
Abstract
Background:
The objective of this retrospective cohort study is to examine the determinants of tooth loss in a Medicaid-enrolled population using claims data from 2016 to 2018.
Methods:
Deidentified administrative claims data for Medicaid-enrolled adults between the ages of 50 and 90 y in 2016 to 2018 were examined using the IBM Watson MarketScan Medicaid Database. The sample size was 91,468. The entire sample was divided into 2 cohorts: no tooth loss cohort (n = 54,786) and tooth loss cohort (n = 36,682). The tooth loss cohort was further divided into 2 groups: 1 to 5 teeth lost (n = 29,141) and 6 or more teeth lost (n = 7,541). Tooth loss was described by age, gender, race, number of commodities, and if periodontal treatment was performed. Logistic regression models were conducted to examine factors associated with tooth loss.
Results:
Within the tooth loss cohort, the patients who had periodontal treatment had higher odds of losing at least 1 tooth (odds ratio [OR], 1.15; confidence interval [CI], 1.10–1.20) and lower odds of losing 6 or more teeth (OR, 0.25; CI, 0.22–0.29). In the regression analysis, the predictive margins of tooth loss for 1 tooth and 6 or more teeth follow a linear path. Compared to no comorbidities, the odds of losing 6 or more teeth increased with 1, 2, or 3+ comorbidities.
Knowledge Transfer Statement:
This study provides significant information about the quantification of comorbidities and its direct correlation with the increased odds of tooth loss. This study also highlighted the protective effect of periodontal treatment on tooth loss. This knowledge can be useful to dental care providers to understand the risk of tooth loss in their patient population.
Keywords
Introduction
Tooth loss is an indicator of poor oral health. Tooth loss or “tooth mortality” is the direct result of oral disease accumulation over the years (Copeland et al. 2004). In older adults, tooth loss can affect their ability to chew and thus influence nutritional intake, further affecting general health and chronic disease management (Makhija et al. 2006; Wu, Liang, et al. 2011). Tooth loss reduces oral health quality of life due to the related pain, inability to eat, and social repercussions (Gerritsen et al. 2010; Cerutti-Kopplin et al. 2016). Oral health problems and tooth loss can affect work presenteeism, meaning that worker performance can be reduced at work (Lima and Buarque 2019).
Tooth loss is associated with several clinical and social factors, including oral and systemic diseases connections, the availability and accessibility of dental services, health care beliefs related to dental care, health insurance and coverage for specific dental procedures, and social factors, such as trust in the dentist, dentists’ attitudes, and cultural differences (Fejerskov et al. 2013; Tan et al. 2016; Dye et al. 2019). Several social determinants of health—such as education, income, and race/ethnicity—are strong predictors of tooth loss (Gilbert et al. 2003; Dye et al. 2019). Less education has been associated with loss of functional dentition and loss of oral health–related quality of life. In addition, income and race/ethnicity are significant determinants of perceived oral health status and tooth retention in adults and older adults (Huang and Park 2015). Hispanic adults have an increased risk of poor self-rated oral health and less retention of teeth compared with White older adults (Wu, Plassman, et al. 2011). African American older adults, especially those belonging to lower socioeconomic status, experience more tooth loss (Gilbert et al. 2003).
Oral diseases, such as dental caries and periodontal disease, are predictors of tooth loss at a population level (Dye et al. 2007; Eke et al. 2012). Several systemic diseases—including cardiovascular diseases, depression, diabetes, dementia, and other cognitive dysfunction—are implicated in dental disease development and tooth loss (Taylor et al. 2004; Okoro et al. 2012). Interaction of periodontal disease with systemic diseases, including diabetes, hypertension, and cardiovascular diseases, may intensify the disease progression, response to dental treatment outcomes, and tooth loss (Borgnakke et al. 2017). Periodontal disease and diabetes have a bidirectional relationship (Löe 1993; Taylor and Borgnakke 2008), and periodontal disease and tooth loss have also been found to be associated with hypertension and stroke (Peres et al. 2012).
Systemic diseases such as high blood pressure, diabetes, dementia, and other cognitive disorders have been associated with poor oral health and tooth loss (Löe 1993; Taylor and Borgnakke 2008; Peres et al. 2012). Several oral health–related conditions associated with systemic diseases or side effects of their medications, such as stomatitis and reduced salivary flow, can lead to increased oral disease and tooth loss (Cerutti-Kopplin et al. 2016).
In this retrospective cohort study, we examined the determinants of tooth loss in the Medicaid-enrolled population using a Big Data approach (IBM Watson MarketScan Medicaid Database from 2016–2018). Claims data were used to determine the outcome and independent variables for this study. We included determinants that are available in this claims database—systemic diseases (comorbidities), dental-clinical (periodontal treatment), and demographics (age, and race) that are associated with tooth loss in adults. We hypothesized that the number of comorbidities that a patient experiences can directly and independently affect the number of teeth lost. Also, patients who have received periodontal treatment would have less tooth loss than patients who have received none. We also hypothesized that age and race play a critical part in tooth loss.
Material and Methods
This study received clearance from the Western Institutional Review Board and was considered an exempt study. The data used for this study were deidentified administrative claims, so no informed consent was required. The administrative claims included data for Medicaid-enrolled adults between the ages of 50 and 90 y in 2016/2017 and were examined using the IBM Watson MarketScan Medicaid Database. This data set contains medical, surgical, and prescription drug experiences for more than 44 million Medicaid enrollees (deidentified) from 13 states. Tooth extraction and periodontal treatment were identified by Codes on Dental Procedures and Nomenclature (CDT) codes D7140, D7210, D7220, D7230, D7240, D7241, D4341–D4355, D4110–D4340, and D4381–D4999, respectively. Individual comorbidities were identified to create the Elixhauser comorbidity index based on International Classification of Diseases, 10th Revision, Clinical Modification (ICD-9-CM) diagnosis codes.
Cohorts
The overall claims sample size was 91,468. The no tooth loss cohort included 54,786. The tooth loss cohort included adults who had at least 1 tooth lost during 2016 to 2018 (n = 36,682) was created and used for all the analysis. The tooth loss cohort was further divided into 2 groups: 1 to 5 teeth lost (n = 29,141) and 6 or more teeth lost (n = 7,541).
Variables
The data variables evaluated include age as a continuous variable, gender (male/female), race (White, African American, Hispanic, and Other), periodontal treatment (no vs. yes), and Elixhauser comorbidity score (0, 1, 2, and 3 or more) (Elixhauser et al. 1998).
Data Analysis
Descriptive analysis was conducted for the no tooth loss cohort comparing no tooth loss to at least 1 tooth loss. Within the tooth loss cohort, the comparison was between 1 and 5 teeth lost to 6 or more for the included population, which is used by several studies that based the outcomes on number of teeth extracted (Bernabé and Marcenes 2011; Tiwari et al. 2016). For descriptive analysis, tooth loss was described by deciles of age, by gender and race, by the number of commodities, and if periodontal treatment was performed. Logistic regression models with an interaction term of race by age were conducted to examine factors associated with tooth loss for both the no tooth loss cohort and the tooth loss cohort. Results from the multivariable logistic models were reported for the study. Also, logistic regression models adjusting for periodontal treatment were analyzed for the association between individual comorbidities and tooth loss for the tooth loss cohort. All analyses were performed using Stata 16.0, and we deemed a P < 0.05 to be statistically significant (StataCorp).
Results
The cohort with tooth loss included 40.1% of the entire sample (n = 91,468). Within this cohort, 79.4% (29,141) of individuals had 1 to 5 teeth lost. When stratified by race, 76.3% of Whites, 84.9% of African Americans, 91.3% of Hispanics, and 74.9% of Others reported between 1 and 5 teeth lost.
When stratified by age, 20.3% of patients aged 50 to 64 years, 23.6% of patients aged 65 to 74 years, 23.8% of patients aged 75 to 90 years had 6 or more teeth lost (Table 1).
Percentage of Patients with and without Tooth Loss in 2016 through 2018 among Adult Medicaid-Enrolled Dental Patients.
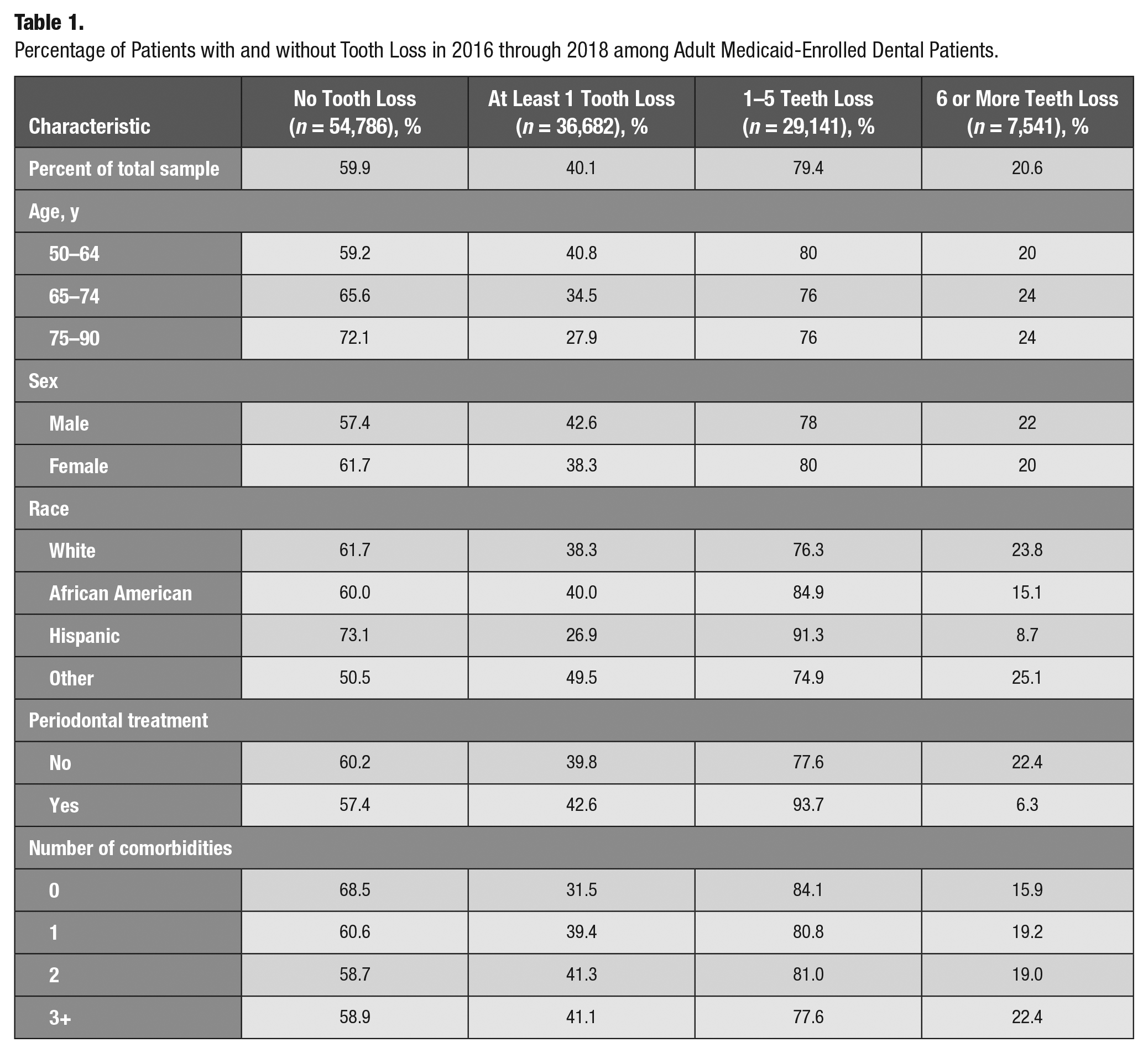
Within the tooth loss cohort, among the patients who had any periodontal treatment between 2016 and 2018, 42.6% had at least 1 tooth loss, and 6.3% of patients had 6 or more teeth lost (Table 1).
In the tooth loss cohort, it was seen that among patients who reported no comorbidities, 31.5% had at least 1 tooth loss. Also, 39.4% of the patients with 1 comorbidity, 41.3% of patients with 2 comorbidities, and 41.1% of patients with 3+ comorbidities had at least 1 tooth loss. For the group with 6 or more teeth lost in the tooth loss cohort, 15.9% of patients with no comorbidities, 19.2% of patients with 1 comorbidity, 19.0% of patients with 2 comorbidities, and 22.4% with 3+ comorbidities had 6 or more teeth lost (Table 1).
Within the no tooth loss cohort, 38.3% of Whites, 40.0% of African Americans, 26.9% of Hispanics, and 49.5% of Others had at least 1 tooth loss, and 76.3% of Whites, 84.9% of African Americans, 91.3% of Hispanics, and 74.9% of Others reported between 1 and 5 teeth lost. When stratified by age, 59.2% of individuals between the ages of 50 and 64 y had no tooth loss.
Table 2 provides the results of the logistic regression for the no tooth loss cohort (no tooth loss compared to at least 1 tooth loss). Patients who received periodontal treatment had increased odds of losing at least 1 tooth compared to patients who did not receive periodontal treatment (odds ratio [OR], 1.15; confidence interval [CI], 1.10–1.20). The odds of losing at least 1 tooth significantly increased with the number of comorbidities (1 comorbidity: OR, 1.48; CI, 1.39–1.57; 2 comorbidities: OR, 1.63; CI, 1.53–1.74; 3+ comorbidities: OR, 1.65; CI, 1.55–1.75).
Logistic Regression Model with Race-by-Age Interaction Term to Examine Factors Associated with at Least 1 Tooth Loss.
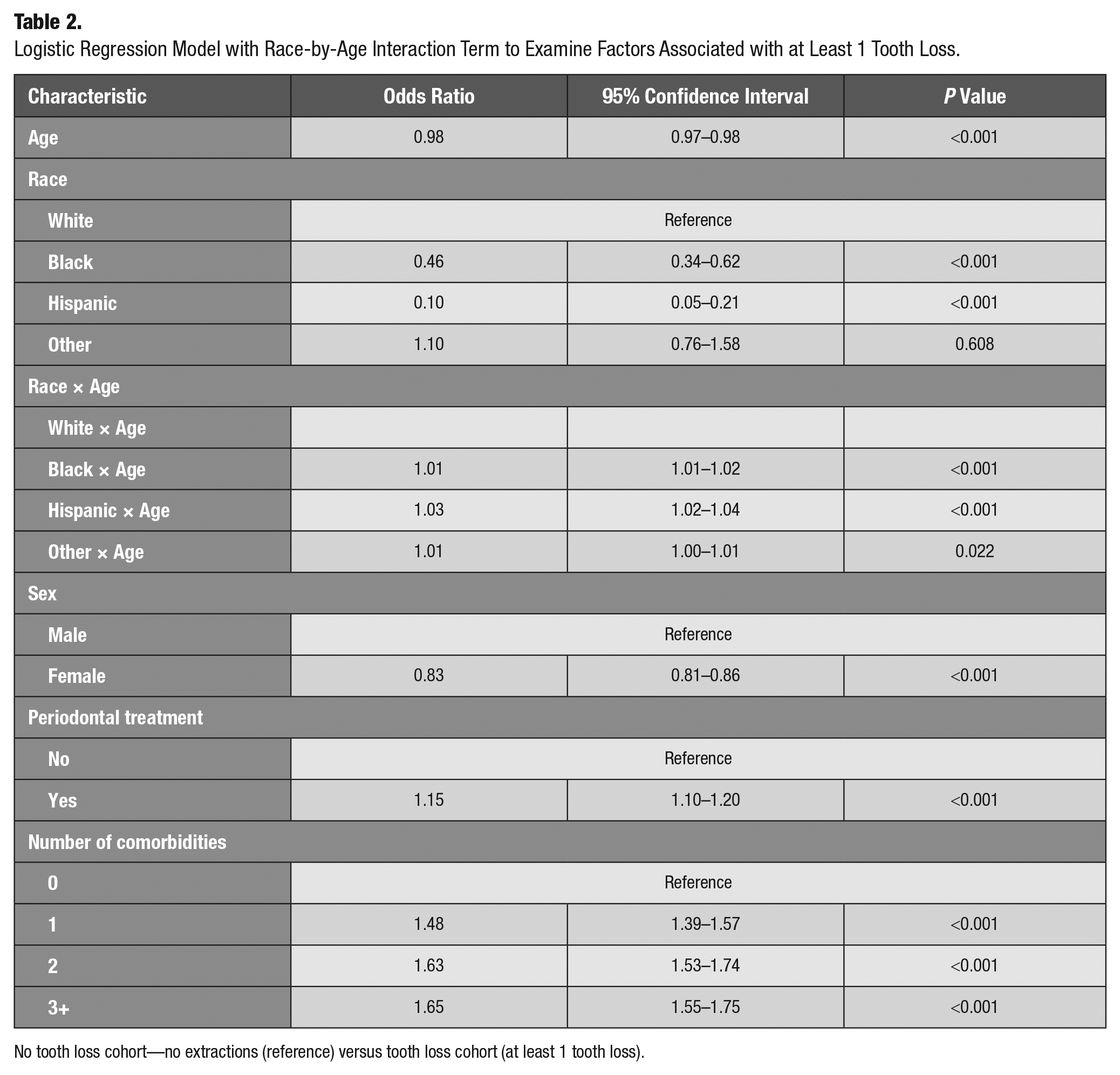
No tooth loss cohort—no extractions (reference) versus tooth loss cohort (at least 1 tooth loss).
Table 3 provides the results of the logistic regression for at least 1 tooth loss cohort. Compared to patients receiving no periodontal treatment, patients who receive periodontal treatment are at lower odds of losing 6 or more teeth (OR, 0.25; CI, 0.22–0.29). Compared to patients with no comorbidities, patients with greater numbers of comorbidities are at significantly greater risk of losing 6 or more teeth (1 comorbidity: OR, 1.26; CI, 1.10–1.45; 2 comorbidities: OR, 1.24; CI, 1.08–1.43; 3+ comorbidities: OR, 1.52; CI, 1.33–1.74).
Logistic Regression Model with Race-by-Age Interaction Term to Examine Factors Associated with 6 or More Teeth Loss.
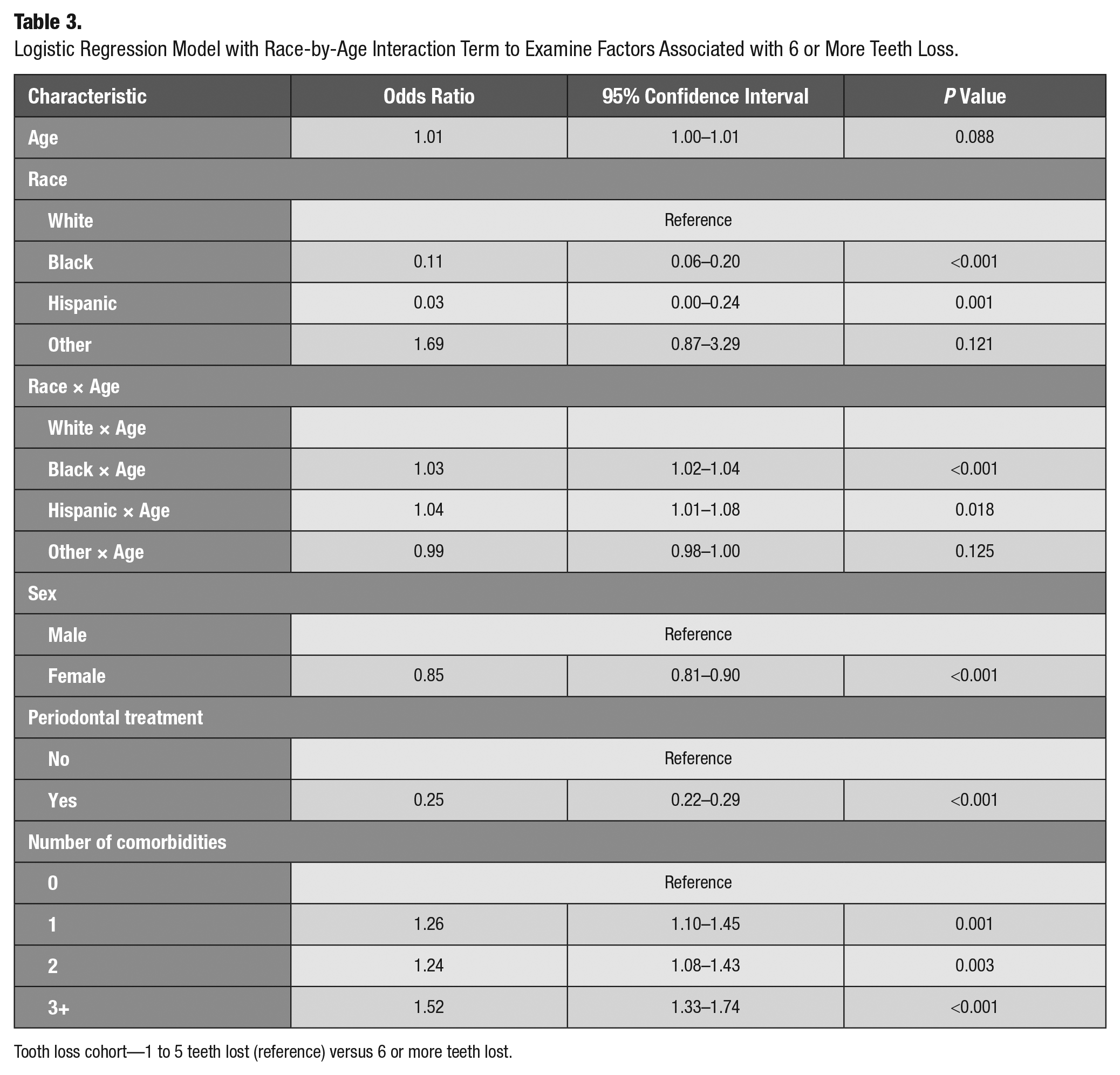
Tooth loss cohort—1 to 5 teeth lost (reference) versus 6 or more teeth lost.
The Figure shows adjusted predictive margins of 6 or more teeth loss by race and age. Risk for tooth loss increased for the White, African American, and Hispanic race categories. The Other race category did not show this same increase (White = 0.22–0.27, African American = 0.12–0.35, Hispanic = 0.06–0.30, and Other = 0.24–0.22).
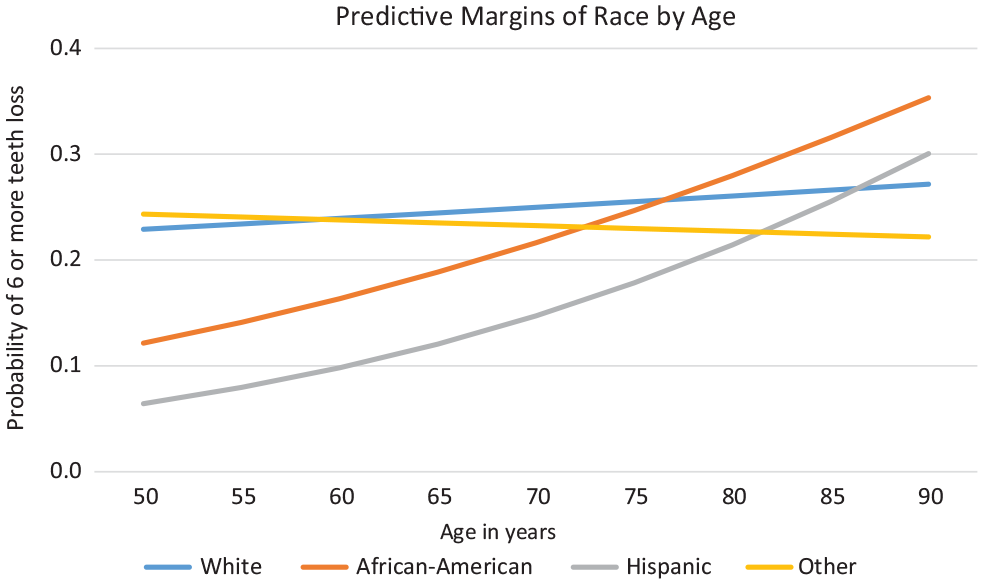
Race and age interactions predicting 6 or more teeth loss.
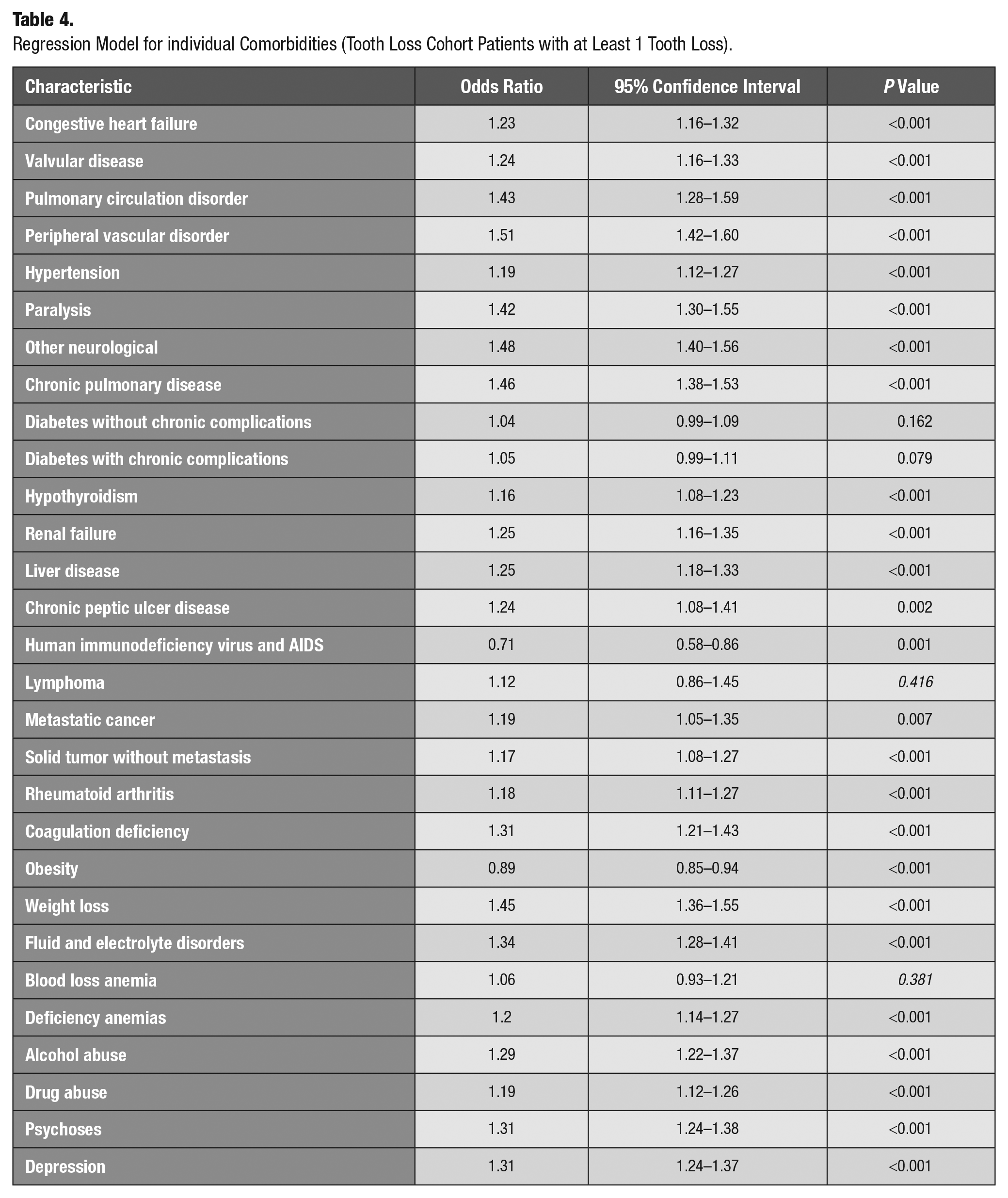
Table 4 presents the results of a multivariable logistic regression model between comorbidities and tooth loss, adjusting for periodontal treatment for the tooth loss cohort with 6 or more teeth lost. People with all the comorbidities except lymphoma, blood loss anemia, and diabetes had significantly higher odds of losing 6 or more teeth. However, people who were diagnosed with human immunodeficiency virus and AIDS and were obese had lower odds of losing 6 teeth or more as compared to those who were not.
Regression Model for individual Comorbidities (Tooth Loss Cohort Patients with at Least 1 Tooth Loss).
Discussion
To our knowledge, this is the first study that has used a large multistate data set to determine the factors associated with tooth loss in a Medicaid-enrolled adult population. This is also the first study to evaluate the relationship between systemic diseases and tooth loss based on diagnostic codes rather than self-reported outcomes. Moreover, this study is the first that compared tooth loss in patients who were not diagnosed with any systemic disease to patients who were diagnosed with 1 or more systemic diseases. Last, this study demonstrated the protective effect of periodontal treatment on tooth loss.
Within the tooth loss cohort, patients between the ages of 50 and 64 y experienced the highest percentage of 1 tooth lost. Patients 65 y and older reported the highest percentage of 6 or more teeth lost. Tooth loss is a cumulative result of dental caries and periodontal disease, and with increasing age, more tooth loss is generally seen as the impact of oral diseases accumulates (Cerutti-Kopplin et al. 2016). The results align with findings from a recent report from the Centers for Disease Control and Prevention that found the mean number of teeth lost was seen in ages 50 to 64 y (Lin et al. 2019). Few states offer adult dental benefits within Medicaid. In 2019, only 18 states offered extensive dental treatment under Medicaid. Most other states provide only an emergency dental treatment option, which includes tooth extraction or no dental benefit (Halasa-Rappel et al. 2019).
This study also evaluated the relationship of race and age together with tooth loss. The interaction increases our understanding that the impact of race and age on tooth loss is not independent of one another and offers an opportunity to explore the tooth loss from a life course approach. In Whites, the probability of more than 6 teeth lost was higher at 50 y compared to African Americans and Hispanics and remained stable as age increased (Figure). It can be speculated that the White population has higher dental care utilization, and as Medicaid may not pay for restorative services, they experience tooth loss earlier (Mueller and Monheit 1988; White 2012). An interaction of age and race predicted that with increasing age, both African American and Hispanic patients had higher odds of 6 or more teeth lost. African Americans and Hispanics historically have poor health outcomes as compared to Whites (Williams and Mohammed 2009). When applying a life course perspective, the disadvantages in health and social disparities experienced by racial and ethnic minorities can have a higher cumulative impact on health and oral health outcomes with age (Gee et al. 2012; Carter et al. 2017). Also, following a life course approach, neglected health behaviors and poor self-rated perception of oral health have a higher impact on dental care utilization, as well as the progression of dental caries and periodontal disease, ultimately leading to higher tooth loss in racial/ethnic minorities (Patrick et al. 2006; Gerritsen et al. 2010; Wu, Plassman, et al. 2011). Recent studies have shown that racial minorities can also experience implicit and explicit bias, which can influence clinicians’ behavior, decision making, and communication process and ultimately can influence treatment planning (Sabbah et al. 2019). All these factors can increase the odds of higher tooth loss for aging African Americans and Hispanics.
One of the promising results from a population oral health perspective was the protective effect of periodontal treatment on tooth loss. Our analyses demonstrated differing outcomes for periodontal treatment—the odds of losing 1 tooth significantly increased with periodontal treatment (Table 2)—as compared to the protective effect of periodontal therapy on reducing the odds of losing 6 or more teeth (Table 3). Previous literature reports that periodontally hopeless teeth that have severe attachment loss could be extracted during periodontal therapy and as a part of supportive periodontal therapy (Machtei et al. 1989; Nibali et al. 2017). This may be one reason that explains the increase in single tooth loss due to periodontal treatment in the tooth loss cohort. Previous research also provides evidence that periodontal therapy and maintenance can reduce multiple tooth loss at the patient level (Chambrone et al. 2010), providing a rationale for the protective effect of periodontal treatment for reduced loss of 6 or more teeth. Thus, initial periodontal management identifies compromised teeth that are removed to optimize a patient’s oral health, but ongoing treatment prevents further demise, thus lowering the rates of multiple extractions (Hirschfeld and Wasserman 1978).
Last, the systemic–oral health impact, especially the quantification of comorbidities diagnosed in a patient and its direct correlation with the increased odds of tooth loss, is the most substantial evidence that this study provides. For both 1 tooth lost and more than 6 teeth lost, it was seen that when compared to no comorbidity or zero comorbidities, having 1, 2, or 3+ comorbidities steadily increased the odds of tooth loss. Data also demonstrated that patients with multiple systemic diseases were associated with 6 or more teeth lost, although no association of increased tooth loss was seen for diabetes. An association with diabetes was seen when the analysis was expanded to include adults aged 30 to 90 y. However, when the analysis was limited to 50 to 90 y, this association was lost. Further research is warranted to better understand the loss of the association between diabetes and tooth loss in older adults.
This evidence of the systemic–oral health impact on tooth loss supports the ongoing promotion of medical-dental integration and interprofessional health care practice to improve all overall health. Interprofessional collaboration is critical to helping patients with chronic diseases maintain their natural detention by establishing referral patterns, health promotion, and education and timely management on risk (Parker et al. 2020).
Like all research, there are a few limitations of this study. It is important to understand that using Big Data, especially claims data, has some limitations as these data were not collected for research perspectives, and thus the authors have to work with the data available in the data set. In addition, the study provides a snapshot of people enrolled in Medicaid in 2016 to 2018. Therefore, it is difficult to understand how patient factors such as continued periodontal home maintenance, regular follow-up visits, and level of risk for each patient affect overall health. In addition, it is not possible to determine why patients choose extractions over restorative treatment. Authors speculate that financial constraints can be one of the most important determinants. Factors such as education, income, barriers to access to care, health literacy, health-seeking behaviors in adults, and health beliefs and perceptions are significant detainments but cannot be evaluated in claims data. In addition, the database does not provide information on the geographical location of the patients; it mentions that the data are from 13 states, but no further information is provided in the database. This study included CDT codes to ascertain treatments provided, but those codes do not provide disease diagnosis. The “Other” group reported under race/ethnicity is a large subgroup that limits our knowledge on who is included within that group.
Despite these limitations, this study provides strong evidence for policymakers to consider policy changes to prevent tooth loss. The evidence of periodontal treatment’s protective effect in the prevention of tooth loss can be used to emphasize the increase in Medicaid adult dental coverage to include periodontal treatment in all states. This evidence can also be used to advocate for medical-dental integration by colocating dental services in medical offices and training medical professionals to identify the dental implications of systemic diseases. Such policies can support achieving oral health goals for Healthy People 2030.
Author Contributions
T. Tiwari, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript; E. Tranby, M. Thakkar-Samtani, J. Frantsve-Hawley, contributed to conception, design, data acquisition, analysis, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.