
Abstract
Objective:
To describe the early feeding, weaning, and oral hygiene practices of children with early childhood caries (ECC), their parents’ knowledge and attitudes regarding infant feeding, and the feeding-related challenges faced by the parents.
Methods:
This descriptive qualitative study involved parents of children with ECC who sought dental treatment at an academic dental college in India. Data were collected though focus groups conducted with the 27 parents of children with ECC, using a focus group discussion guide. Data were analyzed using the content analysis method.
Results:
Community norms, such as learning from the older women in the families or neighborhoods, guided the feeding method, duration of feeding, and weaning. Breastfeeding or bottle-feeding at bedtime beyond 12 mo of age and feeding sugary drinks during weaning were standard practices, despite knowing the risk for dental caries. Parents faced multiple challenges regarding weaning and were unaware of the significance of infant oral hygiene practices.
Conclusion:
In children with ECC, infant feeding practices included prolonged breastfeeding or bottle-feeding beyond the required age, feeding at bedtime, and feeding sugary drinks. Although the parents knew that these feeding habits could increase the risk for caries, they lacked the self-efficacy to translate their knowledge into action during weaning. Also, they lacked awareness regarding infant oral hygiene practices.
Knowledge Transfer Statement:
The study provides information on the feeding habits of infants that can increase the risk for caries, the challenges faced by the parents of these children in altering these risky habits, and their lack of knowledge on infant oral hygiene practices. Policy/decision makers can advocate for pediatricians and pediatric dentists to incorporate anticipatory guidance or motivational interviewing techniques to tailor the preventive program for ECC for Indian children.
Introduction
Dental caries is a common chronic disease affecting all age groups in both developed and developing countries (Selwitz et al. 2007). When caries affects children under the age of 6 y, with 1 or more decayed, missing, or filled primary teeth, it is called early childhood caries (ECC) (American Academy of Pediatric Dentistry 2018). ECC has a multifactorial etiology, such as cariogenic microorganisms, fermentable carbohydrates, and social and behavioral factors (Anil and Anand 2017). ECC, in addition to causing pain and affecting the oral and general well-being of the children, can increase caries risk during adult life (Drummond et al. 2013; Corrêa-Faria et al. 2016). In addition, ECC can increase the need for health care service utilization and emergency visits and thus poses a significant economic burden (Braun et al. 2017).
Studies have explored the causal link between feeding habits during early infancy and ECC (Avila et al. 2015; Feldens et al. 2018). Tham et al. (2015) conducted a systematic review and meta-analysis, reporting that while breastfeeding might not lead to dental caries per se, breastfeeding at bedtime and frequent breastfeeding, especially beyond 12 mo of age, could increase ECC risk. Another systematic review stated that exclusively bottle-fed infants had a higher risk for ECC when compared with the breastfed children (Avila et al. 2015). Furthermore, the frequent intake of sugary food and drinks in the first 12 mo of life is another important risk factor for ECC (Chaffee et al. 2015).
The increased risk for caries because of bedtime breastfeeding or bottle-feeding can be due to the presence of fermentable sugar in the mouth, exacerbated by a lack of oral hygiene care during infancy. Mothers often lack knowledge regarding infant oral hygiene practices and face challenges in their implementation (Finalyson et al. 2019). Early feeding and oral hygiene practices seem to be influenced by cultural and parental factors such as the parents’ knowledge, attitude, and beliefs (Naidu et al. 2012; Walker et al. 2017). Therefore, it is essential to understand existing infant feeding practices in children with ECC, their parents’ knowledge, attitudes, and beliefs on infant feeding, and the challenges the parents face in initiating and maintaining healthy feeding practices for their children to prevent ECC. This study aims to describe the feeding, weaning and oral hygiene practices of children with ECC during infancy, their parents’ knowledge and attitudes concerning infant feeding and weaning, as well as the associated challenges faced by parents of children with ECC. This investigation was a part of our larger study in which we aimed to understand the oral hygiene practices, diet and feeding habits, and dental visit patterns of children with ECC in order to design programs to prevent ECC in our community. Our overarching research question was, “What parental factors increase the risk for ECC in children?” Earlier, we reported on children’s oral hygiene and dietary practices, along with the associated challenges faced by their parents (Suprabha et al. 2021; Shrikrishna Suprabha et al. 2022).
Methods
Study Setting and Design
This descriptive qualitative study (Sandelowski 2000) was conducted at the Department of Pediatric Dentistry at Manipal College of Dental Sciences, Mangalore, an academic dental college in Mangalore, located in the southwest region of India. This dental college provides routine and specialized dental care to all segments of the population in the region at a subsidized cost.
We chose the descriptive qualitative design, which allows for an in-depth exploration of the research question.
Participants
The participants were a convenience sample of parents of children with ECC. Ethics approval was obtained from the institutional ethics committee of Manipal College of Dental Sciences, Mangalore (Ref. No. 17071), and the study was performed following the ethical standards laid down in the Declaration of Helsinki of 1975, as revised in 1983 (World Medical Assembly 1983). Parents were enrolled in the study if they had at least 1 child with ECC and were receiving (or enrolled to receive) treatment for ECC for their children at our institution between March and August 2019. Our designated research staff identified potential participants, contacted them, and provided information about the study. Those who expressed interest in participating were recruited after obtaining written informed consent. Potential participants were excluded if their children with ECC had a history or diagnosis of serious medical conditions or any mental disorders. All participants were given an identification code to maintain their anonymity.
Data Collection
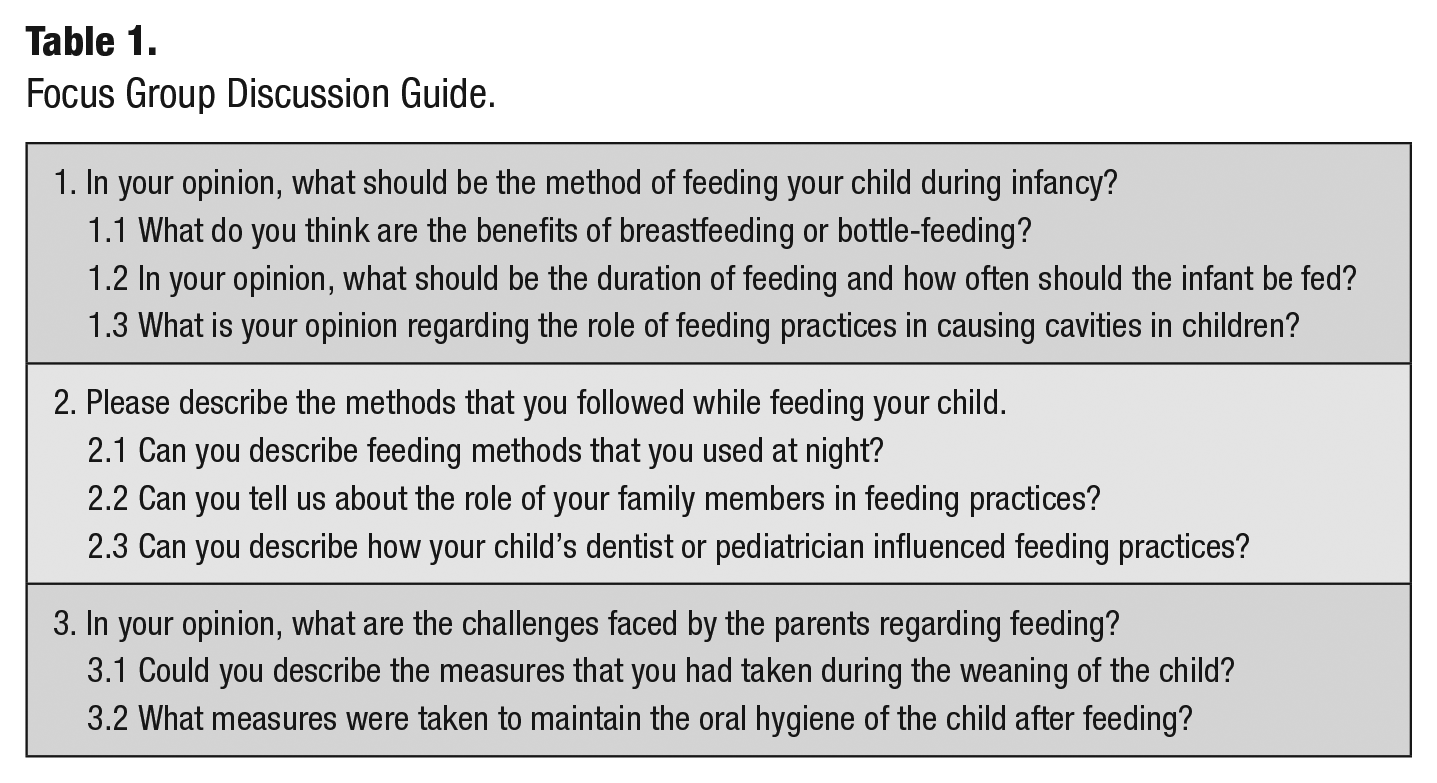
Data were collected through focus groups using a focus group discussion guide created for the study (Table 1). The focus group method was chosen to collect data because it is an efficient method to collect data that is built on group dynamics and allows for the collection of in-depth information in a short period for a considerably large sample. In addition, it allows for the informal discussions required to explore the topics, especially with the participants who know about the topic and could contribute to the discussion (Ochieng et al. 2018). The questions focused on infant feeding practices, weaning, participants’ knowledge and attitudes, and their feeding-related challenges. The focus group discussion guide had open-ended questions with additional probes to obtain an in-depth response on the topic and was developed based on the literature (Cidro et al. 2015; Walker et al. 2017). Two members of the research team (KYM and RS), who belong to the same community, reviewed the focus group discussion guide for relevance and cultural appropriateness. Then, it was pilot tested with 5 potential participants through a focus group discussion for comprehension and clarity. No changes were required for the focus group discussion guide based on participants’ feedback.
Focus Group Discussion Guide.
For the focus group discussions, the participants were seated in a well-ventilated room, away from the dental clinic in a semicircle fashion. A female pediatric dentist from the same institution who had experience conducting qualitative research moderated the focus groups. The focus group discussions were audiotaped (using a digital voice recorder), and field notes were taken. Neither the moderator nor the note taker was involved in caring for the children whose parents participated in the study. At the end of each session, the note taker summarized the key points to validate the collected information was accurate. Also, the participants’ demographic information was collected. The focus groups continued until the content of the collected data reached saturation (Hennink et al. 2019), and no-repeat focus group discussions were conducted. The focus group participants were served refreshments during the focus group discussions, and the participants were paid Rs.100 to cover the participants’ transport cost to attend the focus groups. Furthermore, at the end of each focus group discussion, the participants were given information on ECC and its prevention, following the American Academy of Pediatric Dentistry (2018) guidelines.
Data Analysis
The audiotape recordings were transcribed verbatim, and the data were analyzed using content analysis while maintaining the anonymity of the participants. The collected data were read and reread by 2 research team members who coded the data using the line-by-line coding method. The codes were inductive and deductive. For the inductive coding, the 2 reviewers coded a sample text, checked with each other, and achieved coding consistency. Then, they used the same process to code the entire text, repeatedly assessing the coding consistency by going back and forth and confirming the process (Weber 1990; Zhang and Wildemuth 2005). Categories and subcategories emerged based on the highlighted words and labels that the 2 reviewers used. Deductive coding was based on the theoretical understanding of the researchers (Elo and Kyngäs 2008).
Any disagreements between the reviewers were resolved through consensus to guard against bias and enhance the robustness of our observations (Lincoln and Guba 1985; Zhang and Wildemuth 2005). Also, we maintained an audit trail on how the data were coded, the changes made to the codes, and when the changes were made to maintain the robustness of our data analyses. Descriptive statistics were performed to describe the sample characteristics using SPSS version 27 (SPSS, Inc.). The Standards for Reporting Qualitative Research (SRQR) checklist (O’Brien et al. 2014) was used to ensure the quality of reporting the study findings.
Results
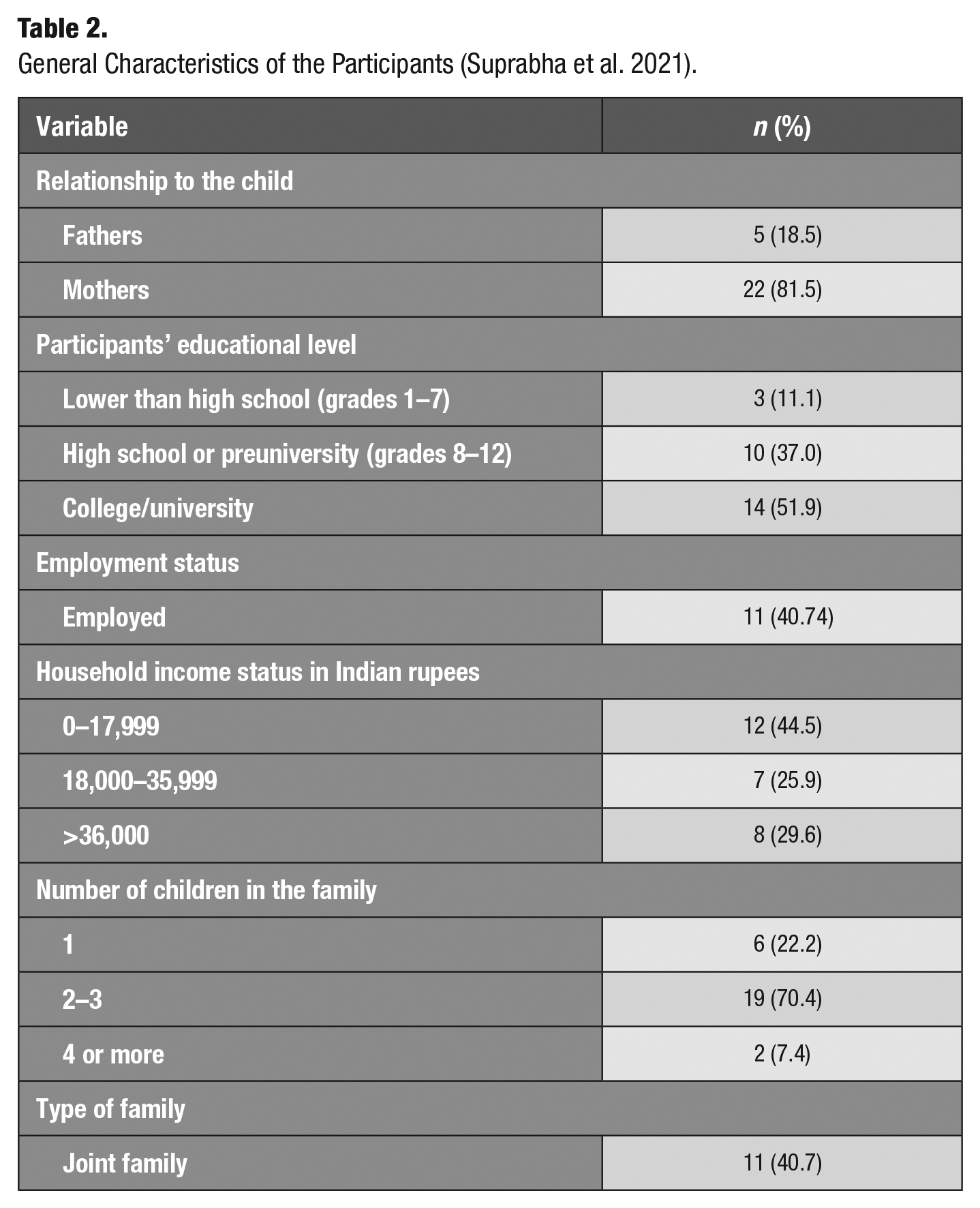
Of the 45 potential participants who were approached, 27 participated. A total of 5 focus groups were conducted, with 4 to 6 participants in each group. Each focus group lasted 1 to 2 h long, with a mean of 68 min. The mean age of participants was 35.15 y, and 70.4% of the participants were from the middle socioeconomic status as per the Kuppuswamy scale (Sharma 2017) (Table 2). The reason for nonparticipation was mainly time constraints.
General Characteristics of the Participants (Suprabha et al. 2021).
Our qualitative data analyses were delineated into 4 categories: 1) infant feeding methods and the reasoning for choosing the method, 2) perceptions of the feeding methods, 3) weaning and associated challenges, and 4) early oral hygiene practices. These categories and their subcategories are described below, using the corresponding quotes of the participants.
Infant Feeding Methods and the Reasoning for Choosing the Method
Most participants reported that they breastfed their infants, except for a small proportion (5) who bottled-fed. Breastfeeding was a norm in the region and the preferred way for feeding infants. Feeding practices were mostly according to community norms, generally adopted by observing or learning from the older women in the families, who were not limited to mothers and grandmothers and often included older women in their neighborhoods. Breastfeeding was mainly done ad libitum (as desired) and often until the child went to sleep.
The reasons for bottle-feeding included a lack of breast milk and, in some cases, the child’s refusal to be breastfed, which occurred when the child reached a certain age (8–12 mo). A mother of 2 children recalled, My elder [older] one was breastfed only for 8 months. After that, he refused to suck milk, so I started with a bottle. I used to use formula milk. For younger one, I only breastfed, I did not give a bottle.
A small percentage of the participants used infant formula (powder) as advised by their child’s pediatricians. None of the participants reported feeding breast milk in bottles, a cup, or a glass. A few reported both breastfeeding and bottle-feeding. However, they reserved bottle-feeding only for when they had to go out because they perceived bottle-feeding to be more convenient and less stressful while they were out in public. The mothers opined that pediatricians generally discouraged the use of bottles. We observed that some participants were more cautious in initiating bottle-feeding because of the fear of habit forming, difficulty in weaning, and the perceived ill effects of bottle-feeding. A mother of 2 children opined, I used to give milk in a steel glass. I breastfed the elder one for 1 year, younger one for 2 years. After that, even if they get up in the middle of the night, I used to give milk in a steel glass [cup]. I never used a bottle. I feared that using a bottle may become a habit. Many people told me this. He was used to drinking water in a steel glass during meals. So giving milk in a steel glass was convenient.
Some participants faced religious barriers to bottle-feeding and did not initiate it. One mother said, In Islam [the religion which I follow], we are forbidden to use a straw while drinking. So, I did not use sippy cups. As my child grew up, I gave her milk in a glass.
Perceptions of the Feeding Methods
Perceived advantages of breastfeeding
Most participants understood the significance of breastfeeding and believed that it is superior to bottle-feeding in terms of nutritional value and ease. They acknowledged that breastfeeding provides an opportunity to establish a bond between the mother and child, which prompted breastfeeding for longer durations. For most, breastfeeding was a healthier option than bottle-feeding, and they believed that breast milk could boost children’s intellectual capacity. A few stated that prolonged breastfed children remain underweight compared with their bottle-fed counterparts. A father of a 4-y-old child stated, If nursed for a long time, babies tend to be healthier. It may affect their weight [they may tend to be underweight], but they will gain it [the required weight] later on. But, they will become more intelligent. Hence we are not aggressive in stopping [breastfeeding].
Yet, they believed that breast milk is better for children’s brain development and contributes to their intelligence. Although their child being underweight was concerning to them, they felt that the benefits of breastfeeding were far superior. Many felt that it is challenging to maintain hygiene with bottle-feeding. One participant (mother) stated, Bottle-feeding at night is very hard. It is difficult to clean the bottle, and it should not be done. My mother, grandmother, used to feed [breastfeed] for 2 to 3 years.
Thus, they thought that bottle-feeding should be reserved only when breastfeeding is impossible.
Perceived benefits and harms of feeding practices
Most participants clearly understood that the sugar content in the milk is responsible for tooth decay. They also knew that, like any other food, milk could cause caries as well, whether it is breast milk, cow’s milk, or infant formula. One father stated, Milk remains in teeth and causes cavities.
The bottle-fed children often slept with the bottle in their mouths. One response was, I used to breastfeed periodically as per the time prescribed by the doctor when she was a very small baby. Later, after 2 years, I started with the bottle. I gave cow’s milk in the bottle. Many a times she would sleep off with milk bottle in the mouth. I used to remove it whenever I see it, after a while.
As mentioned earlier, feeding practices depended on the child’s demand, including nighttime feeding. Many were aware that night feeding is harmful to teeth as there is no opportunity to clear the baby’s mouth after falling asleep. Although parents were aware that prolonged feeding habits could increase the risk for caries, some parents felt it was challenging to break this practice. They felt compelled to continue feeding at night and did not know how to translate their knowledge into practice, indicating a lack of self-efficacy. For example, some of the participants continued feeding at night just to make the child quiet so as not to disturb other members in the same household at night. Two participants responded, When they wake up in the night, in the middle of the night, we feed, and they fall asleep. Otherwise, they don’t sleep at all, they keep crying. Children cry when they are hungry. It is easy to give bottle to them. They stop crying. But should not give too much, only up 2 years. That is OK. Then they have it off on their own.
Many of those who believed that children should not be breastfed or bottle-fed at night as they get older faced similar challenges, as they could not break the night-feeding practice for the same reason. One participant stated, My child sleeps with bottle in the mouth, he does not listen.
To overcome this challenge, some introduced solid foods to their children at a much younger age so that they would not wake up at night hungry, thus lessening the need for nighttime feeding. One such participant (mother) said, After 6 months, we give rice. Usually, they don’t like to breastfeed as they are fulfilled [meaning, not hungry].
Even those who favored nighttime feeding at the child’s demand found it challenging to stop this habit. One participant said, They won’t stop in the night. Daytime I am busy, at night they will need. They are thirsty.
Perceptions of feeding duration
As mentioned earlier, breastfeeding or bottle-feeding continued as long as the child desired, ranging from 1.5 to 3 y. Most of the participants were unsure how long a child can be nursed safely, and their perceptions varied widely. Some felt it is acceptable to feed for up to 6 mo, while some felt fine feeding until 2 y of age for various reasons. Still others believed otherwise, based on their personal experiences, observations, and advice from health care professionals and others. Two participants stated, My dentist told me that feeding should be done only up to 1 year. Two years is too long, probably that is why he got cavities? Up to 1 year is OK. My mother advised to stop. If prolonged they may not agree to stop [stop breastfeeding]. They often bite, and it might affect the health of the mother.
Some feared that breastfeeding for fewer than 2 y could cause a nutritional deficiency in the child. One such concerned parent said, [Breastfeeding] up to 2 to 2½ years it is required. Otherwise calcium deficiency can occur.
Others expressed confusion because their children’s pediatrician advised them not to breastfeed or bottle-feed them beyond 2 y of age, while dentists advised them to stop within 1 y of age. Some participants felt that they did not receive the necessary information on feeding and weaning during their children’s routine health visits to their pediatrician. One parent explained, Elders [older] in the family guide us on weaning. My child’s pediatrician did not advise anything on weaning. Probably if we ask them, they would say. Since elders in the family advise us, I never felt the need to ask.
Weaning and Associated Challenges
Most parents took advice from the older women in the family or neighborhoods regarding weaning and did not seek any professional advice, as they did not deem it necessary to do so. Weaning or stopping bottle-feeding was associated with significant challenges. One mother said, It is difficult to stop bottle-feeding habit. My child falls asleep with a bottle in his mouth. I tried stopping this, but he won’t listen.
Among those who bottle-fed or fed in cups or glasses, the content of the liquids varied from person to person. Most of them used cow’s milk, some with sugar and others without sugar. Switching to drinking using a cup or glass meant sweetening their drinks. Almost all of them agreed that they added sugar or sugary syrups to their drinks, depending on the child’s preferences, mainly to make them more palatable and attractive. Two mothers explained, My first child [daughter], I used bottle. For the second one [boy], he has not used bottle. He drinks milk with glass if I add Bournvita or Horlicks or Hershey’s Syrup. To make the child drink milk in glass. I added little sugar; my child likes it and drinks well.
Parents sweetened their children’s drinks, even though they were aware that adding sugar in the drink could lead to increased tooth decay. Two mothers stated, Without sugar taste, children would not like to drink milk. If we add sugar to milk, then it can cause cavities.
We did not come across any parents seeking advice from the pediatrician or pediatric dentist but relied on the advice of the older women in their family regarding weaning. One participant explained, Elders [older women] in our family, like my mother or my mother-in-law, guided me during weaning. Probably if I had asked pediatricians would say [regarding weaning]. Since elders [older women] advised us, I never felt the need to ask.
Early Oral Hygiene Practices
Most participants did not initiate any oral hygiene habits before teeth eruption. They were not aware of the right way to clean their children’s gum pads after feeding. In addition, children fell asleep soon after feeding as an essential part of the bedtime routine. Among the small proportion of the participants who knew the importance of performing oral hygiene, they faced significant challenges cleaning their children’s mouths without waking them. A few participants stated, My dentist told me about cleaning the mouth [of the child] after breastfeeding. That is all the information I got. How to do it, I do not know. My daughter’s pediatrician had told us that the child can be breastfed for any number of years but the baby should be made to drink water soon after feeding. But babies sleep off soon after feeding. It is difficult to make them drink water and then again put them to sleep.
Some parents understood that their infant feeding practices resulted in tooth decay, only after they visited the pediatric dentist regarding the complaint. One participant stated, Breastfeeding or bottle-feeding can cause cavities . . . this was told to me by child’s children’s dentist, when I took my child for treating her cavities.
However, most parents began brushing their child’s teeth by 1 to 1.5 y of age, and some parents were aware that brushing should begin when the first teeth erupt. Some acknowledged that they did not have the required knowledge to prevent caries in their children. Most of the participants were sad that their children had cavities that affected their families. One participant said, I feel we did not have much knowledge about how to prevent cavities. That is why my daughter got cavity problem or may be it is due to our negligence.
Discussion
This qualitative study was conducted with 27 parents of children with ECC, exploring their knowledge and perceptions of the infant feeding practices, their children’s feeding practices, and the challenges they faced with these feeding practices. Most of the participants said that their children were breastfed and believed breastfeeding to be better than bottle-feeding. The feeding practice, length of feeding duration, and weaning were adopted based on the guidance from the older women in the family or neighborhoods. Prolonged, bedtime feeding, at-will breastfeeding or bottle-feeding, and putting the infant to sleep while feeding were standard practices. As the children weaned off the breast, sweetening drinks was common, despite the parents knowing that such practices could result in dental caries. Many parents faced challenges with weaning and were unaware of infant oral hygiene practices.
Although most of the participants were aware that any milk could increase the risk for caries, they breastfed or bottle-fed their children mainly to soothe or comfort them when upset or as a means to put them to sleep. While breastfeeding per se may not be cariogenic, breastfeeding beyond 12 mo of age coincides with the window of infectivity of the cariogenic bacteria during the eruption of primary teeth (Holgerson et al. 2013; Tham et al. 2015). Breastfeeding beyond 12 mo of age, coupled with exposure to sugar in the diet during weaning, and poor oral hygiene practices led to ECC (Tham et al. 2015; Devenish et al. 2020). A similar practice was observed by most of the parents who participated in our study.
Studies have reported that infant formulas are more cariogenic than breast milk due to the high-sucrose sugar content (Erickson et al. 1998; Peres et al. 2009). Bottle-feeding has been shown to be more cariogenic than breastfeeding (Avila et al. 2015), especially if bottle-feeding is combined with breastfeeding beyond 12 mo of age (Feldens et al. 2018). Cariogenicity increases when the infant falls asleep with the formula-filled bottle in their mouth because it can cause stagnation of milk against the upper incisors (Erickson et al. 1998). Contrary to breast milk, bottle-feeding does not favor the growth of bacteria that suppress the growth of caries causing bacteria such as Streptococcus mutans (Holgerson et al. 2013). Only a few of our participants reported using infant formula in bottles. However, those children were falling asleep with the bottle in their mouths. Some of our participants used a combination of breastfeeding and bottle-feeding, although many reserved bottle-feeding for when they had to go out with their children. Bottle-feeding was preferred, as breastfeeding in public is culturally acceptable in the study location, but only if done discretely (Komodiki et al. 2014).
During weaning, most participants reported adding sugar to cow’s milk while shifting to cups, which they perceived to be more palatable for their child. It is known that sugary drinks increase caries risk in infants and toddlers when fed with or without using bottles (Evans et al. 2013). Parents fed their children sugary drinks even after knowing that sugary drinks increase the risk for caries. Even though parents were aware of the cariogenic effects of nighttime feeding, they let their children sleep without any oral hygiene measures. Parents did not know how to initiate oral hygiene for their children during early infancy. This pattern of behavior has been noted in other populations also, which was attributed to the compassion or convenience of the parents (Lotto et al. 2020).
Most of the study participants were not aware of the implications of infant feeding practices on dental caries. This was mainly because they only learned about feeding norms from older women in the family. This kind of behavior is not atypical to the Indian population included in the study, and it has been observed in the past (Cidro et al. 2015). Our study participants lacked anticipatory guidance from pediatricians or pediatric dentists regarding healthy feeding practices, weaning to solid foods, and maintaining children’s oral hygiene during infancy. Those who did hear about feeding duration from pediatricians and pediatric dentists received conflicting information. Such conflicts have been reported in the past (Naidu et al. 2012). Pediatricians are the first contact for mothers after childbirth. Hence, they are in an excellent position to provide anticipatory guidance regarding infant oral care. However, a consensus is required between pediatricians and pediatric dentists’ professional organizations regarding duration and frequency of feeding, how to initiate oral hygiene, and the weaning process (Gillham et al. 2019). Participants were aware of the risk that nighttime or bedtime feeding and providing sugary drinks poses for the development of caries. However, they were unable to translate their knowledge into action, reflecting a lack of self-efficacy.
Given the severe impact of the ECC, preventive programs should target pregnant women and young parents and incorporate anticipatory guidance from pediatricians and pediatric dentists, with collaboration between the 2 professions. The anticipatory guidance should emphasize breastfeeding up to 6 mo, discourage bedtime breastfeeding beyond 12 mo of age, begin oral hygiene practices before the teeth erupt, begin tooth brushing as and when the first tooth erupts, choose a diet low in sugar at weaning, and be cautious about the sugar content in their children’s foods and drinks. To enhance self-efficacy, motivational interviewing for young parents to modify attitudes and adopt healthy infant feeding practices is required (Vamos et al. 2015). In accordance with Levin et al. (2017), considering the important role of older women in establishing feeding practices and weaning, all community education should target both older women and young parents. Considering there is no remedy that fits all, it is essential to understand the social, cultural, and family dynamics while developing targeted interventions at local or regional community levels. National and global recommendations on the planning and implementation of preventive programs should emphasize the exploration of the knowledge and attitudes of the local population, along with the challenges they face. Further studies into the experiences of caregivers of children without ECC will better our understanding of the implementation of preventative methods for ECC. The following limitations should be considered while interpreting our study observations. As the participants in the study were parents who sought dental treatment for their children, the findings of this study may not reflect the findings of the parents who did not seek dental care for their children. The dental institution where the study was conducted provides access to a majority of the population in the region. However, due to the academic nature of the institution, some parents may face challenges in accessing the institution for the required care. In addition, those who declined to participate in the study may have had different knowledge, attitudes, practices, and challenges. Thus, our observations may not accurately reflect the knowledge and beliefs of the entire population of parents of the ECC children in the region. The findings are reflective of a section of parents of Indian children with ECC with similar characteristics. The data were collected through focus groups, and thus, the participants’ responses may have been influenced by group dynamics and the desire to appease the moderator. However, we took care to encourage the participants to speak without fear of judgment. Nevertheless, we used the descriptive qualitative design that provides an advantage to stay close to the data and present our observations using the participants’ voices. In addition, the focus groups provided an opportunity to gather data from many participants in a short period with group interactions. Given the nature of qualitative research, bias is inevitable, and thus, generalizability is not expected. Although we intended to establish the credibility of our research through member checking and through repeat focus groups, it was not feasible due to the time constraints of the participants. Nevertheless, we maintained the robustness of our study by maintaining a detailed audit trail of our coding to increase the transparency of our analyses.
Conclusion
In children with ECC, infant feeding practices were commonly prolonged beyond the required age, including bedtime feeding. In addition, parents of children with ECC appeared to have acquired knowledge regarding infant feeding practices from the older women in the families or neighborhoods, which are based on perceptions and may not be evidence based. They faced significant challenges during weaning and were unaware of infant oral hygiene practices. Although the participants knew the role of sugar in tooth decay, they lacked self-efficacy to translate their knowledge into action.
Author Contributions
B.S. Suprabha, contributed to conception, design, data acquisition, drafted and critically revised the manuscript; R. Shenoy, contributed to data conception and design, critically revised the manuscript; K.Y. Mahabala, A.P. Nayak, contributed to data acquisition, analysis, and interpretation, critically revised the manuscript; A. Rao, contributed to data acquisition, critically revised the manuscript; V. D’Souza, contributed to design, data analysis and interpretation; critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors thank all study participants for their time and commitment and the Manipal College of Dental Sciences, Mangalore, for providing facilities to conduct the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partly sponsored by Canixa Life Sciences Pvt. Ltd., New Delhi (CI U24233DL2007 PT C163800), which covered the cost of the oral hygiene kits and the travel allowance that were given to the participants, as well as the refreshments that were served during the focus groups. None of the researchers received direct or indirect payments of any kind from the sponsor.