
Abstract
Purpose:
The aim of this 2-arm, parallel-group, 12-mo randomized clinical trial was to compare the effectiveness of semiannual application of 38% silver diamine fluoride (SDF) versus restorative treatment (RT) to manage cavitated caries lesions in primary teeth in a diverse population of children in Michigan.
Methods:
Children aged 2 to 10 y with at least 1 soft cavitated lesion (International Caries Detection and Assessment System 5 or 6) with no pain or signs/symptoms of irreversible pulpitis were recruited and randomly assigned to 2 intervention groups. One random lesion per child received 38% SDF (twice, at a 6-mo interval) or RT. All interventions and assessments were done by calibrated dentists. Primary outcome measures were clinical failure rates: minor (e.g., reversible pulpitis, active/soft lesion or progression, restoration loss or need for replacement/repair, secondary caries) and major (e.g., irreversible pulpitis, abscess, extraction). Parent, child, and provider acceptability was also assessed.
Results:
Ninety-eight children were enrolled and randomized, with a mean (SD) age of 4.8 y (1.8); 46% were female and their mean dmft + DMFT was 6.3 (3.9). Sixty-nine children were assessed at 12 mo (sample was within the planned 30% attrition rate). There were significantly more teeth with minor failures (SDF = 65%, RT = 23%, P ≤ 0.001) and major failures (SDF = 13%, RT = 3%, P ≤ 0.001) in the SDF group than the RT group; 74% of SDF-treated lesions were hard at 12 mo vs. 57% at 6 mo. Providers stated that SDF was easier, faster, and more preferable than RT (P ≤ 0.001). No significant differences were found in parental satisfaction and acceptability. At 12 mo, children in the RT arm felt significantly (P < 0.05) happier with their tooth appearance and stated that their visit to the dentist hurt less.
Conclusion:
At 12 mo, SDF-treated lesions had significantly more minor and major failures than RT, suggesting that SDF-treated teeth need to be closely monitored in a population at high caries risk (ClinicalTrials.gov NCT02601833).
Knowledge of Transfer Statement:
The results of this study can be used by clinicians when deciding whether to restore or apply silver diamine fluoride to cavitated lesions in primary teeth. Information on treatment outcomes and parent, child, and provider acceptability can help guide appropriate treatment decisions and need for monitoring.
Introduction
Dental caries is one of the most prevalent chronic diseases among children worldwide (Kassebaum et al. 2015). There are profound disparities in caries experience, with children from low socioeconomic and minority groups experiencing significantly higher disease rates (Dye et al. 2015). There are also issues related to access to preventive services and care (US Centers for Medicare and Medicaid Services 2020). The current standard of care for management of cavitated carious lesions is focused on restorations or extractions. Many young children who need extensive treatment, are uncooperative, or have immature cognitive functioning, disabilities, or medical conditions are treated under general anesthesia (American Academy of Pediatric Dentistry 2016; Schroth et al. 2016). Cavitated carious lesions that go untreated may lead to adverse outcomes associated with nutritional intake, sleep, daily activities, self-esteem, pain, infection, and quality of life (Crystal et al. 2017; Crystal and Niederman 2019; Singh et al. 2020).
When caries lesions cavitate and need to be restored, many effective options are available, including conservative strategies requiring no or selective caries removal (Santamaría et al. 2020). If placing a restoration is not possible due to behavioral, economic, or access-to-care issues or when there is a desire for a less invasive intervention, lesions can be arrested by making them self-cleansable with good access to brushing with fluoride toothpaste (van Strijp and van Loveren 2018) or controlled with use of products such as 38% silver diamine fluoride (SDF), an effective alternative to arrest lesions in the primary dentition (Crystal et al. 2017; Slayton et al. 2018; Urquhart et al. 2019; Seifo et al. 2019). In 2014, 38% SDF was introduced into the United States as a medical device to treat hypersensitivity. As SDF is an alternative to restorative intervention, it would be helpful to understand how these interventions compare in terms of clinical outcomes and patient and provider acceptability to aid in guiding clinical decision making. At the time, there were no randomized clinical trials (RCTs) comparing SDF and restoration in the treatment of cavitated lesions among young children in terms of clinical failure outcomes, pain, and acceptability. Therefore, the purpose of this RCT was to compare the short-term (1 y) effectiveness of semiannual application of 38% SDF in primary teeth with restorative treatment (RT) while assessing provider, parent, and patient acceptability.
Materials and Methods
This study was approved by the institutional review boards at the University of Michigan and Mott Children’s Health Center and registered in ClinicalTrials.gov (NCT02601833; November 2015). Written consent was obtained from the parent/legal guardian of each child. Recruitment spanned from 2016 to 2019. The last examination was in September 2020.
Trial Design
This 2-arm, parallel-group, 12-mo RCT was conducted in 98 children aged 2 to 10 y with at least 1 active/soft caries lesion into dentin in a primary tooth, scored 5 or 6 by ICDAS criteria (International Caries Detection and Assessment System 2020). These scores were chosen as SDF trials have included lesions with exposed dentin to allow for application of SDF and assessment of dentin hardness (i.e., the equivalent of ICDAS 5 and 6). Active patients of Mott Children’s Health Center and the University of Michigan School of Dentistry were invited to participate. Only 1 randomly selected tooth per child was included. Caries lesions were on teeth with at least one-third of the crown remaining, no pulpal exposure, anticipated exfoliation >12 mo, and no spontaneous or elicited pain or signs of periapical infection. Children were excluded if they were wards of the state or they had hereditary enamel/dentin developmental defects, known allergy to heavy metals or restorative materials, or medical conditions that would prevent treatment in the dental clinics.
Once enrolled, participants were randomly allocated (1:1) to 1 of 2 treatment groups in blocks of 4 per a random number generator. The study statistician stratified randomization by site. Envelopes provided by the statistician with the randomized treatment order were prepared by the study manager and located at each clinical site for use. There were 4 in-person clinical visits: baseline and 3, 6, and 12 mo. To enhance retention and check for adverse events, intermediate phone calls took place at 1, 2, 4.5, and 9 mo. Clinical examinations took place by trained and calibrated dentists with an explorer, dental mirror, air, and light.
Study dentists were pediatric dental residents at the Mott Children’s Health Center and University of Michigan School of Dentistry, who were recalibrated yearly. Over the study period, 15 dentists were calibrated, with 5 responsible for the majority of data collection. Calibration included assessment of ICDAS scoring, dentin color, and dentin texture. Acceptable intra- and interexaminer reliability (vs. a senior examiner; M.F.) was assessed as kappa = 0.7. Further training consisted of assessment of dmft/DMFT scores, plaque removal from the lesion site, major and minor failure criteria (Table 1), radiographic and questionnaire data, and SDF use. Study dentists were also responsible for providing the interventions (SDF and RT).
Major and Minor Failure Criteria: Primary Study Outcomes.
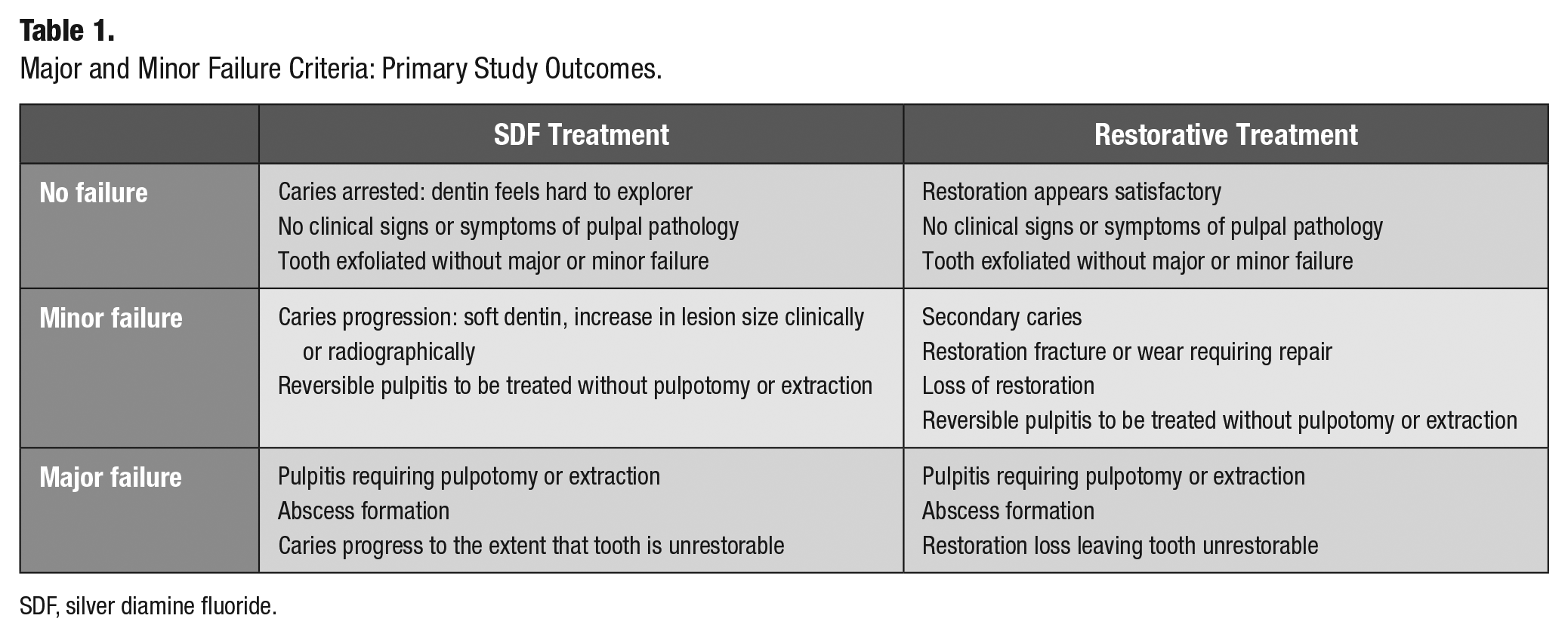
SDF, silver diamine fluoride.
Lesions were initially assessed by severity (ICDAS score), dentin color (yellow, brown, black), periapical radiograph depth (outer, middle, or inner third of dentin), and dentin texture (soft, hard). For lesion and restoration assessment, teeth were cleaned with a toothbrush, dried with air, and assessed visually without magnification by using light and an explorer. Soft dentin was defined as any explorer penetration with light force (Chu et al. 2002). Time to complete the treatment was recorded, including any behavior management.
Primary outcome measures assessed at each follow-up visit were clinical failure rates: minor and major (Table 1; Santamaría et al. 2014). Patients in both arms were evaluated at each visit for caries experience based on dmft + DFMT scores: teeth with cavitated lesions (ICDAS, 3 to 6) and teeth that were missing or filled due to caries. Periapical and bitewing radiographs were obtained at 6 and 12 mo to monitor for failures, with additional radiographs when clinically necessary. Pulpal status was assessed at all visits by asking about symptoms of pain and evaluating signs or symptoms of irreversible pulpitis.
At each in-person visit, parents completed questionnaires about their child’s demographics, diet and oral hygiene habits, experience and access to dental care, pain (Versloot et al. 2006), and parental acceptance and satisfaction with study treatment (Innes et al. 2013). Child participants were assessed with the Wong-Baker scale (Wong and Baker 1988) to determine how they felt about how their teeth look (very happy/not happy or sad/very sad), how their teeth feel (they feel great, sometimes they hurt, they hurt always), how their visit to the dentist was (easy/some easy and some hard/hard), and how their visit to the dentist felt (didn’t hurt at all, hurt a little, hurt a lot).
Treatment Procedures
Restorative Treatment
Local anesthesia and behavior guidance were used as needed. The study tooth received RT, with level of caries removal and type of material used selected per the case following current RT guidelines (e.g., American Academy of Pediatric Dentistry 2018).
38% SDF Treatment
The study carious lesion was treated with 38% SDF (Advantage Arrest; Elevate Oral Care) at baseline and 6 mo. The selected tooth was isolated and dried, and SDF was applied on the entire carious dentin. Excess was blotted dry to prevent unnecessary swallowing.
At every visit participants were given 1) dietary advice to decrease the frequency and amount of sugar-containing snacks and drinks, particularly in between meals and at bedtime, 2) age-specific toothbrushing instructions and fluoride toothpaste recommendations, and 3) fluoride varnish applications (biannually).
Sample Size Calculation
A power analysis was completed with nQuery (GraphPad Software; DBA Statistical Solutions) to determine sample size. Calculations were based on a 2-tailed test, α = 0.05, and β = 0.20, with estimated 12-mo failure rates (minor + major; primary study outcome) of 29% for RT (Santamaría et al. 2014; the authors used the same major and minor failure criteria for RT) and 63% for SDF (37% arrest rate). This estimate was based on 1 of the minor failure criteria for which there are data (lesions not arrested), given that inclusion of children younger than those seen in most trials at the time could lead to higher failure rates due to technique difficulties, as in a recent study (Mabangkhru et al. 2020). The resulting sample size was 98 with an attrition rate of 30%.
Statistical Analyses
Data were managed via REDCap (Research Electronic Data Capture). Data sets were exported and analyzed with SAS version 9.4 (SAS Institute). Chi-square tests or Fisher’s exact tests were used for comparisons between the groups for categorical variables such as sex, brushing habits, satisfaction, and minor and major failures. Wilcoxon rank sum tests were used for comparisons between the groups for age and dmft + DMFT. To impute missing data in the intention-to-treat analyses of failure outcomes, a simulation-based imputation of missing data was used for the 12-mo failure outcomes. The imputation used slightly higher failure rates for the dropouts than those observed within the 2 groups (SDF = 15% major failure, 70% minor failure, 15% nonfailure; RT = 5% major failure, 15% minor failure, 80% nonfailure) and was performed to create 10,000 imputed data sets. Results for 12-mo failure outcomes are also presented with a simple carry forward of the missing data. Several risk factors (position of tooth in arch, type of surface treated, radiographic lesion depth, dmft + DMFT, and oral hygiene habits) were evaluated separately for association with failure via logistic regression, with the study arm as a covariate. The significance level was set at 5% for all tests.
Results
Baseline Sociodemographics
An overall 111 children were screened: 13 were screen failures and 98 were enrolled, randomized, and treated (RT = 42, SDF = 56; for CONSORT diagram, see Figure). For a portion of the study period, 13 participants were randomized before treatment was provided, due to a gap between the initial screening and the baseline visit, resulting in conditions changing and lesions not being eligible. Thus, as they were ineligible before treatment was provided, they were considered not enrolled in the study and were not in any analyses. Because the participants had been randomized, their randomization IDs could not be reused.
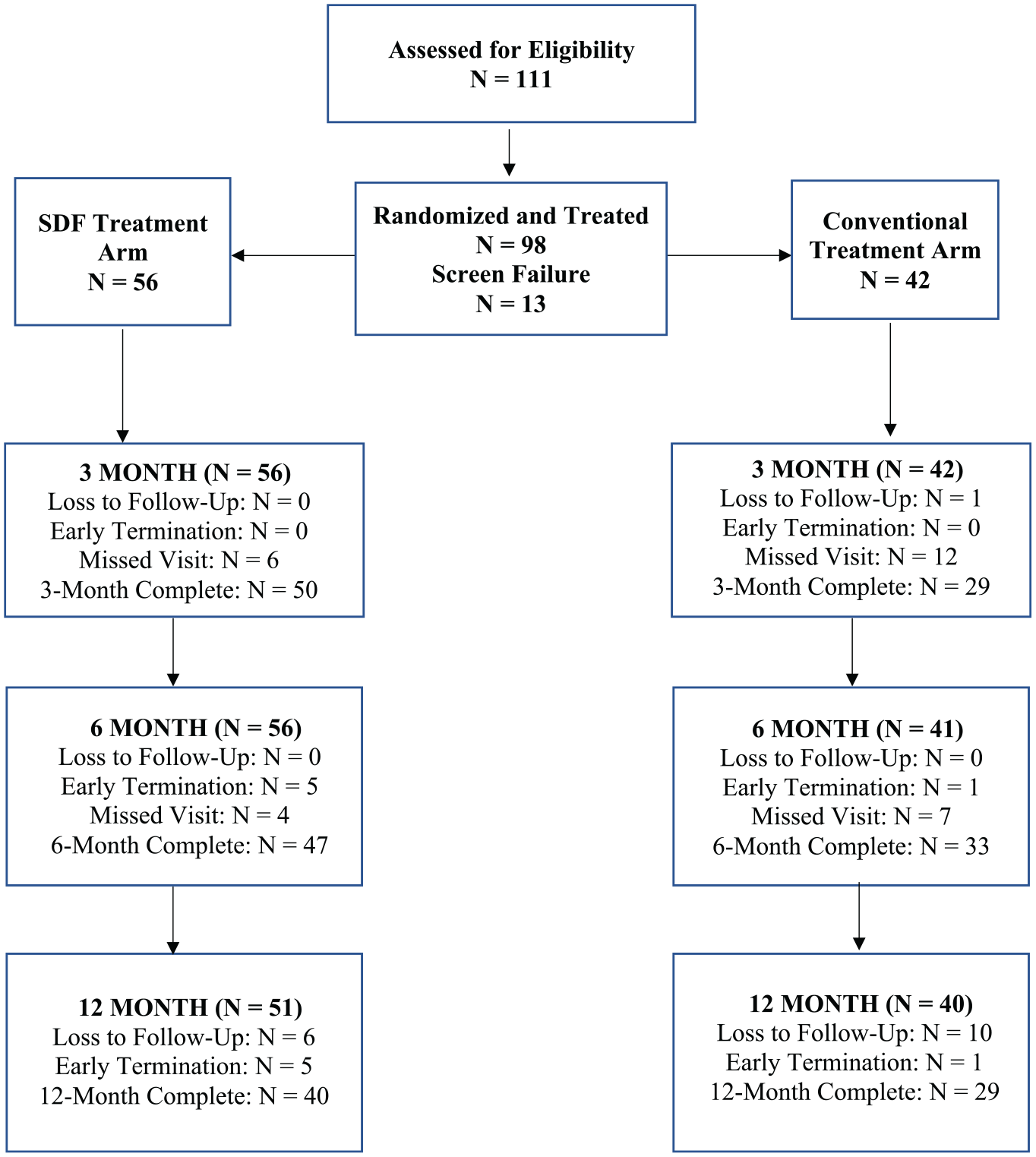
CONSORT flow diagram of children’s progress over 12 mo in the trial. SDF, silver diamine fluoride.
Forty-five participants were female (46%) and 53 were male (54%). The mean (SD) age was 4.8 y (1.8). A variety of races/ethnicities were represented. There were no significant differences(P < 0.05) between the groups for age, sex, or race/ethnicity distribution at baseline (Table 2).
Children’s Sociodemographics, Diet, Oral Hygiene, and Pain.
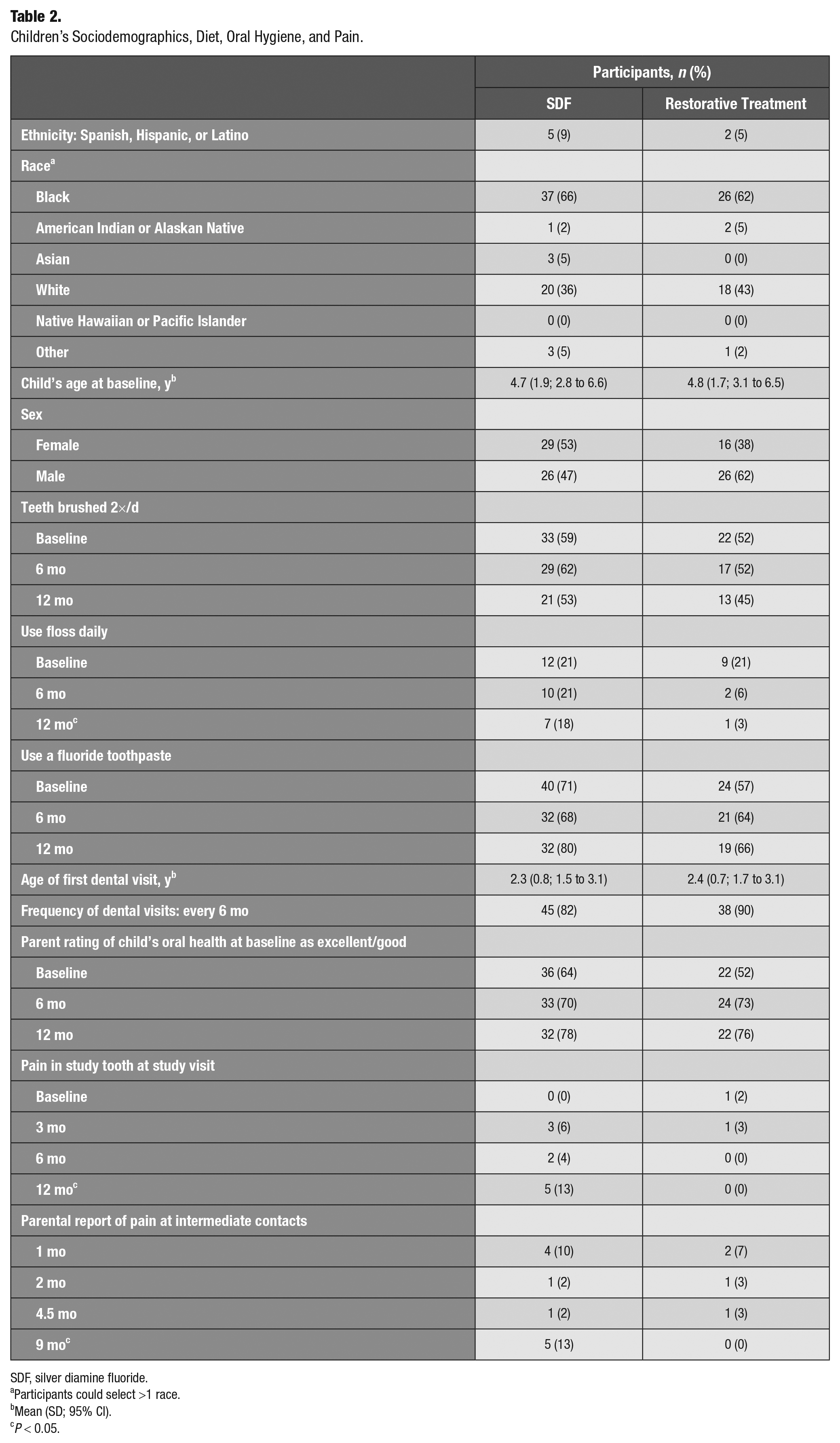
SDF, silver diamine fluoride.
Participants could select >1 race.
Mean (SD; 95% CI).
P < 0.05.
Follow-up
Sixty-nine children (70%) completed the 12-mo visit (SDF = 40, RT = 29; Figure). Twelve participants were terminated early (lesion progressed = 7, tooth developed another lesion = 1, moved = 3, no time = 1), and 17 were lost-to-follow up. Participants lost to follow-up were not significantly different (P > 0.2) than those who completed the trial in terms of baseline characteristics; however, they were more common within the RT group (P < 0.001; odds ratio, 7.9). Trial visits were paused between March and August 2020 due to COVID-19, with 9 participants affected: missed 12 mo (2 in RT), 12 mo out of window (4 in SDF and 2 in RT), and 6 mo out of window (1 in SDF).
Clinical Data
There was a significant difference in minor failures between the arms at 3 mo (P < 0.001), 6 mo (P < 0.001), and 12 mo (P < 0.001), with the SDF arm experiencing more minor failures (Table 3). The SDF arm also experienced significantly more major failures at 12 mo (P < 0.001). Of the 6 major failures in the SDF group, 2 (33.3%) were due to radiographic signs of periapical infections; 1 (16.7%) was at first a minor failure (pain due to reversible pulpitis), which progressed to a radiographic sign of periapical infection and extraction; 1 (16.7%) was a tooth extraction; 1 was a minor failure (lesion progression) that became an extraction; and 1 (16.7%) was a minor failure first (pain due to reversible pulpitis) and then a radiographic sign of periapical infection. Of the 36 minor failures in the SDF group, 25 (69.4%) were due to lesions being active/soft; 7 (19.4%) were due to lesions being active/soft and showing progression; 3 (8.3%) were signs of progression yet lesions were hard; and 1 (2.8%) was pain due to reversible pulpitis yet the lesion was hard. Of the 3 minor failures in the RT group, 1 (33.3%) was due to a missing restoration; 1 (33.3%) was due to reversible pulpitis; and 1 (33.3%) was due to secondary caries and lesion progression.
Treatment Success and Minor and Major Failures throughout the 12-mo Trial Period.
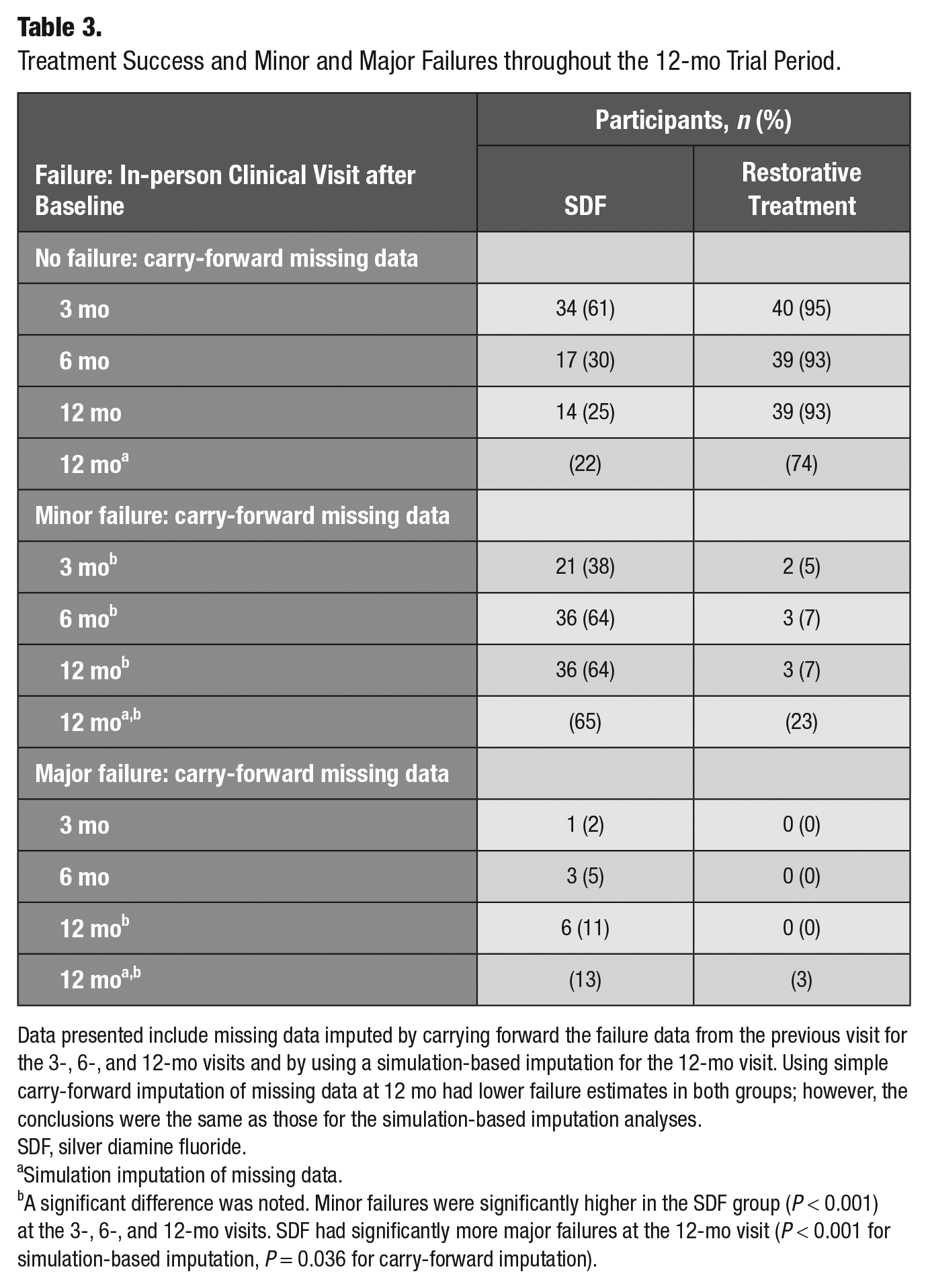
Data presented include missing data imputed by carrying forward the failure data from the previous visit for the 3-, 6-, and 12-mo visits and by using a simulation-based imputation for the 12-mo visit. Using simple carry-forward imputation of missing data at 12 mo had lower failure estimates in both groups; however, the conclusions were the same as those for the simulation-based imputation analyses.
SDF, silver diamine fluoride.
Simulation imputation of missing data.
A significant difference was noted. Minor failures were significantly higher in the SDF group (P < 0.001) at the 3-, 6-, and 12-mo visits. SDF had significantly more major failures at the 12-mo visit (P < 0.001 for simulation-based imputation, P = 0.036 for carry-forward imputation).
At baseline the mean (SD) dmft + DMFT score was 6.3 (3.9). There was a significant difference in scores between groups at baseline (P = 0.034) and 6 mo (P = 0.042), but these differences were not statistically significant at 3 and 12 mo (Table 4). Caries experience was not significantly associated with development of failures (P = 0.22). There was no significant difference in the baseline lesion radiographic depth between treatments, and this was not significantly associated with development of failures (P = 0.44).
Children’s Caries Experience and Lesion Characteristics.
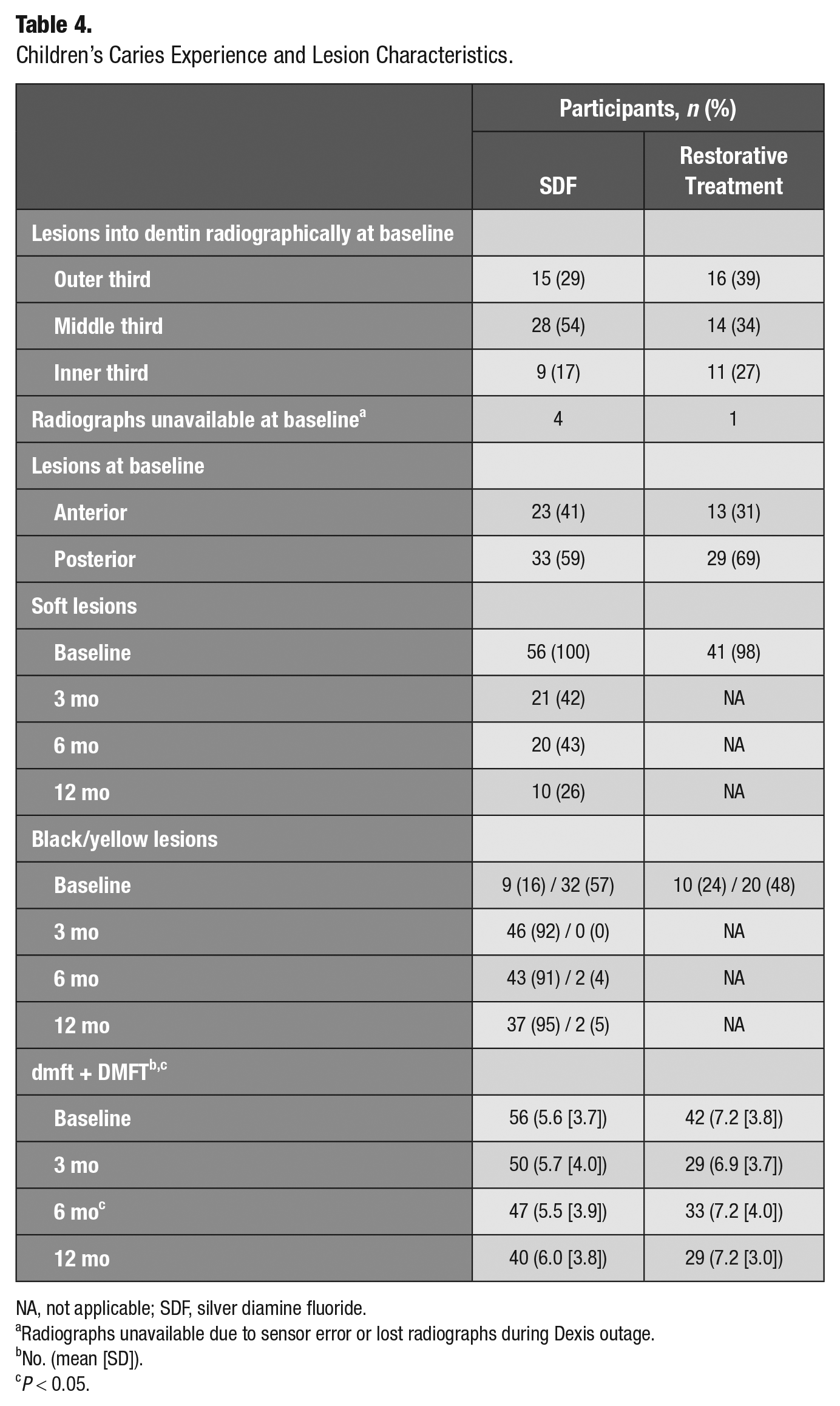
NA, not applicable; SDF, silver diamine fluoride.
Radiographs unavailable due to sensor error or lost radiographs during Dexis outage.
No. (mean [SD]).
P < 0.05.
Of the 98 study lesions at baseline, 62 (63.3%) were on primary molars, 21 (21.4%) on primary canines, and 15 (15.3%) on primary incisors. There was no significant difference between the arms regarding tooth surfaces treated (P = 0.39) or position of tooth in the arch (anterior vs. posterior, P = 0.31; Table 4) and between these variables and development of a failure (P = 0.08). There was no significant difference in lesion color between the groups at baseline (P = 0.56), with the majority of lesions being yellow. At follow-up, the majority of lesions in the SDF arm were black (Table 4).
Plaque removal at the lesion site was evaluated at each visit. There was a significant difference between the arms at 3 mo (P = 0.002) and 6 mo (P = 0.004), with the SDF arm having significantly more visible plaque (i.e., poorer plaque removal) than the RT arm. There was no significant difference at 12 mo (P = 0.14). Plaque removal was not significantly associated with development of failures (P = 0.10).
Oral Hygiene and Dietary Habits
At baseline, there were no significant differences (P = 0.45) in a child’s frequency of dental visits, with every 6 mo being most frequent. There were no significant differences in parental rating of child’s oral health at baseline (P = 0.37), 6 mo (P = 0.90), and 12 mo (P = 0.88; Table 2), with ratings improving over time (P < 0.05). Rating of child’s oral health was not significantly associated with development of failures (P = 0.09).
No significant difference (P < 0.05) in oral hygiene habits was found between treatments at any visit (Table 2), and these were not significantly associated (P > 0.15) with development of failures. Most parents reported that their child brushed twice per day and brushed on “his/her own with adult supervision” or “alone.” There were no statistical differences (P < 0.05) in dietary snack choices (foods and beverages) between the arms at all study visits, with “chips and crackers” and “fruit” being the most common snack foods and “juice” and “water” the most common beverages. The exception was Gatorade, which was more frequent (P = 0.040) in the RT arm than the SDF arm at baseline.
Pain
There was no significant difference in reports of pain between the arms at any visit except at 9 mo (P = 0.046) and 12 mo (P = 0.050), in which the SDF arm had significantly higher reports of pain. There were no unanticipated adverse events in any of the arms at any visit.
Provider Preference
At baseline, dentists were asked to rank the difficulty of treatment, preference of treatment provided as compared with treatment typically provided for a similar lesion, and length of treatment time. When compared with RT, SDF was rated as significantly easier (P < 0.001), more preferable (P < 0.001), and faster (P < 0.001). When measured, SDF was significantly faster (P < 0.001) than RT (mean, 5 vs. 30 min).
Parent Preference
At 6 and 12 mo there were no significant differences (P > 0.05) in parental acceptability, satisfaction, and preference between treatments. The majority of parents stated that they had no concerns with their child’s tooth appearance after treatment, were not dissatisfied with the tooth color, did not believe that their child was concerned with the tooth appearance, and were willing to have another tooth treated with the same treatment modality as the study tooth.
Child Preference
At 12 mo, children in the RT arm versus the SDF arm felt happier with how their teeth looked (P = 0.047), and their dental visit hurt less (P = 0.049). No significant differences (P > 0.05) were noted in any prior visits, with the majority of children stating that they were happy with how their tooth looked, that their tooth felt great, and that their visit was easy and did not hurt.
Discussion
In this 12-mo RCT, the use of RT to treat cavitated lesions in the primary teeth of young children resulted in significantly fewer failures than biannual application of 38% SDF. Most trials on SDF have measured success and failure based solely on lesion arrest (i.e., change in lesion hardness). Minor and major failures have been used in the dental caries trial literature when comparing strategies in which the primary outcome of “failure” is based on a number of diverse clinical outcomes, which may vary by treatment (Innes et al. 2011; Santamaría et al. 2014; Santamaría et al. 2018). In this study, assessment of SDF’s success or failure included lesion progression and arrest, as well as other clinically relevant variables (Table 1). The outcome of “major failure” refers to a catastrophic failure that will lead to severe damage (irreversible pulpitis) or loss of the tooth. As expected, there were very few major failures in this trial, yet SDF had significantly more than RT.
In short periods such as this 12-mo trial, the success rate of RT is generally high, even when there is great variation depending on lesion extension, material, and technique used (Santamaría et al. 2020), with stainless steel crowns having higher success rates and glass ionomers having higher failure rates. Santamaría et al. (2014) reported major + minor failure rates of 29% for RT (primarily based on use of compomers) at 12 mo. Our combined RT failure rate (primarily stainless steel crown, amalgam, and resin composite) was 7% in the intent-to-treat analyses via a simple carry-forward method to impute missing data or 26% per a simulation-based imputation, with both methods arriving at the same conclusions.
In this trial, biannual use of 38% SDF was effective in arresting (i.e., hardening) 57% of lesions at 6 mo and 74% at 12 mo, despite most lesions turning black. The majority of SDF failures were related to lesions that did not arrest and/or progressed, which may have affected differences in child acceptability at 12 mo. Trial results are in agreement with systematic and umbrella reviews, which conclude that 38% SDF is effective in arresting cavitated lesions in primary teeth, with arrest rates increasing after multiple applications (Seifo et al. 2019; Urquhart et al. 2019) and ranging from 65% to 91% (Duangthip et al. 2015; Gao, Zhao, et al. 2016; Gao, Zhang, et al. 2016; Seifo et al. 2019). Evidence-based practice guidelines in the United States support the biannual application of 38% SDF (Crystal et al. 2017; Slayton et al. 2018) as used in this trial. In contrast with other studies (Zhi et al. 2012; Duangthip et al. 2016), this trial found that the position of the tooth in the arch or the type of surface was not associated with failure rates, which is similar to the finding of Abdellatif et al. (2021). In addition, the trial did not find an association of lesion depth with failure rate. Similar to other studies (Santamaría et al. 2014), there were difficulties removing plaque at 3 and 6 mo in the nonrestored group (SDF arm), and even when it was hypothesized that failures would be associated with plaque accumulation (van Strijp and van Loveren 2018), this did not affect 12-mo failure rates. The method of assessing plaque accumulation was subjective (visual) and might not have been precise enough to capture the activity of the accumulating biofilm in the cavitated lesions.
Zhi et al. (2012) reported arrest rates of 43% at 6 mo and 53% at 12 mo after biannual application of 38% SDF and only 31% at 6 mo and 29% at 12 mo after restoration with glass ionomer. Mabanghkru et al. (2020) found much lower SDF arrest rates (35.7%) when targeting 1- to 3-y-olds at 12 mo. The type of material (Santamaría et al. 2020) and definition of arrest in the restorative group (i.e., lesion covered by material) may explain the differences as compared with this trial. An RCT compared over 12 mo the biannual use of 38% SDF to atraumatic RT (ART) to arrest lesions in the primary teeth of children 3 to 8 y old (Abdellatif et al. 2021). No significant differences in lesion arrest occurred at 6 and 12 mo between treatments. The study considered a restored lesion arrested if the restoration covered the cavity, there was partial or total restoration loss, or the lesion was hard or rough in an asymptomatic tooth. In this trial, a restoration failure to the point that the lesion is available for assessment of activity (texture, roughness) would be considered a minor failure. Similar to this trial, Abdellatif et al. (2021) found that SDF was faster (3.3 min) than ART (14.4 min). ART is a less invasive approach and would require less chair time than the RT techniques that were ultimately chosen by dentists in this trial. ART was not excluded in this trial, as all materials and techniques were available at the discretion of the operator as appropriate to the case. Yet none of the operators chose to use ART, suggesting that an assessment might be warranted of how conservative approaches in caries lesion management are being incorporated and used. Vollú et al. (2019) compared over 12 mo the efficacy of 30% SDF versus ART in children 2 to 5 y old and also noted that SDF was faster and had similar results to ART in lesion arrest, child anxiety, aesthetic perception of treatment, and quality of life.
There was no significant difference with regard to pain, except toward the end of the trial, with pain being reported more frequently in the SDF arm. A recent study showed no significant differences in pain and infection among various types of restorative and nonrestorative treatments (Innes et al. 2020).
Similar to Innes et al. (2020) study, there were no differences in parental preference, acceptability, and satisfaction between treatments in this trial. This trial was based on a diverse group representative of the diverse population in Ann Arbor and Flint, Michigan. Yet, the trial was not designed to assess responses among population subgroups (by race, ethnicity, socioeconomic status, etc.), an area where future studies are needed. Parents’ trust in the dental provider could likely be an important factor affecting treatment satisfaction, regardless of treatment choice (El-Yousfi et al. 2020; Innes et al. 2020). RCTs may also select a sample population that is willing to accept either treatment.
This trial has several limitations. The choice of material and technique in the RT group was left to the dentist, with none choosing ART. The study was not powered to compare different types of restorative materials or cavity preparation/removal techniques with SDF. Recruitment of participants was initially slow, in part because SDF was new in the United States and unknown to clinicians and patients and then affected by the COVID-19 pandemic and the Flint water crisis. Early in the study, the municipal water in Flint was contaminated with lead, which led to difficulties with recruitment. The impact that the water crisis and possible lead contamination may have had on study participants is unknown. As a result of the length of recruitment, several pediatric dentistry residents were calibrated. Nevertheless, there were 5 main examiners throughout the study (W.Y., A.S., Z.Z., R.A., and J.C.), who were recalibrated annually. In addition, the gold standard (M.F.) remained constant. The participant age of this trial was wide to allow inclusion of ICDAS 5 and 6 lesions on all primary teeth, anterior and posterior. Yet the study was not powered to assess differences among age groups or subgroups of the population, an interesting future research question. To overcome differences in study completion by the 2 study groups, missing data were imputed. Moreover, dropouts were more common in the RT group, which was expected to have fewer failures given the choice of materials ultimately used in the trial. As such, any bias would be toward finding fewer group differences in the failure outcomes, yet our results clearly show differences between groups. Finally, this trial did not address the role that SDF could play prior to placement of a restoration. This is an area of significant interest where future studies are needed, given that many clinicians end up restoring SDF-treated teeth. A recent RCT suggested that prior treatment with SDF does not affect the success rate of ART but does have a very small yet statistically significant effect on treatment time (4.8 vs. 5.1 min; Jiang et al. 2020).
In conclusion, SDF-treated lesions had significantly more major and minor failures at 12 mo as compared with restored lesions. This suggests that these lesions need close monitoring in a child population at high caries risk.
Author Contributions
J. Cleary, contributed to data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; R. Al-Hadidi, A. Scully, Z. Zaid, contributed to data acquisition, analysis, and interpretation, critically revised the manuscript; W. Yahn, contributed to design, data acquisition, analysis, and interpretation, critically revised the manuscript; J.R. Boynton, contributed to data acquisition and interpretation, critically revised the manuscript; G.J. Eckert, contributed to design, data analysis, and interpretation, drafted and critically revised the manuscript; E. Yanca, contributed to data interpretation, critically revised the manuscript; M. Fontana, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
We thank the dentists who helped identify participants for the study (Stacie Sueda, Doug Fujawa, Caroline Beitel, Tara Groff, Stephanie Shin, Erica Wu, Zohra Saleh, Betsey Baumann Smeenge, Stephen Sueda, and David Weishuhn). Additionally, we thank Dr. June Chu-Chun Hsiao, Dr. Litsa Karaouzas, Dr. Petros Papagerakis, and Dr. Tracy de Peralta for their participation in the graduate pediatric dentistry thesis committees.
Declaration of Conflicting Interests
M. Fontana is a scientific advisory consultant for the Delta Dental Plans Association. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Delta Dental Plan of Wisconsin and the Renaissance Health Service Corporation of Michigan.