
Abstract
Background:
A number of studies in patients with periodontitis have compared scaling and root planning (SRP) combined with an adjunctive treatment to SRP alone. Within that literature, an array of studies with overlapping investigators has consistently yielded substantially greater effects of adjunctive treatments than had been previously noted. This report investigates discrepancies between that cluster of research and the most recent American Dental Association (ADA) systematic review.
Methods:
This review was preregistered at https://osf.io/4meyd/. A search using the Scopus platform identified 32 articles published from 2010 to 2017 by investigators affiliated with the Government Dental College and Research Institute (GDCRI) in Bangalore, India. The primary outcome used in this meta-analysis was the change in clinical attachment level (CAL) after 6 mo. Effect sizes were estimated using Comprehensive Meta-Analysis software after categorizing agents into groups based on pharmacologic similarity.
Results:
The search identified 32 studies encompassing 5 sets of adjunctive agents. Across the GDCRI studies, the CAL averaged 1.67 mm (95% confidence interval [CI]: 1.43–1.91 mm), substantially exceeding values reported in the ADA review (mean: 0.39 mm, 95% CI: 0.27–0.51 mm). For categories of studies in which comparable subgroup estimates were available, the evaluations yielded overlapping estimates of SRP alone, but CAL estimates were discrepant for both locally delivered antimicrobials (GDCRI studies: mean: 1.45 mm, 95% CI: 0.63–2.27 mm; ADA review: mean: 0.38 mm, 95% CI: 0.16 –0.60 mm) and systemic antibiotics (GDCRI studies: mean: 1.35 mm, 95% CI: 0.97–1.73 mm; ADA review: mean: 0.39 mm, 95% CI: 0.21–0.57 mm).
Conclusion:
In the literature on adjunctive agents supplementing SRP, findings from investigators linked to GDCRI stand out as having significantly more favorable estimated effects. Meanwhile, some agents studied by GDCRI-linked investigators have not been investigated by other researchers. In the absence of a clear explanation for discrepant results, it is recommended that unusually favorable reported effects of adjunctive agents be viewed with caution.
Knowledge Transfer Statement:
The present meta-analysis observed an unusually large effect size of adjunctive agents to scaling and root planning in studies conducted by the same research group. These results were not consistent with trials on adjunctive agents and previous reports. As this research group has exclusively tested most of the agents, their results must be viewed with caution until other independent groups replicate the studies and reproduce the effect size.
Keywords
Introduction
Therapeutic agents adjunctive to scaling and root planing (SRP) have demonstrated modest adjunctive efficacy (Smiley et al. 2015b; John et al. 2017). Studies of systemic antibiotics and local delivery of antimicrobials run by several different and independent investigator groups had to use large sample sizes to demonstrate relatively modest adjunctive effects (Jeffcoat et al. 1998; Garrett et al. 1999; Williams et al. 2001). In contrast, 4 recent meta-analyses of locally delivered statins showed large adjunctive effects in much smaller sample sizes (Estanislau et al. 2015; Ambrosio et al. 2018; Bertl et al. 2018; Muniz et al. 2018). Careful review of the included studies in the statin systematic reviews revealed that most studies were conducted in India by the same group of authors (Pradeep, Kumari, et al. 2013; Pradeep, Rao, et al. 2013; Rao, Pradeep, Bajaj, et al. 2013; Pradeep, Karvekar, et al. 2015; Kumari et al. 2016; Pradeep, Garg, Kanoriya, et al. 2016; Kumari et al. 2017; Martande et al. 2017; Pradeep, Kanoriya, et al. 2017; Priyanka et al. 2017). Hence, one of the systematic reviews recommended that “confirmation of these results, and especially of the effect size, from other research groups is warranted.”
The replication of clinical trial outcomes at different clinical sites by independent investigators is required to verify new findings. Systematic reviews and meta-analyses then compare results among different clinical sites and investigators. Given that the above research team has conducted studies with large adjunctive effect sizes for a plethora of adjunctive agents including a unique focus on statins (Agarwal et al. 2012; Bajaj et al. 2012; Pradeep, Kalra, et al. 2012; Pradeep, Sharma, et al. 2012; Sharma and Pradeep 2012a, 2012b; Pradeep, Bajaj, et al. 2013; Pradeep, Kumari, et al. 2013; Pradeep, Priyanka, et al. 2013; Pradeep, Rao, Bajaj, et al. 2013; Pradeep, Rao, Naik, et al. 2013; Rao, Pradeep, Bajaj, et al. 2013; Rao, Pradeep, Kumari, et al. 2013; Pradeep et al. 2014; Martande et al. 2015; Pradeep, Karvekar, et al. 2015; Pradeep, Singh, et al. 2015; Priyanka, Kalra, Saquib, Kudyar, et al. 2015; Priyanka, Kalra, Saquib, Malgaonkar, et al. 2015; Kumari et al. 2016; Martande et al. 2016; Pradeep, Garg, Kanoriya, et al. 2016; Pradeep, Garg, Raju, et al. 2016; Pradeep, Patnaik, et al. 2016; Agarwal et al. 2017; Kumari et al. 2017; Martande et al. 2017; Pradeep, Kanoriya, et al. 2017; Pradeep, Patnaik, et al. 2017; Priyanka et al. 2017; Sharma et al. 2017; Kanoriya et al. 2018), we aimed to conduct a systematic review with quality assessment and meta-analysis of their studies evaluating the effect of adjunctive agents to SRP for patients with periodontitis in comparison of SRP alone.
The goal of this article is to report the results of a meta-analysis of studies on adjuncts with SRP conducted by studies affiliated with the Government Dental College and Research Institute (GDCRI) in Bangalore, India, associated with an individual researcher (A.R. Pradeep) and to determine the overall effect of the intervention on clinical attachment level (CAL) and test its consistency. We also aimed to determine the population and/or study design factors (initial severity of attachment level, number of sites per subject, type of subject sample, size of the SRP effect in the control group) that might have influenced the effect size as well as the level of heterogeneity in these studies. Study elements such as effect size, size of the SRP effect in the control group, and initial attachment level will be compared, when possible, to the corresponding results from the American Dental Association (ADA)–related meta-analysis (Smiley et al. 2015a, 2015b). A companion report presents the search strategy and assessment of reporting the quality of the included studies (part 2).
Materials and Methods
A preregistration record of this systematic review and meta-analysis can be found online at https://osf.io/4meyd.
The detailed search strategy and quality assessment were outlined in the companion article. The PRISMA flowchart is included in the companion article as well (part 2). Articles were retrieved using Scopus and PubMed search engines. Briefly, we included only randomized controlled trials (RCTs) examining the effect of SRP and adjuncts limited to authorship by Pradeep. Study populations were limited to periodontitis patients. We included studies with data at baseline and 6 mo. Studies published from 2010 to 2017 were included. Cohort, nonrandomized trials, or observational studies were excluded. RCT reports in languages other than English were excluded. RCTs that included furcation defects and adjuncts such as lasers, photodynamic therapy, and platelet fibrin were excluded.
The following data were extracted from the included studies independently (K.A.-A., J.C.G.), using a data extraction sheet developed based on the Cochrane Handbook for Systematic Reviews of Interventions guidelines (Cumpston et al. 2019):
Baseline clinical parameters: pocket depth, CAL, and bone fill
Sample size in each group
Number of intervention arms in each study and each group
Population characteristics
Follow-up period
Clinical parameters at 6 mo: pocket depth, CAL, and bone fill
Type of adjuncts used in each intervention
Based on the CONSORT guidelines, there is an expectation that these data should be reported as part of an RCT protocol (Moher et al. 2012). The absence of such information was considered in the quality assessment of these articles, or articles were excluded per our inclusion and exclusion criteria. Given the above, authors were not contacted for additional information.
Statistical Methods
The first step of the analysis was to determine if there was evidence to support an overall effect for the adjunctive therapies and to estimate the individual study effect sizes. The program used for analysis was Comprehensive Meta-Analysis (Borenstein 2013). In the analysis, the adjunctive agents were categorized into 5 pharmacologic groups (local antibiotics, systematic antibiotics, statins, metformin, bisphosphonates, and other agents). In the other agent category, we included boric acid and aloe vera, which could not be otherwise categorized. The heterogeneity of the studies (inconsistencies between the studies) was primarily evaluated with I² (Borenstein 2013; Higgins et al. 2003) as it describes the percentage of variation in the outcome variable across studies that is due to heterogeneity rather than chance. Studies with multiple arms and, hence, multiple active agents, were treated in the meta-analysis (Fig. 1) as individual studies. This approach allowed for the direct comparison of the therapeutic CAL difference between control and active agent with other reports. The significance levels were not adjusted for multiple comparisons with the control groups. Both fixed effects and random effects models were used. The more conservative random effects model is shown in the report. To determine which model (either fixed or random effects) was the most appropriate for summarizing the treatment effects in the meta-analysis, the heterogeneity of the studies was investigated. Some authors (Higgins et al. 2003) have suggested levels of I2 of 25%, 50%, and 75% as criteria for mild, moderate, and severe heterogeneity, respectively. Most of the groups of studies in this analysis were characterized by severe levels of heterogeneity, with the exception of the adjunctive categories of bisphosphonates and systemic antibiotics that showed moderate levels of 50.83 and 60.67, respectively. Because of the high levels of heterogeneity, random effects were used to summarize the studies in this report. The fixed effects model was also run, and results were similar to those from the random effects model, although not shown.
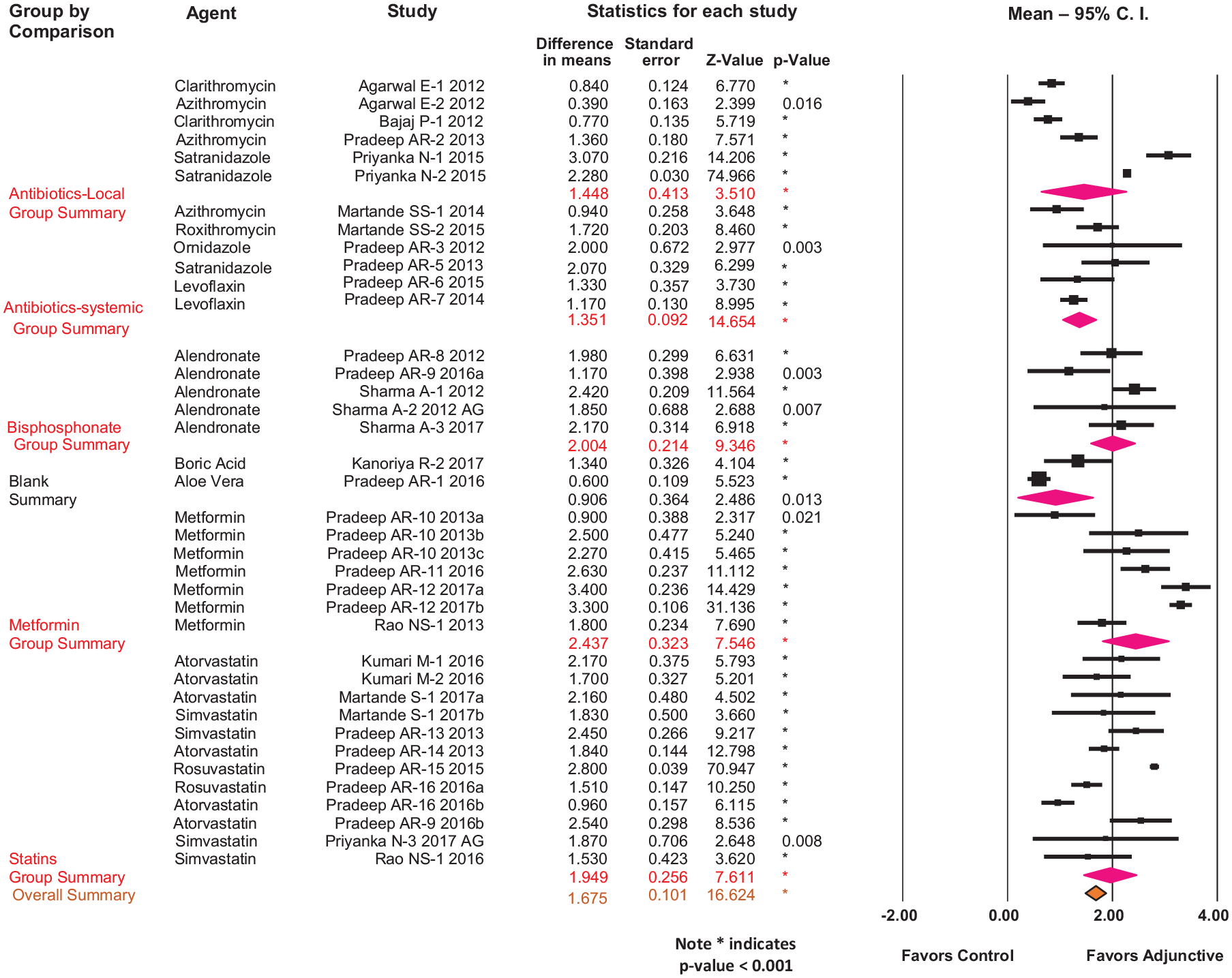
Forest plot of the overall effect size and the effect size of each adjunctive agent derived from the Government Dental College and Research Institute studies estimated by random effects model.
The next set of analyses were aimed to determine if the effect size could be explained by clinical factors in the studies. Hence, the following variables were investigated: 1) mean CAL at baseline in the control group, 2) effect size of SRP in the control arm, and 3) type of patient population. When possible, these data attributes were compared with those of the ADA review. To evaluate these effects, descriptive statistics and appropriate analysis of variance models using the study as the unit of analysis and the study sample size as the weight in the model were performed. Some of these potential predictor variables were not distributed evenly across the different agents, and that was considered, where appropriate. In addition, the analysis of the results was not adjusted for the multiple arms.
The goal of the final set of analyses was to compare the size effect of SRP alone (control group) and/or the adjunctive effect of various agents between the GDCRI studies and the ADA review. Spearman rank test was used for correlation analysis. Two similar adjunctive therapies, systemic antibiotics and local delivery of antibiotics, were compared, and the adjunctive effect was assessed. The data shown in the ADA meta-analysis results did not directly derive from the ADA manuscript but from the raw data of the ADA report. This was necessary so that we could run summary statistics as stratified by adjunct group. Only studies that reported baseline values for both groups were included in the table. Therefore, the studies in the ADA report without an estimate SRP effect were not included. In addition, only one study (Martande et al. 2016) of the GDCRI studies was included in the present meta-analysis as well as the ADA review.
Results
Thirty-two studies with 38 comparisons (active arms versus control arms) were included in the meta-analysis of the GDCRI studies (Fig. 1). There were 12 different agents studied and grouped into 5 pharmacologic categories. The included studies had similar study designs, similar subject inclusion/exclusion criteria, and nearly identical sample size. More detailed characteristics of each study are reported in the quality assessment part of this project (part 2).
Table 1 also summarizes comparative data of the results retrieved from the GDCRI studies and the ADA systematic review. The number of comparisons (N) of the active arms versus the control arms in each study are presented in Table 1. Several studies by the GDCRI group used more than 2 active arms, producing higher numbers of comparisons. The overall mean CAL effect was estimated to be 1.67 mm (95% confidence interval [CI]: 1.43–1.91 mm); the parallel findings from the ADA review yielded an overall mean of 0.39 mm (95% CI: 0.27–0.51 mm). Point estimates of the CAL effect for subgroups of the GDCRI studies ranged from 0.91 mm to 2.44 mm (Table 1). For the categories in which comparable estimates were available from the ADA review, the evaluations yielded overlapping estimates of SRP alone, but CAL estimates were discrepant for both locally delivered antimicrobials (GDCRI studies: mean: 1.45 mm, 95% CI: 0.63–2.27 mm; ADA review: mean: 0.38 mm, 95% CI: 0.16–0.60 mm) and systemic antibiotics (GDCRI studies: mean: 1.35 mm, 95% CI: 0.97–1.73 mm; ADA review: mean: 0.39 mm, 95% CI: 0.21–0.57 mm). The GDCRI studies also included multiple studies yielding estimated CAL effects for bisphosphonates (mean: 2.00 mm, 95% CI: 1.58–2.42 mm), metformin (mean: 2.44 mm, 95% CI: 1.80–3.08 mm), statins (mean: 1.95 mm, 95% CI: 1.53–2.37 mm), and other miscellaneous adjunctive treatments (mean: 0.91 mm, 95% CI: 0.13–1.69 mm). Therefore, irrespectively of the type of adjunctive agent, we found much larger effect sizes compared with the ADA review.
Comparison between the Results Obtained from the GDCRI Studies’ Meta-Analysis and the ADA-Related Systematic Review. a
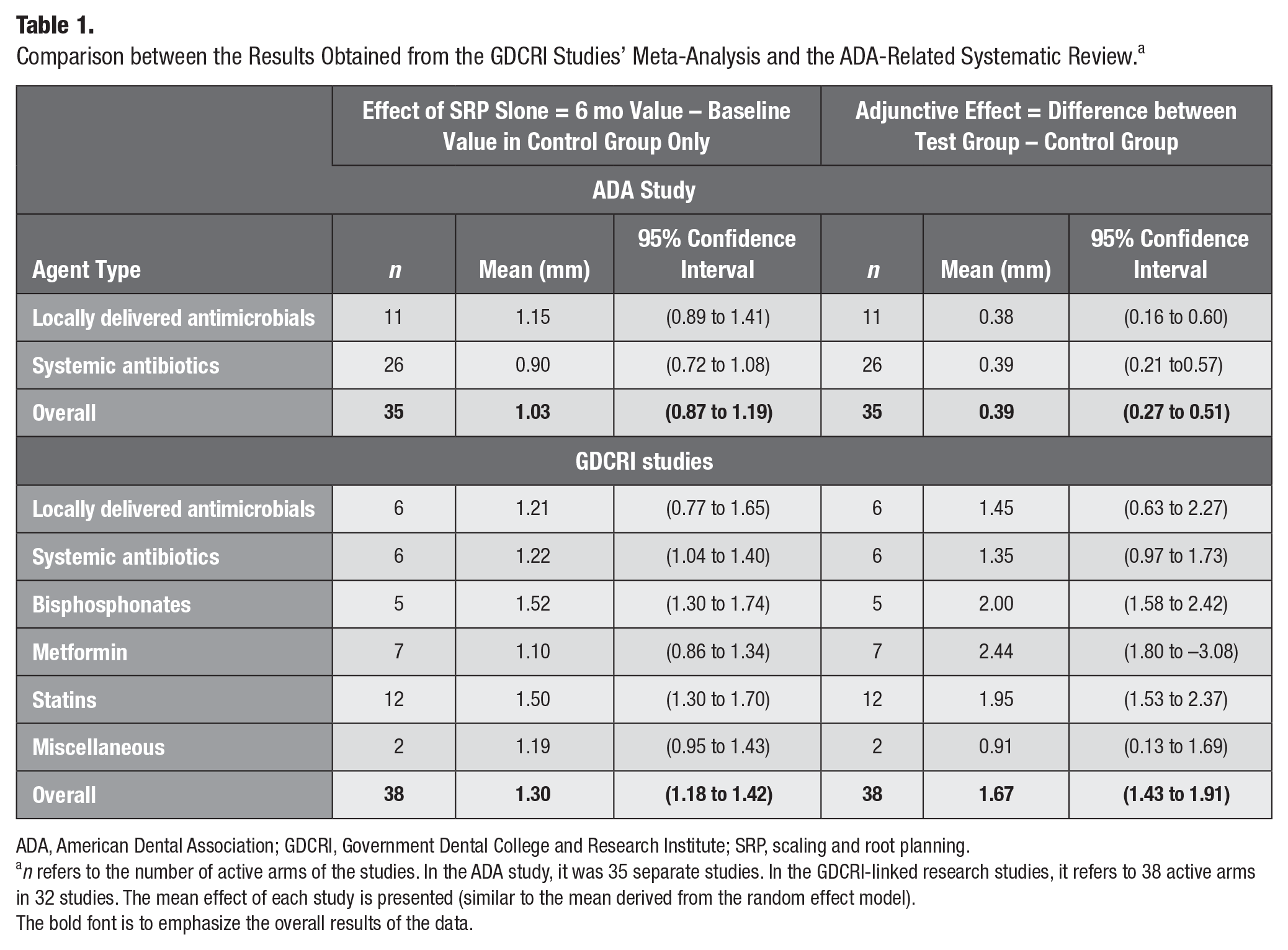
ADA, American Dental Association; GDCRI, Government Dental College and Research Institute; SRP, scaling and root planning.
n refers to the number of active arms of the studies. In the ADA study, it was 35 separate studies. In the GDCRI-linked research studies, it refers to 38 active arms in 32 studies. The mean effect of each study is presented (similar to the mean derived from the random effect model).The bold font is to emphasize the overall results of the data.
There was a great deal of methodological and statistical similarity among the GDCRI studies. There was a consistent sample size for both test and control groups, of 27.03 (95% CI: 23.98–30.08) for the control group and 27.33 (95% CI: 24.19–30.48) for the test group. The sample size of the 38 comparisons in the 32 studies ranged between 18 to 33 subjects and 17 to 34 subjects for the control and test groups, respectively. Thus, there was a very narrow range of sample sizes.
The clinical inclusion criteria were similar for all studies as well. While in most of the studies, the investigators included only 1 site per subject, within the 13 studies focusing on either local or systemic antibiotics, there were 3 studies that used more than 1 site per subject. The mean response for the adjunctive effect in studies that used 1 site was 1.51 mm (SE = 0.47 mm), whereas the 3 studies with more than 1 site per subject had a mean adjunctive of effect of 1.48 mm (SE = 0.26 mm). The difference between the 2 groups was not significantly different.
Another effect of interest was related to the patient population. Most of the studies in this review consisted of subjects with chronic periodontitis (CP); however, in 6 studies, the subjects were smokers with CP and in 7 studies, the subjects were diabetic with CP. Systemic antibiotics were not evaluated in smokers and/or diabetics. In an analysis of variance model with the remaining agents present, there were no clinically important statistically significant differences between the adjunctive effect for CP alone, CP smoker, and CP diabetic subjects of 1.35 mm, 1.27 mm, and 1.42 mm, respectively (Table 2). Thus, the number of sites investigated within the subjects as well as the subject characteristics could not explain the size of the adjunctive effects found in the report.
Summary of Adjunctive Effect Stratified by Population Medical Profile for Chronic Periodontitis for the GDCRI Studies.
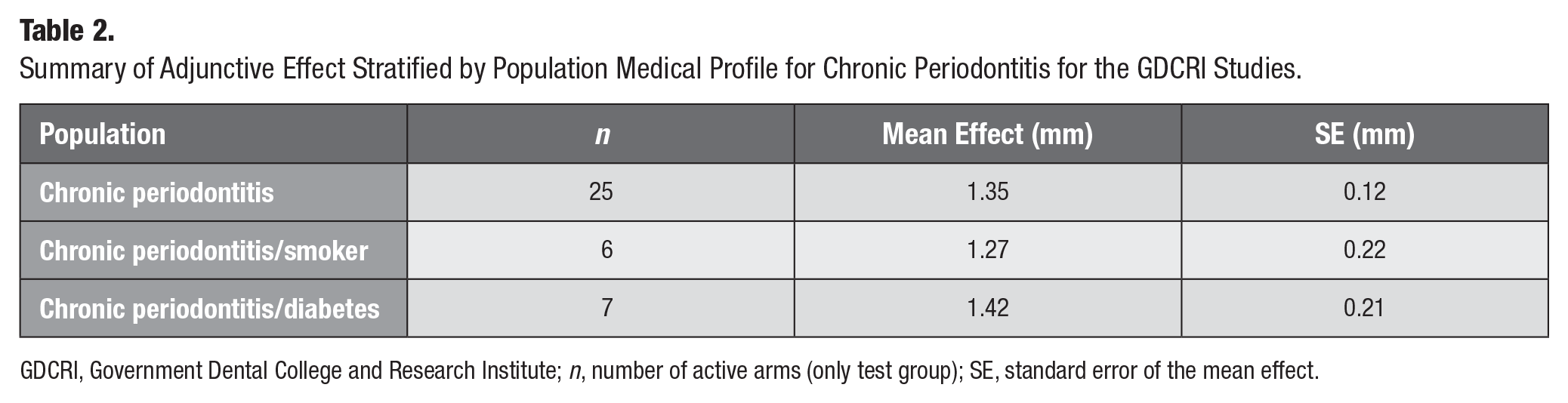
GDCRI, Government Dental College and Research Institute; n, number of active arms (only test group); SE, standard error of the mean effect.
The severity of disease at baseline was investigated to determine if it influenced the adjunctive effect. A moderator variable (mean control baseline CAL level) was regressed against the difference between adjunctive and control arms (the adjunctive effect). No relationship could be found between the size of the adjunctive effect and size of the initial control mean attachment loss of the individual studies in this review. The estimated correlation of 0.19 between the 2 effects was modest and not statistically significant (Fig. 2). Thus, the initial attachment loss in the reports could not explain the size of the adjunctive effects.
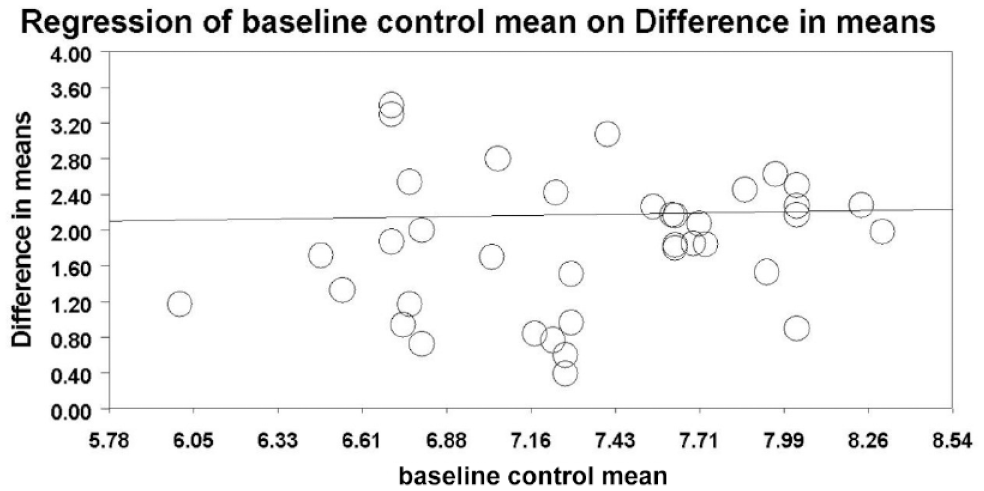
Evaluation of the effect of baseline clinical attachment level (severity of periodontitis) on the adjunctive effect size (difference in means).
All included studies reported large and significant treatment effects. The effects separated by agent types (Table 1; Fig. 1) demonstrated a consistent finding in the meta-analysis: a very large effect size for the adjunctive effect of all agents tested (test minus controls over 6 mo), as shown in the forest plot of the data (Fig. 1; Table 1). The overall adjunctive mean CAL effect of studies grouped by type of adjunctive agent was 1.67 mm, ranging from a mean of 0.91 mm to a greatest mean group of 2.44 mm.
In addition, the GDCRI studies reported a larger overall mean effect of SPR alone (1.30 mm) compared with the ADA review (1.03 mm), suggesting that GDCRI studies were perhaps treating more severe periodontitis cases. However, when limiting the analysis in the systemic antibiotic studies, the GDCRI group reported a mean effect of SRP alone (1.22 mm), which was fairly similar to the ADA review (1.15 mm). Results also showed that the effect size of SRP alone did not change with sample size, because of the similarity of sample size across the studies (Appendix Figure 1). More importantly, these differences in effect size of SRP alone did not explain the nearly 3 times greater adjunctive effect in the GDCRI studies compared with the ADA review, regardless of the way the data were evaluated.
Discussion
The primary objective of this report was to determine the overall adjunctive effect of the GDCRI studies and compare it to the ADA-related meta-analysis. This report also included the assessment of population and/or study design factors that could explain the large effect size in the GDCRI studies. We found that the overall adjunctive effect in the meta-analysis of the studies by the GDCRI studies was 1.67 mm, whereas the corresponding effect in the ADA review was 0.39 mm. When limiting the analysis on studies of systemic and local antibiotics, we observed that the adjunctive effect by GDCRI studies was 3 times greater than the effect reported by the ADA review. Further, we found that periodontitis severity at baseline, sample size, and other population characteristics could not explain the large adjunctive effects in the GDCRI studies.
The direct comparison with the ADA-related review and meta-analysis put the size of the adjunctive effect of the GDCRI studies in context with other current literature on adjunctive therapies. The ADA systematic review was a state-of-the-art review on the status of adjunctive agents using the change in CAL as a primary outcome (Smiley et al. 2015b). The ADA systematic review was accompanied by recommendations on the efficacy of the adjunctive therapies (Smiley et al. 2015a). Thus, the ADA systematic review provided a comprehensive analysis based on existing evidence on adjunctive agents.
Interestingly, evidence on locally delivered agents such as metformin, bisphosphonates, boric acid, aloe vera, and almost all of the studies on statins was produced exclusively by the GDCRI group in the absence of strong mechanistic evidence of biological plausibility.
Although there is no evidence to support the geographic gradient in the clinical response to periodontal treatment, Indian populations might have a more pronounced response to adjunctive periodontal treatment. This could be a hypothesis to be tested. If, indeed, this hypothesis is confirmed, the results of GDCRI research studies might not be generalizable to other populations and hence might be characterized by limited external validity. It is important to emphasize that 45% of included RCTs were published in the Journal of Periodontology, disseminating results with potentially limited external validity to US readership. In any case, before accepting adjunctive agents as efficacious, additional research involving experiment replication by independent investigators is needed (Munafò et al. 2017).
Limitations
As with any meta-analysis, the information in this report consists of summaries of summaries; thus, the conclusions are limited, and there may be other underlying effects that could be the reason for the large adjunctive effects that were present but we were not able to investigate or were not reported properly.
Conclusion
In this report, studies from the same group of authors seemed to obtain a large effect size of adjuncts to SRP. These results are consistent despite a wide range of both type and different class of adjuncts. Some of these agents are similar to agents tested in other centers, but most are unique and have not been evaluated by other centers and other investigators. The results are not consistent with the studies in the literature and seem to be tested in a similar manner that has been used by other investigators. Before the results of some of these unique agents can be accepted, they need to be tested by other investigators at different centers.
Author Contributions
J.C. Gunsolley, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript; K. Al-Abedalla M. Shaqman, contributed to design and data acquisition, drafted and critically revised the manuscript; E. Ioannidou, contributed to conception, design, and data interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844211039722 – Supplemental material for Unusual Findings in Trials Evaluating Adjuncts to Scaling and Root Planing: Meta-analysis (Part 1)
Supplemental material, sj-docx-1-jct-10.1177_23800844211039722 for Unusual Findings in Trials Evaluating Adjuncts to Scaling and Root Planing: Meta-analysis (Part 1) by J.C. Gunsolley, K. Al-Abedalla, M. Shaqman and E. Ioannidou in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health (NIH)/National Institute of Dental and Craniofacial Research (NIDCR) R34 DE027410 awarded to E. Ioannidou.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.