were clinically acceptable at 1 y. Of the 12 restorations that failed within the year, 3 were due to recurrent caries, 8 were completely or partly missing, and 1 was due to loss of the tooth. Of the Fuji II LC restorations, 89.5% were clinically acceptable at 6 mo, and this had fallen to 84.9% at 1 y. Eleven restorations in total failed within 12 mo of placement, and 4 of these were due to recurrent caries. The remaining 7 were completely or partly missing.
Cumulative Survival Rates for Root Restorations at 6 and 12 mo.
The results of the logistic regression model are reported in Table 4. Of the variables examined, Biodentine restorative material, xerostomia, and close proximity to the gingival margin/extension of the cavity subgingivally were all associated with an increased risk of restoration failure. Restorations placed on the distal root surface were found to have increased odds of success at 1 y compared to those placed on the buccal root surface. The lower limit of the 90% CI for the OR of restorative material was 0.06, which fell well below an acceptable OR of 0.41; therefore, the null hypotheses of inferiority by greater than 15% cannot be rejected at the 5% level of significance.
ORs and 95% CIs for Survival of Restorations According to Different Variables.
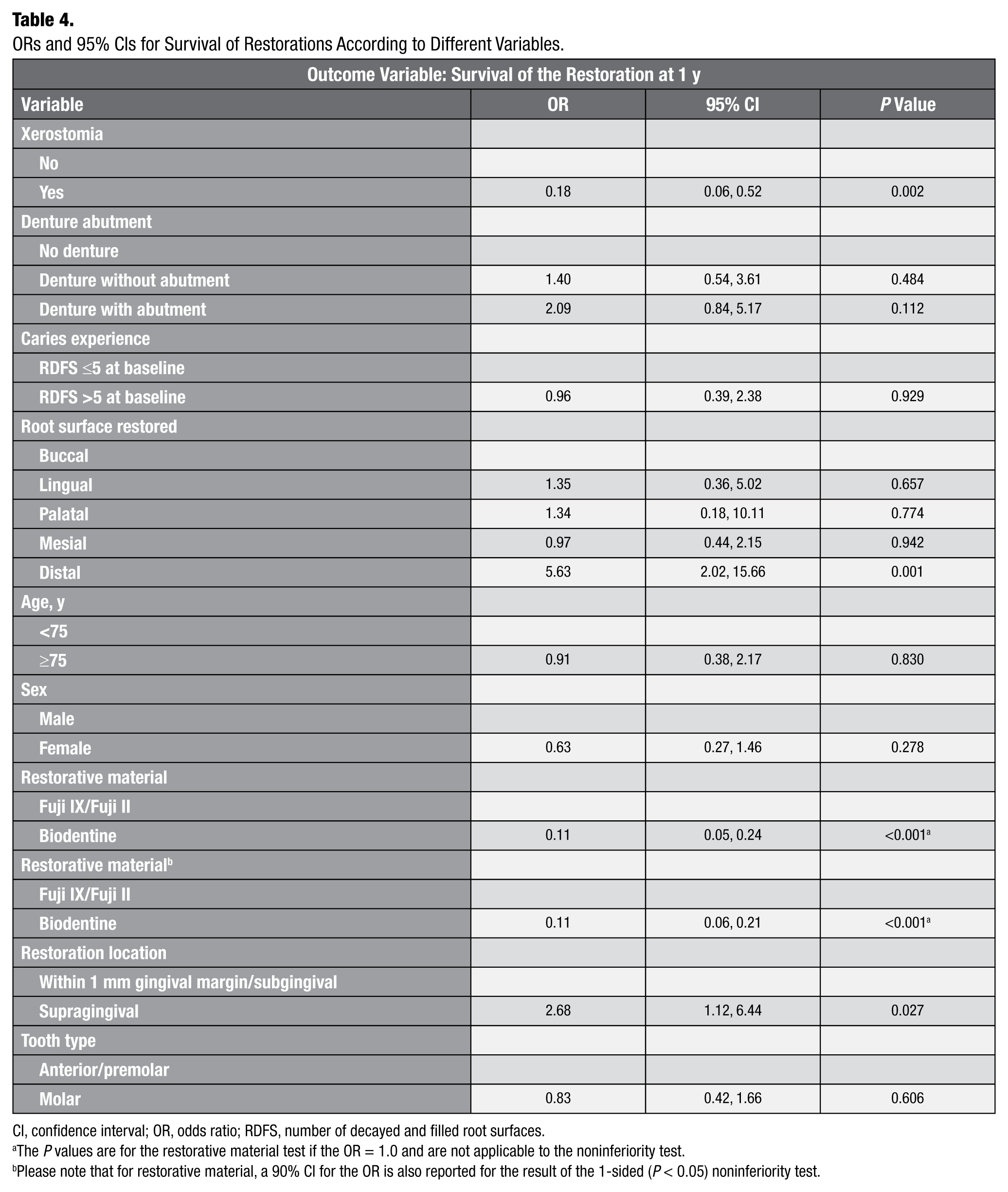
CI, confidence interval; OR, odds ratio; RDFS, number of decayed and filled root surfaces.
The P values are for the restorative material test if the OR = 1.0 and are not applicable to the noninferiority test.
Please note that for restorative material, a 90% CI for the OR is also reported for the result of the 1-sided (P < 0.05) noninferiority test.
Discussion
There is a scarcity of data regarding the performance of different restorative materials for the operative treatment of root caries. In particular, most data available relate to profoundly xerostomic patients after radiotherapy to the oral cavity. This study represents one of a small number that recruited independently living older adults without a history of oral cancer and radiotherapy.
Unusually for oral research, more men than women participated in this study. While approximately equal numbers of males and females were assessed for eligibility, women tended to have more treated root caries lesions (i.e., more restorations on their root surfaces), while men tended to have more active cavitated lesions and were therefore eligible for participation in this research. Fifteen percent of participants displayed hyposalivation as measured by timed collection of stimulated saliva. This proportion is not surprising as a recent meta-analysis comparing the salivary flow rates of younger and older adults found that the aging process is associated with reduced salivary flow even in nonmedicated individuals (Affoo et al. 2015). Over half of participants (55.3%) wore a removable dental prosthesis, which is a recognized risk factor for root caries (Ritter et al. 2010). The mean decayed missing filled teeth of the group was 24.7, which is similar to that reported for this age group in the most recent national oral health survey in Ireland (Whelton et al. 2007).
Resin composite could not be used as a control in this study as many root caries lesions extend subgingivally, and isolation would not have been possible to allow predictable dentine bonding. Therefore, both a conventional high-viscosity GIC and an RMGIC were chosen as controls. Previous clinical studies have shown that both of these materials have similar survival rates in root caries lesions (Lo et al. 2006; da Mata et al. 2015). There was a higher rate of failure of Biodentine restorations compared to the Fuji IX GP Extra or Fuji II LC. As the operator placing the restorations would have had more clinical experience in handling glass ionomer cement and resin modified cement, there was concern that operator technique may have increased the failure rate of the material. However, an analysis comparing the survival of the first 40 Biodentine restorations to the final 40 did not show any statistically significant difference between the 2 groups, thus reducing the probability that the failures could be attributed to an operator “learning curve.”
Encapsulated versions of the GIC and RMGIC were used in this study, and so the powder/liquid ratio of these materials and handling characteristics were consistent. Despite following the manufacturer’s instructions (i.e., adding 5 drops of liquid to the powder in the capsule), there was more variability in the consistency of the Biodentine, and this may be a factor in the survival of these restorations. It is also important to note that the setting time of Biodentine is 12 min, which is much longer than that of Fuji IX GP Extra (2.5 min) or Fuji II LC (command set in 20 s). This longer setting time allows a wider window of opportunity for moisture contamination during the initial set, which would weaken the final cement.
In all materials, the risk of failure was higher when placed in a cavity that was in close proximity to the gingival margin (within 1 mm) or that extended subgingivally. Seventy-nine percent of cavities restored in this study were located in this area and would have been subject to the dynamic flow of gingival crevicular fluid (GCF). This may be detrimental to Biodentine restorations, which demonstrate a high level of washout (Grech et al. 2013). This tendency of the freshly prepared cement to disintegrate upon early contact with blood, saliva, or GCF is a fundamental drawback when placing this material subgingivally.
As is the nature of carious lesions on root surfaces, many of the cavities were broad and shallow in form. Box-form cavities were not prepared, and conservative caries removal dictated cavity design. Consequently, the restorations placed were thin in section. It is probable that most of the restorations placed in this clinical trial were shallower than those in the trial reported by Koubi et al. (2013), which restored class II cavities in posterior teeth. There is no minimum bulk recommended for Biodentine restorations in the manufacturer’s instructions. Also, large areas of the cavity floor of these cavities were composed of caries-affected dentine; therefore, the bonding substrate was caries-affected dentine rather than normal-cut dentine. In the package inset, the manufacturers of Biodentine recommend that as much decay as possible should be removed from the cavity. An in vitro study is currently running to assess if and how much carious tissue can be left. A combination of all the factors discussed above may account for the higher failure rates reported in this trial than the previously published clinical trial (Koubi et al. 2013).
The survival rates of Fuji IX GP Extra and Fuji II LC in this study were similar to those reported in similar studies on the restoration of root caries (Lo et al. 2006; da Mata et al. 2015).
Conclusions
Based on the results of this study, Biodentine cannot be recommended for the restoration of root caries in older adults. Fuji IX GP Extra and Fuji II LC displayed similar success rates, and GIC and RMGIC continue to be the best available options for the operative treatment of root caries.
Author Contributions
M. Hayes, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; C. da Mata, contributed to data acquisition and analysis, critically revised the manuscript; S. Tada, contributed to data acquisition, critically revised the manuscript; G. McKenna, M. Cole, F.M. Burke, P.F. Allen, contributed to conception and design, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
M. Hayes was supported by a grant awarded by the Health Research Board (HPF/2012/7). This study was financially supported by Septodont. Saliva testing kits were provided by Ivoclar vivadent.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.