
Abstract
This systematic review aimed to assess the association between food and drink consumption around bedtime—specifically, food and drinks containing free sugars—and the risk of dental caries in children. Five electronic databases were searched (PubMed, Ovid Medline, EMBASE, Web of Science, and Scopus) to identify studies that investigated any relationship between food and drink around bedtime and dental caries in 3- to 16-y-old children. The Agency for Healthcare Research and Quality domain guidelines were used to assess the quality of the individual studies, while GRADE guidelines assessed the quality of studies based on the body of evidence. From 1,270 retrieved titles, 777 remained after removal of duplicates. Of these, 72 were reviewed in full. Eighteen studies fulfilled the inclusion criteria and were included in the analysis: 13 cross-sectional, 4 cohort, and 1 case-control. Studies were categorized into 3 age groups: 3- to 5-y-old, 6- to 11-y-old, and 12- to 16-y-old children. Based on the Agency for Healthcare Research and Quality criteria, 6 of the 18 studies were rated as providing good-quality evidence; 8 were rated as fair; and 4 were categorized as being of poor quality. It was not possible to conduct a meta-analysis, because of the considerable variations in the type of bedtime exposure and outcome measures. The studies showed a consistent positive association across the 3 age groups, with all 7 studies on preschool children reporting significant positive associations. However, the quality of the body of evidence pertaining to the consumption of food and drinks at bedtime (specifically, food and drinks containing free sugars) and risk of caries was rated as “very low.” The results suggest that restricting free sugars before and at bedtime may reduce the risk of caries, but studies with improved design are needed to confirm this.
Introduction
Dental caries is the most common global disease affecting children (Marshall et al. 2003; Marcenes et al. 2013). The caries process involves the interaction among acid-producing bacteria, sugars, and host factors, including teeth and saliva over time (Selwitz et al. 2007). Free sugars are monosaccharides and disaccharides that manufacturers, cooks, or consumers add to food and drinks and are the sugars naturally found in honey, syrups, fruit juices, and fruit juice concentrates (World Health Organization 2015). The World Health Organization (2015) guidelines on sugars intake for adults and children recommend that intake of free sugars not be >10% of one’s total energy intake, with a conditional recommendation to limit this intake to <5%. The Scientific Advisory Committee on Nutrition (2015) also recommended restricting daily free sugars intake of the population to <5% of total dietary intake. While the totality of evidence provides a basis for limiting the amount of free sugars consumed in the diet, few studies have explored the relationship between caries and patterns of eating free sugars throughout the day (Moynihan and Petersen 2004; Scientific Advisory Committee on Nutrition 2015).
Food and drink consumed around bedtime as a caries risk factor has not been explored through systematic review. Consuming food and drinks containing free sugars around bedtime could be an important risk factor because salivary flow decreases markedly during sleep, reducing the self-cleansing effect and buffering capacity of saliva in the oral cavity (Weber-Gasparoni et al. 2007). This reduced nocturnal salivary flow shifts the balance toward demineralization rather than remineralization (Nauntofte et al. 2003). Evidence-based clinical guidelines recommend twice-daily toothbrushing with a fluoridated toothpaste, with 1 of the occasions being before bedtime (Duckworth and Moore 2001; Marinho et al. 2003). Therefore, it is important that studies assessing the association between caries and bedtime eating/drinking control for fluoride exposure, particularly at bedtime, as an important confounder. Another important factor to consider is the total amount of free sugars consumed during the day, because bedtime free sugars consumption could be a proxy measure of children’s high total daily intake of free sugars.
This systematic review addressed 3 questions: 1) Does food or drink consumption at bedtime increase the risk of dental caries in children? 2) Does consuming foods containing free sugars at bedtime increase the risk of dental caries in children? 3) Does consuming drinks containing free sugars at bedtime increase the risk of dental caries in children?
Materials and Methods
Protocol and Registration
This review followed the PRISMA guidelines (i.e., Preferred Reporting Items for Systematic Reviews and Meta-analyses; Moher et al. 2015). The protocol was registered in the National Institute for Health Research database (http://www.crd.york.ac.uk/PROSPERO; protocol CRD42016033744).
Eligibility Criteria
Studies included in this review were selected following PICOS elements, as follows (Centre for Reviews and Dissemination 2009).
Participants
Healthy children aged 3 to 16 y were included. This age coincides with the time of greatest caries risk for children (Mejàre et al. 2014).
Intervention and Exposure
The exposure was any food and drink consumption around bedtime or before sleep—specifically, consuming food or drinks containing free sugars around bedtime. Time limits were not set in terms of the length of time prior to bedtime that children had eaten or drank. However, studies had to make reference to food and drink consumption related to bedtime or sleeping.
Comparison
Comparison included either no comparison group or a control group not exposed to food/drink around bedtime.
Outcome
The outcome was dental caries or early childhood caries as assessed through clinical examination. Studies reported caries prevalence, incidence, and severity as measured by DMFT, dmft, DMFS, dmfs, DFS, and deft or by comparisons between caries or no-caries groups or higher- and lower-caries groups.
Study Design
Randomized controlled trials (RCTs) and non-RCTs, as well as prospective and retrospective cohort studies, case-control studies, and cross-sectional studies, were considered for inclusion.
The excluded studies did not include children aged 3 to 16 y or were studies that assessed nocturnal breastfeeding or nocturnal bottle-feeding with infant formula milk. Studies that assessed medicines containing sugars and therapeutic diets provided to children with health problems or medical conditions (other than diabetes mellitus) were also excluded.
Information Sources and Search Strategy
A comprehensive search identified relevant studies through 5 electronic databases (PubMed, Ovid Medline, EMBASE, Web of Science, and Scopus). There was no restriction placed on the time of publication (up to May 10, 2017); the search was limited to English-language articles. A Google Scholar and reference search and a hand search of reference lists from identified publications and previously published related systematic reviews were also carried out to identify any other relevant published work and potential studies eligible for inclusion. The search strategy is shown in Appendix 1.
Study Selection and Data Extraction
Two reviewers (K.B., S.W.P.) independently assessed the titles and abstracts of all identified studies. The authors also obtained and independently assessed the full articles of the studies that potentially met the inclusion criteria but lacked information in the title and abstract. A third reviewer (V.M.) resolved any disagreements between the 2 reviewers.
The following information was extracted into data extraction forms: study setting, study population, inclusion/exclusion criteria, baseline characteristics, details of the exposure, study methodology, recruitment, study completion rate, dental caries outcomes, and information relating to study quality.
Quality Assessment
The included studies were independently assessed by 2 reviewers using the Agency for Healthcare Research and Quality system (Owens et al. 2010), which assesses 8 domains: study question, study population, comparability of subjects, outcome measurement, statistical analysis, results, discussion, and funding. The quality of the studies was rated as good, fair, or poor (Helfand and Balshem 2009).
For each review question, studies were organized by design (i.e., cohort or cross-sectional) to enable data synthesis by the “best available evidence” (Petticrew and Roberts 2006). The quality of the body of the best available evidence for each research question was then evaluated with the GRADE Working Group guidelines (Atkins et al. 2004). The GRADE system (https://gradepro.org/) rates the overall quality of evidence based on design limitations, consistency of the results across the available studies, the precision of the results, directness, likelihood of publication, and risk bias. The GRADE profile analysis categorized the quality of the body of evidence as high, moderate, low, or very low. Limitations in the study quality, inconsistency of results, uncertainty about the directness of evidence, and the presence of plausible residual confounding lowered the quality grade of the evidence. The footnotes related to these limitations are included in Appendix Table 5 (S1–S3).
Results
Study Selection
The 5 electronic databases identified 1,267 articles; 3 additional studies were identified from references lists. After removal of duplicate articles, 777 articles were included in the screening stage. After title screening, 138 articles were included in the abstract screening stage; 72 articles were then included for full-text reading. Reviewers retrieved and independently assessed the full-text articles of eligible studies, with any disagreements resolved by discussion with the third review author (V.M.). The interobserver agreement between the examiners selecting the articles calculated a kappa score of 0.85, indicating almost perfect agreement. Eighteen studies fulfilled the inclusion criteria and were included in the analysis (Fig.). Excluded studies and the reason for exclusion are provided in Appendix 2.
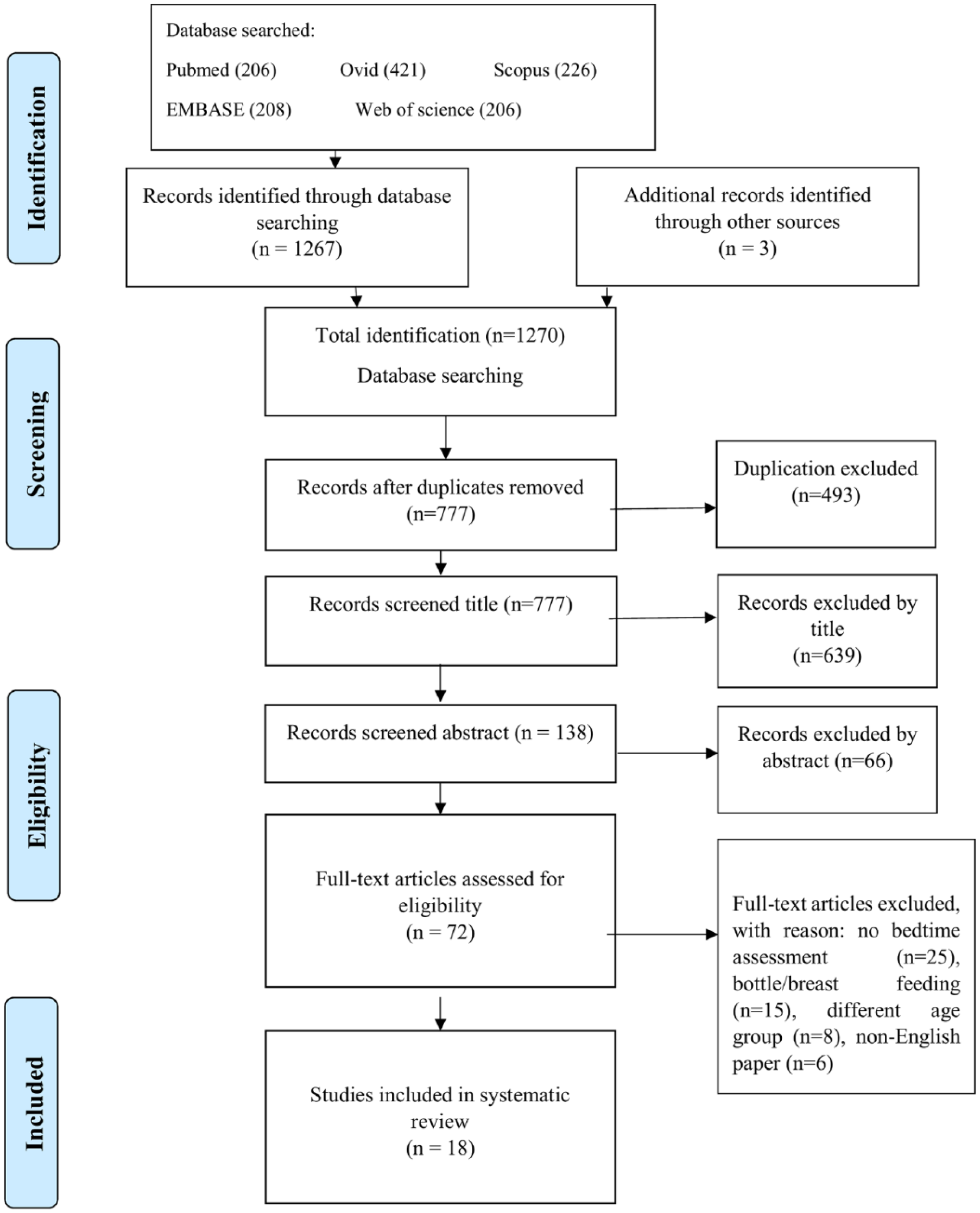
A PRISMA flow diagram showing the number of articles identified at each stage of the search.
Study Characteristics
Table 1 summarizes the characteristics of the included studies. Studies were classified according to 3 age groups: 3- to 5-y-olds, 6- to 11-y-olds, and 12- to 16-y-olds. Of the 18 studies, 4 were cohort studies (Rugg-Gunn et al. 1984; Levine et al. 2007; Gao et al. 2010; Lee and Messer 2010). One was a case-control study (Palmer et al. 2010), and 13 were cross-sectional studies (Palmer 1971; Levine 2001; Sayegh et al. 2002; Skeie et al. 2006; Declerck et al. 2008; Hashim et al. 2009; Li et al. 2011; Huew et al. 2012; Lueangpiansamut et al. 2012; Lakhanpal et al. 2014; Hoffmeister et al. 2016; Palacios et al. 2016; Goodwin et al. 2017). Appendix 3 provides the full list of references. Eight studies assessed caries in primary teeth (Sayegh et al. 2002; Skeie et al. 2006; Declerck et al. 2008; Hashim et al. 2009; Gao et al. 2010; Palmer et al. 2010; Li et al. 2011; Hoffmeister et al. 2016). Seven articles investigated caries in permanent teeth (Palmer 1971; Rugg-Gunn et al. 1984; Huew et al. 2012; Lueangpiansamut et al. 2012; Lakhanpal et al. 2014; Palacios et al. 2016; Goodwin et al. 2017). Three articles assessed caries in primary and permanent teeth (Levine 2001; Levine et al. 2007; Lee and Messer 2010).
Summary of Included Studies: Characteristics and Exposure-Outcome Relationship.
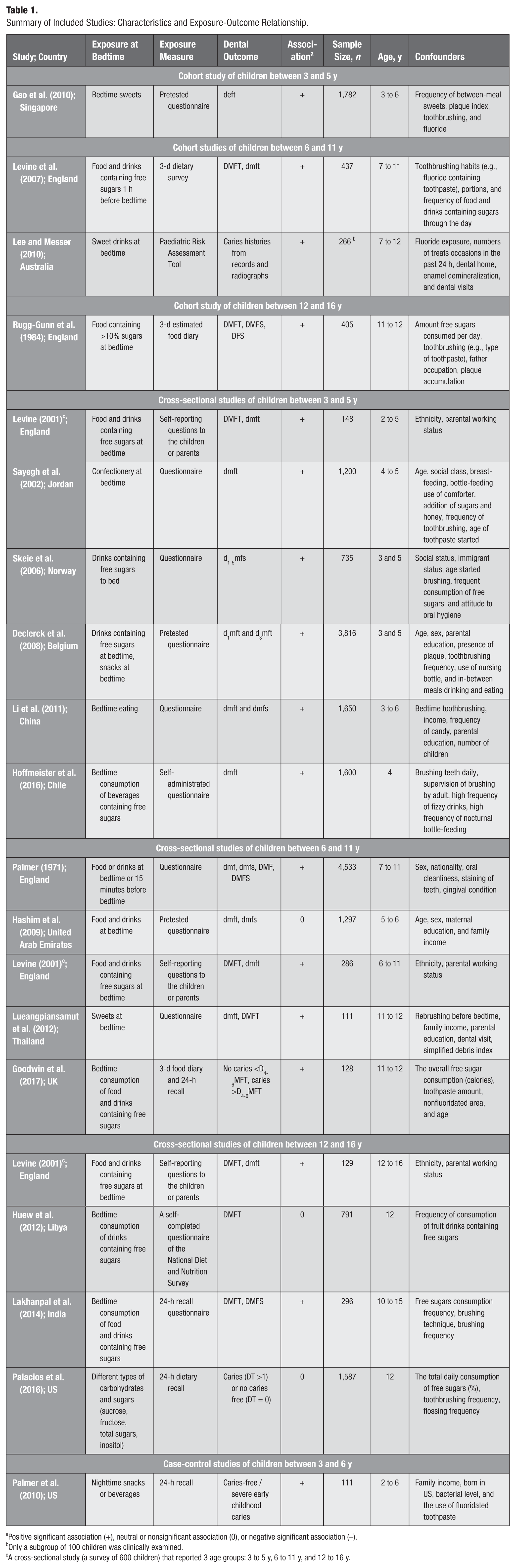
Positive significant association (+), neutral or nonsignificant association (0), or negative significant association (–).
Only a subgroup of 100 children was clinically examined.
A cross-sectional study (a survey of 600 children) that reported 3 age groups: 3 to 5 y, 6 to 11 y, and 12 to 16 y.
Quality Assessment of Studies
In terms of evidence quality per the criteria of the Agency for Healthcare Research and Quality, 6 studies were rated as good, 8 as fair, and 4 as poor (see Appendix 4). A meta-analysis to address any of the 3 review questions was not feasible, because of the inability to pool the data from cross-sectional studies owing to the variability in the caries outcomes (i.e., DMFS, dmfs, DMFT, dmft, caries, and fissure caries increment) and the different ways that the outcomes were presented (i.e., mean caries index, odds ratios, caries prevalence, and number of children with caries experience). There were also variations in the follow-up periods and the type of the exposures at bedtime, specifically related to whether the exposure contained free sugars. For all 3 research questions, it was not possible to produce a risk-of-bias funnel plot, because only 4 longitudinal studies were included in the systematic review.
Quality Assessment of the Body of Evidence with GRADE
As part of the GRADE process, the consistency of the associations across the study types was reviewed for the 3 age groups (Table 1). For children aged 3 to 5 y, all 7 studies (1 cohort, 5 cross-sectional, and 1 case-control) showed a consistent positive association between bedtime food/drink and dental caries. For children aged 6 to 11 y, both cohort studies and 4 of the 5 cross-sectional studies showed a significant positive association. One study showed a nonsignificant association. For children aged 12 to 16 y, 1 cohort study and 2 of the 4 cross-sectional studies reported a significant positive association. The remaining 2 cross-sectional studies showed a nonsignificant association.
In the absence of RCTs, the GRADE assessment for each research question was based on cohort studies and cross-sectional studies. Three GRADE profile tables were produced to address the 3 review questions (see Appendix 5).
Does Consuming Food or Drinks at Bedtime Increase the Risk of Dental Caries?
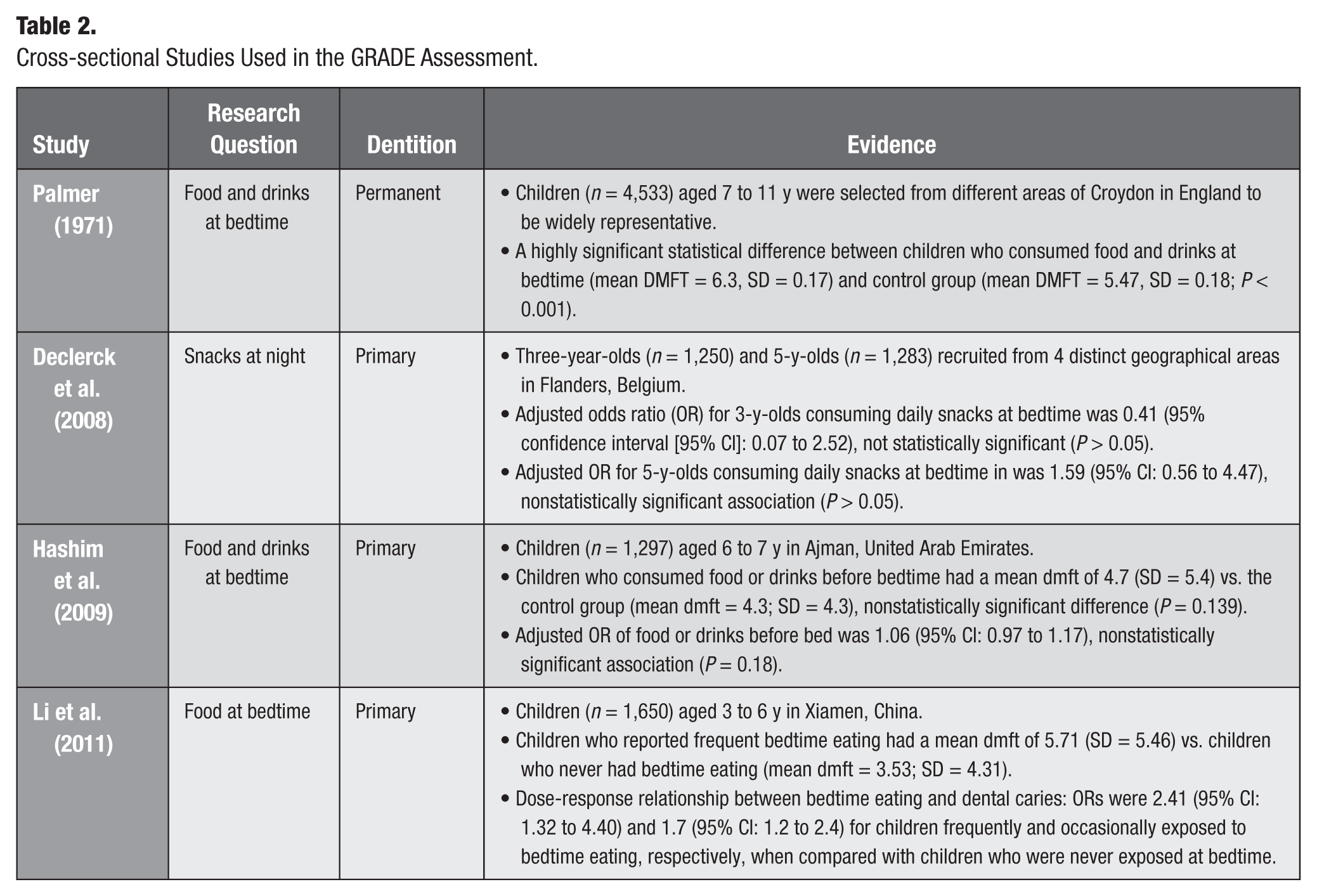
Four cross-sectional studies provided the best available evidence on the effect of consuming foods or drinks at bedtime and on caries risk (Table 2). Three studies investigated primary teeth, and 1 assessed children with permanent teeth. The studies were consistent with 3 of the 4 showing a statistically significant association between food or drinks at bedtime and risk of dental caries (Palmer 1971; Declerck et al. 2008; Li et al. 2011). Two cross-sectional studies assessed the consumption of food and drinks at bedtime without specifying if the food or drinks contained free sugars. Neither study reported food and drinks separately (Palmer 1971; Hashim et al. 2009; Table 2). Overall, the quality of evidence was “very low” for assessing the association between food and drinks consumed at bedtime and caries in children (see Appendix Table 5: S1). The reason for the quality downgrade was related to the plausible confounding that would reduce the effect. The studies did not control for confounding factors, such as brushing before bedtime, fluoride exposure, and daily intake of free sugars.
Cross-sectional Studies Used in the GRADE Assessment.
Does Consuming Foods Containing Free Sugars at Bedtime Increase the Risk of Dental Caries in Children?
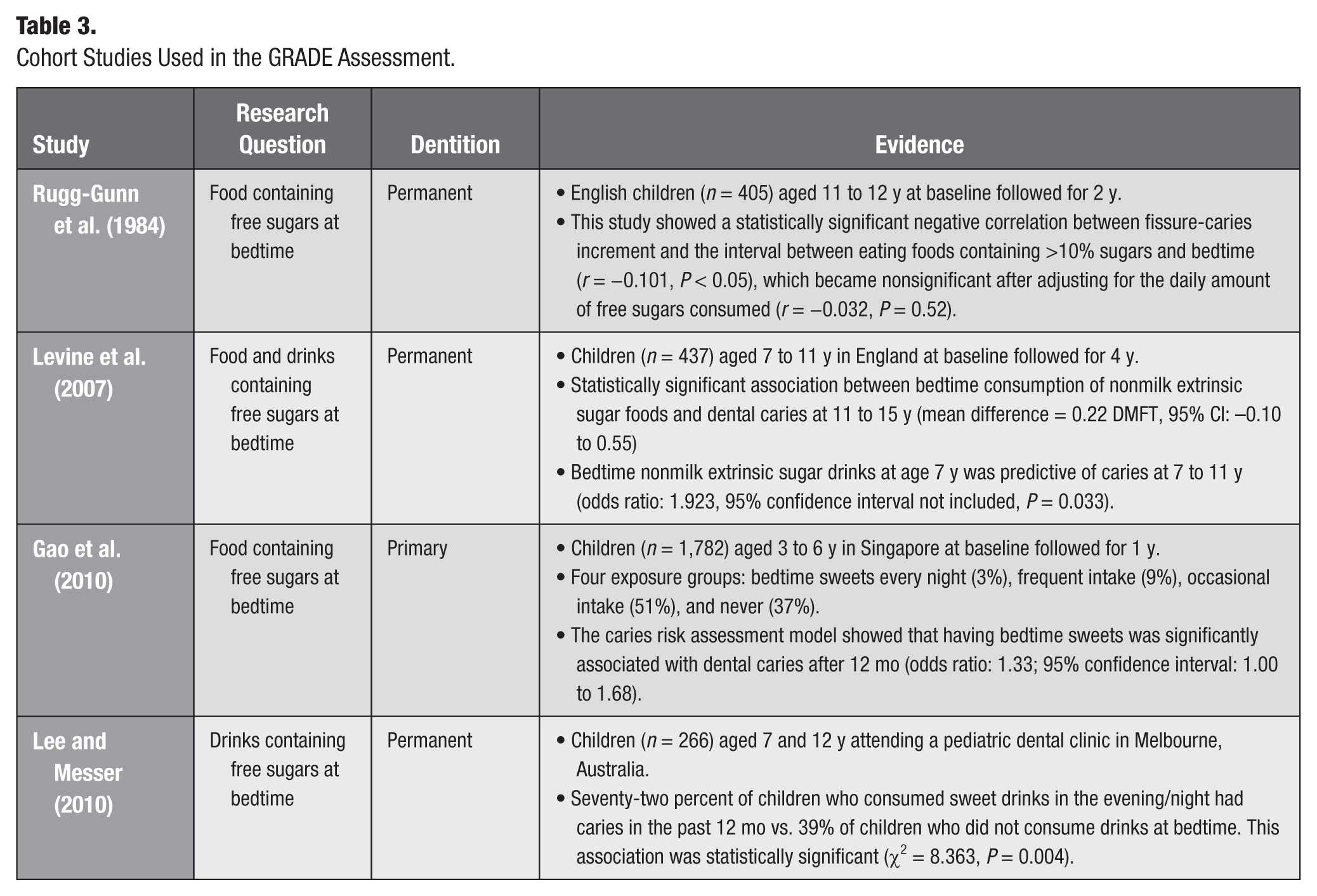
Three cohort studies investigated the causal relationship between consuming food containing free sugars at bedtime and caries risk and were used for the GRADE profile analysis (Appendix Table 5: S2). Two cohort studies included children with permanent teeth, and 1 included children with primary teeth. The cohort studies were consistent in showing higher caries levels among children specifically exposed to food containing free sugars at bedtime (Table 3; Rugg-Gunn et al. 1984; Levine et al. 2007; Gao et al. 2010). The quality of the evidence was downgraded to very low because of the plausible confounding. Of the 3 cohort studies, 2 did not control for the total amount of free sugars consumed during the day. All cohort studies controlled for toothbrushing and fluoride; however, none of them assessed bedtime toothbrushing.
Cohort Studies Used in the GRADE Assessment.
Consistent with the GRADE analysis of the cohort studies, analysis of 3 cross-sectional studies showed a positive statistical association between bedtime exposure to food containing free sugars and dental caries in children (Table 1). One cross-sectional study specifically assessed the association between sweets (i.e., the consumption of snacks containing free sugars) and caries in permanent teeth (Lueangpiansamut et al. 2012), while 1 study assessed consumption of confectionery at bedtime in primary teeth (Sayegh et al. 2002). The third study assessed caries in primary and permanent teeth (Levine 2001). These cross-sectional studies also found an increased risk of dental caries among children who consumed snacks containing free sugars at bedtime (Levine 2001; Sayegh et al. 2002; Lueangpiansamut et al. 2012).
Does Consuming Drinks Containing Free Sugars at Bedtime Increase the Risk of Dental Caries in Children?
Two cohort studies were used for the GRADE profile analysis relating to the risk of dental caries and consumption of drinks containing free sugars at bedtime (Appendix Table 5: S3; Levine et al. 2007; Lee and Messer 2010). Both cohort studies assessed dental caries in children with permanent teeth and separately reported drinks and foods containing free sugars. The studies showed a consistent statistically significant positive association between risk of dental caries and consumption of drinks containing free sugars at bedtime. The GRADE profile analysis classified the evidence as very low (Appendix Table 5: S3).
Data from cross-sectional studies were consistent with the cohort studies. For primary dentition, 4 of the 5 cross-sectional studies found a highly significant association between consuming drinks containing free sugars at bedtime and dental caries (Levine 2001; Skeie et al. 2006; Declerck et al. 2008; Hoffmeister et al. 2016). For the permanent dentition, 1 cross-sectional study showed a statistically significant association between drinks containing free sugars at bedtime and the mean DMFT of children aged 6 to 11 y (Levine 2001).
Although the 3 cross-sectional studies assessed food and drinks containing free sugars and caries in permanent teeth, they did not report data for drinks and foods separately. Two studies showed a significant positive association between consuming food or drinks containing free sugars and dental caries in children (Lakhanpal et al. 2014; Goodwin et al. 2017).
Discussion
This systematic review assessed the evidence related to the caries experience of children aged 3 to 16 y and the consumption of any food or drinks, as well as food and drinks containing free sugars, at bedtime. Eighteen articles were identified that fulfilled the inclusion criteria, all of which were observational studies (i.e., no RCTs). The studies were categorized into 3 age groups to recognize the different eating and drinking habits that children have across the life course. This systematic review provided the most consistent evidence for the relationship between bedtime exposures to free sugars and caries in younger children, with all 7 studies on preschool children (3 to 5 y) reporting statistically significant positive associations.
Despite the studies showing consistent positive associations, the quality of evidence related to all 3 research questions was classified as “very low.” The main reasons for this rating related to the type of study (observational) and the failure to control for plausible confounders. For example, 2 cohort studies assessed drinks containing free sugars at bedtime; however, neither study controlled for the total daily intake of free sugars by children, and for this reason, the evidence was downgraded (risk of plausible confounding).
Study Design
The GRADE criteria for evaluating the strength of the body of evidence recognizes (in the absence of RCTs) the importance of assessing evidence from studies based on other designs. However, observational studies provide lower-quality evidence, and all 18 studies included in this systematic review were observational and, as such, initially classified as “low” (GRADE Working Group and Oxman 2004). Caution should always be applied when relying on cross-sectional studies to assess the relationship between diet and dental caries because one cannot establish a temporal relationship between exposure and outcome. Assessment for the risk of bias with funnel plots was not possible; therefore, the presence of publication bias cannot be excluded, though data were not downgraded for this factor. A further limitation of this systematic review is that it included English-language articles only, which may have increased the risk of publication bias.
Lack of Controlling for Confounders
Eight of the included studies investigated toothbrushing frequency among children (Sayegh et al. 2002; Levine et al. 2007; Declerck et al. 2008; Lee and Messer 2010; Gao et al. 2011; Li et al. 2011; Lakhanpal et al. 2014; Palacios et al. 2016). Four studies assessed other toothbrushing-related factors, such as age of starting toothbrushing (Sayegh et al. 2002; Skeie et al. 2006; Li et al. 2011; Hoffmeister et al. 2016), types of toothpaste (Rugg-Gunn et al. 1984; Sayegh et al. 2002; Lee and Messer 2010), and parental supervision of toothbrushing (Skeie et al. 2006; Hoffmeister et al. 2016). However, only 2 studies specified the timing of toothbrushing as being before bedtime or in the evening (Li et al. 2011; Lueangpiansamut et al. 2012).
Most of the included studies did not control for the daily amount of free sugars consumed by children. Rugg-Gunn et al. (1984) controlled for the daily amount of total sugars consumed and the bedtime exposure and showed that the relationship between bedtime free sugars and caries was not significant after controlling for total daily intake of free sugars. However, Goodwin et al. (2017) controlled for the total amount of free sugars consumed in the day and found that free sugars consumption at night was possibly a more important determinant of caries experience than free sugars snacks during the day. The percentage of energy from free sugars was not significantly different between those children who consumed free sugars in the hour before bed and those who did not (19.8% vs. 18.8%), indicating that bedtime sugars consumption was not simply a proxy for overall free sugars consumption. This systematic review underscores the importance of primary studies assessing fluoride exposure at bedtime and the daily intake of free sugars to exclude these important confounders.
Variations in the Measurement of Bedtime Exposure
The definition of bedtime sugars intake varied among the studies. Two studies (Levine 2001; Levine et al. 2007) used a dietary questionnaire and defined bedtime consumption as 1 h before bed. In contrast, Palmer (1971) defined bedtime as being in bed or within 15 minutes of the child going to bed. Rugg-Gunn et al. (1984) measured the length of time between food/drink intake (categorized according to free sugars content) and bedtime. The other studies defined bedtime without specifying the time before sleep, using more vague questions involving eating or drinking before bedtime (Hashim et al. 2009), bedtime eating (Li et al. 2011), drinks at bedtime (Skeie et al. 2006; Hoffmeister et al. 2016), drinks at night or snacks at night containing free sugars (Declerck et al. 2008), eating sweets before bedtime (Gao et al. 2010; Lueangpiansamut et al. 2012), and confectionery eaten at bedtime or nighttime (Sayegh et al. 2002). The variation identified in this review suggests that future studies should adopt a standard definition or reach a consensus about what is meant by bedtime exposure to allow comparison among them.
Clinical Implications: Existing Guidelines That Make Recommendations about Bedtime Food and Drink Intake
Several clinical guidelines have made recommendations about patterns of eating, which have not been based on systematic review or robust analysis of the best available evidence. The NHS Health Scotland (2012) guideline recommends avoiding foods and drinks containing free sugars at bedtime. This guideline cites supporting evidence from 3 previously published guidelines and 1 professional society lecture paper (Committee on Medical Aspects of Food Policy 1989; World Health Organization 2003; Moynihan 2005; Levine and Stillman-Lowe 2009). Public Health England’s (2014) evidence-based toolkit “Delivering Better Oral Health” recommends not eating or drinking in the last hour before bed. This recommendation cites a cross-sectional study that includes a comparison of 600 children in North England (Levine 2001). The American Academy of Pediatric Dentistry (2017) recommends limiting the provision of drinks and snacks containing free sugars to children at night to reduce the risk of caries in children. The guidelines of the Australian Ministry of Health (2014) recommend that children do not have food and drinks at bedtime. The European Academy of Paediatric Dentistry (2008) guidelines on the prevention of early childhood caries discourage the frequent intake of sweet drinks, especially at nighttime. In the United Kingdom, The Scientific Basis of Oral Health Education recommends avoiding drinks or snacks containing free sugars at bedtime (Levine and Stillman-Lowe 2014). The authors state that the recommendation is supported by the majority of relevant research studies; however, they cite only 1 reference to support this statement (Levine 2001).
This current evidence synthesis provides an objective and more robust analysis of the totality of the evidence relating to children aged 3 to 16 y. Using the current analysis to set recommendations through the GRADE process (Atkins et al. 2004) would require evaluation of factors, including the balance of desirable and undesirable effects, value and preferences, and the use of resources to implement recommendations—which was beyond the scope of the current work. In setting formal recommendations, it would be important to consider any undesirable effects of limiting bedtime dietary intake, such as risk of undernutrition, because bedtime intakes may make an important contribution to overall energy intake. However, only limiting foods and drinks that contain free sugars is likely to reduce overall intake of free sugars, which would have a desirable impact on health.
Research Requirements
This systematic review identified no RCTs and few cohort studies investigating whether bedtime food and drink increases risk of dental caries in children aged 3 to 16 y. The limited and very low-quality evidence highlights the need for well-designed primary research exploring the relationship between food and drink consumption at bedtime, especially food and drinks that contain free sugars, and the risk of dental caries. Future studies should consider adopting a standard definition of bedtime exposure to free sugars and ensure that studies adequately control for the daily amount of free sugars and fluoride exposure at bedtime as key confounders.
Conclusion
The outcome of this systematic review provides consistent albeit very low-quality evidence to support current recommendations to limit consumption of foods and drinks containing free sugars at bedtime for children aged 3 to 16 y. This evidence was more consistent for preschool-age children than older groups.
Author Contributions
K. Baghlaf, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; V. Muirhead, P. Moynihan, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript; S. Weston-Price, contributed to data acquisition, critically revised the manuscript; C. Pine, contributed to conception, design, and data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
We thank the authors of the studies included in this systematic review for providing further information and data from their primary studies.
A supplemental appendix to this article is available online.
The authors received no financial support and declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.