
Abstract
Introduction:
A key purpose of denture provision is to enable eating, yet the body of evidence pertaining to the impact of dentures on wide-ranging nutritional outcomes has not been systematically reviewed.
Objectives:
To systematically review published evidence pertaining to the effect of wearing removable dental prosthesis on dietary intake, nutritional status, eating function, and eating related–quality of life (ERQoL).
Methods:
Eight questions relating to the impact of wearing dentures on nutritional outcomes were addressed. The target population was healthy adults aged ≥18 y. Data sources included Medline, Embase, CINAHL, and PubMed. Included were all human epidemiologic studies. The Newcastle-Ottawa score was used for appraisal of study quality. Harvest plots, vote counting, and accompanying narrative provided the basis for synthesis.
Results:
Of the 1,245 records identified, 134 were retrieved and eligibility assessed by 2 reviewers, and 41 studies were included in the synthesis (14 rated good quality, 20 fair, and 7 poor). The balance of data supported a positive impact of wearing full (5/7 studies) or partial (3/3 studies) dentures (vs. no dentures) on nutritional status, though no clear direction of effect was detected for the impact of dentures on dietary intake. The balance of data clearly showed that objective measures of eating function were compromised in full (14/15 studies) and partial (6/7 studies) denture wearers as compared with the dentate. Data showed that ERQoL was also compromised in denture wearers as compared with the dentate (3/3 studies). However, data showed a positive impact of wearing dentures on ERQoL (5/5 studies) as opposed to wearing no dentures.
Conclusion:
The balance of evidence shows that despite no clear pattern on impact of wearing dentures on measured dietary intake, in those with tooth loss, wearing dentures can have a positive impact on nutritional status and enjoyment of eating.
Knowledge Transfer Statement:
The results of this systematic review can be used to advocate for health care services to address prosthodontic need to benefit nutritional outcomes. The findings will be of use in educating health care professionals on the impact of wearing dentures and not addressing prosthodontic need on nutritional outcomes.
Introduction
Tooth loss in adults remains prevalent in many countries, and a large proportion of older adults rely on full or partial dentures for aesthetics, speaking, and eating. For example, in Australia 47% of adults aged ≥75 wear dentures (Do and Luzzi 2019), and the most recent UK data show that approximately 45% of those aged 75 to 84 y wear dentures (Public Health England 2020). By contrast, some low- and middle-income countries have a high prevalence of prosthodontic need, yet edentulism without prosthetic rehabilitation is common (de Oliveira Ferreira et al. 2014).
Tooth loss directly causes reduced chewing and eating function and results in avoidance of some foods. Observational studies report that tooth loss is associated with a poor diet, including lower intakes of fruits and vegetables (Nakamura et al. 2019), dietary fiber (Iwasaki et al. 2016), and protein (Iwasaki et al. 2016; Mendonça et al. 2018) and an increased risk of undernutrition (Zelig et al. 2018). However, a recent systematic review of longitudinal studies concluded that limited data were inconsistent (Gaewkhiew et al. 2019) and a causal relationship has not been established. If observed differences in nutritional outcomes by dental status are directly due to loss of function, it could be hypothesized that rehabilitation with dental prosthesis would result in improvement in nutritional indicators. Indeed, a key aim of providing dentures is to improve eating function and promote nutritional well-being; yet, despite the wealth of evidence pertaining to the association between tooth loss and nutritional outcomes, a systematic appraisal has not been performed to date of the evidence relating to the impact of wearing dentures on nutritional well-being. The aim of this research was to explore the impact of wearing dentures on eating and nutrition. The objective was to conduct a systematic appraisal of all available published literature pertaining to the impact of wearing dentures on dietary intake, measures of nutritional status and eating function, and eating-related quality of life (ERQoL; i.e., enjoyment of eating and social and emotional issues around eating). The overall research question was as follows: In adults, does wearing dentures, as compared with not wearing dentures, affect nutritional status and eating-related well-being?
Methods
A systematic review was conducted and reported according to the PRISMA statement (http://www.prisma-statement.org). The protocol was developed a priori and is available on Figshare (Moynihan and Varghese 2021). The specific questions addressed in this review were as follows.
In adults, does being edentulous and wearing full dentures, as compared with being edentulous and not wearing dentures or being dentate (with ≥20 natural teeth), reduce or increase
1) Risk of inadequate nutritional intake?
2) Risk of undernutrition?
3) Eating-related quality of life?
4) Eating function (mastication and swallowing measured subjectively or objectively)?
In adults, does being edentulous and wearing partial dentures, as compared with being partially dentate and not wearing dentures or being dentate (with ≥20 natural teeth), reduce or increase
5) Risk of inadequate nutritional intake?
6) Risk of undernutrition?
7) Eating-related quality of life?
8) Eating function (mastication and swallowing measured subjectively or objectively)?
Eligibility Criteria
The review included systematic reviews, randomized controlled trials, cohort studies, quasi-experimental studies, and quantitative observational studies (for the assessment of ERQoL, semiquantitative studies).
The following hierarchy was applied as a framework for narrative synthesis of the best available evidence (Petticrew and Roberts 2006): systematic reviews, randomized controlled trials, quasi-experimental studies, cohort studies, case-control studies, and cross-sectional studies. Only peer-reviewed studies published between January 1, 1980, to August 26, 2019, were considered for inclusion. Articles written in non-English language were included if they presented an English-language abstract.
Participants were apparently healthy adults aged ≥18 y from any country. The exposure variable was wearing complete or partial dentures, and the comparators were being edentulous without wearing full dentures (for edentulous), being partially dentate without wearing partial dentures (for partially dentate), and being dentate (≥20 natural teeth; for edentulous and partially dentate).
The outcome variables reported dietary intake (intake of energy, protein, fiber, saturated fat, and fruit/vegetables), indices of nutritional status (low body mass index, low Mini Nutrition Assessment score, percentage weight loss, low protein intake), measures of eating function (objective measures of chewing, biting, and swallowing foods and perceived chewing function scores), and ERQoL (e.g., self-reported semiquantitative data on eating problems including comfort, pleasure, flavor, and food avoidance; excluding predefined list or scores). Details of the exposure and intervention, control and comparator, and outcomes relating to each question are presented in Appendix Table 1.
Search Strategy
Relevant information was identified and retrieved by conducting searches of the following reference databases: Medline, Embase, and CINAHL. The search strategy is presented in Appendix Tables 2 to 4.
Study Selection and Data Extraction
Titles and abstracts of all records identified in the electronic search were assessed, and records that were clearly ineligible were eliminated by 1 reviewer. A random 10% sample of all records identified from searches were screened by a second reviewer, and interrater reliability was assessed. Any differences between the reviewers’ decisions were resolved by discussion, and if consensus was not reached, a third reviewer (P.M.) was consulted.
When the studies apparently met the inclusion criteria or insufficient information was in the abstract, 2 reviewers evaluated the full article. Difference between the reviewers’ decisions was resolved by discussion, and when consensus was not reached, a third reviewer was consulted. The reasons for exclusion of studies in this phase were logged. Data extraction was undertaken by 1 reviewer and checked by a second (P.M.). Disagreements between the reviewers was resolved by consensus, with involvement of a third reviewer (R.V.) where necessary.
Quality Assessment
The quality of the studies was assessed by 2 reviewers using the Newcastle-Ottawa Quality Assessment Scale, where stars are awarded by quality in terms of selection of participants, comparability of groups, and assessment of exposure or outcome (Wells et al. 2009). The quality of the studies was classified as good, fair, or poor based on the stars in each domain (selection, comparability, and exposure/outcome), following the Newcastle-Ottawa scale guidelines. A good quality score required 3 or 4 stars in selection, 1 or 2 stars in comparability, and 2 or 3 stars in exposure and outcomes. A fair quality score required 2 stars in selection, 1 or 2 stars in comparability, and 2 or 3 stars in exposure and outcomes. A poor quality score reflected 0 or 1 star in selection, 0 stars in comparability, or 0 or 1 star in exposure and outcomes (Appendix Table 5).
Synthesis
Evidence was grouped according to the 8 questions and each organized by study type and design (Fig. 1, Appendix Table 6). For each research question, a vote-counting approach based on direction of effect was employed to weight 1) the evidence showing a positive relationship between the exposure and outcome with 2) the evidence showing a negative relationship. This was based not on statistical significance but on direction of effect, with a 5% cutoff difference between groups as an arbitrary level of nutritional significance (McKenzie and Brennan 2019). Data were formulated into harvest plots to summarize study characteristics and the weight of evidence in relation to specific questions (Ogilvie et al. 2008). Where a study reported >1 outcome variable with respect to a research question (i.e., showing contrasting effects), separate data points were used to depict the identified outcome variables in the harvest plots. This approach was supplemented with a narrative synthesis of findings based on a “best available evidence” approach (Petticrew and Roberts 2006).
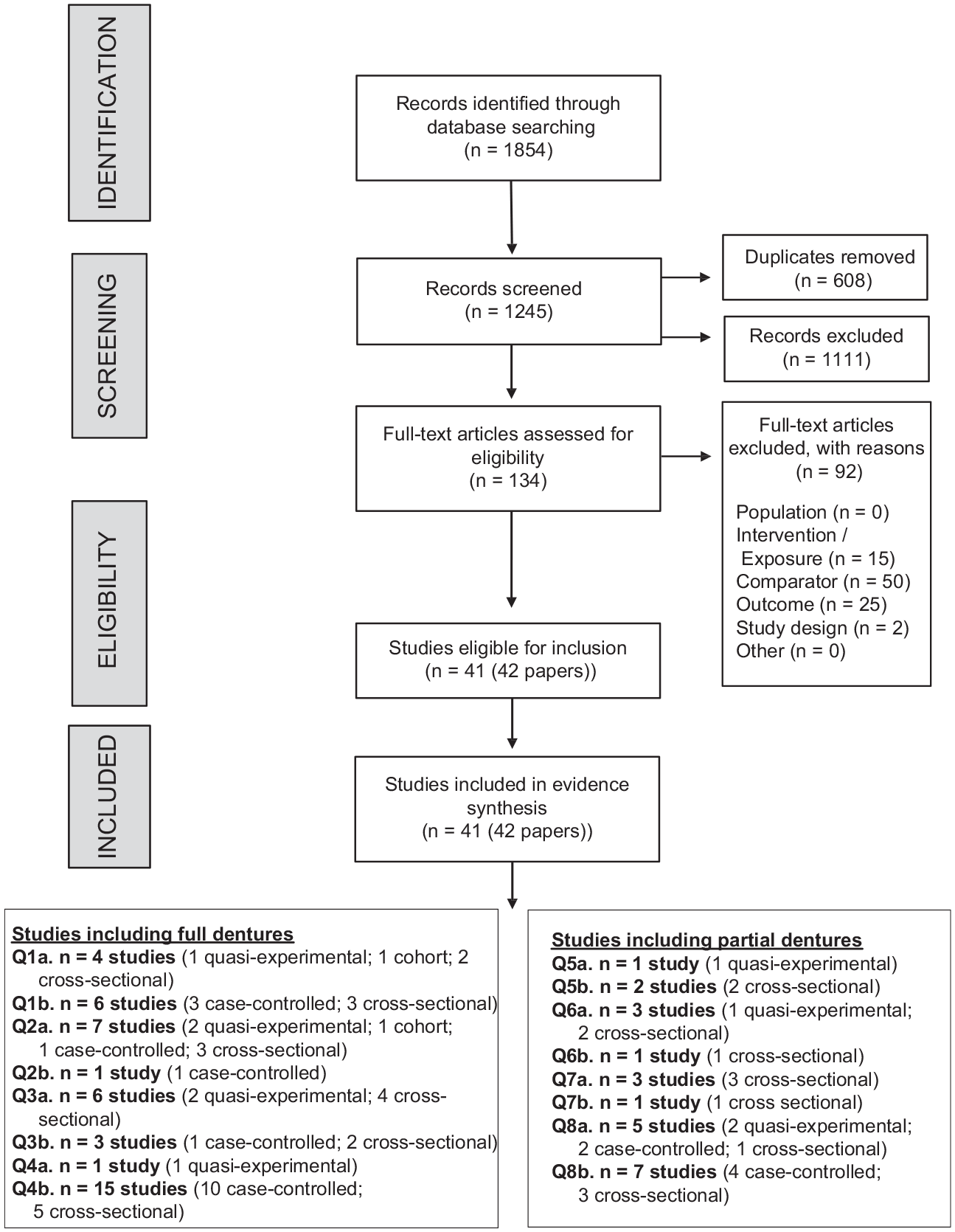
PRISMA flow diagram.
Results
Figure 1 shows the results of searching, the process of screening, and study exclusion to result in 41 studies in 42 articles. In total, 1,854 records were returned, reducing to 1,245 following removal of duplicates. The interrater reliability score indicated near perfect agreement for the 10% of articles screened in duplicate (kappa, 0.81). The reasons for exclusions on full-text screening are provided in Figure 1 and Appendix Table 7. The assigned Newcastle-Ottawa scores are provided in the Table, and details on components of the final score are presented in Appendix Table 5.
A breakdown of the number of studies for each main research question, in total and by study design, is provided in Figure 1 and Appendix Table 6. A brief description of the studies is provided in Appendix Table 8. A summary of the body of evidence pertaining to each question is presented in the Table, and the evidence synthesis is depicted in harvest plots in Figures 2 to 4. The results are considered in turn by research question.
Question 1: Does being edentulous and wearing full dentures reduce or increase risk of inadequate nutritional intake as compared with (Q1a) being edentulous and not wearing dentures and (Q1b) being dentate with ≥20 teeth?
Ten studies conducted in Asia, Europe, and the United States had data pertaining to the impact of wearing full dentures on nutritional intake (Table). In 4 studies, the comparator was being edentulous and not wearing dentures: all showed no association except 1 cross-sectional study (rated poor quality), which cited a lower intake of energy in denture wearing as compared with being edentulous and not wearing dentures (Sareela et al. 2016). Based on study type, the best available evidence came from the quasi-experimental study (Madhuri et al. 2014), which was rated fair quality and found no significant changes in intake of energy or macronutrients (obtained by one 24-h diet recall) in older Indian adults before versus following provision of complete dentures. Overall, to answer question 1a, these data suggest that being edentulous and wearing full dentures does not reduce or increase the risk of inadequate nutritional intake when compared with being edentulous and not wearing dentures.
Summary of Included Studies.

Full references to the articles cited in this table are presented in the Appendix.
BMI, body mass index; EMG, electromyography; FFQ, food frequency questionnaire; MNA, Mini Nutrition Assessment; NOS, Newcastle Ottawa Scale (quality assessment: 0 to 9, low to high quality; Wells et al. 2009).
+, a positive and significant relationship between denture wearing and nutritional outcome. 0, no significant relationship. –, a negative and significant relationship between denture wearing and the nutritional outcome. Significance based on direction of effect with a 5% cutoff for a nutritionally meaningful difference.
Mean or range.
Swallowing threshold test: percentage expectorated food passing through sieve.
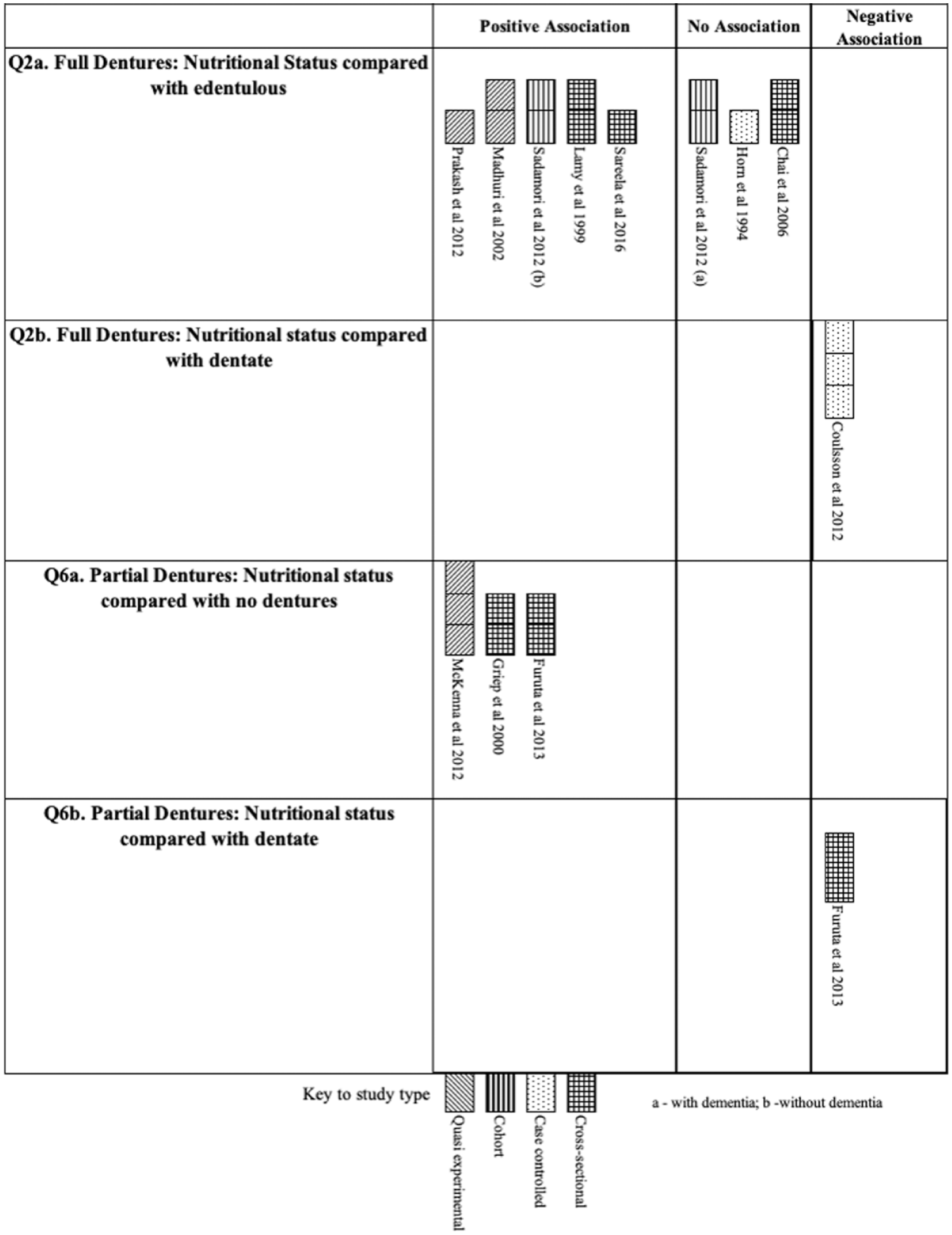
Harvest plot to illustrate weight of evidence for positive or negative effect of wearing full and partial dentures as compared with (
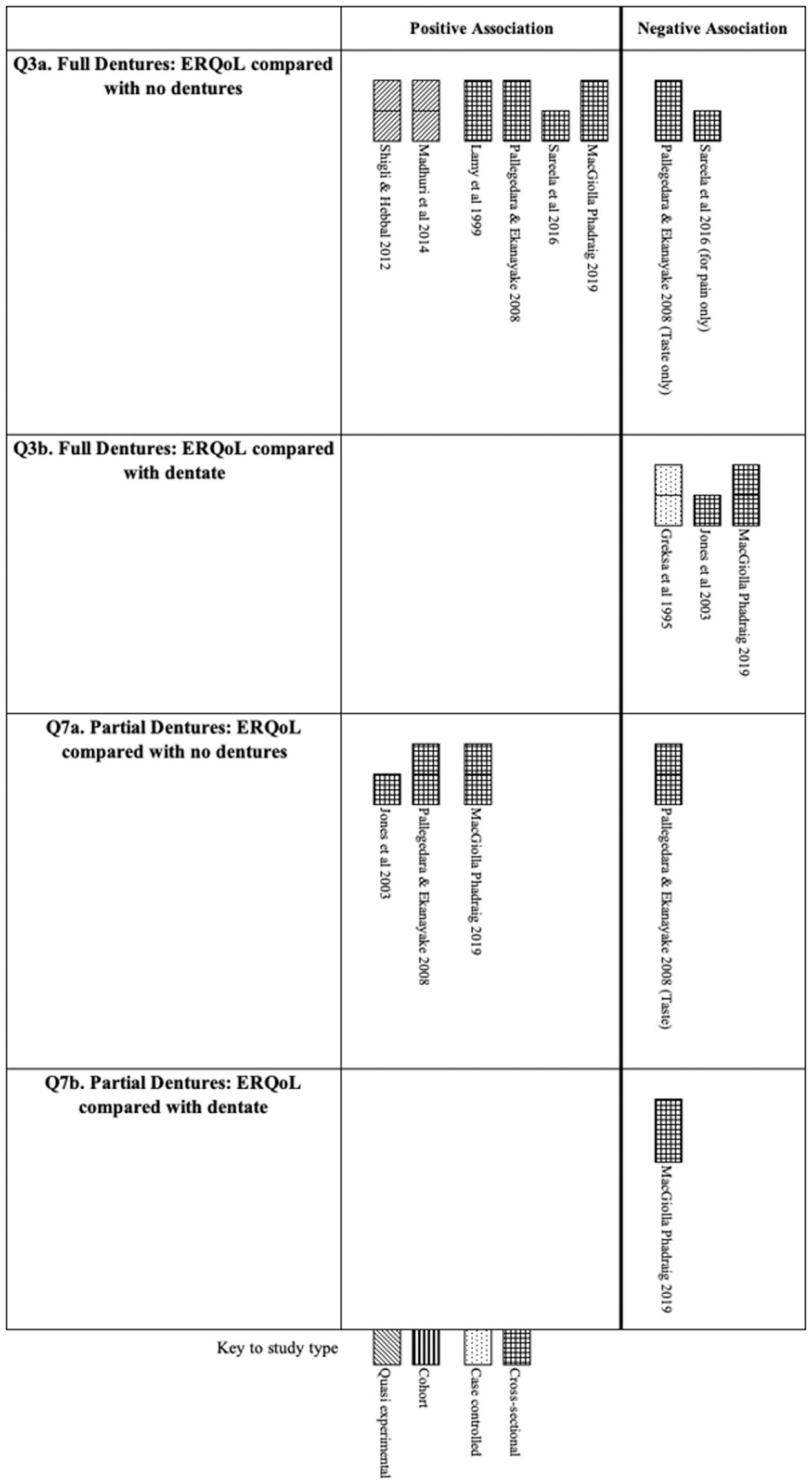
Harvest plot to illustrate weight of evidence for positive or negative effect of wearing full and partial dentures as compared with (
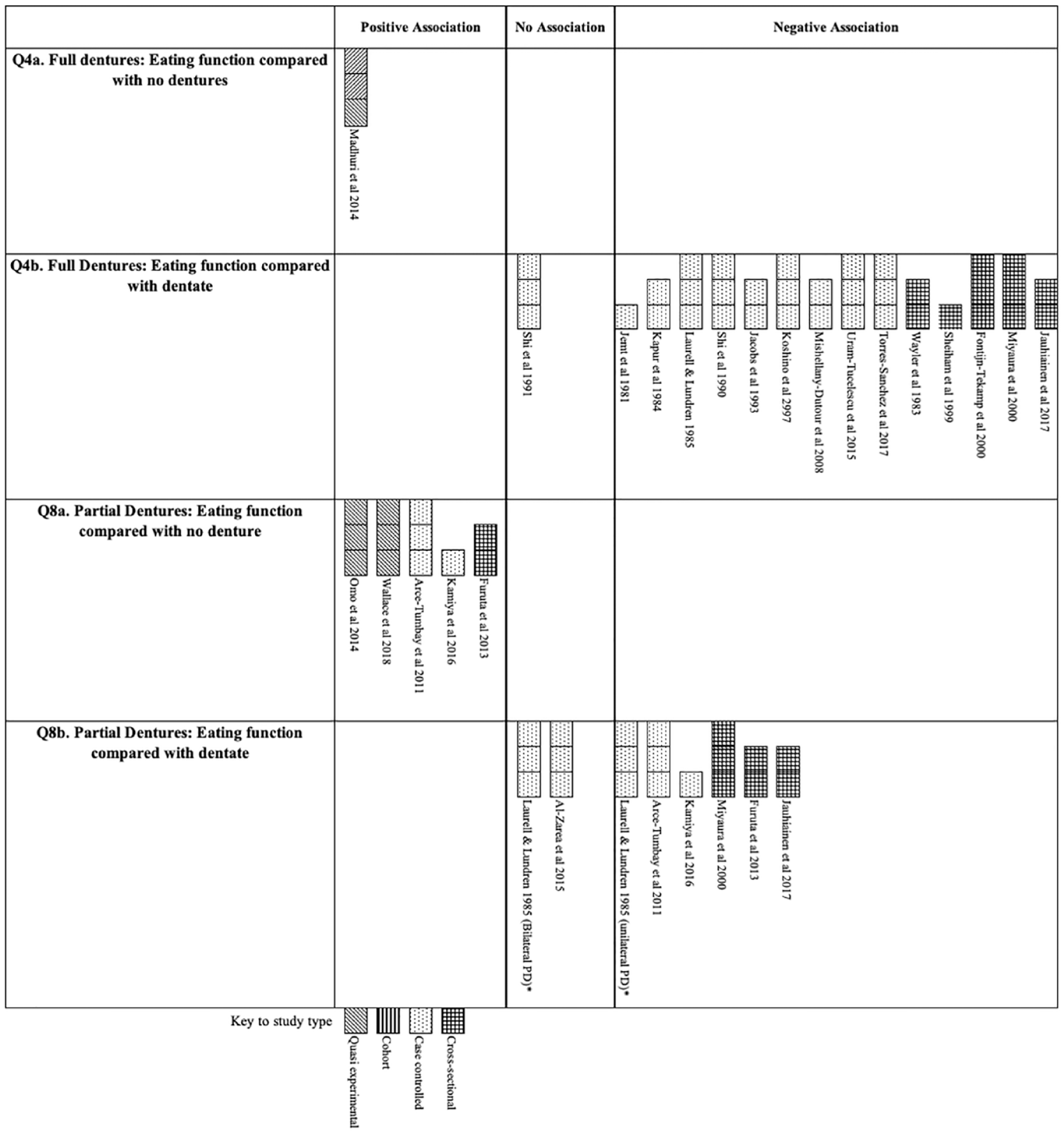
Harvest plot to illustrate weight of evidence for positive or negative effect of wearing full and partial dentures as compared with (
Six studies compared wearing full dentures with being dentate. Of these, 4 studies, all of fair quality, reported on energy intake: 2 cited at least 1 positive association (1 for females only) indicating that denture wearers had a higher intake of energy as compared with the dentate (Marshall et al. 2002; Jauhianen et al. 2017); 2 indicated no association (1 for males only; Greksa et al. 1995; Jauhianen et al. 2017); and 1 reported a negative association (Cousson et al. 2012). Three studies, all rated fair quality, reported on protein intake: 2 cross-sectional studies cited a negative association (with denture wearers having a lower protein intake [Marshall et al. 2002]; 1 for men only [Jauhiainen et al. 2017]), and 2 showed no association (Greksa et al. 1995; 1 in women only [Jauhiainen et al. 2017]). Three studies (1 rated good quality and 2 fair) measured fiber intake, with all showing at least 1 negative association (Nowjack-Raymer and Sheiham 2003; Cousson et al. 2012) and 1 for females only (Jauhiainen et al. 2017). One study, rated fair quality, measured saturated fat intake and found no association (Jauhiainen et al. 2017).
Based on study design, the best available evidence was from 3 case-control studies: 2 studies, 1 rated good quality and the other fair, measured fruit and vegetable intake, and both revealed a negative association (Greksa et al. 1995; Bradbury et al. 2008). The other study, which was rated good quality, indicated a lower intake of energy and fiber in denture wearers as compared with dentate controls (Cousson et al. 2012). Overall, based on the available data, being edentulous and wearing full dentures does not increase the risk of inadequate nutritional intake when compared with being dentate, with the exception of fruit and vegetable intake and fiber intake. Overall, there was much heterogeneity among studies with respect to nutritional outcomes measured, and a harvest plot depicting these data is presented in Appendix Figure 1.
Question 2: Does being edentulous and wearing full dentures reduce or increase risk of undernutrition as compared with (Q2a) being edentulous and not wearing dentures and (Q2b) being dentate with ≥20 teeth?
Eight studies had data pertaining to question 2: 2 quasi-experimental studies, 1 cohort study, 2 case-control studies, and 3 cross-sectional studies. No study was rated good quality. In 7 studies, the comparator was edentulous without dentures: 5 showed a positive association between wearing dentures and nutritional status as compared with wearing no dentures (1 study for people with dementia only; Sadamori et al. 2012), and 3 showed no association (1 for those without dementia only; Sadamori et al. 2012; Fig. 2). Based on study design, the best available evidence was provided by 2 quasi-experimental studies, both of which revealed a positive effect of wearing dentures on nutritional status as assessed by Mini Nutrition Assessment score (Prakash et al. 2012) and body mass index (Madhuri et al. 2014). However, the quality rating of these studies was poor and fair, respectively. Overall, to answer question 2a, the balance of the best available data suggests that being edentulous and wearing full dentures does reduce the risk of undernutrition as compared with being edentulous and not wearing dentures.
In 1 good-quality study, the comparator was being dentate. This study showed a negative association between wearing dentures and nutritional status; however, confounders were not accounted for (Cousson et al. 2012). Therefore, there are insufficient data to answer question 2b.
Question 3: Does being edentulous and wearing full dentures reduce or increase eating-related quality of life as compared with (Q3a) being edentulous and not wearing dentures and (Q3b) being dentate with ≥20 teeth?
Eight identified studies had data pertaining to question 3: 2 quasi-experimental studies, 1 case-control study, and 5 cross-sectional studies (Fig. 3). In 6 studies (5 rated fair quality and 1 poor), the comparator was edentulous without dentures: all showed at least 1 positive association between wearing dentures and ERQoL as compared with not wearing dentures. Two studies, both cross-sectional (1 rated poor quality and 1 fair), found at least 1 negative association: Saarela et al. (2016) for data pertaining to pain on eating only and Pallegedara and Ekanayake (2008) for data pertaining to perception of taste only. Overall, to answer question 3a, being edentulous and wearing full dentures does increase ERQoL when compared with being edentulous and not wearing dentures.
In 3 studies, the comparator was being dentate: all indicated a negative association between wearing dentures and ERQoL. Overall, to answer question 3b, being edentulous and wearing full dentures does reduce ERQoL as compared with being dentate.
Question 4: Does being edentulous and wearing full dentures reduce or increase eating function (mastication and swallowing) as compared with (Q4a) being edentulous and not wearing dentures and (Q4b) being dentate with ≥20 teeth?
Sixteen studies were identified with data pertaining to question 4: 1 quasi-experimental study, 11 case-control studies, and 4 cross-sectional studies. Data were from studies conducted in Asia, Europe, and United States (Table, Fig. 4). In 1 quasi-experimental study of fair quality, the comparator was being edentulous without dentures, and there was a positive association between provision of full dentures and chewing ability (Madhuri et al. 2014). However, there are insufficient data to answer question 4a. In 15 studies, the comparator was being dentate, and 14 showed a negative association between wearing dentures and eating function. Only 1 study (of fair quality) showed no association, and it did not account for age difference between denture wearers and dentate comparators (Shi et al. 1991). The best available evidence came from case-control studies, with 9 of 10 studies finding a negative association. Overall, with respect to question 4b, being edentulous and wearing full dentures reduces eating function (mastication and swallowing) when compared with being dentate.
Question 5: Does being partially dentate and wearing partial dentures reduce or increase the risk of inadequate nutritional intake as compared with (Q5a) being partially dentate and not wearing dentures and (Q5b) being dentate with ≥20 teeth?
Three studies conducted in Europe and the United States had data pertaining to question 5, including 1 randomized controlled trial with within-group data relevant to this review (i.e., quasi-experimental data) and 2 cross-sectional studies (Table). In 1 study of good quality, the comparator was being partially dentate before dentures, which showed a positive association between wearing partial dentures and intake of energy, protein, and fiber and no association for intake of fruits and vegetables (Moynihan et al. 2000). However, there are insufficient data to answer question 5a. In 2 studies, both cross-sectional and rated fair quality, the comparator was being dentate: both found no association between nutrient intake and wearing partial dentures as compared with being dentate. Overall, there are insufficient data to answer question 5b. Overall, there was much heterogeneity among studies with respect to nutritional outcomes measured, and a harvest plot depicting these data is presented in Appendix Figure 1.
Question 6: Does being partially dentate and wearing partial dentures reduce or increase risk of undernutrition as compared with (Q6a) being partially dentate and not wearing dentures and (Q6b) being dentate with ≥20 teeth?
Three studies had data to address question 6: 1 quasi-experimental study (rated good quality) and 2 cross-sectional studies (both rated fair quality). Data were from studies conducted in Asia and Europe (Table, Fig. 2). All studies had a comparator group of being partially dentate without dentures, and all showed a positive association between wearing partial dentures and nutritional status. Overall, with respect to question 6a, being partially dentate and wearing partial dentures reduces risk of undernutrition as compared with being partially dentate and not wearing dentures.
One cross-sectional study of fair quality had a dentate comparator and found a negative association between wearing partial dentures and nutritional status as compared with the dentate (Furuta et al. 2013). However, there were insufficient data to answer question 6b.
Question 7: Does being partially dentate and wearing partial dentures reduce or increase eating-related quality of life as compared with (Q7a) being partially dentate and not wearing dentures and (Q7b) being dentate with ≥20 teeth?
Three studies with data pertaining to question 7 were identified, and all were cross-sectional. Two were rated fair quality and 1 poor. Data were from studies conducted in Asia, Europe, and the United States (Table, Fig. 3). All 3 studies noted a positive association between wearing partial dentures (vs. not wearing dentures) and ERQoL. One study (rated fair quality) revealed 1 negative association for data pertaining to impact on perception of taste only (Pallegedara and Ekanayake (2008). Overall, with respect to question 7a, being partially dentate and wearing partial dentures increases ERQoL when compared with being partially dentate and not wearing dentures. In only 1 study, a comparator was being dentate, and this cross-sectional study, rated fair quality, indicated a negative association between wearing partial dentures and ERQoL (Mac Giolla Phadraig 2019). However, there are insufficient data to answer question 7b.
Question 8: Does being partially dentate and wearing partial dentures reduce or increase eating function (mastication and swallowing) as compared with (Q8a) being partially dentate and not wearing dentures and (Q8b) being dentate with ≥20 teeth?
Nine studies, reported in ten papers, had data that addressed question 8: 2 quasi-experimental studies, 4 case-control studies, and 3 cross-sectional studies. Data came from studies conducted in Africa, Asia, Europe, and the Middle East (Table, Fig. 4). In 5 studies (3 rated good quality, 1 fair, and 1 poor), the comparator was a partially dentate group that did not wear dentures, and all 5 studies cited a positive association between denture wearing and eating function. Overall, with respect to question 8a, being partially dentate and wearing partial dentures does increase eating function (mastication and swallowing) when compared with being partially dentate and not wearing dentures.
Seven studies reported data with a dentate comparator group: 6 studies (3 rated good quality, 2 fair, and 1 poor) cited at least 1 negative association (1 for unilateral denture only; Laurell and Lundren 1985), and 2 (both good quality) found no association (1 for bilateral denture only; Laurell and Lundren 1985). Overall, with respect to question 8b, being partially dentate and wearing partial dentures reduces eating function (mastication and swallowing) when compared with being dentate.
Discussion
To our knowledge, this is the first systematic review to investigate the impact of wearing dentures on a number of nutrition-related outcomes, including dietary intake, nutritional status, ERQoL, and eating function. Data came primarily from Asia, Europe, and the United States; the only data from South America, Africa, and the Middle East related to question 8. There were no data from Australia or New Zealand. With the exception of studies pertaining to eating function (for which the majority came from case-control studies), data identified in this review primarily came from cross-sectional studies. There were few data from cohort and quasi-experimental studies and none from randomized controlled trials. However, the lack of randomized controlled trials to address the questions of this review is likely due to ethical reasons (i.e., randomly assigning prosthetic treatment to 1 group while withholding from the control group would be unethical).
Impact of Dentures on Risk of Inadequate Nutritional Intake
The data did not suggest an impact of wearing dentures on the intake of macronutrients (question 1). Although denture wearers consistently showed a lower intake of fiber and fruits/vegetables as compared with the dentate, data pertaining to this impact were few (question 1). Moreover, studies were diverse in the nutrient outcomes explored, and many studies failed to use robust and validated nutrition assessment methods, were underpowered, and/or did not control for potential confounding (for details of these limitations, see Appendix Table 8). Assessment of the impact of dental function on diet and nutritional outcomes requires robust methodologies and a standardized approach to increase accuracy of results and facilitate cross-study comparisons (Moynihan et al. 2000).
Previous research has shown the edentulous to consume a less healthy diet than the dentate with respect to intake of fruits/vegetables and fiber (e.g., Chari and Sabbah 2019). However, a causal relationship between tooth loss and a poor diet has not been proven. If the effect was causal, some improvement in dietary intake on prosthetic rehabilitation would be expected, despite the inability of rehabilitation to totally mitigate the impacts of tooth loss, as rehabilitation does improve perceived chewing function. Still, the current review was unable to demonstrate this. Moreover, previous research on the impact of optimizing or replacing conventional full dentures has failed showed an impact on dietary intake in the absence of dietary intervention (Bradbury et al. 2006). Nevertheless, optimizing dentures and concurrent dietary intervention has shown a positive impact on diet (Bradbury et al. 2006: Suzuki et al. 2018).
The nutritional methods applied to studies that compared nutrient intake in partial denture wearers were adequate (see Appendix Table 8). However, the amount of data was too sparse to draw any conclusion, with only 1 quasi-experimental study comparing partial dentures with no dentures and 2 cross-sectional studies comparing partial denture wearers with the dentate. With respect to full and partial dentures, there is a need for well-designed prospective studies that use appropriate and validated nutrition and statistical methods to elucidate any impact of prosthetic rehabilitation on the intake of energy, macronutrients, fiber, and fruits/vegetables (i.e., nutrients associated with risk of noncommunicable diseases).
Impact of Wearing Dentures on Risk of Undernutrition
Despite the balance of evidence supporting a positive impact of wearing dentures (full and partial) on nutritional status as compared with not wearing dentures, there was much diversity in the nutritional outcome measures used (body mass index, Mini Nutrition Assessment, weight loss, and other nutrition screening tools) and limitations in data reporting; none of the data were rated good quality. There were insufficient data comparing risk of undernutrition between full or partial denture wearers and dentate persons to draw any conclusion, and more well-designed studies are required to determine if provision of dentures fully mitigates the impact of tooth loss on risk of undernutrition. Undernutrition in older people is a global problem with far-reaching consequences for morbidity and mortality (Favaro-Moreira et al. 2016). The current findings, though not based on good-quality studies, suggest that for those with loss of teeth, provision of dentures may help mitigate undernutrition; the results also indicate that closer attention to oral health status be considered in strategies for prevention on undernutrition in older persons.
Impact of Wearing Dentures on ERQoL
The balance of data pertaining to ERQoL demonstrated that in the edentulous and partially dentate, wearing dentures was associated with a better ERQoL; however, the ERQoL of denture wearers was inferior to that of fully dentate persons. Data pertaining to the impact of wearing partial dentures (question 6) were fewer and solely based on cross-sectional studies, thus specifying a need for prospective studies on the impact of provision of partial dentures on ERQoL as well as on diet and nutritional status.
Impact of Wearing Dentures on Eating Function
The balance of data clearly showed that full and partial denture wearers have reduced eating function when compared with the dentate despite the heterogeneity in measures used to assess eating function. Data unanimously demonstrated better eating function in the partially dentate with dentures than in those without. However, the review identified a lack of evidence pertaining to the impact on eating function of full versus no dentures, with the 1 identified study reporting data on perceived chewing scores only but nonetheless indicating a positive effect. These data demonstrate a need for clinicians to manage patient expectations around level of restoration of eating function with dentures and provide practical advice on coping strategies around eating to mitigate reduced eating functionality (Roessler 2003). Despite the lack of data from objective measures, the data on ERQoL clearly show an advantage to the edentulous of wearing dentures.
Limitations of the Review
Several limitations to the current study need to be acknowledged. First, it did not explore the impact of replacement or optimization of full or partial dentures in existing denture wearers on the nutritional outcomes, and this warrants exploration. The questions pertaining to intake of nutrients did not include the impact of wearing dentures on the micronutrient intake. However, this review focused on the intake of macronutrients known to be associated with risk of noncommunicable diseases (obesity, type 2 diabetes mellitus, and cardiovascular disease) and undernutrition (energy and protein intake). The search did, though, identify the studies that reported on the impact of wearing dentures on intake of micronutrients: most found negative and null findings (Greksa et al. 1995; Cousson et al. 2012; Han and Kim 2016; Saarela et al. 2016; Jauhiainen et al. 2017); yet, none appropriately adjusted micronutrient intakes for energy intake. The review also excluded studies for which there was not an English-language abstract, which may in part explain the lack of data from Latin American, Middle Eastern, and African countries. Finally, studies pertaining to ERQoL were limited to those providing quantitative and semiquantitative data, and studies employing purely qualitative data were excluded. Qualitative data may provide a more in-depth assessment of the nuanced impact of wearing dentures on eating. Future studies exploring the impact of wearing dentures on ERQoL should consider qualitative as well as quantitative evidence synthesis.
Conclusion
Although there are insufficient data to compare the nutritional status of denture wearers with the dentate, the best available evidence suggests that wearing dentures (full or partial) over not wearing dentures may reduce risk of undernutrition. Moreover, despite full denture wearers having poorer ERQoL when compared with the dentate, wearing full dentures may improve ERQoL. The balance of evidence shows that denture wearers (full and partial) have reduced eating function as compared with the dentate. Sufficient data show that wearing partial dentures improves eating function in those with tooth loss. There is a need for more well-designed prospective studies—with regard to nutritional methodology and sample size while controlling for confounders—to determine any impact of prosthetic rehabilitation with dentures on the intake of energy and nutrients.
Author Contributions
P. Moynihan, contributed to the conception, design, and interpretation of the data, drafted and critically revised the manuscript; R. Varghese, instigated the project and contributed to the conception and interpretation of the data, critically revised the manuscript. Both authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844211026608 – Supplemental material for Impact of Wearing Dentures on Dietary Intake, Nutritional Status, and Eating: A Systematic Review
Supplemental material, sj-docx-1-jct-10.1177_23800844211026608 for Impact of Wearing Dentures on Dietary Intake, Nutritional Status, and Eating: A Systematic Review by P. Moynihan and R. Varghese in JDR Clinical & Translational Research
Footnotes
Acknowledgements
We thank Lisa Lovelidge, PhD, and Clare Gurton, BSc (hons), from Lucid for providing editorial and medical writing support, including searching, screening, and interrater reliability assessments, which were funded by GSK. We gratefully acknowledge the contribution of Dr. Edoardo Aromataris from the Joanna Briggs Institute at The University of Adelaide for guidance on the evidence synthesis and for feedback on the manuscript. The views expressed are our own.
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P. Moynihan’s institution received a consultancy fee with respect to some of the work on which this article is based. R. Varghese is an employee of GSK Consumer Healthcare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded in part by GSK.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.