
Abstract
Introduction:
The Rocky Mountain Network of Oral Health is 1 of 3 regional projects funded by the Health Resources and Services Administration (2019 to 2024) focusing on caries prevention through medical-dental integration (MDI) in community health centers (CHCs). MDI models included provision of preventive oral health services (POHS) at medical visits by the medical team (model 1), by integrated dental hygienists (DHs; model 2), or a hybrid of these models (model 3). The overarching aim is to evaluate the effectiveness of these models on 3 objectives: (1) ≥50% receive POHS, (2) ≥75% with high caries risk receives dental referral, and (3) ≥30% of parents/caregivers set an oral health goal for the child.
Methods:
Primary care association practice facilitators (PFs) recruited 22 CHCs to participate from Arizona, Colorado, Montana, and Wyoming. CHCs completed oral health needs assessments prior to participating. PFs coached CHCs using an MDI change package. CHCs submitted monthly and 6-mo, aggregated, deidentified population metrics for children aged 0 to 40 mo receiving well-child care visits. Monthly CHC-specific reports were used by PFs with teams in continuous quality improvement activities. POHS delivery trends over time were assessed using a linear mixed model, adjusting for number of eligible patients during each 6-mo reporting period.
Results:
Participating CHCs were urban (55%), rural (36%), and frontier (8%). Twelve (55%) had co-located dental clinics. Ten CHCs implemented model 1, 5 implemented model 2, and 7 implemented model 3. From September 2020 to August 2023, CHCs reported providing 91,604 POHS to eligible children. After adjustment, there was significant improvement over time for all objectives: objective 1: F(5, 90) = 4.66, P = 0.0008; objective 2: F(5, 90) = 2.99, P = 0.0151; objective 3: F(5, 90) = 4.56, P = 0.0009.
Conclusions:
The implementation of 3 MDI models across 22 CHCs in 4 states resulted in a meaningful increase in POHS delivery. POHS delivery by both medical and embedded DHs was associated with the most substantial increase in POHS delivery.
Knowledge Transfer Statement:
The results of this study can be used by medical and dental providers when deciding which approach they wish to use when planning the delivery of preventive oral health services at medical visits.
Introduction
Disparities in oral health and access to dental care persist across various populations, reflecting socioeconomic, racial, and geographical differences (Dye et al. 2007). Limited access to preventive and restorative dental services exacerbates these disparities, disproportionately affecting marginalized communities and underserved populations (Northridge et al., 2020). Factors such as income, insurance coverage, and geographical location influence an individual’s ability to access timely and adequate dental care (Schrimshaw et al., 2011; Northridge et al., 2020). This inequitable distribution of oral health resources contributes to disparities in outcomes, with certain groups, including young children, experiencing higher rates of caries and related complications (Beltran-Aguilar et al., 2005; Dye et al. 2007).
There is an emerging opportunity to integrate oral health services into medical visits, thereby reaching a broader population and potentially addressing disparities in accessing dental care. Leveraging primary care settings to deliver preventive oral health services (POHS), such as fluoride varnish and oral health education, presents a promising strategy. (Pahel et al. 2011) Integrating oral health into primary care not only enhances accessibility but also emphasizes the interconnectedness of oral health with overall health and is patient centered. By leveraging existing medical infrastructure, this integration could effectively address disparities in dental care access and contribute to improved oral health outcomes for diverse populations. (Quinonez RB et al. 2006) There is a gap, however, in our understanding of models implementing medical-dental integration (MDI).
The Rocky Mountain Network for Oral Health Integration (RoMoNOH) aims to integrate POHC into community health centers (CHCs) and address disparities in oral health care access, promote oral health services at medical visits, and foster collaboration among oral health professionals, health care providers, policy makers, and community organizations. CHCs play an important role in providing POHS to low-income families with limited access to dental care. The overarching aim of the RoMoNOH was to increase delivery of POHS to young children receiving primary medical care in CHCs through 3 models of care delivery including POHS delivered by medical providers, dentals hygienists (DHs) embedded in the medical team, and/or a hybrid of these 2 approaches.
Methods
Project Overview
The RoMoNOH is 1 of 3 Networks for Oral Health Integration funded by the United States Department of Health and Human Services Maternal and Child Health Bureau, with the overarching goal of improving the oral health of young children aged 0 to 3 y through the provision of POHS during medical primary care visits (2019 to 2024). The RoMoNOH developed, implemented, and evaluated MDI models aimed at providing POHS, including caries risk assessment, oral health education, fluoride varnish application (FVA), dental referrals, and parental oral health goal setting (OHGS), to children during medical visits at 22 CHCs in Arizona, Colorado, Montana, and Wyoming. MDI models included POHS delivered by the medical team, a DH embedded in the medical team, or a hybrid of these two. A 4-state learning collaborative led the implementation of the RoMoNOH and was composed of a project director, project manager, data manager, subject matter experts, and state primary care association (PCA) practice facilitators (PFs) who were primarily responsible for facilitating MDI activities in participating CHCs.
CHC Recruitment
In 2019, PCA PFs recruited 22 CHCs to participate in the project (Arizona [8], Colorado [8], Montana [3], Wyoming [3]). Each CHC completed a baseline assessment to determine their community’s oral health needs, which assessed the CHCs’ unique annual patients (count), patients’ age distribution, medical and dental provider full-time equivalents, co-located dental clinics, and current delivery of POHS at medical visits.
The RoMoNOH used a quality improvement (QI) approach, guided by an MDI change package and its drivers and associated activities (Appendix). The MDI change package was developed from the evaluation of previous MDI efforts (Braun et al. 2013; Braun et al. 2016; Braun et al. 2023). The change package drivers included data-driven improvement, engaged leaders, engaged providers and staff, devoted time to drive practice change, and team-based care strategies.
Implementation
Provider education
PFs directed health care medical and dental team members to an on-demand eLearning training with 5 modules related to provision of POHS including Introduction to Oral Health, Clinical Skills and Integrating Oral Health, Oral Health Communication and Education, Interprofessional Collaboration, and Perinatal Oral Health. Users earned 1 continuing education credit per module upon completion.
Practice facilitation
PFs coached their state’s CHCs from September 2020 through October 2023 implementing MDI change package activities. Each PF supported 2 to 8 CHCs within their state. The PFs met with each CHC roughly monthly to review metric QI run charts and CHC’s progress toward reaching project objectives. PFs reviewed staff training and workflows on provision and documentation of POHS and extraction of discrete data from the electronic health record for reporting. PFs coached CHCs on identifying opportunities for POHS delivery and documentation improvement using a variety of pragmatic, nonscripted QI methods including Plan-Do-Study-Act, Lean, and Six Sigma (Christoff 2018; Ninerola et al., 2020; Ojo et al., 2022). The PFs completed monthly online coaching assessments, which quantified and summarized their coaching activities for each MDI change package driver. PFs provided 1,079.5 h of coaching to 22 CHCs from September 2020 through October 2023.
Project incentives
Each CHC received incentive benchmark payments for developing a population registry ($3,500), reporting accurate monthly metrics ($2,000/y), reaching objective 3 ($8,000), if 50% of children aged 24 to 40 mo received at least 3 FVAs within their lifetime ($8,000), and for demonstrated sustainability ($11,000). Evidence of sustainability included system changes to support ongoing provision of POHS (e.g., modifications of relevant policies and procedures, standards-of-care documents, standard oral health QI metrics, onboarding training, and optimization of the electronic health record).
Evaluation
Objectives
The project objectives focused on POHS delivery for young children attending primary well-child care visits (WCVs) and included (1) 50% receive any POHS, (2) 75% of children at high caries risk receive a dental referral to a dental provider, and (3) 30% of parents/caregivers completed OHGS.
Population
The target population of the project was children aged 0 to 40 mo receiving primary WCVs in CHCs. While most CHCs provided POHS to broader populations (e.g., older children, pregnant people), we intentionally focused our evaluation on young children. Eligible children included individuals aged 0 to 40 mo with a WCV in the reporting period and previous WCV at the reporting CHC.
Metrics
Metrics included monthly and 6-mo counts of unduplicated, eligible children seen in those reporting periods and counts of who received a caries risk assessment (CRA), dental referral, FVA, and parent OHGS on behalf of the child. Any POHS provided by a medical and/or dental provider in the reporting month was included. CHCs submitted aggregated, deidentified POHS metrics for eligible children through the REDCap database. The evaluation team developed a data dictionary with detailed definitions for each metric using existing medical and dental diagnoses and/or existing billing codes whenever possible, and proxy codes when needed. All CHCs had to optimize their electronic medical and/or dental record for metric documentation and data extraction. Each CHC was trained on metric definitions, provided support on developing a data-collection process, and was retrained with team-member turnover. The evaluation team conducted a quality check of each month’s metrics and reconciled data discrepancies whenever possible. Six-month reporting periods were August 2020 through January 2021, February 2021 through July 2021, August 2021 through January 2022, February 2022 through July 2022, August 2022 through January 2023, and February 2023 through July 2023.
Metric data analysis
We used descriptive statistics to summarize baseline CHC characteristics. The primary outcome for analysis of change over time was the number of eligible patients per CHC who met criteria for objectives 1 to 3 during each 6-mo period. The initial time period represents the 6 mo prior to the beginning of the intervention. All data were collected at the CHC level. We used general linear mixed effects regression models with random intercept for CHC, adjusting for the average number of eligible patients during each 6-mo time period. Time was coded as a categorical variable (0 to 5) to capture nonlinear change. We assessed overall improvement over time (main effect for time) as well as differential improvement by integration model type (time × model). Hypothesis tests were 2 sided with α = 0.05 or P values reported. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc.).
These methods comply with the STROBE protocol. The Colorado Multiple Institutional Review Board exempted this evaluation from human subjects research.
Results
CHC Baseline Characteristics (2018)
At baseline, 12 (55%) CHCs were in urban settings, rural 8 (36%), and frontier 2 (8%). The mean number of total annual unique patients receiving care in the participating CHCs was 8,938 (range 1,702 to 40,180). The average patient visits/day/CHC was 69 (range 9 to 294). Twelve (54%) had co-located medical and dental clinics, 7 (32%) had affiliated but not co-located dental clinics, and 3 (14%) had no affiliated dental clinic. One CHC did not provide care to young children but was preparing to soon. POHS were being provided in 8 (41%) of the CHCs, but the CHCs wanted to improve their POHS delivery. Seventeen (77%) had an integrated medical and dental record; 3 CHCs did not have any electronic dental record.
Provider Oral Health Education
A total of 287 unique members of the health care team completed at least 1 eLearning module. In total, 1,068 modules were completed (module 1: 249, module 2: 247, module 3: 205, module 4: 185, module 5: 172).
MDI Model
Twelve (55%) of the 22 CHCs selected to implement an embedded DH model. Of these, 5 implemented the RDH-only model in which CRA, FVA, and OHGS were provided by the embedded DH. Seven CHCs implemented a hybrid model in which some patients received POHS from the medical team and some by the embedded DH. At 2 CHCs implementing the hybrid model, the medical providers completed some of the POHS (e.g., CRA) and then referred the patient to the embedded DH who then provided additional POHS. In 1 CHC, the medical team coordinated with dental residents for POHS, rather than a DH. In the other 10 CHCs, the medical providers provided all the POHS.
Between September 2020 and August 2023, CHCs reported providing 91,604 POHS to children aged 0 to 40 mo (by state: Arizona [28,445], Colorado [59,403], Montana [1,200], and Wyoming [2,556]). Across the project, objectives 1 and 3 were achieved. Objective 1 (50% of eligible children receive a POHS at a medical visit) was met in the third of seventh 6-mo reporting periods and maintained thereafter (Fig. 1). Objective 2 (50% of children at high risk for caries receive a dental referral to a DH or dentist) was not met, but there was a steady increase over all seven 6-mo reporting periods (Fig. 1). Objective 3 (30% of parents of children set an OHG) was met in the fifth of seventh 6-mo reporting periods and continued to improve thereafter (Fig. 1). By CHC, 22 (100%) met objective 1, 17 (77%) met objective 2, and 18 (82%) met objective 3 (Table 1).
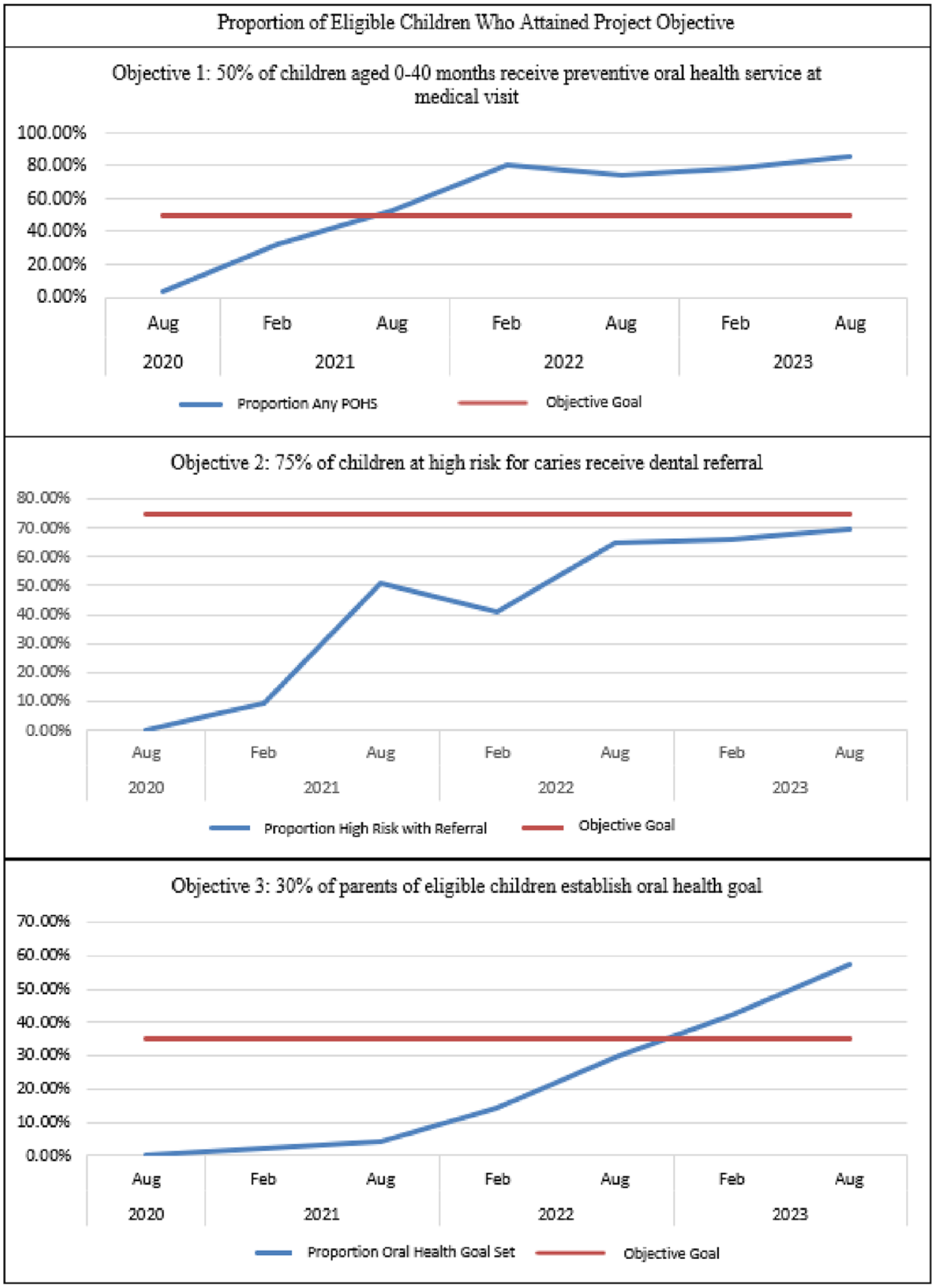
Proportion of eligible children who attained the project objective.
Community Health Centers’ Progress at Reaching Project Objectives (2019-2023).
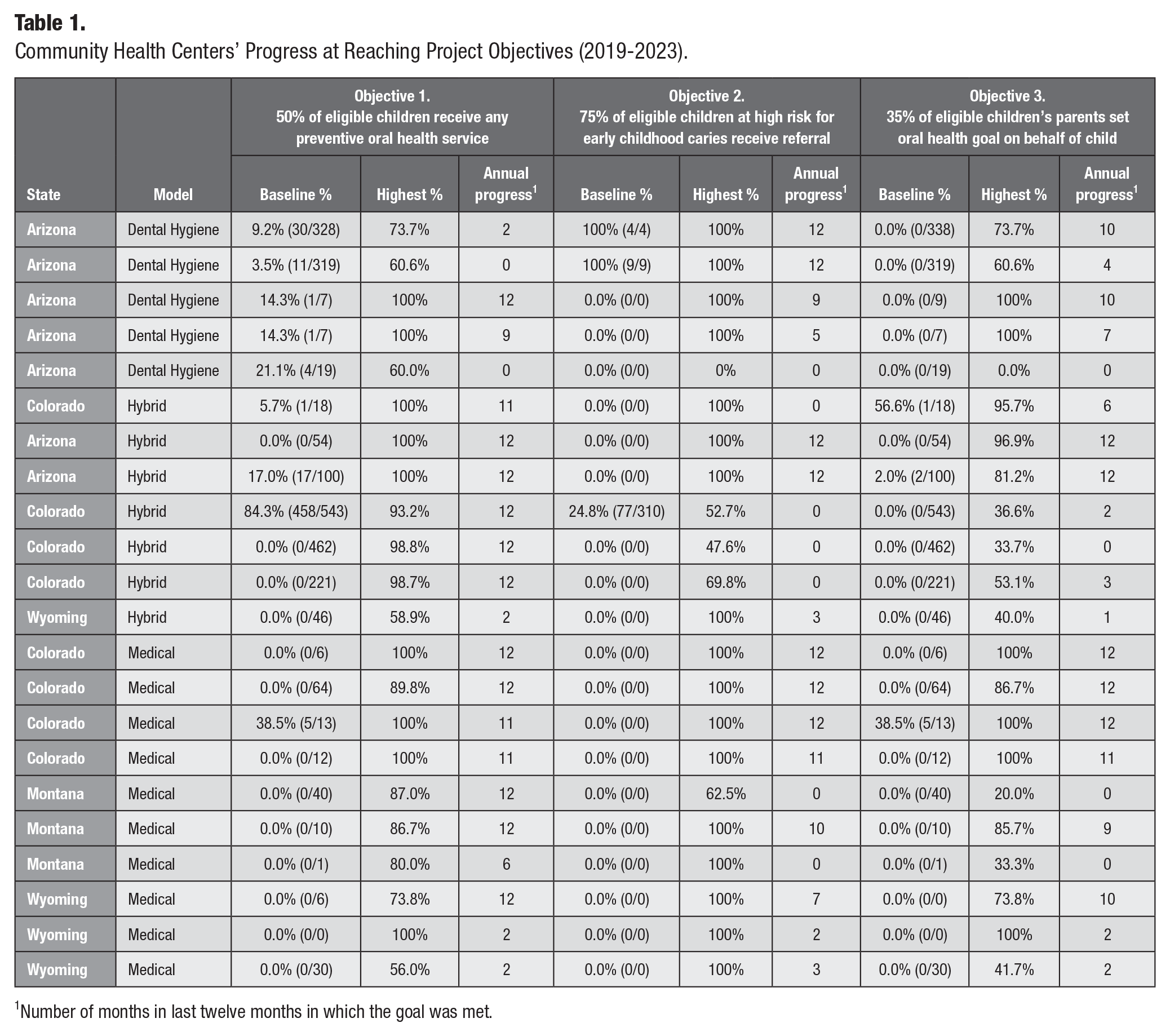
Number of months in last twelve months in which the goal was met.
Adjusting for the average number of eligible patients during each 6-mo reporting period, there was significant improvement over time for all project objectives (Fig. 2): objective 1: F(5, 90) = 4.66, P = 0.0008; objective 2: F(5, 90) = 2.99, P = 0.0151; objective 3: F(5, 90) = 4.56, P = 0.0009. When analyzing objective trends over time by implementation model, statistically significant differential changes for objectives 1, 2, and 3 (Fig. 3) were found: P = 0.004, P = 0.0071, and P = 0.0083, respectively. CHCs implementing the embedded DH model 2 had significant improvement for objective 3 (Fig. 3): P = 0.0395. CHCs implementing the medical/embedded DH hybrid model 3 had statistically significant change over time for all objectives (Fig. 3; P = 0.004, P = 0.0196, and P = 0.0072, respectively).
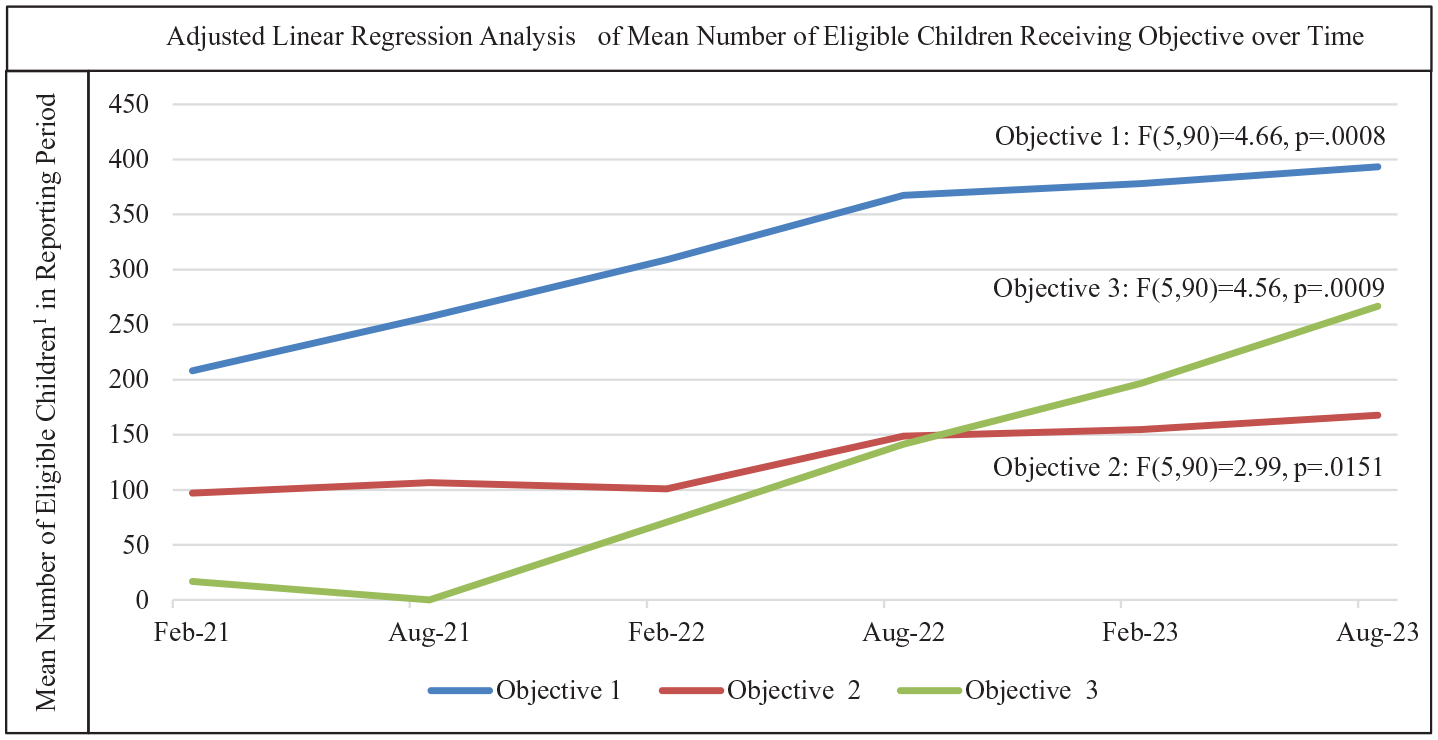
Adjusted linear regression analysis of the proportion of eligible children receiving preventive oral health services.
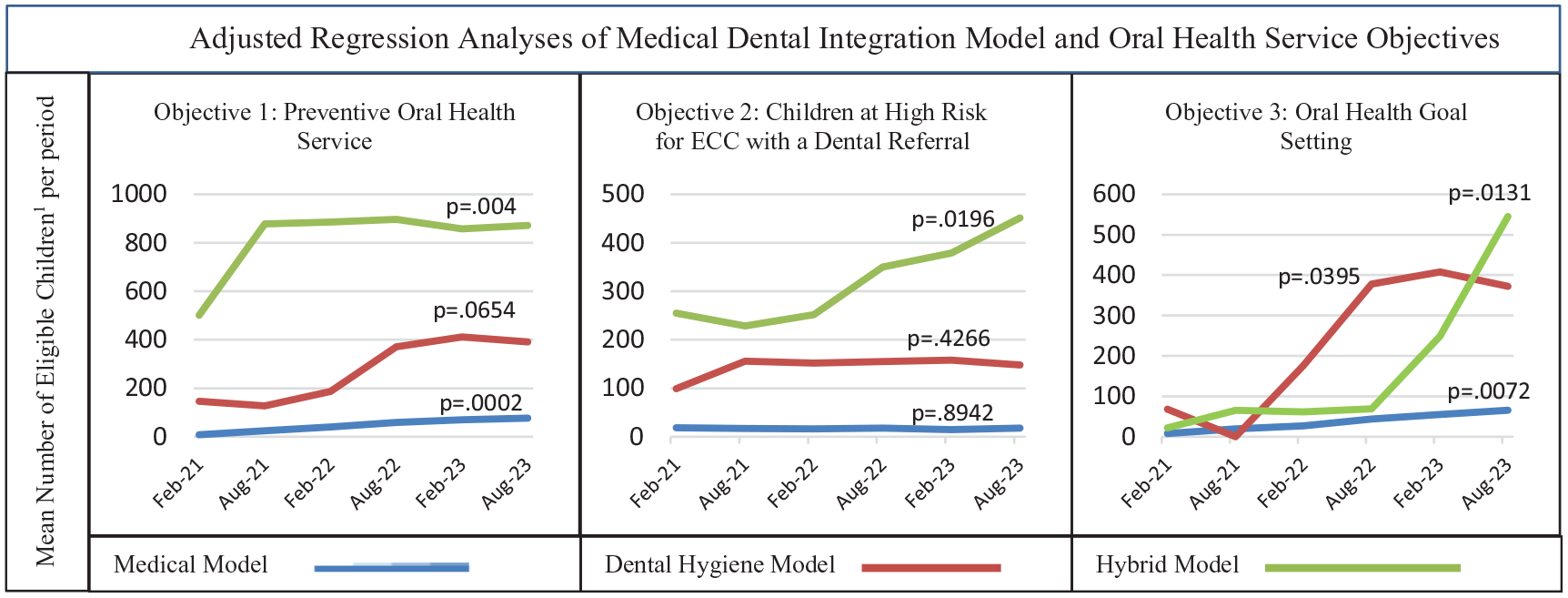
Adjusted regression analyses: associations of medical dental integration model and objectives.
Discussion
The overarching aim of this pragmatic MDI intervention was to increase delivery of POHS to young children aged 0 to 40 mo at medical WCVs in 22 CHCs in 4 states (2019 to 2023). Three POHS delivery models were implemented based on the CHC’s oral health needs and choice including delivery by medical providers (model 1), DHs embedded into the medical team (model 2), or a hybrid of these 2 models (model 3). Across the project, there were meaningful and statistically significant improvements in POHS delivery over time. The POHS delivery model was related to overall progress toward meeting project objectives with the hybrid model of POHS delivery by both the medical providers and embedded DHs reaching the most children.
This evaluation of 3 models of POHS care delivery in medical CHCs in 4 states contributes new findings to the growing literature describing MDI models. We have not found other comparisons of these approaches. The intervention’s use of pragmatic approaches/tools contributed to the successful implementation of the project and are replicable. These include the use of on-demand eLearning modules for educating medical and dental providers, the utilization of PFs from states’ PCAs with virtual coaching meetings that allowed for project implementation across a broad geographic area, and the 4-y duration allowing most CHCs sufficient time to implement the necessary changes they needed to make, including optimization of electronic health records for POHS documentation, hiring and onboarding of embedded DHs in models 2 and 3, and development of POHS-delivery processes and workflows.
The CHCs’ baseline characteristics influenced their POHS delivery model choice, which in turn influenced the adjusted regression analysis results. The 7 CHCs implementing the hybrid model were larger; consequently, more children received POHS across all objectives. Alternatively, the 10 CHCs implementing the medical model were small with similar influences. In CHCs implementing the medical model, statistically significant improvements were found in the number of children receiving any POHS (objective 1) and OHGs specifically (objective 3). However, the small subset of children documented to be at high ECC risk (objective 2) seen at these CHCs likely influenced this result. Five CHCs implemented the dental hygiene–only model—2 of which were larger and 3 smaller. In these CHCs, the DHs provided care to a subset of patients referred to them by the medical team. The lack of statically significant improvements for objectives 1 and 2 in the DH-only model is likely influenced by the higher number of children seen in these CHCs who did not receive any POHS in the CHC. These children were generally cited to have an outside dental home where they were already receiving POHS. Hence, the CHCs’ size and the oral health needs of the population they serve influenced the MDI model they implemented and emphasizes that no one model fits all CHC’s oral health needs. Larger CHCs may benefit from implementing a hybrid model, and smaller CHCs can still see improvement by engaging their medical providers in the POHS delivery.
This evaluation has limitations. First, the intervention’s pragmatic nature permitted measurement of progress toward attaining project objectives over time; however, it lacked a direct comparison group. CHCs were not randomized to POHS delivery model; therefore, the observations that CHCs implementing certain models had greater improvement does not constitute causal inference about which model is best. Associations between model and results may be influenced by additional factors we have not assessed such as oral health need and/or change package activities. In addition, we did not measure the intervention’s impact on caries. CHCs reported aggregated, deidentified measures/metrics extracted from the electronic health records rather than patient-level data, which limited our ability to track an individual patient’s experience over time. Furthermore, it describes high-level results of a large intervention but does not describe the variety of real-world activities that occurred within CHCs during a major global event (i.e., the COVID-19 pandemic) that are likely to have influenced the intervention’s progress. Further evaluation of the RoMoNOH approach is warranted to better understand factors contributing to our results.
This project relates to previous MDI published work that describes various examples of “medical dental integration.” MDI describes a range of models including medical and dental care provided in co-located settings (Braun et al., 2013; Pourat et al., 2015), POHS delivery by medical providers (Braun et al., 2017; Close et al. 2010), or delivery of dental services by DHs embedded into primary care medical teams (Braun et al., 2013; Braun and Cusick 2016; Braun et al., 2021). Our findings provide new contributions to the growing body of MDI evidence. An environmental scan by Atchison et al. (2018) of U.S. MDI activities with publications from January 2000 through August 2017 categorized services as POHS provided by medical care providers, POHS provided by dental providers in nondental settings, preventive health services provided by dental providers, or care coordination using dedicated personnel and technology. Atchison et al. highlighted 4 different programs including a large state program that supports medical providers in POHC delivery; a referral program for patients with diabetes identified in the medical setting; a coordinated care organization, which used dedicated patient coordinators, technology, and coordinated payment and referral mechanisms to facilitate care; and a small program describing a DH embedded in an OB/GYN clinic. They concluded that the integration of dental and medical care increased access to and coordination of patient care by means of offering health care services traditionally provided by the other profession but highlighted that additional evaluations of MDI programs and MDI studies are needed. In a 2022 scoping review by Gupta et al. (2022), the authors cited a gap in descriptions of MDI implementation approaches. They reviewed 16 articles and concluded there is need for additional studies and descriptions of MDI models to inform policy and practice (Gupta et al., 2022). Our work of implementing 3 MDI models within 1 program across a large geographic region is novel and contributes to filling the MDI evidence gap.
The effectiveness of caries prevention of FVA by primary care providers to children aged 0 to 5 y is evidenced by the U.S. Preventive Services Task Force’s recommendation B for FVA by medical providers to young children under age 5 y in 2014 and again in 2021 (Clark and Braun 2021). Barriers to provision of POHS by medical providers historically include difficulty in applying the varnish, integration of the dental procedures into practice, resistance among staff and colleagues, and dentist referral difficulties (Lewis et al., 2005; Close et al., 2010), but barriers to this approach have not recently been investigated, which is a knowledge gap that warrants new investigation. Our evaluation contributes to the literature describing the implementation of MDI models to support medical practices in providing MDI care and has potential to reduce cited barriers. Understanding these barriers may also lend insights into future oral health promotion opportunities targeting medical providers, including their use of silver diamine fluoride to manage caries.
Our findings also contribute to descriptions of embedding DHs into medical teams. The integration of dental providers into medical care teams is an emerging model with promise to increase access to dental services and prevent and reduce caries (Braun et al. 2023). Dental hygiene practice acts vary by state with direct access to DHs permitted in 42 states (American Dental Hygiene Association 2023). The embedded DH approach focuses on bringing dental care to patients rather than referring patients out for care, similar to integrated behavioral health care. The embedded DH model has potential to increase access to dental services given the historical siloing of medical and dental care and the lack of mechanisms to coordinate medical-dental care.
The integration of the provision of POHS into primary care through any MDI approach requires the buy-in of medical and dental providers, as well as system leaders to advocate for system-level changes required for efficient integrated care workflows. Health care systems without these drivers have a higher chance of experiencing barriers, resulting in lack of MDI adoption and sustainability. Emerging evidence supports MDI through various approaches. Medical practices can benefit from reviewing their patient’s current oral health care needs and access to dental services in their communities and identifying approaches to fill gaps and coordinate medical and dental care. Advocating for the electronic health information exchange between medical and dental providers will support MDI models, as will integrating payment systems for services. In addition, our findings contribute established processes and infrastructure to national “recognition programs,” such as those used in the National Committee for Quality Assurance’s Patient-Centered Medical Home integration of behavioral healthcare services (Philip 2019).
Conclusions
This MDI intervention aimed to enhance the provision of POHS to young children in 22 primary care CHCs. Implementing 3 POHS delivery models tailored to CHC needs, the intervention was associated with significant improvements in POHS delivery over time. The hybrid model, integrating both medical providers and embedded DHs, emerged as an important factor influencing impact. The intervention’s alignment with FVA application recommendations by medical providers to young children underscores its significance in advancing oral health care practices. Furthermore, the integration of DHs into medical teams holds promise in enhancing access to dental services. Successful MDI approaches require gathering support from medical and dental teams, along with leadership advocacy for systemic changes. This necessitates a concerted effort to identify gaps, facilitate care coordination, advocate for health information exchange, integrate payment systems, and establish recognized processes like other health care recognition programs.
Author Contributions
P.A. Braun, C. Flowerday, A. Bienstock, T. Callaghan, K. Freeman, M. Gable, L. Ramirez, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; L.M. Dickinson, contributed to conception, design, data analysis and interpretation, drafted and critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of work.
Supplemental Material
sj-doc-2-jct-10.1177_23800844241273771 – Supplemental material for Delivery of Oral Health Services at Medical Visits through 3 Medical Dental Integration Models
Supplemental material, sj-doc-2-jct-10.1177_23800844241273771 for Delivery of Oral Health Services at Medical Visits through 3 Medical Dental Integration Models by Lisa J. Heaton, Tamanna Tiwari, Eric P. Tranby, P.A. Braun, C. Flowerday, A. Bienstock, T. Callaghan, K. Freeman, M. Gable, L. Ramirez and L.M. Dickinson in JDR Clinical & Translational Research
Supplemental Material
sj-pdf-1-jct-10.1177_23800844241273771 – Supplemental material for Delivery of Oral Health Services at Medical Visits through 3 Medical Dental Integration Models
Supplemental material, sj-pdf-1-jct-10.1177_23800844241273771 for Delivery of Oral Health Services at Medical Visits through 3 Medical Dental Integration Models by Lisa J. Heaton, Tamanna Tiwari, Eric P. Tranby, P.A. Braun, C. Flowerday, A. Bienstock, T. Callaghan, K. Freeman, M. Gable, L. Ramirez and L.M. Dickinson in JDR Clinical & Translational Research
Footnotes
Acknowledgements
The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by the Health Resources and Services Administration, U.S. Department of Health and Human Services, or the U.S. government. We would like to acknowledge and thank all our partner CHCs, the Network for Oral Health Integration Learning Collaborative, and the RoMoNOH Steering Committee members for their support of this work. None of the authors have any conflicts of interest. All authors contributed to this work and have given full approval and agreement to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Health Resources and Services Administration of the U.S. Department of Health and Human Services as part of an award totaling $6.4 million with zero percent financed with nongovernmental sources.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.