
Abstract
Introduction:
Older adults are more susceptible to a common respiratory infection: pneumonia. Nearly 1 million older adults per year are hospitalized for community-acquired pneumonia in the United States.
Objective:
To examine whether wearing removable dentures are associated with an increased risk of pneumonia incidence in a geriatric population.
Methods:
We conducted a retrospective cohort study among patients >65 y of age within a large academic health system (University of Rochester Medical Center). The medical and dental electronic records from 2010 to 2018 were reviewed and used for data collection. The exposure was removable denture wearing. The main outcome variables were the incidence of pneumonia and time to event of pneumonia. A Cox proportional hazards regression was used to examine the association between pneumonia onset and wearing removable dentures, adjusting for demographics, socioeconomic status, and medical and dental conditions.
Results:
A total of 2,364 patients were included, with 1,189 (50.29%) in the denture-wearing group and 1,175 (49.70%) in the non–denture wearing group. The annual pneumonia incidence rate per 100,000 persons was 1,191 in the denture-wearing group and 128 per 100,000 persons in the non–denture wearing group, with a crude incidence rate ratio of 9.33 (95% CI, 5.41 to 18.81;
Conclusions:
Wearing removable dentures was found to be a risk predictor for pneumonia incidence among the geriatric population even after accounting for other risk factors.
Knowledge Transfer Statement:
Wearing removable dentures was found to be a risk predictor of pneumonia incidence among older adults. Although the current study does not imply a causal relationship between denture wearing and pneumonia, clinicians and older patients could reference the study results when choosing dental prostheses to restore missing teeth.
Keywords
Introduction
The geriatric population faces significant challenges for systemic and oral health care (Tavares et al. 2014; Hung et al. 2019). Globally, 810 million people are >60 y of age, and this figure is expected to reach 2 billion by 2050 (22% of the entire global population; Fonds des Nations Unies pour la population 2012). Edentulism (tooth loss) is a debilitating and irreversible condition serving as a terminal marker of an ongoing oral and systemic disease process (Friedman and Lamster 2016). Although the prevalence of complete tooth loss has declined over the last decade, edentulism remains a significant oral disease worldwide, especially among older adults (Slade et al. 2014). In the United States, current estimates suggest that nearly 20% of the population wears some form of removable dentures (full or partial, maxillary and/or mandibular); the predicted number of adult populations in need of dentures will be 8.6 million in 2050 (Slade et al. 2014).
Intriguingly, previous studies have indicated a possible association between removable denture wearing and respiratory and pulmonary diseases, including pneumonia. Dentures have been indicated as the potential reservoirs for microorganisms associated with aspiration pneumonia and chronic obstructive pulmonary disease (COPD; Scannapieco 1999). Microorganisms considered respiratory pathogens have been found in the denture base (e.g., Streptococcus pneumonia, Haemophilus influenza, staphylococci, and Candida spp.; Hinuma and Grace 1967; Budtz-Jorgensen 1992, 1994; Smith et al. 2003; Verran 2005). Furthermore, through a cohort study among 453 Japanese older adults in assisted living who wore dentures, Iinuma et al. (2015) showed that overnight denture wearing was associated with a 2.3-fold higher risk of pneumonia incidence. Although the study results suggested a potential association between denture wearing during sleep and increased pneumonia incidents, the results in the Iinuma et al. study cannot be generalized to the independent living geriatric population, given the lack of a non–denture wearing group and the participants being dependent older adults who were ≥85 y old. Understanding the association between denture wearing and pneumonia is vital because pneumonia is one of the most common causes of death in adults aged >65 y (Chong and Street 2008; Brar and Niederman 2011).
Therefore, our study aimed to examine the association between removable denture wearing and pneumonia incidence in the geriatric population through a retrospective cohort study. Our hypothesis was that removable denture wearing is associated with an increased risk of pneumonia incidence in the geriatric population.
Methods
Study Design
This retrospective cohort study comprised patients at the University of Rochester Medical Center (URMC) from 2010 to 2018. The URMC includes entities that provide medical and dental care. The medical and dental records of eligible participants were extracted and used for data collection. This study was approved by the University of Rochester Research Subject Review Board (RSRB00071791). This study followed the STROBE reporting guidelines (Strengthening the Reporting of Observational Studies in Epidemiology).
Participants
The inclusion criteria were as follows. Patients had to have available records in the medical and dental systems during the study observation period (July 1, 2010–July 1, 2018). They also had to be ≥65 y old at end of the study observation period. We used 65 y of age as a cutoff because pneumonia incidence is higher among people ≥65 y old; specifically, one-sixth of pneumonia cases reported yearly occur among individuals ≥65 y old (Torres et al. 2013). Furthermore, patients had to have no history of pneumonia at the baseline of the study. Criteria related to exposures were as follows:
Nonexposure group: without removable denture insertion during the study period (partial or complete, acrylic or cast base, mandible or maxilla)
Exposure group: with removable denture insertion during the study period (partial or complete, acrylic or cast base, mandible or maxilla)
The exclusion criteria were 1) removable dentures prior to the study observation period and 2) severe systemic diseases, such as HIV, lung cancer, and severe immunodeficiency, prior to and during the study period. Patients with these systemic diseases were excluded due to the elevated risk for pneumonia (Sanders et al. 2006; Huang and Crothers 2009).
Study Groups
Study patients were grouped by removable denture insertion (partial or complete) during the study period. The nonexposure group did not have removable denture insertion and was followed for 8 y. The exposure group had removable denture insertion at the URMC Eastman Institute for Oral Health during the study period. These removable dentures were made to replace missing teeth to meet patients’ aesthetic or food-chewing needs. The participants in the exposure group were enrolled into the study on a rolling basis. For instance, 142 participants who had removable denture insertion in 2010 were enrolled in year 1 and followed for 8 y, and 162 participants who had removable denture insertion in 2011 were enrolled in year 2 and followed for 7 y. The participants enrolled in each year are indicated in Figure 1.
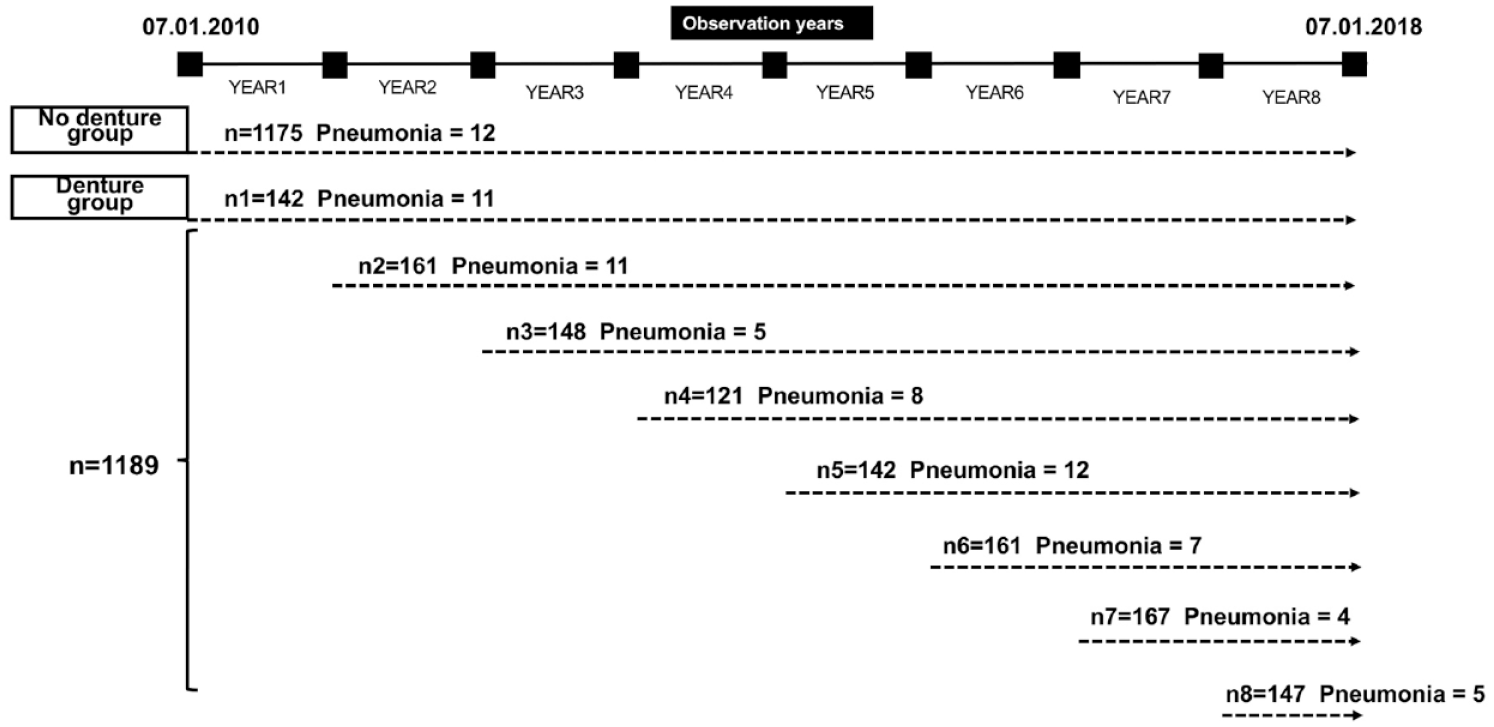
Study design and pneumonia events among each observational group.
The patients of the exposure and nonexposure groups were included on a 1:1 ratio. Specifically, a record of 6,938 patients who were ≥65 y old was initially identified: 1,317 with and 5,621 without removable denture insertion during the study period. Among the 1,317 patients with removable dentures, all patients who met the inclusion and exclusion criteria were enrolled (N = 1,189). Among the 5,621 patients without removable dentures, 4,424 met the inclusion and exclusion criteria, and of these, 1,175 were selected out of a random sequence to keep the 1:1 enrollment ratio with the denture group.
Primary Outcome
The primary outcomes were the incidence of pneumonia and time to event of pneumonia. The diagnosis of pneumonia was made by study patients’ medical care providers and charted in the medical records. The following ICD-10 codes were used for identifying pneumonia events: pneumonia–unspecified organism (J18.9), pneumothorax-unspecified (J93.9), lobar pneumonia–unspecified organism (J18.1), other pneumonia–unspecified organism (J18.8), and pneumonitis due to inhalation of food and vomit (J69.0). The following parameters that reflect pneumonia severity were also extracted: hospitalization, medical department where health care was provided, duration of hospital stays if hospitalized, pneumonia-related death, and second incidence of pneumonia.
Covariates
Other variables obtained from study patients’ medical and dental records included the following:
Demographics: age (continuous data), sex (male/female), race (African American, Caucasian, Asian, others), ethnicity (Hispanic/non-Hispanic), and urban/suburban (indicated by residency zip code)
Oral health conditions: caries related (DMFT [number of decayed, filled, missing teeth]), periodontal (history of scaling and root planning), oral mucosal (history of oral candidiasis), numbers of fixed dental prosthesis (crown and dental implant), dentures types (complete, partial, combination), denture locations (maxillary, mandibular, both), and denture materials (acrylic and cast)
Medical conditions: asthma, chronic kidney disease, COPD, diabetes, stroke, smoking status (not including former smokers), antibiotic use, codeine or narcotics use, blood thinner use, and receipt of pneumococcal vaccine Pneumovax23 and Prenar13
Sample Size Calculation
The annual pneumonia incidence rate is 34 per 1,000 (3.4%) people ≥75 y old (Hoare and Lim 2006). We assume that the incidence is 2% in the nonexposure group (non–denture wearing) and 4% in the exposure group (denture wearing); as such, a sample size of 1,141 patients in each group will achieve 80% power to detect the proposed incidence difference with a significance level of 0.05.
Statistical Analysis
Differences in the demographic, socioeconomic, medical, and dental characteristics between the exposure and nonexposure groups were compared via a chi-square or Fisher’s exact test for categorical data or t test for continuous data. The age of pneumonia onset between groups was compared by a Mann-Whitney U test. To compare the severity of pneumonia between groups, a Mann-Whitney U test was used to compare the duration of hospital stay (days); a chi-square or Fisher’s exact test was used to compare the percentage of hospitalization, the particular medical clinic when patients sought care (e.g., emergency department), percentage of pneumonia-related death, and percentage of second incidence of pneumonia.
To analyze factors associated pneumonia time to event, we first used log-rank tests to preselect factors that indicate a significant difference in time to event between the exposure and nonexposure groups. Second, we used a Cox proportional hazards regression analysis to evaluate the influence of multiple variables on the event time of pneumonia. These variables included factors identified to be significant from log-rank tests and other commonly recognized confounders for pneumonia. Variables that have extremely low cases between the comparison groups were not in the regression analysis—for example, only 1 COPD case was identified among the non–denture wearing group; hence, COPD was not advanced to the regression analysis. The hazard ratio (HR) and 95% CI were calculated to evaluate the influence of denture wearing on pneumonia time. Statistical analysis was conducted through SAS statistics software, version 9.4 (SAS Institute). The significance level was set to 0.05 in the analyses.
Results
Demographic and Medical Background
A total of 2,364 patients were included in the study: 1,189 in the denture group and 1,175 in the nondenture group. The demographic, medical, and dental characteristics of the study patients are shown in the Table. Regarding sex, age distribution, ethnicity, and residency location (urban or suburban), no statistical differences were detected between the groups (P > 0.05). Denture wearers appeared to have more compromised medical conditions when compared with the non–denture wearers—for example, more were current smokers, and more had a history of ischemic stroke, asthma, chronic kidney disease, COPD, and diabetes mellitus (P < 0.001).
Demographic, Medical, and Oral Characteristics of Study Patients.
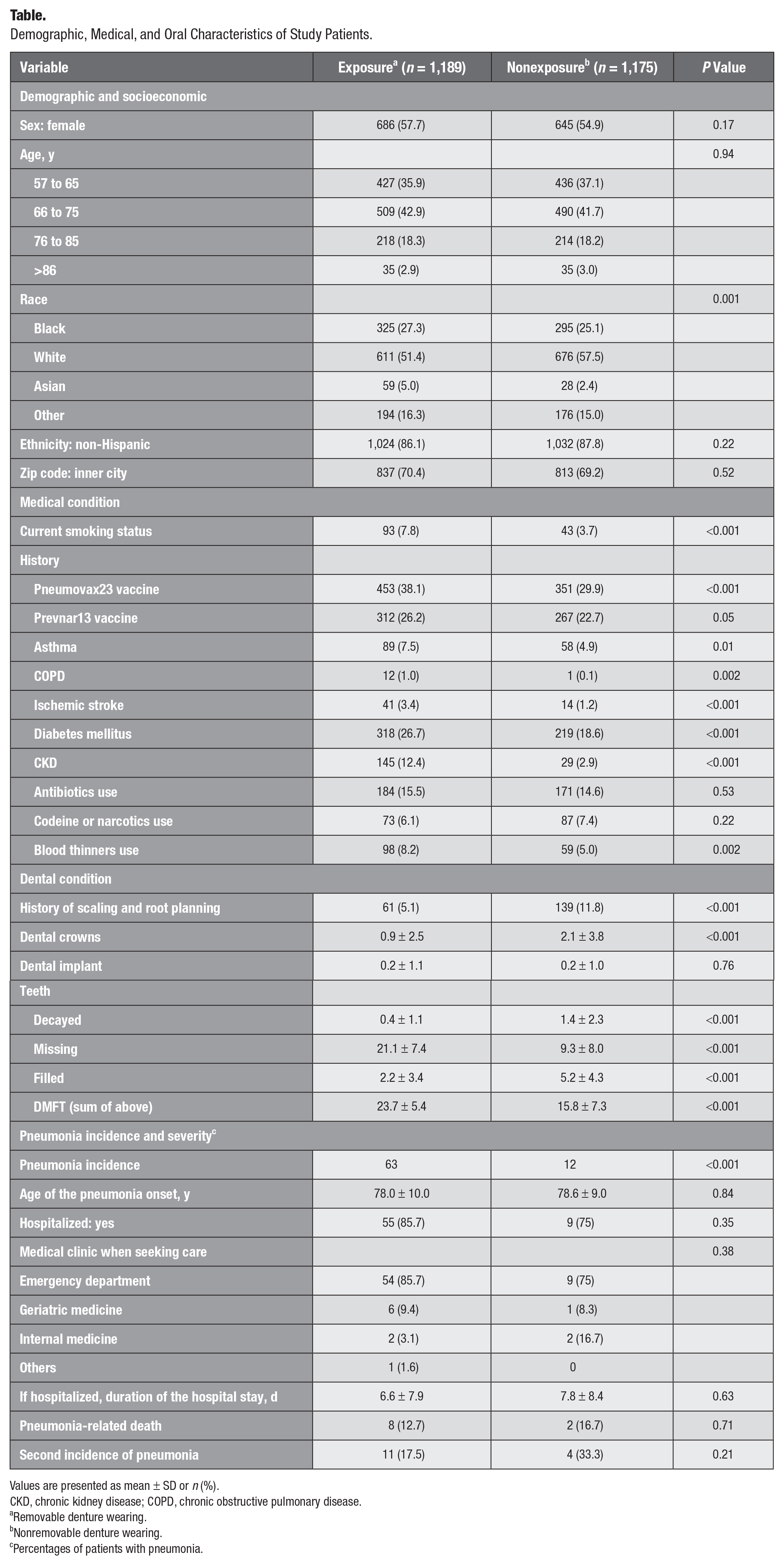
Values are presented as mean ± SD or n (%).
CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease.
Removable denture wearing.
Nonremovable denture wearing.
Percentages of patients with pneumonia.
Oral Conditions and Denture Characteristics
As compared with non–denture wearers, denture wearers had more missing teeth and fewer filled or crowned teeth (P < 0.001). The patients who received scaling and root planning (periodontal treatment) were fewer in the denture-wearing group (5.1%) than in the non–denture wearing group (11.8%, P < 0.001). No difference was detected for dental implant presence (P = 0.76).
The study patients in the denture-wearing group were categorized by denture type (complete, 45.44%; partial, 37.24%; combination, 17.32%), denture location (maxillary, 24.10%; mandibular, 12.05%; both, 63.85%), and denture material (acrylic, 62.43%; cast, 37.57%).
Pneumonia Incidence and Event Severity
During the observational period, 63 pneumonia cases occurred among denture wearers and 12 cases occurred among the non–denture wearers. The annual incidence rate per 100,000 persons was 1,191 in the denture-wearing group and 128 per 100,000 persons in the non–denture wearing group, with a crude incidence rate ratio of 9.33 (95% CI, 5.41 to 18.81; P < 0.0001). The pneumonia cases in each group are indicated in Figure 1. The difference in the years to pneumonia onset was significant between the groups (P < 0.001; mean ± SD): 2.02 ± 2.00 y from denture insertion to pneumonia onset among denture wearers and 4.83 ± 2.17 y from the beginning of the study to pneumonia onset among the non–denture wearers. Significantly, among the 63 pneumonia events in the denture-wearing group, 38 occurred in the first year of denture insertion and 6 within the first 2 y of denture insertion, whereas among the 12 events in the nondenture group, only 1 patient developed pneumonia within the first 2 y. The mean age of pneumonia onset of the denture wearers and non–denture wearers was 78.0 ± 10.0 and 78.6 ± 9.0 y, respectively (P = 0.84).
None of the parameters reflecting pneumonia severity were significantly different between the groups (P > 0.05; Table). Notably, pneumonia-related death occurred among 12.7% and 16.7% of the exposure and nonexposure participants (P = 0.65). The second incidence of pneumonia occurred among 17.5% and 33.3% of the exposure and nonexposure participants (P = 0.24).
Survival Estimation of the Factors Associated with Pneumonia Event Time
From log-rank tests, we identified individual variables that were associated with increased or lowered pneumonia incidence. We plotted the survival curve to visualize their impact. The model estimated that approximately 98.3% of the study patients would remain free of pneumonia by year 8. The 8-y survival was lower among non-Hispanic patients (98.0%; Fig. 2A), older patients (Fig. 2B), and patients with diabetes mellitus (97.9%; Fig. 2C). Intriguingly, the 8-y survival among denture wearers was 95.8%, significantly lower than the survival of non–denture wearers (99.3%; Fig. 2D).
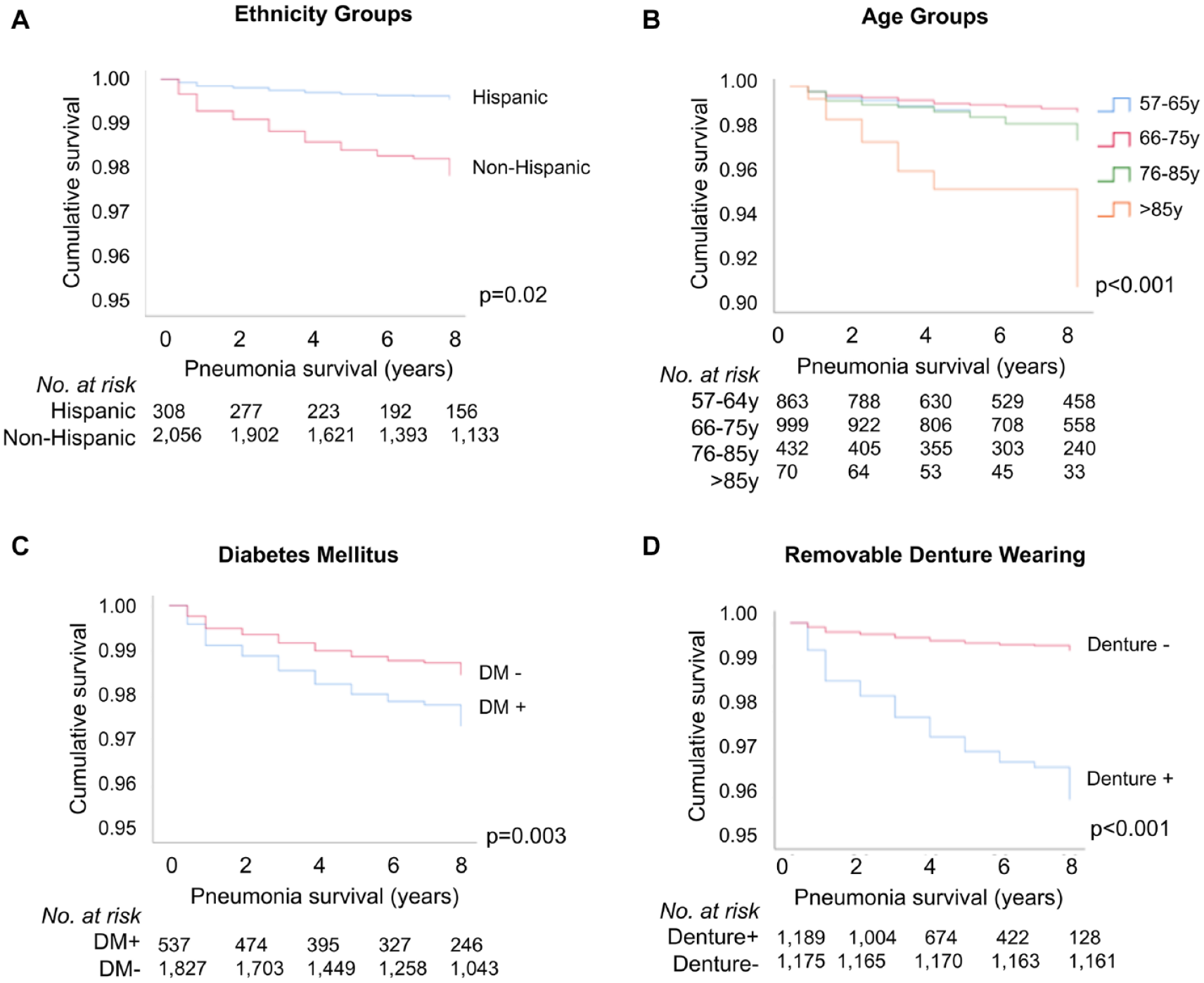
Pneumonia event time probability estimation: (
Second, we used a Cox regression analysis to provide an effect estimate by quantifying the difference in survival between patient groups and adjusted for confounding effects of variables (see Fig. 3). The risk of developing pneumonia was positively associated (P < 0.05) with removable denture wearing (HR, 7.68; 95% CI, 3.91 to 15.08), patient age (76 to 85 y vs 57 to 65 y: HR, 1.86 [95% CI, 1.01 to 3.44]; >85 y vs 57 to 65 y: HR, 5.43 [95% CI, 2.49 to 11.85]), and diabetes mellitus (HR, 1.89; 95% CI, 1.17 to 3.06) and negatively associated with ethnicity (Hispanic vs. non-Hispanic: HR, 0.23; 95% CI, 0.06 to 0.86).
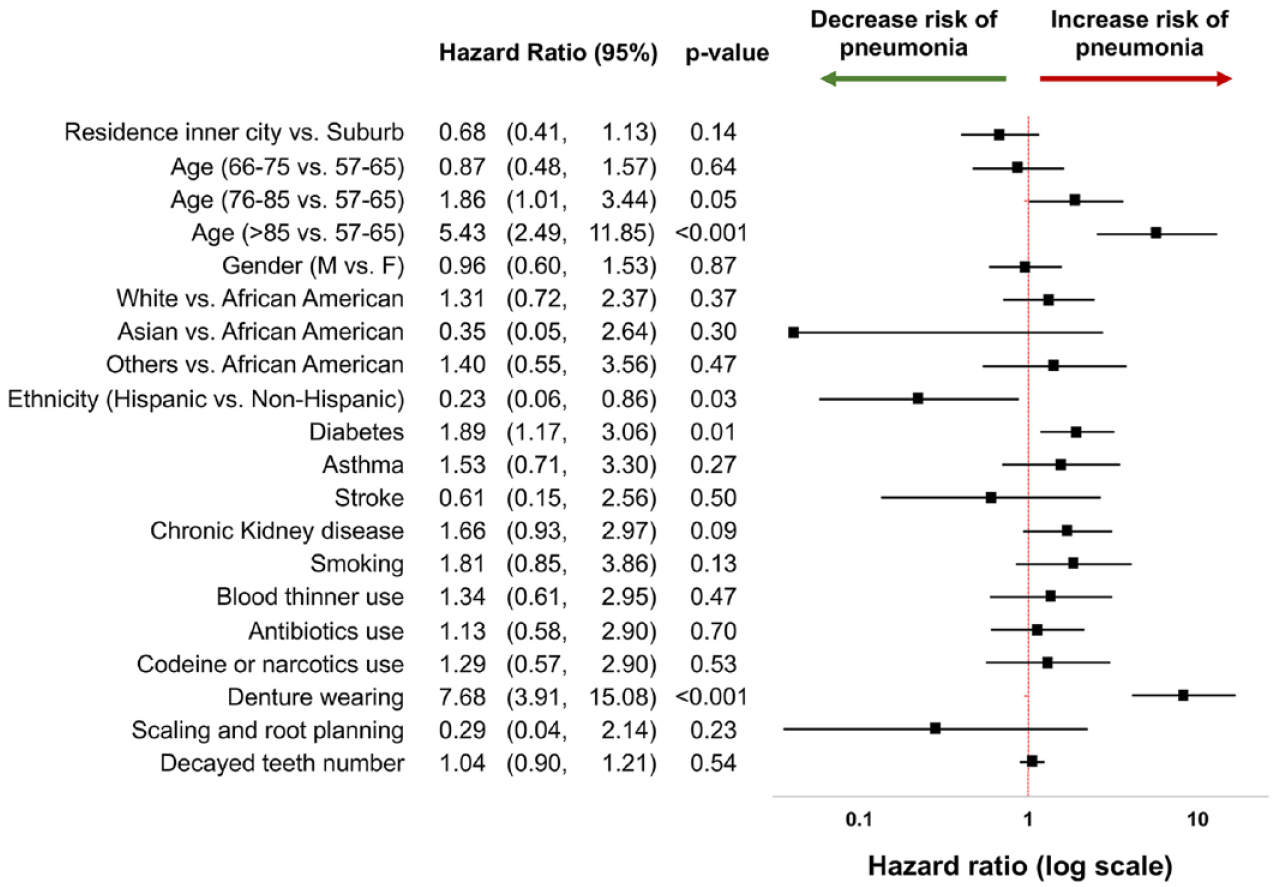
Forest plots for hazard ratio of pneumonia time to event among older adults. A Cox regression analysis was used to examine the factors that were associated with the pneumonia event time in the study population. Our study results indicate that several factors were associated with a higher risk of pneumonia incidence, which could be used as risk indicators for the incidence of pneumonia in the geriatric population.
Interaction between Age and Denture Wearing in Pneumonia Event Time
We examined the interactive effect of age and denture wearing on pneumonia survival. The survival difference between denture wearers and non–denture wearers was augmented as patients became older (Fig. 4). The 8-y survival between denture wearers and non–denture wearers in the age group 57 to 65 y was 96.5% and 99.4%, with a 2.7% difference (P < 0.001; Fig. 4A). However, the difference significantly increased to 77.0% versus 96.0% between denture wearers and non–denture wearers among those >86 y old, with a 19% difference (P = 0.001; Fig. 4D).
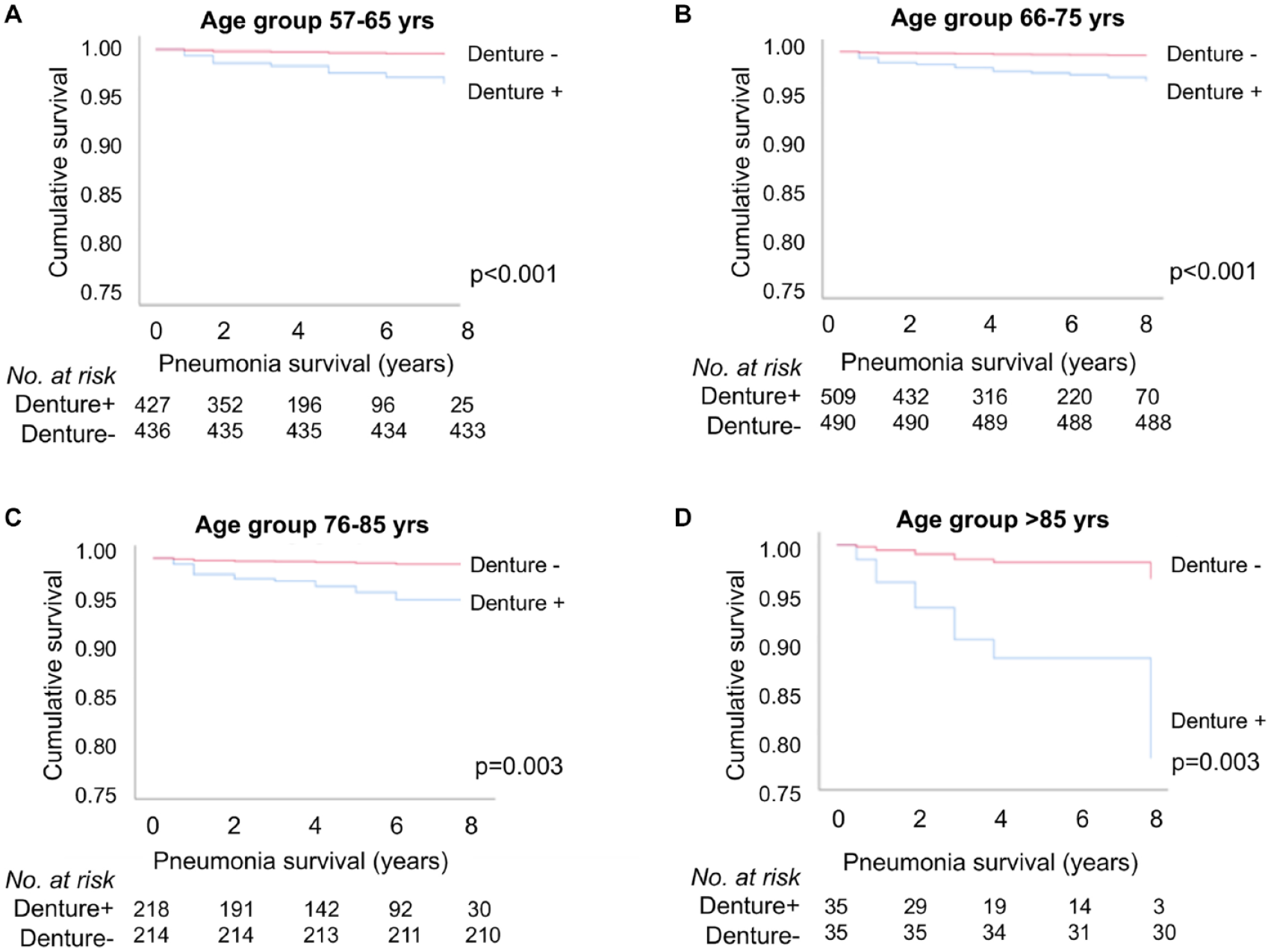
Pneumonia survival for denture wearers stratified by age groups. The survival difference between denture wearers and non–denture wearers was augmented as patients got older. (
Discussion
In the United States, community-acquired pneumonia afflicts approximately 5.6 million people per year and is the sixth-leading cause of death (Graves 1992; Niederman 2009). More significant, >90% of pneumonia-related deaths occur in individuals ≥65 y old (Brar and Niederman 2011; Chong and Street 2008). The commonly known risk factors for pneumonia are age, alcoholism, asthma, immunosuppression, heart disease, and institutionalization (Rothan-Tondeur et al. 2003; Bohl et al. 2017). Our study revealed a novel finding that the risk of developing pneumonia was 6 times higher in the patients who wore removable dentures (exposure group) as compared with those who did not have a history of removable denture wearing (nonexposure group). This study is novel for the following ways: 1) assessment of the association between denture wearing and a critical medical disease, pneumonia, among the independent living geriatric population and 2) 8-y longitudinal assessment of a relatively large geriatric cohort.
Several pathways are speculated to link denture wearing and incidence of pneumonia. First, dentures may act as a reservoir for respiratory and systemic opportunistic pathogens (Sumi et al. 2003; Sumi et al. 2007; O’Donnell et al. 2016) and harbor a niche for antibiotic-resistant bacteria (Smith et al. 2003; Kerver et al. 2013). The removable denture base (acrylic) favors the accumulation of plaque/biofilm, a complex polymicrobial consortium of bacteria and yeasts. It is reported that with the inflammatory serum released due to mucosal irritation among denture wearers, a more diverse microbial community with the predominance of fastidious anaerobes was found in the denture base when compared with dental plaques accumulated on the teeth (Wade et al. 1997; Wilson et al. 1997; Nikawa et al. 1998; Kazor et al. 2003). Continuous swallowing or aspiration of the microorganisms accumulated on the denture base may predispose the denture wearers to risks of infections, such as respiratory infection and pneumonia.
Second, improper handling of denture hygiene might introduce a pathway of infections. For example, when dentures are not in use, some denture users may leave their dentures in a nonhygienic environment. This practice might lead to their contamination with pathogenic microorganisms that do not belong to the normal oral flora. Moreover, it is suggested that hospitalized and institutionalized older adult denture wearers may be at increased risk of cross-contamination when health care workers are handling the dentures without adequate hygiene measures (Sumi et al. 2003).
The evidence is scant that supports the positive association between diabetes mellitus and increased pulmonary diseases (e.g., pneumonia; Koziel and Koziel 1995; Falguera et al. 2005). Although an increased prevalence of pneumonia-related hospitalizations has been observed in diabetic aging Western populations (Fry et al. 2005; Thomsen et al. 2006), the clinical course leading to the comorbidity (pneumonia) is not well understood. Underlying biological mechanisms may include decreased leukocyte function and harmful effects of hyperglycemia (Koziel and Koziel 1995; Fine et al. 1997; McAlister et al. 2005). Hyperglycemia could cause intra- and extracellular dehydration, electrolyte abnormalities, and depressed immunity (Umpierrez et al. 2002). Furthermore, impaired lung function and pulmonary microangiopathy have been observed among diabetic patients (Koziel and Koziel 1995).
Worth noting, variables that significantly deviate from commonly published data by professional organizations were not in the regression analysis. Notably, the percentage of patients in our study who received a pneumococcal vaccine (22.7% to 38.1%) was significantly lower than the national data, where the Centers for Disease Control and Prevention reported that 64.8% to 76.3% of adults aged ≥65 y old have received a pneumococcal vaccine (Kramarow 2020). The reasoning could be that individuals often receive pneumococcal vaccination at pharmacies instead of medical offices, which could contribute to the incomplete data collection regarding our study patients’ pneumococcal vaccination status. Hence, pneumococcal vaccination was not in the regression analysis.
Limitations
The following limitations should be considered when interpreting the study results.
Since this retrospective cohort study involved only medical and dental record review, we were not able to collect data regarding the confirmation of dental-wearing status, denture quality (denture fitting and retention), denture hygiene, and microorganisms present in the oral cavity of the study patients or on the denture base. Therefore, we are unable to make definite speculation of the exact role of denture wearing in the elevated pneumonia risk.
In addition, a high pneumonia incidence rate in the denture-wearing group may be due to an unclean oral condition rather than a denture-wearing condition. Due to the nature of the retrospective cohort, we extracted dental/oral data from the existing dental records. Since the cleanliness of the oral cavity has not been a standardized parameter that would be routinely collected during dental visits, we were not able to collect and assess related information. Therefore, missing data on the cleanliness of the oral cavity could lead to an overestimated risk of denture wearing and pneumonia incidence. A future prospective study should incorporate this critical factor into data analysis.
The data collected on medical conditions were measured as binary variables; hence, the severity of those conditions was not taken into account to measure the confounding effects.
The study results cannot be generalized to populations residing outside of the Rochester, New York, area. Rochester is the third-most populous city in New York State. The URMC is 1 of the 2 leading comprehensive care providers for Rochester residents holding private and state-supported medical insurance. The patient population that visits the URMC is made up of approximately 40% African American, 40% Caucasian, and 20% other.
Since we had access to just the medical and dental information from the electronic record in 1 academic institute, study patients might have seen medical or dental providers outside the electronic system that we accessed. The study results might under- or overestimate the associations observed. For instance, we might overestimate the association observed under the circumstance that more patients in the nondenture groups had obtained dentures from outside dentists. In contrast, under the condition that more of the denture group’s pneumonia events occurred at outside medical facilities when compared with the nondenture group, we might underestimate the association between denture wearing and pneumonia incidence.
With these recognized limitations, future studies assessing the role of removable denture wearing in respiratory health among a geriatric population should consider a prospective cohort study design. Specifically, parameters that relate to denture type (complete or partial), denture base material, denture quality, microorganism carriage, and study patients’ oral health status should be carefully examined to elucidate the underlying mechanisms and identify potential strategies for prevention. Furthermore, individuals who report cleaning their dentures daily experience lower rates of pneumonia than those who do not clean their dentures regularly (Kusama et al. 2019). Current commercially available denture-cleaning tablets aim to reduce bacterial counts but not target other microorganisms, such as Candida species (Duyck et al. 2016), which are commonly detected in denture bases and considered pneumonia pathogens. Future studies that examine the antifungal efficacy of denture cleansers warrant attention.
Conclusions
Although findings suggest that wearing removable dentures can increase pneumonia risk among geriatric patients, studies are warranted to discern the role of denture-related microbiological mechanisms and that of unrelated comorbidities.
Author Contributions
H. Alzamil, J. Xiao, contributed to conception, design, data acquisition, analysis and interpretation, drafted and critically revised the manuscript; T.T. Wu, contributed to data acquisition, analysis and interpretation, drafted and critically revised the manuscript; E. van Wijngaarden, M. Mendoza, H. Malmstrom, K. Fiscella, D.T. Kopycka-Kedzierawski, R.J. Billings, contributed to data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J. Xiao’s work is supported by grant from the National Institutes of Health, National Institute of Dental and Craniofacial Research (K23DE027412). T.T. Wu’s work is supported by grant from the National Science Foundation (NSF-CCF-1934962).