
Abstract
Methods:
In this single-center cross-sectional survey, 57 dentists were given a clinical scenario in combination with a patient’s relevant clinical photographs and radiographs depicting either a Black or White patient presenting with a decayed tooth and associated symptoms of irreversible pulpitis. Explicit bias was measured through a questionnaire, which evaluated participants’ course of treatment, strength of recommendation, and their perception of patients’ dental cooperativeness. Implicit bias was evaluated through brief implicit associate tests.
Results:
Recommendation for root canal treatment (RCT) in the White patient condition was significantly higher than in the Black patient condition (χ2 = 4.77,
Conclusions:
Dentists’ decision making was affected by the race of the patient, resulting in a greater likelihood of extractions (less RCT) for Black patients presenting with a broken-down tooth and symptoms of irreversible pulpitis.
Knowledge Transfer Statement:
The results of this study can be used by clinicians to understand the impact that unconscious racial bias may have on their treatment planning decisions. This information can create awareness, thereby reducing the impact that potential biases can have on the treatment patients receive.
Keywords
Introduction
Bias is an inclination for or against a person or a group, as it allows for ones’ personal opinions to influence judgment. Bias can be further subdivided into implicit and explicit. Explicit biases are thoughts that we express openly, are made with full conscious awareness, and are usually a reflection of the individual’s attitudes and beliefs. The individual believes his or her evaluation to be correct and acts accordingly upon it (Blair and Banaji 1996; Quillian 2006).
Implicit bias arises from subconscious thoughts (cognitive processing) or beliefs that may potentially affect one’s understanding, approach, and decision making. Unlike explicit bias, individuals are not consciously aware of their unintentional bias, which is initiated unknowingly (Devine 1989; Hofmann et al. 2005). The term implicit bias can be used to describe attitudes toward people or associated stereotypes without our conscious knowledge. In dentistry, for example, this may manifest itself in clinicians’ attitudes, with patient management therefore being affected positively or negatively by their patients’ skin color, ethnicity, or racial background (Haider et al. 2013). Implicit and explicit racial biases are distinct from one another, and both have shown to be effective predictors of behavior (Greenwald et al. 2009).
Over the past 50 years (Bobo 2001; Devine et al. 2012), there has been a marked decline in explicit biases toward racial groups, but implicit bias has been shown to still be prominent and persistent (Dovidio and Gaertner 1998). An organization known as Project Implicit was set up, allowing people to take implicit association tests (IATs) to assess unconscious racial bias in the United Kingdom and 18 other countries. The results showed that in the United Kingdom, 69% of participants working in health care had unconscious racial biases. The level of implicit bias ranged from 66.3% in the United States to as high as 70.1% in Europe.
It had been suggested that “race associated differences in health outcomes are due to racism” (Krieger et al. 1993). It is essential that potential effects of racism that may be a cause for differences in health outcomes are examined.
There is also evidence to show that within the US health care system and among health care providers, racism exists (institutional racism). Polls carried out in the United States show that Americans believe Black and White people receive the same level of health care (Lillie-Blanton et al. 2000). However, implicit biases, favoring White people in comparison to Black and Hispanic patients, have been shown to be commonplace among doctors in the United States (Eggers 1995; Smedley et al. 2003; Green et al. 2007; Sabin et al. 2009).
There are significant disparities in the outcome of health care between Black and White patients. Studies have shown that Black patients fare worse in treatment outcomes in almost every category, including cancer, surgical care, and heart disease (Sheifer et al. 2000; Aranda et al. 2008; Bang et al. 2010). Other findings show an association of adverse health outcomes and racial discrimination, indicating that racial biases may contribute to the unequal treatment of certain populations, resulting in subsequent health disparities (Maynard et al. 1986; Whittle et al. 1993; Furth et al. 2000; Epstein et al. 2000; Smedley et al. 2003).
Such disparities in literature have been reviewed, and it has been concluded that the most important contributor to racial disparities in health status is the difference in the quality of medical care given to racial/ethnic minorities (Nelson 2002). Research has shown that such patterns of bias are seen in individuals who believe that they hold no such bias toward members of a particular ethnicity (Banaji et al. 1997). Interestingly, this outcome has also been seen with both Black and White participants (Banaji et al. 1997; Nosek et al. 2014), although to a lesser degree from Black participants.
Endodontic treatment is an effective and predictable treatment option for the management of irreversible pulpitis and apical periodontitis in teeth with severe loss of tooth structure (Salehrabi and Rotstein 2004). Another effective alternative treatment option is extraction; however, the loss of a tooth can result in reduced occlusal stability (Craddock 2007) and compromised aesthetics, and replacement options such as fixed partial dentures or implants may result in damage of adjacent teeth (Saunders and Saunders 1998; Al-Quran et al. 2011) or have a significant economic cost for the individual and/or the community (Jepson and Allen 1999).
A number of studies have researched the influence that implicit and explicit bias may have on medical health care outcomes, but no such study has been conducted within the field of dentistry.
The aim of this study was to determine whether explicit and implicit racial bias predicts the recommendation of root canal therapy or extraction for White and Black patients with irreversible pulpitis. We aim to determine whether different treatment decisions are made for Black versus White patients and to determine whether such differences (if any) are related to the presence of explicit or implicit racial bias. Our null hypothesis is therefore that the race of a patient does not affect dental clinicians’ recommendation for root canal treatment.
Method
This was a single-center cross-sectional survey of dentists working within the endodontic department at the University of Cagliari, Italy, in both the primary and secondary care setting. Eligible participants were qualified dentists working within the hospital (including postgraduate students). Data were collected over a period of 1 mo, commencing in October 2017. A subset of 58 individuals working within the hospital were approached by research staff on a daily basis and invited to participate in the study. This ensured every provider working within the postgraduate department of the hospital had an opportunity to participate during our recruitment phase, of whom 57 agreed to participate and 1 withdrew. The partial results from the participant who withdrew were not used in our analysis, leaving a total of 57 participants.
The survey was registered and approved by the local ethics committee (PG/2017/7126). Verbal and written informed consent was obtained from each participant, and it was also stipulated that they could withdraw at any point during the study. To mitigate response bias, participants were not fully informed of the study’s intent and told only that the purpose of the study was to explore restorability decisions. The participants were directly recruited (unknown to the researchers) and approached within the hospital. They were randomly assigned by a computer-generated randomization list prepared by an investigator with no clinical involvement into group A or B. The corresponding program would subsequently be run and the participant directed to review a clinical vignette depicting either a Black or White patient. The group allocation and sequence were concealed from the researcher and participant.
Clinical Vignette
A vignette was designed to indicate a diagnosis of irreversible pulpitis for which root canal treatment would be a valid treatment option. The same clinical case was used throughout the study with either a Black or a White patient assigned to it. This vignette was created as a web-based survey (Google forms). To reduce bias, images depicting the patient were created from the same individual but generated as a White and a Black version to try and ensure that both were as similar as possible (Fig. 1).

Case presented in vignette. The bottom 4 figures show the images that accompanied the clinical scenario. The top 2 images show those used according to the Black patient and White patient condition.
These new patient images were created by selecting a mixed-race (Black/White) female, who was then made up by a professional makeup artist to look either “White” (northern European) or “Black” (Afro-Caribbean). Professional photos were taken and manipulated using digital software (Adobe Photoshop) to emphasize the European and African features. Ten versions of each race type were created and reviewed by 25 independent evaluators (not involved in the study) who rated each picture with respect to age and attractiveness. After the images were rated, the 2 (1 Black and 1 White) that were most closely matched according to the results (exhibited average scores of 5 on a scale of 1 to 10 and an average age of 30 to 35 y) were selected.
A panel of experienced academic clinicians in restorative dentistry assessed a series of cases that were borderline restorable and had been successfully treated. From these treated cases, pretreatment clinical photographs and the corresponding radiographs of a carious and fractured molar were selected.
Two vignettes were then created describing a 34-y-old woman presenting at the clinic with symptoms of irreversible pulpitis. The race of the patient was indicated by a photograph of a woman accompanied by 2 clinical photographs and 2 periapical views (in parallax) of the tooth in question (Fig. 1). The vignette was created to allow for variations in the treatment options, whereby recommendations other than root canal treatment, such as extraction, were possible.
Examiners were asked to rate the likelihood that the patient’s symptoms were due to irreversible pulpitis and whether they would advise root canal treatment or extraction for the patient, as well as the strength of their recommendation. Following the clinical decision, further questions on their perception of the patient (stubborn, anxious, intelligent) and whether participants preferred treating Black or White patients, their feelings toward them, and their perceptions on how each group was cooperative were also posed. In all cases, either a 5- or 10-point Likert scale was used. Participants were then questioned on their demographics and work environment and given a set of pre- and posttest questions regarding their opinions on unconscious bias and IATs (online Appendix).
Brief Implicit Association Test
An implicit association test was used to measure implicit biases. Using Inquisit software (Millisecond), 2 Brief Implicit Association Tests (BIATs) were used—a race preference BIAT and a race dental cooperativeness BIAT, the latter having been specifically created for this study. Implicit association tests have been shown to have incremental predictive validity compared to self-report (Greenwald et al. 2009) and can be applied and adapted to measure a various number of topics. The BIAT is a variation and has the advantage of reduced time compared to the IAT to measure associations while maintaining the design of the original IAT (Nosek et al. 2014). As a result, the changes in design simplify instructions and reduce the need for multiple practice blocks (Nosek et al. 2014). The BIAT has been shown to be an effective measure of attitudes, identities, and stereotypes (Meyer et al. 1988).
The race preference BIAT measured participants’ implicit association of race with likeable and unlikeable terms, while the race dental cooperativeness BIAT measured implicit associations between Black and White people and dental recommendations. The race preference BIAT (Fig. 2) compared the average time it takes for participants to categorize images of Black and White people with words reflecting likable and unlikable terms such as wonderful, best, awful, and worst. The dental cooperativeness BIAT used the same categories except, instead of likable terms, we used cooperative and uncooperative statements relating to dental treatment such as “irregular attender” or “easily anaesthetized.”
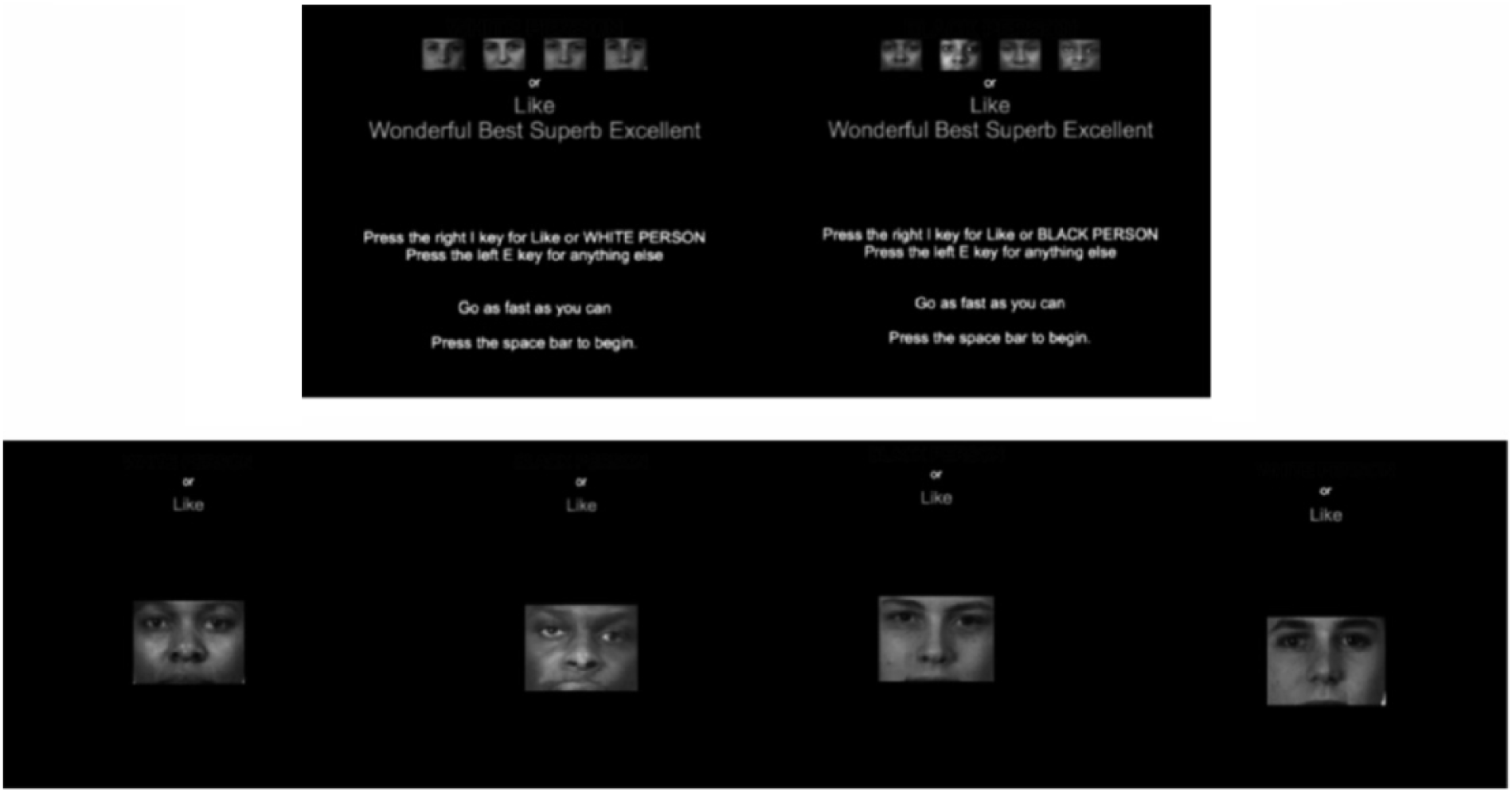
Brief Implicit Association Test (BIAT) sample screens and stimuli. Images of Black or White people and “likeable” and “unlikable” words.
Each BIAT was split into 8 blocks with associations. Four asked the participant to associate “likable” terms with images of White people, and another 4 blocks associated “likable terms” with images of Black people. Each block alternated a total of 4 times. The first 4 were used as practice trials, allowing the participant to acclimatize to the task. The next 4 were used to determine the final result. Stronger associations of likable words and White or Black faces were measured through reaction times.
Participants were asked to first complete the vignette (depicting the clinical scenario) and questionnaire to assess participant demographics. This was followed by the race and dental cooperativeness BIAT and debriefing on the true nature of the research. A posttest questionnaire was then administered to evaluate participants’ views on the research topic.
The BIAT result is a categorical variable and a measure of strength for automatic associations through average reaction times. The diagnosis of irreversible pulpitis and root canal treatment (RCT) decision were classified as the dependent variables and primary outcome. The decision for or against RCT was measured using a dichotomous scale (yes or no), and the diagnosis and strength of their recommendation (RCT or Extraction) were measured using 5-point Likert scales.
Both measures for implicit and explicit bias were recorded as relative preferences for White versus Black people. Chi-square tests were used to compare the decision for or against RCT and demographic characteristics of participants. Independent t tests were used to compare the BIAT scores and strength of recommendation of RCT/extraction. These tests compared the mean average values of responses between each group. Analysis of variance (ANOVA) models were used to evaluate the effects of the race of dentist, recommendations of RCT, and interactions on the BIAT scores. This allowed us to address the following questions: do dentists make different treatment decisions for Black versus White patients, and do dentists express this?
Results
A total of 57 dentists completed the survey, of whom 29 were assigned the White patient condition and 28 assigned the Black patient condition.
Diagnosis of Irreversible Pulpitis and Decision Making
There was a near-equal diagnosis of irreversible pulpitis regardless of whether the patient was Black (71.14%) or White (72.4 %). Recommendation of root canal was stronger in the White patient condition (86.21%) compared to 60.71% in the Black patient condition. Chi-square tests were used to compare the recommendation for RCT (yes/no) between groups and demographic characteristics (Table 1). Recommendation for RCT in the White patient condition was significantly higher than in the Black patient condition (χ2 = 4.77, P < 0.05).
Chi-Square Tests to Compare the Recommendation for Root Canal Treatment (Yes/No) between Groups and Demographic Characteristics.
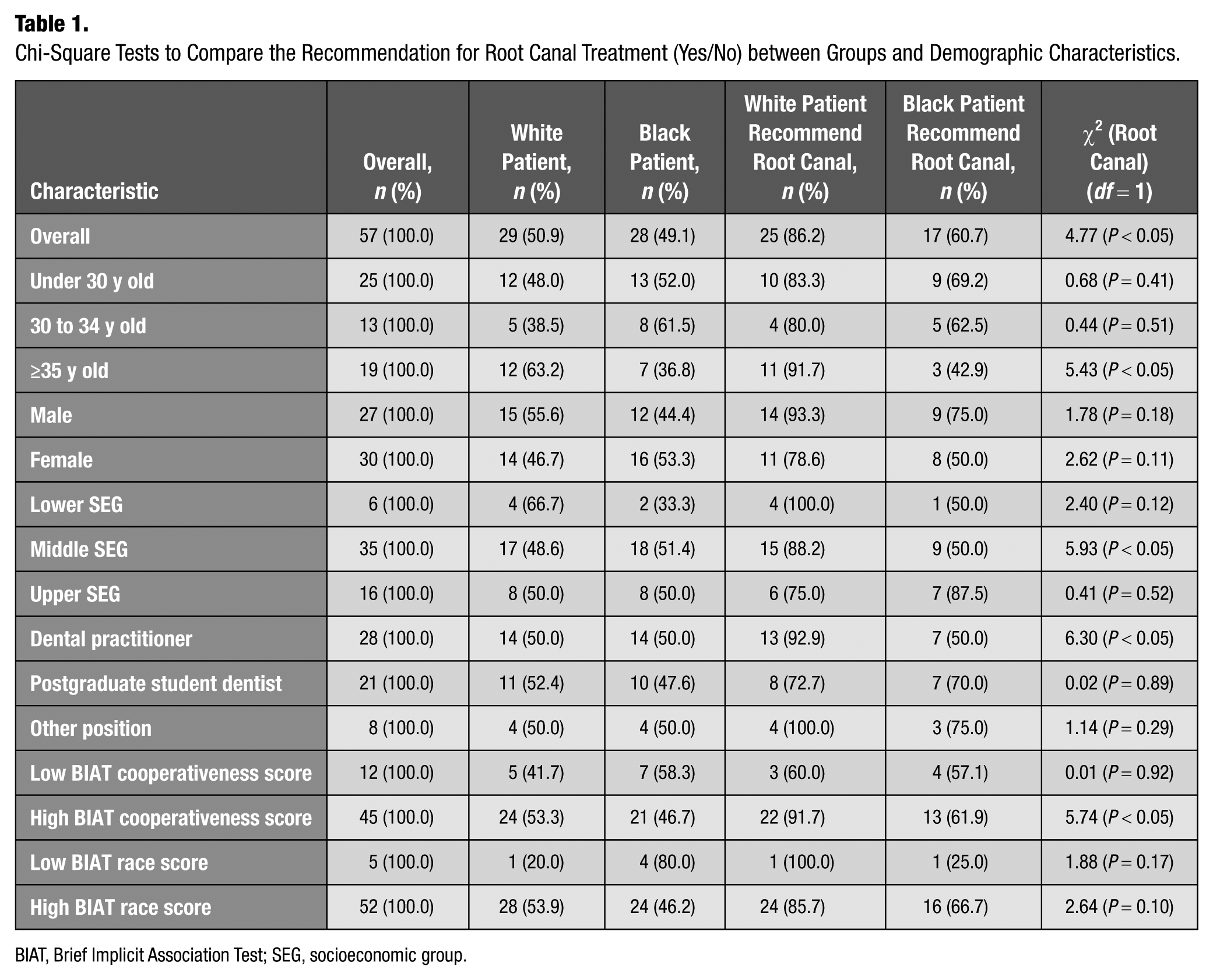
BIAT, Brief Implicit Association Test; SEG, socioeconomic group.
When asked about the strength of prescription of extraction, the distribution of responses indicates a bias toward extraction in the Black patient condition compared to the White patient condition. Notably, in the White patient condition, 89.65% of participants would “definitely” or “probably” not recommend extraction (combined percentages) compared to exactly 50.00% in the Black patient condition (Fig. 3).
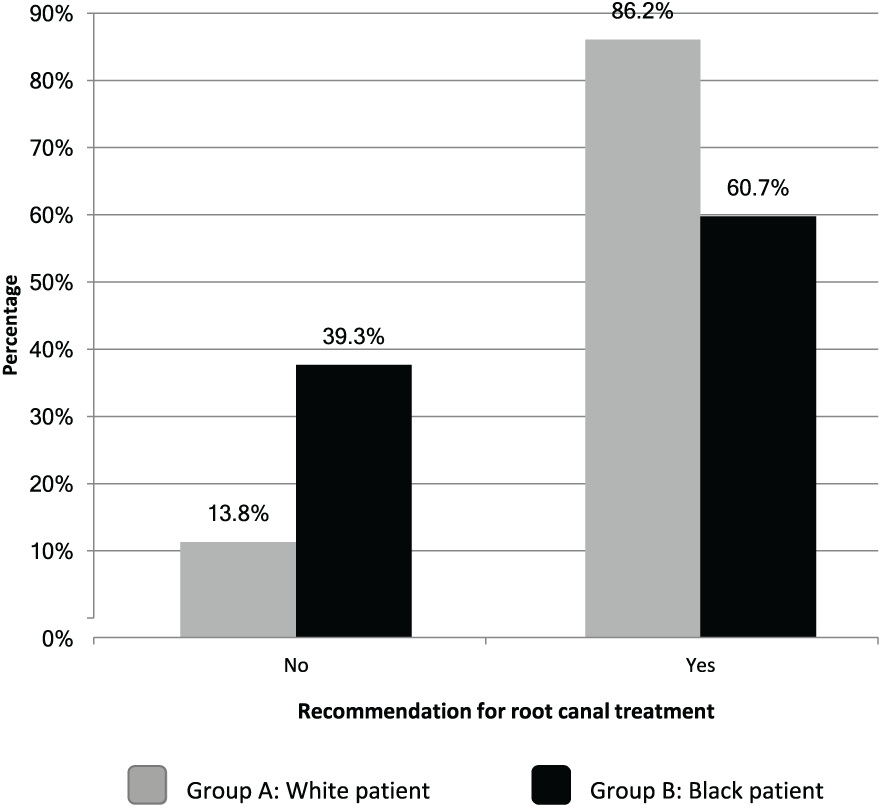
Bar chart showing percentage of participants who recommended root canal treatment in White/Black case scenarios.
Clinicians’ Explicit Racial Biases
One significant difference was found between the experimental conditions in the explicit bias questions. This was in response to whether, if Black patients were treated differently, this was likely due to their behavior. Interestingly, agreement with this statement was stronger in the White patient condition than in the Black patient condition (df = 55, t = 1.98, P = 0.05).
Questionnaire Responses
Participants were more likely to accept the decision of a Black patient than a White patient (Q7) (df = 55, t = 2.56, P = 0.01). Participants were also more likely to say that the patient would be fearful of dental procedures (df = 55, t = 2.37, P = 0.02) and well educated in the White condition (df = 48.8, t = 2.21, P = 0.03). In contrast, participants felt more confident in earning the patients’ trust in the Black condition (df = 44.3, t = 4.25, P < 0.01).
BIAT Race and Cooperation Score
Overall, 91.23% and 78.95% of all participants displayed high BIAT race and cooperation scores, respectively, showing a pro-White bias in both categories. This trend was shown irrespective of the patient condition.
Strength of Recommendation: Root Canal and Extraction
Those with a high IAT cooperation score (Table 2) were significantly more likely to strongly recommend root canal (df = 43, t = 2.66, P = 0.01). The same finding was present for those with a high IAT race score (df = 50, t = 2.06, P = 0.04). Those who did not recommend root canal in the Black patient condition appeared to have a stronger opinion that tooth extraction was the correct course of treatment (df = 13, t = 2.14, P = 0.05). Similarly, those with a high IAT cooperation score were significantly more likely to strongly recommend extraction in the Black patient condition (df = 28.7, t = 3.20, P < 0.01), as were those with a high IAT race score (df = 38.5, t = 2.61, P = 0.01).
Comparisons of Cooperation and Race IAT Scores by Vignette and Demographic Characteristic.
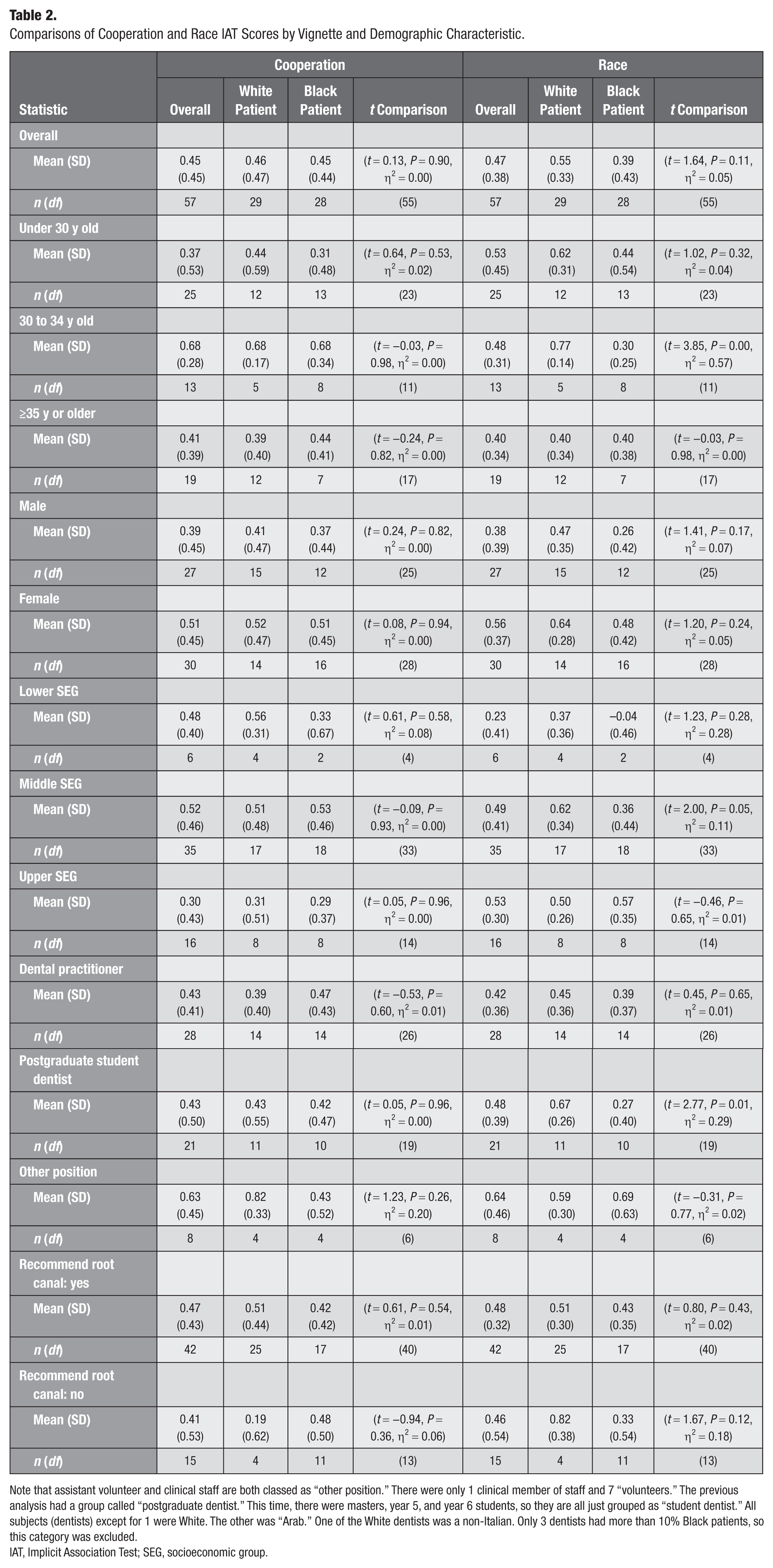
Note that assistant volunteer and clinical staff are both classed as “other position.” There were only 1 clinical member of staff and 7 “volunteers.” The previous analysis had a group called “postgraduate dentist.” This time, there were masters, year 5, and year 6 students, so they are all just grouped as “student dentist.” All subjects (dentists) except for 1 were White. The other was “Arab.” One of the White dentists was a non-Italian. Only 3 dentists had more than 10% Black patients, so this category was excluded.
IAT, Implicit Association Test; SEG, socioeconomic group.
Interaction between IAT and Recommendation of RCT
ANOVA models were created to test whether the race of the patient interacted with the treatment in predicting the IAT score. Only in the race IAT score was a significant difference indicated in scores (f = 5.37, P = 0.0243). It can be deduced that in this result, those who did not recommend root canal had a more pro-White IAT race score in the White patient condition than in the Black patient condition. This result would seem to indicate that not recommending root canal (recommending extraction) might be due to racial bias.
Postsurvey Questions
No significant differences were found between the participants in each group in the postsurvey questions. The item closest to significance was question 4 (If I had known what this study was about in more detail I would not have participated), where those assigned to the White patient condition had a tendency to be less enthusiastic (df = 30.2, t = 1.50, P = 0.14). Notably, though, the mean average responses of both groups were very close to 1 (i.e., close to a mean average of “strongly disagree”).
Discussion
This study showed that clinicians’ decisions to recommend RCT were affected by the race of the patient, and there was a clear bias toward RCT in the White patient model and extraction in the Black patient model. Generally, clinicians had a pro-White bias in both race and cooperation tests irrespective of the patient condition.
To our knowledge, this is the first study to apply sociocognitive measures of bias to determine if unconscious bias influences dentists’ treatment decision making on tooth restorability according to race.
The original design for the study called for a standard IAT. Pilot study results showed that participants were becoming unfocused due to the length of time it took to complete a standard IAT; therefore, the BIAT test was used instead of the standard IAT. We also chose to exclude the general cooperative IAT component from the study. A new BIAT was specially created to measure implicit bias specific to dental care, referred to as the Kings College London dental BIAT. The distinguishing factors between the BIAT and the standard IAT are fewer block trials and a focus on just 2 of the 4 categories in each 4-category test block. Previous research also indicated that the BIAT functions similarly to the standard IAT (Sriram and Greenwald 2009; Nosek at el. 2014).
Results show that for the majority of clinicians, less than 10% of their patients are Black, which is expected, as the number of Black citizens within Italy accounts for a limited percentage of the population (Cittadini Stranieri in Italia 2018). Interestingly, in 2017, a marked increase in migrants arriving in Italy (United Nations High Commissioner for Refugees 2018) was reported, most of whom belong to lower socioeconomic groups and are unemployed.
Participants showed a predominant bias toward White people and were significantly more likely to recommend RCT in the White patient condition and extraction in the Black patient condition. In truth, we are all susceptible to biases, which can be more prominent during stressful periods or when we are multitasking or fatigued (Ma et al. 2013). As a result, we cope by relying on judgments made without careful reasoning, resulting in simpler decisions that may not necessarily have been the best.
The results also revealed those over 35 y old and postgraduate student dentists in the White patient condition were more likely to exhibit a pro-White bias than those who had taken part in the Black patient condition (Appendix Table 12). This may indicate that age and experience may influence bias and treatment planning decisions, although in this study, age was unevenly distributed between experimental conditions (Appendix Table 3). Numerous studies show that there is a relationship between age and prejudice (Pettigrew 2006) and that older adults are less able to control their automatic prejudice (Stewart et al. 2009). The interaction between age upon both bias and overcoming bias in this area requires further investigation.
Interestingly, the posttest questionnaire revealed that generally, participants felt it was a worthwhile experience to explore biases, although participants in the White patient condition were less enthusiastic. Theoretically, those in the White patient condition may have been more comfortable with the experiment as they did not have to “explore” biases as deeply as those in the Black patient condition. Ultimately by creating awareness, bias can be recognized and reduced. Devine et al. (2012) looked at long-term reductions in implicit bias through a multifaceted habit-breaking intervention and found that after 12 wk, there were dramatic reductions.
Ultimately, the recommendations for tooth extraction may be due to assumptions made about race. For example, the subject may have assumed that the Black patient was financially poorer. This would be classified as stereotyping, which is described as an oversimplified, usually negative attitude people hold toward those outside of their own social group. This can lead to inaccuracies in social perception and contribute to prejudiced attitudes. Statistics from the department of work and pensions show that ethnic minorities such as Black British are twice as likely to live in low-income households. Heuristically, this would generally be true but not always true, so this would indicate a prejudice in belief about income levels based on race.
However, the reasoning behind the decision making could be innocent. For example, dentists may be second-guessing whether they want to ask a patient if she or he would want to pay for something that they suspect the patient could not afford. This is still a form of bias, through an attempt to prevent the patient from feeling awkward. Therefore, it would be an empathetic action to prevent hurt feelings in the patient rather than an action based purely on notional bias. It is quite difficult to separate this effect as a source of bias from other kinds of bias.
The reality of working in the health care system, whereby time constraints are placed upon professionals, allows for an environment whereby implicit biases can take effect. In order for this to shift, awareness needs to be created to allow for reflection and change. It might be reasonable to introduce this concept to the dental curriculum, creating early awareness and active prevention. Although it might not be likely to completely eliminate the impact that biases can have upon the decisions we make, a reduction in the occurrence is a worthy result.
Conclusion
Dentists’ decision making was affected by the race of the patient, resulting in a greater likelihood of extractions (less RCTs) for Black patients presenting with a compromised tooth and symptoms of irreversible pulpitis.
Racial bias might influence the quality of care received by Black patients.
Author Contributions
N. Patel, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; F. Mannocci, S. Patel, contributed to conception, design, and data interpretation, critically revised the manuscript; E. Cotti, G. Bardini, contributed to data acquisition, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_2380084418812886 – Supplemental material for Unconscious Racial Bias May Affect Dentists’ Clinical Decisions on Tooth Restorability: A Randomized Clinical Trial
Supplemental material, DS_10.1177_2380084418812886 for Unconscious Racial Bias May Affect Dentists’ Clinical Decisions on Tooth Restorability: A Randomized Clinical Trial by N. Patel, S. Patel, E. Cotti, G. Bardini and F. Mannocci in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors acknowledge I. McLaurain (Statistical Information Solutions) and O. Amoroso for their contributions to and support of this research.
A supplemental appendix to this article is available online.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.