
Abstract
Introduction:
The historical separation between medicine and dentistry has resulted in the creation of separate health records, which have the potential to negatively impact patient care and safety. Of particular importance, errors or omissions in medication lists in separate electronic health records (EHRs) may lead to medical errors and serious adverse outcomes.
Objective:
This study aimed to compare medication lists reported in the EHRs of active patients treated by both the University of Michigan School of Dentistry and Michigan Medicine to determine if differences exist.
Methods:
In this cohort study, EHRs of a population of 159,733 patients that the University of Michigan medical and dental clinics share in common were investigated for agreement in the reporting of 16 medications. After exclusion of minors and patients not seen in the last 5 y, records of 27,277 patients were examined.
Results:
The maximum percentage of agreement in medications reported in both records was 52% for levothyroxine, and the minimum was 7% for sildenafil. The medical record had a significantly higher number of unique medications than the dental record, suggesting higher underreporting in the dental setting.
Conclusion:
The lack of agreement in the report of medications with serious dental and medical implications argues in favor of unification of records and use of available technology to increase accurate medication reporting.
Knowledge Transfer Statement:
The results demonstrate a lack of agreement between medications reported in medical and dental records, which can have serious implications to patients’ health. A unified health record, employing available technology to increase accurate medication reporting, would mitigate this problem.
Keywords
Introduction
Interprofessional healthcare requires sharing of data among providers to facilitate collaboration on treatment decisions and to optimize patient care (Glassman et al., 2016). The historical separation between medical and dental records creates unnatural and unnecessary barriers to achieving this aim (Kalenderian et al. 2016; Jain 2018). For example, high blood pressure readings in the dental office may trigger the cancellation of dental procedures and unnecessary medical consultation requests that could be avoided if dentists had access to medical records showing the patient’s hypertension is being managed (Yarows et al. 2020). Physicians also consider dental information to be relevant for their practice (Acharya et al. 2017; Simon et al. 2019), but they do not have ready access to dental records that document their patient’s dental treatment, oral health, and drug prescriptions. The importance of communication between dentists and physicians became clear during the opioid crisis, since dentists are major prescribers of opioids (e.g., after tooth extraction surgeries) (Nalliah et al. 2020).
Avoiding mistakes in patient-reported information during appointments, especially regarding medications, is imperative when sharing data across health professions and records. A high prevalence of errors in medication reporting, especially omissions, has been described in both the medical and dental settings (De Winter et al. 2011; Choi et al. 2017). It is likely that having separate medical and dental records contributes to inaccuracies in medication reporting, as has already been shown for the reporting of underlying health conditions such as diabetes or hypertension (Adibi et al. 2020). This is expected to become an increasing problem, as populations worldwide are living longer with chronic illness, which requires chronic use of medications.
By identifying a cohort of 159,733 patients that the University of Michigan School of Dentistry and Michigan Medicine shared in common, we had a unique opportunity to investigate the agreement in medications reported in the medical and dental electronic records in a large sample of individuals. Here we report the discrepancies found and discuss the technologies available to mitigate this problem.
Methods
Study Design
The study, approved by the University of Michigan IRBMed (HUM00169814), investigated 16 active medications in separate electronic health records (EHRs) (MiChart, for Michigan Medicine; and MiDent, for the School of Dentistry) from 159,733 shared patients. An honest broker (School of Dentistry programmer external to the study team) extracted deidentified information from both EHRs (Fig. 1). Then, Python scripts were used to compare matching of medications lists between the health records. Quality assessment of the data extraction was obtained from a subset of 500 records using 2 medications (warfarin group, sildenafil group); data tables obtained from both records were observed to confirm the agreement (or lack of) observed by the data extraction and analysis scripts.
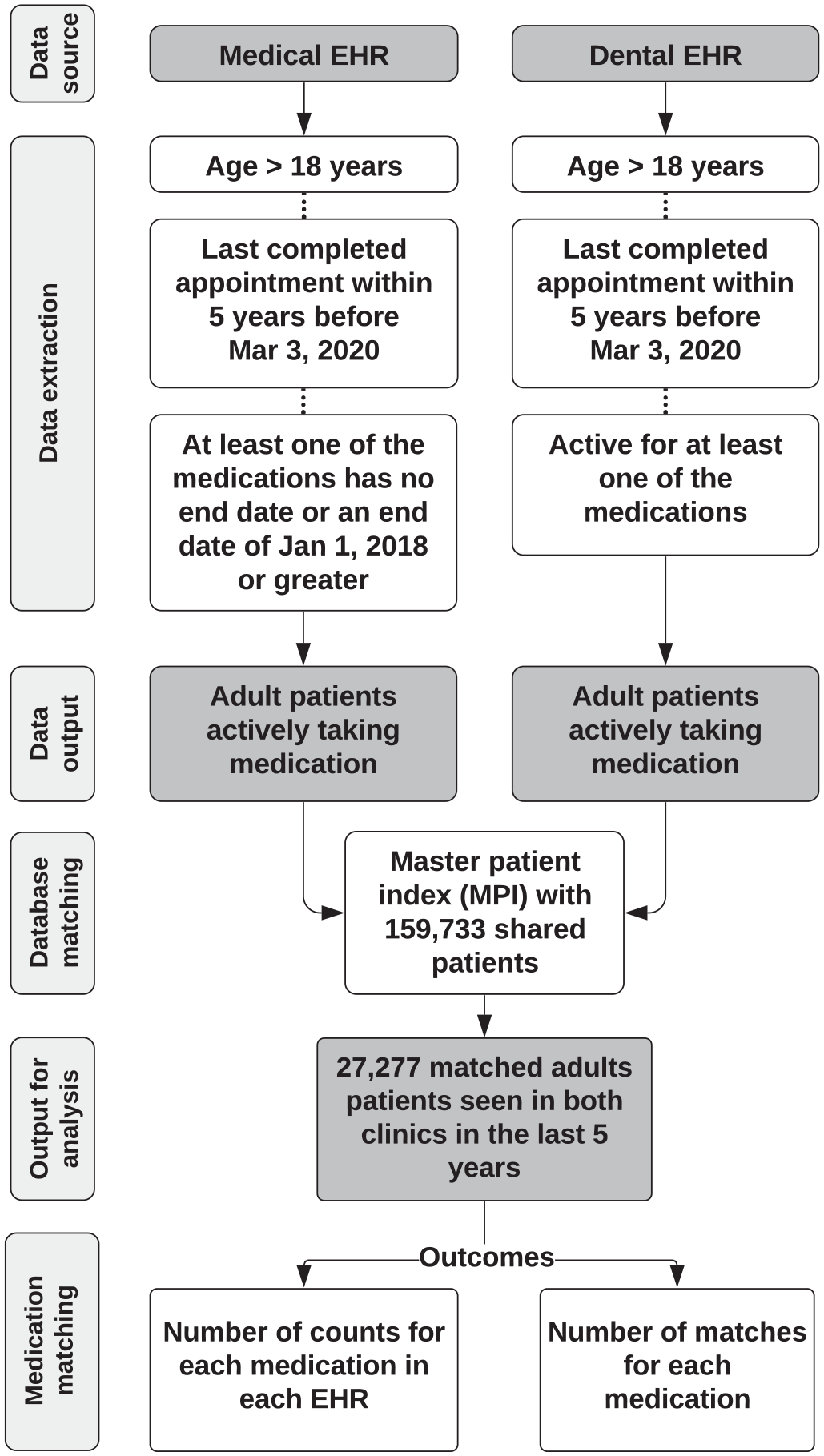
Study flowchart. MPI is the Master patient index, a unifying list of the patients that Michigan Medicine and the School of Dentistry share. EHR, electronic health record.
Medication Identification
Generic drugs were chosen from the 2019 ClinCalc DrugStat Database (available at: https://clincalc.com/DrugStats/Top200Drugs.aspx). The thirteen most prescribed medications in the list were included. Insulin and warfarin, not among these, and sildenafil, not listed, were included due to their possible serious complications, including hypoglycemia, bleeding and hypotension, respectively. Both generic and brand name drugs were included in the analysis. Medications with different commercial names but with the same active ingredient were grouped (Appendix Table 1).
Prescribed medications are entered into both health records using structured lists. While additional drug information can be entered into open text fields, matching on open text fields requires natural language processing. Due to the complexity of using natural language processing, only the structured information was investigated in this study.
Data Extraction and Analysis
Figure 1 depicts the data extraction and analysis process. Data from the University of Michigan School of Dentistry EHR, MiDent (axiUm, Vancouver, Canada), was retrieved via structured query language (SQL) from the medication section of the Health History form. A similar set of MiChart (Epic Systems, WI, United States) data was also obtained from the Michigan Medicine Health System Data Warehouse (HSDW) Patient Summary List. SQL scripts included only patients 18 y or older, and patients whose last appointment in each of the clinics was within the last 5 y (as of March 3, 2020). The scripts were customized to the characteristics of each of the databases; for example, in the dental EHR, medications listed as “active” were retrieved from the Health History form; in the medical EHR, medications with either no end date or an end date of January 01, 2018 or greater were retrieved. The honest broker collected these data and compared each set of patients against a Master Patient Index (MPI) (containing 159,733 records) that consolidated unique patients in both records. The honest broker then de-identified this combined result set, assigning each patient a unique 24-character identifier.
Data was then analyzed using a Python script to produce frequency counts for each medication in each EHR, including also the counts of medications reported in both systems. As an addendum to raw Python data, the open-source pandas library was employed to provide a binary comparison between the 2 health records. A simple script counted the presence of each medication in each health record as well as the agreement in health records.
Results
After exclusion of minors and patients without at least 1 visit in the last 5 y in either of the clinics, 27,277 patient records were available.
The number of individuals taking each medication according to the EHR (Fig. 2) shows that the most frequent of the medications investigated was omeprazole, and the least frequent was sildenafil. Matching between both EHRs varied from 7% (sildenafil) to 52% (levothyroxine) (Fig. 3). Most of the unmatched medications were observed in the medical EHR, although for all drugs there was a small percentage (ranging from 2.0% to 19.1%) of medications reported only in the dental EHR.
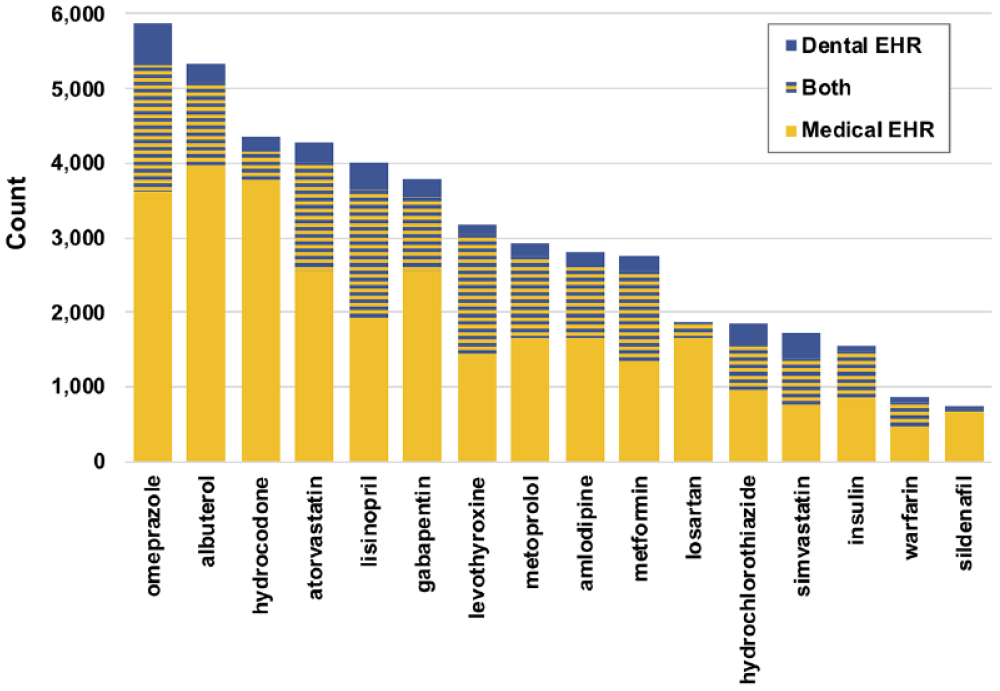
Number of EHRs presenting each of the medications investigated, according to the source system (Medical EHR, Dental EHR, or both), ordered by frequency of total report (from 27,277 records of shared patients). EHR, electronic health record.
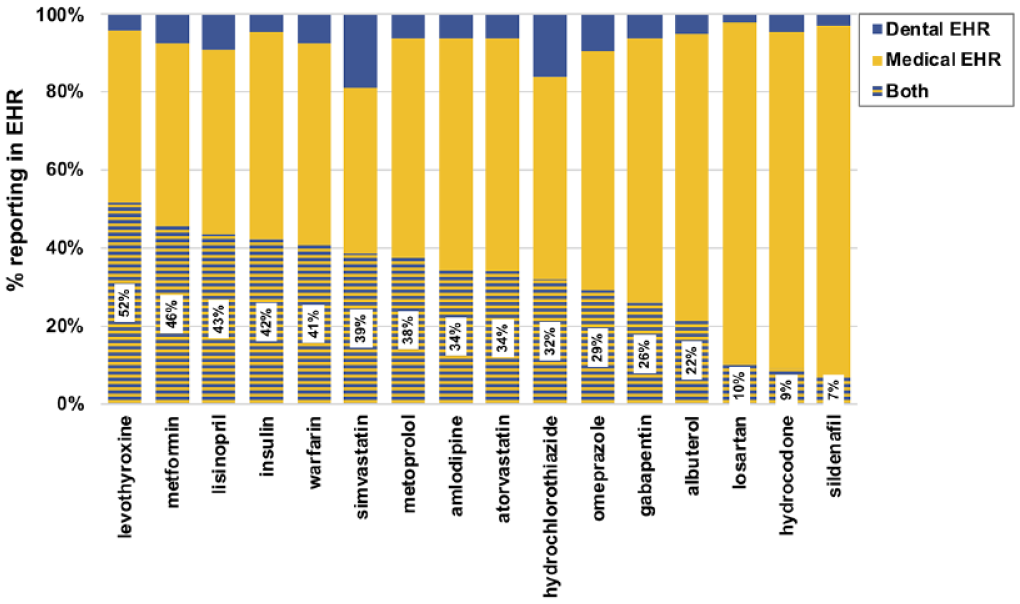
Percentage of reporting of each medication investigated, ordered by percentage of matching in both EHRs (from 27,277 records of shared patients). EHR, electronic health record.
Discussion
The current study once again shows the difficulties in obtaining precise medication reporting in health records (Choi et al. 2017). The dental EHR was the most impacted by medication omissions that could significantly impact the wellbeing of the patient under treatment. For example, the dental EHR missed more than 90% prescriptions of sildenafil; dangerous hypotension could be produced in the dental office if the dentist is unaware of the prescription and uses nitroglycerin to control chest pain in the dental chair. Patients may have been embarrassed to report using sildenafil, which is prescribed for treatment of erectile dysfunction. It is possible that other drugs that are used to treat conditions that patients might find embarrassing, or not related to dental treatment, are also underreported. Future studies might investigate disparities in reporting of a more comprehensive list of medications.
The few studies investigating the accuracy of medical information available in dental records show results similar to the ones reported here (Choi et al. 2017; Patel et al. 2018). The main advantage of this study is the large sample size investigated, suggesting that the discrepancies observed by others in smaller scale studies are not isolated findings. The fact that this study only included data from 1 institution may be seen as a limitation. However, one may argue that this would make the sample more homogeneous, especially if we consider that providers from the same region would follow similar practices. Another limitation is that the dental record relies on patient self-report, and individuals with more complex medical history are less likely to report their medications accurately (Allin et al. 2013). However, discrepancies between the medical and the dental record are not limited to medications, as it was previously shown that up to 29% of patients misreport their hypertension to their dental clinicians (Adibi et al. 2020).
In this study we only retrieved information from structured text fields from both EHRs. Out of scope were the various phrases in the “other” free-text entry fields such as treatment notes, whose interpretation required natural language processing and other machine learning techniques (Wang et al. 2017). The extent to which this may have led to the poor matching is unknown. Our choice to include only active patients (seen in both clinics in the last 5 y) and restrict the search to medications that have been reported in the records recently or currently aimed to reduce disparities caused simply by outdated records. We chose not to narrow the search to include only dental visits that occurred after a medical visit, which may have increased the number of prescription reporting irregularities in the dental record.
Nevertheless, the choice for the experimental approach used here derives from our particular interest to improve our respective EHR systems and their interoperability that in turn would improve the EHR data. For example, an electronic prescribing system, especially one that calls upon a national platform such as Surescripts, could improve the documentation of medications prescribed (Rowan et al. 2017). While on the School of Dentistry EHR roadmap, electronic prescribing did not exist at the time of this study. Another approach could be the use by both entities of a drug vocabulary supported by RxNorm (Hoopes et al. 2018). A further improvement would be the implementation of data exchange standards to facilitate the rapid and consistent transfer of clinical information electronically, such as HL7 FHIR (Health Level 7 Fast Healthcare Interoperability Resources) Release 4, which has seen significant adoption in recent years (Evans 2016). Specifically, the FHIR resource “MedicationRequest” contains information regarding the dispensation and administration of drugs. Pervasive incorporation of such interoperable data standards could further ease the patient burden of medication self-reporting in multiple EHRs. Without both systems using standards and best practices, true interoperability is not possible (Evans 2016). This in turn, compromises patient care.
While we concur with others (Simon et al. 2019) who have advocated for improved quality of dental records and data sharing standards, we also advocate for a unified record. Medication information shared across medical and dental records will offer the opportunity to improve access to accurate medication data, as well as increase the quality of these data. This in turn will improve the care provided to patients (St Sauver et al. 2017). Ultimately, a future goal would be a single unified health record (Kalenderian et al. 2016; Adibi et al. 2020).
Author Contributions
L.M.A. Tenuta, contributed to conception, design, data analysis, and interpretation, drafted the manuscript; C. Canady, contributed to design, data acquisition, analysis, and interpretation, critically revised the manuscript; R.M. Eber, L. Johnson, contributed to conception, design, data analysis, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-pdf-1-jct-10.1177_23800844211004525 – Supplemental material for Agreement in Medications Reported in Medical and Dental Electronic Health Records
Supplemental material, sj-pdf-1-jct-10.1177_23800844211004525 for Agreement in Medications Reported in Medical and Dental Electronic Health Records by L.M.A. Tenuta, C. Canady, R.M. Eber and L. Johnson in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The authors thank Max Kolasinski (Office of Dental Informatics, School of Dentistry, University of Michigan) for the help with data extraction. The authors also thank Thankam Thyvalikakath, from the Indiana University School of Dentistry, and Romesh Nalliah, from the University of Michigan School of Dentistry for the helpful discussions and suggestions.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.