
Abstract
Introduction:
Markers of poor oral health are associated with impaired cognition and higher risk of Alzheimer disease (AD) and thus may help predict AD.
Objectives:
The aim of this study was to evaluate the cross-sectional association between empirically derived groups of 19 IgG antibodies against periodontal microorganisms and cognition in middle-aged and older adults.
Methods:
The study population consisted of participants of the third National Health and Nutrition Examination Survey (NHANES III) (1988 to 1994), who were 60 y and older, among whom cognition and IgG antibodies against 19 periodontal microorganisms were measured (
Results:
In multivariable quantile regression analyses, the Orange-Red (Prevotella melaninogenica, Prevotella intermedia, Prevotella nigrescens, Porphyromonas gingivalis) and Yellow-Orange (Staphylococcus intermedius, Streptococcus oralis, Streptococcus mutans, Fusobacterium nucleatum, Peptostreptococcus micros, Capnocytophaga ochracea) cluster scores were negatively associated with cognition. A 1-unit higher cluster score for the Orange-Red cluster was associated on average with a lower cognitive score (β for 30th quantile = −0.2640; 95% confidence interval [CI], −0.3431 to −0.1848). Similarly, a 1-unit higher score for the Yellow-Orange cluster was associated with a lower cognitive score (β for 30th quantile = −0.2445; 95% CI, −0.3517 to −0.1372).
Conclusion:
Groups of IgG antibodies against periodontal microorganisms were associated with lower cognition among free living adults 60 years and older, who were previously undiagnosed with cognitive impairment. Though poor oral health precedes the development of dementia and AD, oral health information is currently not used, to our knowledge, to predict dementia or AD risk. Combining our findings with current algorithms may improve risk prediction for dementia and AD.
Knowledge Translation Statement:
IgG antibodies against periodontal microorganisms were associated with lower cognition among adults 60 years and older previously undiagnosed with cognitive impairment. Periodontal disease may predict cognition among older adults.
Keywords
Introduction
Early Alzheimer disease (AD) diagnosis may improve its management and slow disease progression (Nousia et al. 2018). Developing new biomarkers complementing existing diagnostic tools can potentially contribute to early AD diagnosis and risk prediction (Keshavan et al. 2017; Weiner et al. 2017). IgG antibodies against selected periodontal microorganisms precede the development of cognitive impairment by several years (Sparks Stein et al. 2012), and IgG levels remain elevated in the blood for up to 15 y following initial exposure to periodontal disease (Papapanou et al. 2004; Lakio et al. 2009). IgG antibodies against periodontal microorganisms may therefore be useful novel biomarkers to predict AD risk. Oral microorganisms are closely related to AD (Dominy et al. 2019), and periodontal microorganisms are found in higher quantities in the brains of individuals with AD (Dominy et al. 2019). Clinical and microbiological markers of periodontal disease were associated with the higher incidence of all-cause mortality and AD dementia and AD mortality among middle-aged and older US adults followed up over 26 y (Beydoun et al. 2020). Although oral health and AD are associated (Leira et al. 2017), oral health measures are not currently used to assess risk of AD (Dye et al. 2009), impaired cognition, or dementia.
The overall goal of our study was to identify oral health–related markers of early cognitive decline that could then be used to identify at-risk individuals for subsequent interventions to slow cognitive decline. We have reported that empirically derived groups of IgG antibodies against 19 periodontal microorganisms consistently predicted all-cause, cardiovascular, and cancer mortality in the Third National Health and Nutrition Examination Study (NHANES III) follow-up study (Qi et al. 2020; Zhong et al. 2020). The main rationale for evaluating naturally occurring groups of IgG antibodies against periodontal microorganisms was to capture effects of possible microbial interactions involved in the development of periodontal disease (Socransky and Haffajee 2005). In addition to providing insights into possible microbial interactions, groups could also be markers of systemic outcomes. In addition, chances of type I error would decrease while evaluating groups compared with individual organisms (Wang et al. 2007).
The aim of this study was to evaluate the association between these empirically derived groups of 19 IgG antibodies against periodontal microorganisms and cognition in middle-aged and older adults.
Materials and Methods
Data Source
We used data from the NHANES III, which was conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC) between 1988 and 1994 in a representative sample of the noninstitutionalized civilian US population, consisting of 39,695 individuals aged 2 mo and older. Data were collected via household interview, medical and dental examination, and laboratory tests with strict quality control procedures. Detailed information on survey methodology is described elsewhere (Ezzati et al. 1992; US Department of Health 1992; National Center for Health Statistics 1994).
Population Description
IgG antibodies against 19 periodontal bacteria were analyzed in 2008 from stored serum samples for 8,153 NHANES III participants who were 40 y and older at the time of examination (CDC and NCHS 2008). Cognitive function was evaluated among respondents 60 y and older. We used data from participants with complete data on IgG antibody titers against periodontal microorganisms and cognitive function (N = 5,162). Checkerboard immunoblotting with quantification was used to assess IgG antibody levels against multiple species, which was validated against enzyme-linked immunosorbent assay (ELISA) (Sakellari et al. 1997; Papapanou et al. 2000).
Exposure Measures
Cluster formation and naming the clusters
The exposure measures were IgG antibody titers against 19 periodontal pathogens grouped into 4 mutually exclusive groups using cluster analysis, which is described in detail in a prior study (Merchant et al. 2014). These consisted of the following:
Cluster 1: Orange-Red (Prevotella melaninogenica, Prevotella intermedia, Prevotella nigrescens, Porphyromonas gingivalis)
Cluster 2: Red-Green (Tannerella forsythia, Treponema denticola, Aggregatibacter actinomycetemcomitans, Eikenella corrodens, Selenomonas noxia, Veillonella parvula, Campylobacter rectus)
Cluster 3: Yellow-Orange (Staphylococcus intermedius, Streptococcus oralis, Streptococcus mutans, Fusobacterium nucleatum, Peptostreptococcus micros, Capnocytophaga ochracea)
Cluster 4: Orange-Blue (Eubacterium nodatum, Actinomyces naeslundii)
The cluster names were adapted from the nomenclature used by Socransky and Haffajee (2002, 2005) to describe periodontal microorganism groups related to clinical periodontal conditions, where Red and Orange complexes indicate periodontal disease, Yellow and Purple complexes indicate healthy periodontium, Blue complex indicates both healthy and disease state, and Green complex weakly indicates periodontal disease.
Clusters were named based on the composition of microorganisms in each cluster. For example, cluster 1 contained antibodies against 4 microorganisms, 3 of which were from Socransky’s Orange complex and one from the Red complex and was named the Orange-Red cluster (P. melaninogenica, P. intermedia, P. nigrescens, P. gingivalis). The remaining clusters were named similarly.
Calculating cluster score
A score for each cluster was calculated by summing z scores of standardized log-transformed IgG titers for each antibody in that cluster. For example, the Orange-Red cluster score was computed using antibody titers against P. melaninogenica, P. intermedia, P. nigrescens, and P. gingivalis; z scores of log-transformed antibody titers for these titers were summed to obtain a score for that cluster, and so on (Merchant et al. 2014).
Outcome
Cognition was measured using a version of the Mini-Mental State Examination (MMSE), which was administered in the home interview and at the mobile examination center (Pfeiffer 1975; Perkins et al. 1999; Obisesan and Gillum 2009). It consists of 6 orientation, 6 recall, and 5 attention-related questions. Each correct response was assigned 1 point, and an incorrect response received a score of 0 points. The outcome used in these analyses was the total score, which was obtained by summing the points assigned to the responses and ranged from 0 to 17, with higher scores indicating better cognitive function. The 6 orientation items asked about the day of the week, the date, and participant’s complete address, including street, city or town, state, and ZIP code (adult questionnaire). To evaluate recall, the interviewer told the participant the names of 3 items (apple, table, and penny) and asked him or her to repeat them. Each participant was given up to 6 tries to learn the words. If they correctly recalled the items at any of the 6 tries, the response was considered correct. This exercise was repeated after assessing attention to give a maximum of 6 points for recall. To evaluate attention, the interviewer asked the participant to serially subtract 3 from 20 and repeat this for up to 5 times. For example, they were asked to subtract $3 from $20, $3 from $17, and so on and assigned 1 point for each correct answer. We used the total MMSE score as a continuous variable in our analyses.
Covariates
Covariates to control for potential confounding factors included age (40 to 64 y, ≥65 y); sex (male and female); race (Black, White, and other); educational level (<12 y, ≥12 y completed education); poverty income ratio (PIR), which was divided into 3 groups (≤1.3, 1.3 <PIR ≤3.5, >3.5); smoking status (current, former, never smoker); drinking status (drinker and nondrinker); body mass index (BMI), including normal (≤24.9 kg/m2), overweight (25 to ≤29.9 kg/m2), and obese (≥30 kg/m2); diabetes; hypertension; other comorbidities (heart disease, cancer, stroke); periodontal disease; and annual dentist visits. Oral health measures were obtained from the Oral Examination component of NHANES III (National Center for Health Statistics 1992).
Statistical Analysis
As the outcome measure (cognitive score) was highly skewed, we opted to use quantile regression for the primary analyses rather than transforming the outcome and using least squares regression. The advantages of this approach were, first, the results remained on the natural scale, making them more interpretable; second, quantile regression does not require assumptions about distribution of residuals and is not sensitive to outliers (Bottai et al. 2010); and, finally, it was possible to evaluate associations between antibodies and cognition at different parts of the outcome distribution (Bottai et al. 2014). For the primary analyses, we used quantile regression to evaluate the relation between antibody clusters and cognition score from the 30th and 70th quantiles. Confidence intervals (CIs) were obtained by resampling. For the sake of completeness, we repeated the analyses using least squares regression after log transforming the cognitive score. In all analyses, we controlled for age, sex, race, educational level, PIR, smoking status, drinking status, BMI, diabetes, hypertension, other comorbidities, periodontal disease, and annual dentist visits. We further conducted stratified analyses by age group, sex, race, and whether the individual visited a dentist in the past year.
Data management and statistical analyses were conducted using SAS 9.4 (SAS Institute). The sample weights provided by NHANES III were used in all procedures. The threshold for statistical significance was 0.05. This study is compliant with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. These analyses were classified as nonhuman subjects research by the Institutional Review Board of the University of South Carolina.
Results
The potential confounders were similarly distributed across the extreme antibody categories for each of the 4 clusters with some exceptions (Table 1). Individuals in the highest antibody group compared with the lowest were proportionately older in the Red-Green group and younger in the Orange-Blue group but similar in the Orange-Red and Yellow-Orange groups. Diabetes prevalence was lower in the top category of Red-Green, Yellow-Orange, and Orange-Blue groups but higher in the Orange-Red group. Individuals visited a dentist in the past year less often in the top category of the Red-Green and Orange-Red groups and more often in the Yellow-Orange and Orange-Blue groups. Periodontal disease was more prevalent in the top categories of the Red-Green, Orange-Red, and Yellow-Orange clusters but lower in the Orange-Blue cluster (Table 1).
Descriptive Characteristics (Weighted) of Adults Aged ≥60 y with Information on Antibodies against Periodontal Microorganisms and Measures of Cognition, Third National Health and Nutrition Examination Study.
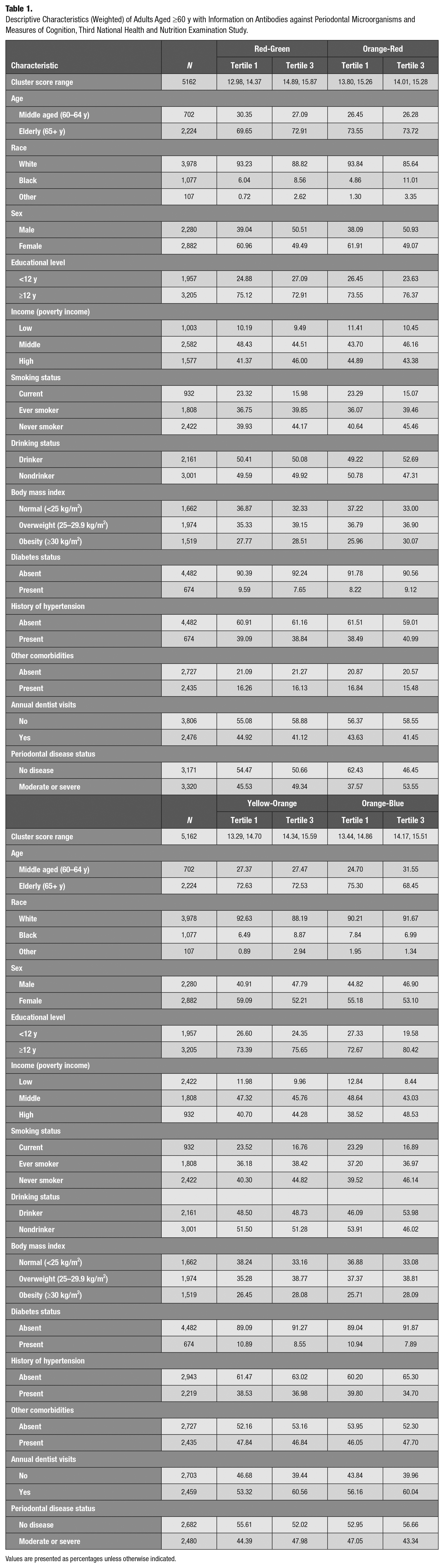
Values are presented as percentages unless otherwise indicated.
In quantile regression analyses, the Orange-Red and Yellow-Orange cluster scores (positively associated with periodontal disease) were negatively associated with cognition after controlling for age, sex, race, educational level, poverty income ratio, smoking status, drinking status, BMI, diabetes, hypertension, other comorbidities, periodontal disease, and annual dentist visits. A 1-unit increase of the cluster score for the Orange-Red cluster was associated on average with a lower cognitive score (β for 30th quantile = −0.2640; 95% CI, −0.3431 to −0.1848) (Table 2). The Red-Green cluster score (positively associated with periodontal disease) was associated with a higher cognitive score, and the Orange-Blue cluster (negatively associated with periodontal disease) was not associated with cognition (Table 2, Figure). The associations were stronger in the 30th versus 70th quantile for the Orange-Red, Yellow-Orange, and Red-Green clusters, P < 0.05 (Table 2, Figure).
Associations between Antibody Clusters and Cognitive Score among Adults Aged ≥60 y, Third National Health and Nutrition Examination Study.
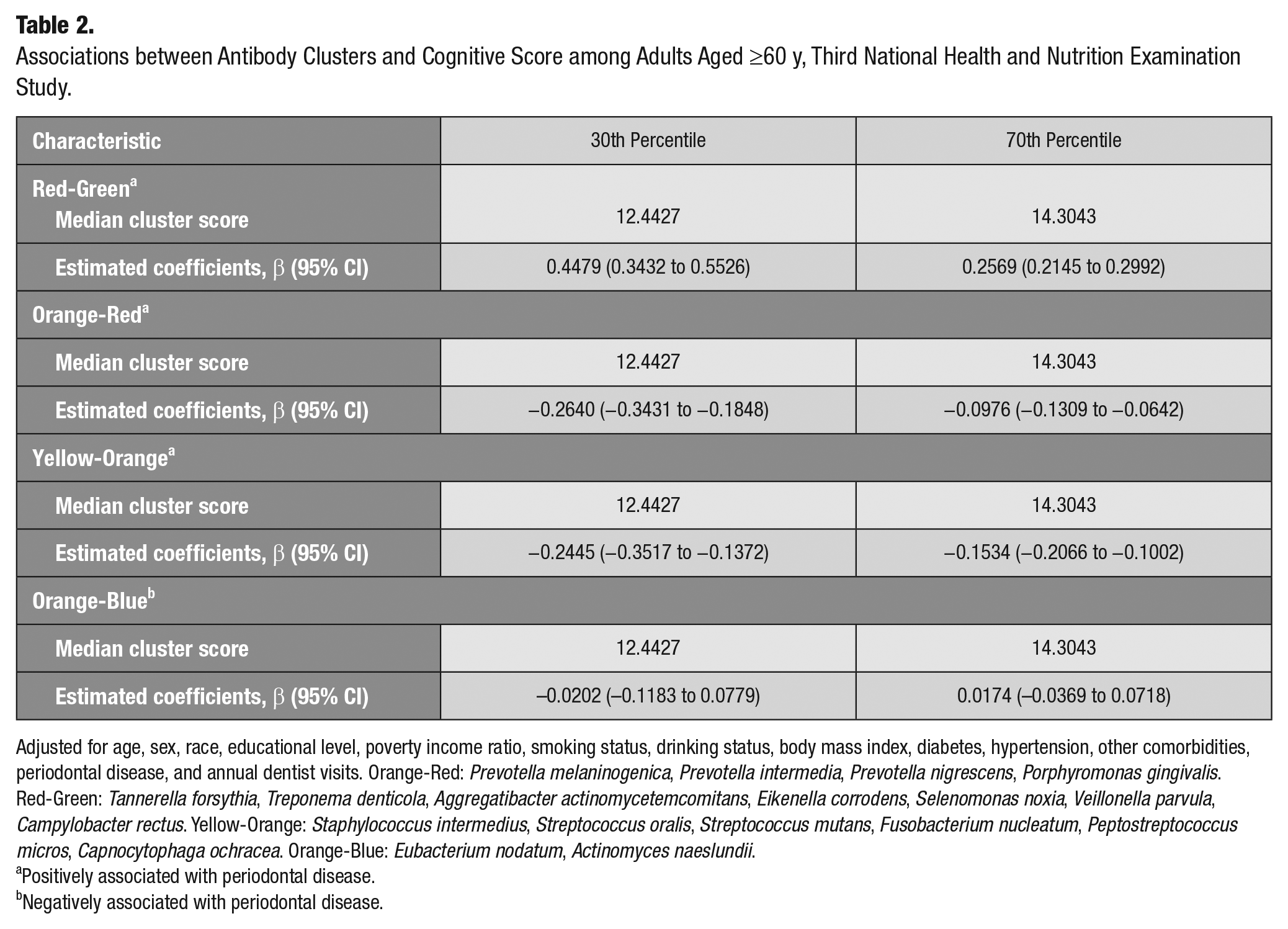
Adjusted for age, sex, race, educational level, poverty income ratio, smoking status, drinking status, body mass index, diabetes, hypertension, other comorbidities, periodontal disease, and annual dentist visits. Orange-Red: Prevotella melaninogenica, Prevotella intermedia, Prevotella nigrescens, Porphyromonas gingivalis. Red-Green: Tannerella forsythia, Treponema denticola, Aggregatibacter actinomycetemcomitans, Eikenella corrodens, Selenomonas noxia, Veillonella parvula, Campylobacter rectus. Yellow-Orange: Staphylococcus intermedius, Streptococcus oralis, Streptococcus mutans, Fusobacterium nucleatum, Peptostreptococcus micros, Capnocytophaga ochracea. Orange-Blue: Eubacterium nodatum, Actinomyces naeslundii.
Positively associated with periodontal disease.
Negatively associated with periodontal disease.
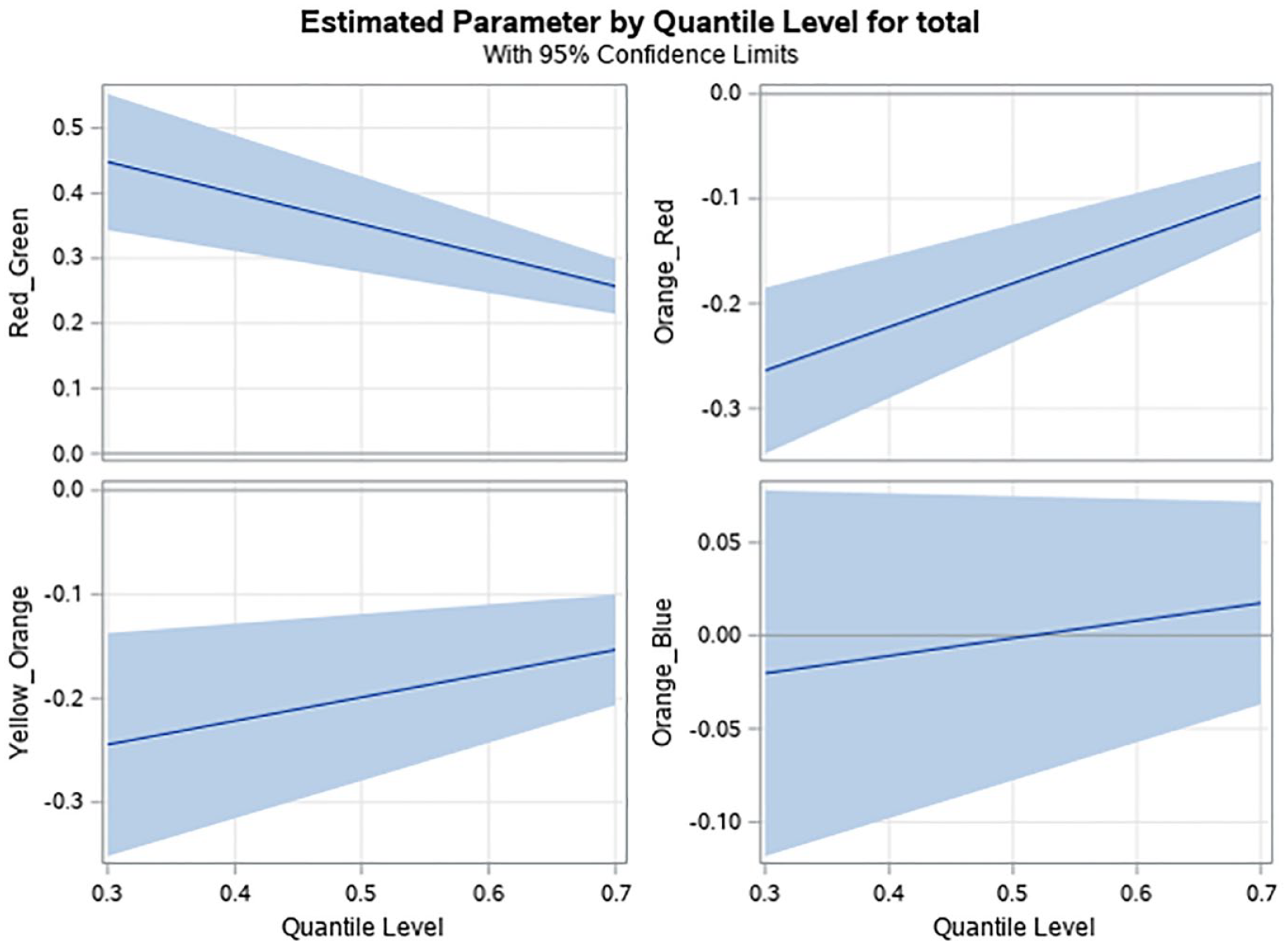
Association between periodontal antibody groups and cognitive score from quantile regression models evaluated at 30th and 70th percentiles after the adjustment of the other covariates. P value evaluating difference in parameter estimates of 30th and 70th percentiles <0.05 for Red-Green, Orange-Red, and Yellow Orange groups. Orange-Red: Prevotella melaninogenica, Prevotella intermedia, Prevotella nigrescens, Porphyromonas gingivalis. Red-Green: Tannerella forsythia, Treponema denticola, Aggregatibacter actinomycetemcomitans, Eikenella corrodens, Selenomonas noxia, Veillonella parvula, Campylobacter rectus. Yellow-Orange: Staphylococcus intermedius, Streptococcus oralis, Streptococcus mutans, Fusobacterium nucleatum, Peptostreptococcus micros, Capnocytophaga ochracea. Orange-Blue: Eubacterium nodatum, Actinomyces naeslundii. Orange-Red, Red-Green, and Yellow-Orange were positively associated with periodontal disease. Orange-Blue was negatively associated with periodontal disease.
Qualitatively similar results were obtained from linear regression analyses adjusted for the same covariates as in the quantile regression models with the outcome (cognitive score) log transformed (Appendix Table 1).
The associations were generally consistent across categories of age group, sex, race, and whether participants visited a dentist in the past year (Appendix Table 2). The median antibody scores for individuals who visited a dentist in the past year were lower than those who did not.
Discussion
Higher levels of IgG antibodies from the Orange-Red and Yellow-Orange groups (positively associated with periodontal disease) were related with lower cognitive scores among free-living adults 60 y and older previously undiagnosed with cognitive impairment. The associations were stronger at the lower ends of the antibody distributions, indicating that even low levels of periodontal disease could be associated with poor cognition.
There is a growing body of evidence linking poor oral health with increased risk of AD, dementia, and poor cognition. AD was positively associated with periodontal disease (odds ratio [OR], 1.69; 95% CI, 1.21–2.35) and severe periodontal disease (OR, 2.98; 95% CI, 1.58–5.62) in a well-conducted systematic review and meta-analysis (Leira et al. 2017). Individuals with tooth loss had a higher risk of dementia than individuals without tooth loss (relative risk [RR], 1.34; 95% CI, 1.19–1.51); risk of dementia increased in a dose-dependent manner (RR, 1.01; 95% CI, 1.00–1.02) for each additional tooth lost in a recent meta-analysis of 8 cohort studies published until June 2018 consisting of 14,362 individuals and 2,072 dementia cases (Chen et al. 2018). Tooth loss was associated with increased risk of dementia (OR, 1.18; 95% CI, 1.15–1.22), while periodontal treatment was associated with reduced dementia risk (OR, 0.96; 95% CI, 0.93–0.99) in a population-based, propensity score–matched cohort of >200,000 individuals in South Korea (Yoo et al. 2019). Dementia risk was associated with poor oral hygiene and suboptimal oral health (gingivitis, dental caries, tooth loss, edentulousness) in another recent systematic review (Daly et al. 2018). Dementia was also associated with increased risk of developing periodontal disease (Ma et al. 2021). The Orange-Red cluster includes antibodies against P. gingivalis and P. intermedia. IgG antibodies against P. gingivalis were associated with dementia incidence and AD mortality (Beydoun et al. 2018; Beydoun et al. 2020), and antibodies against P. intermedia and F. nucleatum (Yellow-Orange cluster) were higher among AD cases compared with controls (Sparks Stein et al. 2012). Infection by P. gingivalis and P. gingivalis lipopolysaccharide (Pg-LPS) administration increased Aβ production and induced inflammation and neurodegeneration in animal studies (Costa et al. 2021). Pg-LPS simultaneously induced inflammation-dependent bone loss around the teeth (similar to destruction associated with periodontal disease) and memory decline in middle-aged mice (Gu et al. 2020). Our results are thus consistent with prior findings and are biologically plausible.
The positive association between the Red-Green cluster cognitive scores was an unexpected finding. As antibodies in the Red-Green cluster are indicative of periodontal disease, similar to antibodies in the Orange-Red and Yellow-Orange clusters, we expected to observe a negative association between this cluster and cognition. One explanation for this finding could be survivor bias due to the cross-sectional study design. The Red-Green cluster, which includes IgG antibodies against A. actinomycetemcomitans, was positively associated with mortality in a prospective study conducted in this population (Qi et al. 2020). Antibodies against A. actinomycetemcomitans have been associated with AD (Noble et al. 2014) and have been shown to induce damage to hippocampal cells in vitro (Diaz-Zuniga et al. 2019). It is possible that individuals characterized by the Red-Green cluster who previously died had poor cognition, and participants of the current cross-sectional investigation were survivors with better cognition. These findings need to be verified in future prospective studies.
This study had some limitations. While directionality could not be ascertained because of the cross-sectional design, the findings could be used for prediction. Likewise, although the data were from an older sample, the relationship between exposure and outcome remain valid. As with any observational study, residual confounding is possible even after controlling for many factors. Differences in incidence and prevalence of amnestic and nonamnestic dementia between Blacks and Whites have been reported (Katz et al. 2012), but we were unable to distinguish the difference. Antibody scores of those who visited a dentist in the past year were lower than those who did not, which may be the result of periodontal treatment or maintenance therapies, but we could not verify this. However, the associations between the antibody clusters and cognitive scores were qualitatively similar among those who visited or did not visit a dentist in the past year. Finally, measurement error in assessing the outcome could attenuate the associations.
The study also had some strengths. This was a large, population-based sample, which contributed to greater external validity of the findings. The data were collected with strict quality control, and many potential confounders were available for adjustment, which increased the internal validity of the results. Evaluating impaired cognition in relation to empirically derived antibody groups rather than single antibodies reduces the likelihood of false-positive findings (Wang et al. 2007) and captures the natural in vivo grouping of antibodies. Furthermore, this approach accounts for potential interactions between the antibodies, which may be critical because the immune responses in mice infected with multiple periodontal microorganisms were different compared with infections from single microorganisms (Rivera et al. 2013). Although poor oral health is associated with worse cognition, it is not used to predict undiagnosed cognitive loss in clinical practice. This may be because although most primary care physicians agree about the importance of assessing the oral health needs of their adult patients, they feel inadequately trained to do so (Vernon et al. 2021). If our findings are confirmed in subsequent studies, IgG antibodies against periodontal microorganisms could be clinically useful oral health markers predicting undiagnosed cognitive loss.
Groups of IgG antibodies against periodontal microorganisms were associated with lower cognition among free-living adults 60 y and older who were previously undiagnosed with cognitive impairment. Oral health information is currently not used in clinical practice to predict undiagnosed cognitive loss. If these findings are confirmed in subsequent studies, information from IgG antibodies could be combined with established risk factors to improve prediction of undiagnosed cognitive loss.
Author Contributions
A.T. Merchant, contributed to conception, design, data acquisition, drafted and critically revised the manuscript; F. Yi, N.P. Vidanapathirana, contributed to data analysis, critically revised manuscript; M. Lohman, R.D. Newman-Norlund, J. Fridriksson, contributed to data interpretation, critically revised manuscript; J. Zhang, contributed to data analysis and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844211072784 – Supplemental material for Antibodies against Periodontal Microorganisms and Cognition in Older Adults
Supplemental material, sj-docx-1-jct-10.1177_23800844211072784 for Antibodies against Periodontal Microorganisms and Cognition in Older Adults by A.T. Merchant, F. Yi, N.P. Vidanapathirana, M. Lohman, J. Zhang, R.D. Newman-Norlund and J. Fridriksson in JDR Clinical & Translational Research
Footnotes
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: These analyses were supported by grant 1R21AG070449-01 from the National Institute on Aging.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.