
Abstract
Introduction:
In 2011, the Institute of Medicine (IOM) recommended a minimum of 4 clinical oral health competencies for nondental professionals to promote optimal oral health, including (1) recognizing risk for oral disease through competent oral examinations and (2) making and tracking referrals.
Objectives:
We determined whether California school nurses (SNs) knew about specific components of the 2 IOM competencies mentioned above using 3 clinical case scenarios following the Association of State and Territorial Dental Directors Basic Screening Survey Methodology.
Methods:
In this cross-sectional study, a 23-item pilot-tested online survey was completed by 358 active California School Nurses Organization members between April and June 2023. We conducted univariate, bivariate, and multivariable linear regression analyses.
Results:
For the first scenario, 61% of SNs correctly identified the condition as “root tips,” with 93% indicating correctly that such a case should be referred immediately. In the second scenario, almost 77% of SNs correctly identified “untreated tooth decay,” with 50% correctly suggesting that a child with untreated tooth decay without dental pain should visit a dental office within several weeks. In the third scenario, almost 50% correctly identified an abscessed tooth, with 75% indicating that a child with this condition should be referred immediately. Multivariable adjusted linear regression analysis showed that SNs with a bachelor’s degree or lower had significantly lower overall knowledge in accurately identifying dental conditions and choosing appropriate dental referrals (P = 0.02).
Conclusions:
At least half of the participating SNs accurately identified the dental conditions and chose the appropriate dental referrals. The educational status of SNs was a strong predictor of SNs’ overall knowledge of identifying oral health conditions and appropriate dental referrals. SNs, when adequately trained, can assess oral health needs and make appropriate dental referrals as part of school-linked dental programs.
Knowledge Transfer Statement:
SNs can identify common dental conditions in children and appropriately refer them to a dental professional. When adequately trained, they can be a valuable resource in implementing school-linked dental programs.
Keywords
Introduction
Dental caries remains the most common chronic childhood disease (National Institutes of Health, 2021). Dental caries in children have many harmful effects, including oral pain, difficulty focusing, missed school days, not performing well academically, and lower self-esteem (Guarnizo-Herreño and Wehby 2012; Seirawan et al. 2012; Detty and Oza-Frank 2014).
Identifying dental caries and preventing its progression and morbid health consequences can be achieved if school children have regular access to a trained health professional within the school premises who can perform a simple oral health screening, identify the dental condition, and appropriately refer them to dental professionals for further treatment. The school nurse (SN) may be the first person a child encounters to seek any services when in need of health care within a school environment. Nondental professionals such as SNs can take a role in improving the oral health care of school children.
The National Association of School Nurses (NASN) endorsed a policy statement by the American Academy of Pediatrics that highlighted the critical role of SNs in the early identification of dental problems (Moysés et al. 2003). SNs are crucial health care team members who can raise awareness of establishing a dental home for children (Wright 2015). The Institute of Medicine (IOM; now referred to as the National Academy of Medicine) recommended a minimum set of core clinical oral health competencies for nondental professionals, who, when trained in these competencies, will be able to promote optimal oral health, be a valuable source in oral health needs assessment, and make appropriate dental referrals based on current oral health needs (IOM and National Research Council 2011). These competencies include (1) recognizing the risk for oral diseases through competent oral examinations, (2) providing basic oral health information, (3) integrating diet and lifestyle counseling with oral health counseling, and (4) being able to make and track referrals to dental professionals when a person is in need for dental care.
Few studies show that SNs can effectively identify oral health complications in school children. SNs, in a Texas-based study, effectively identified various oral health conditions, including toothaches, loose teeth, periodontal problems/bleeding gums, hygiene problems, orthodontic complications, and crooked teeth or malocclusion (Peterson et al. 1999). In another study in which SNs performed oral health needs assessment of third- and sixth-grade children, 82% of referred school children with dental needs received dental care from dentists, suggesting SNs can contribute to the early detection of dental caries and referrals (Tetuan et al. 2005).
More than 60% of California third graders (2018–2019) experienced dental caries (Darise et al. 2021). This prevalence rate is much higher than the national prevalence (2011–2016) of 52% in children 6 to 8 y old (Centers for Disease Control and Prevention 2021). The rate of untreated dental caries was as high as 22% in California third graders, indicating unmet dental needs in these children (Darise et al. 2021). SNs in California schools can be a great resource in performing oral health needs assessment and dental referrals as part of routine health care screening in school children, thereby identifying dental caries and other oral conditions as early as possible. However, to conduct successful oral health needs assessment and dental referrals, California SNs should be competent in at least 2 of the 4 IOM-recommended clinical oral health competencies for nondental professionals. Therefore, we determined if California SNs are knowledgeable in (1) identifying common oral diseases and (2) choosing appropriate dental referral recommendations for those dental conditions. We also determined if SNs were willing to perform annual oral health screenings. In addition, we wanted to determine factors that predict SNs’ overall knowledge in identifying common oral diseases and choosing the appropriate dental referral recommendations.
Materials and Methods
The University of California, Los Angeles, Office of the Human Research Protection Program determined that the study meets the criteria for an exemption from Institutional Review Board (IRB) review (IRB No. 23-000177). We formatted this article using STROBE guidelines (von Elm et al. 2007).
Survey Instrument
For this cross-sectional study, we administered an adapted version of a 23-item survey to 1,738 California School Nurses Organization (CSNO) members. The 23-item survey was adapted from a previously pilot-tested survey administered to Pennsylvania School Nurses Association and Practitioners (PSNAP) members in 2018 (unpublished data). Before conducting the study with PSNAP members, the survey was tested for face and content validity and test-retest reliability. The survey was first sent to 3 dental public health experts to derive feedback on the survey structure and content. After integrating the input from the experts, the survey was tested with 12 SNs. The same survey was administered among 12 SNs after 3 wk. We tested their responses with 3 major clinical case scenarios (assessed through 6 questions). The Cohen’s kappa for test-retest reliability ranged between 0.78 and 0.85, indicating a minimum of a moderate level of agreement across all 6 questions (McHugh 2012). This same survey, administered to PSNAP members, was also used for the study with CSNO members.
We used 3 clinical case scenarios, using images of specific dental conditions/diseases from the Association of State and Territorial Dental Directors (ASTDD) “Basic Screening Survey: An Approach to Monitoring Community Oral Health” report (ASTDD 2022). This document is available for public use for a fee, and permission to use images from this document was obtained. In the first scenario, SNs viewed an image of root tips due to tooth decay. In the second, SNs viewed an image of a tooth with untreated decay, and in the third, an image of an abscessed tooth. To clarify what specific condition they were looking at, the conditions/images were illustrated with black arrows pointing toward the lesion/condition. After viewing each image, the CSNO members were asked to identify the correct dental condition/disease shown in that image using a multiple-choice response question. After identifying the condition/disease for each image, SNs were asked to choose the correct referral recommendation for each of the 3 dental diseases/conditions using a multiple-choice response question. SNs were also asked if they would perform annual oral health screenings for children in the schools where they work (yes/no). The survey also asked demographic questions about the SNs: age, race, ethnicity, education level, and number of schools they work at.
Data Collection
We used standard guidelines to improve the online survey response rates (Dillman et al. 2009). The survey was first adapted into an online version using the Survey Monkey online platform, and a data collection link was created. The CSNO maintains an updated email list of its members. We requested CSNO to send the online survey link to their active members (N = 1,738) as of April 2023. CSNO sent its members the first email announcement with the online survey link in mid-April 2023. CSNO sent the first email reminder 2 wk after the initial email announcement. The second reminder was sent in mid-May, and the final reminder was sent by the end of May 2023. The survey was open until the end of June 2023. The SNs were first asked to consent to take the survey.
Data Management and Analysis
The sample was categorized into those working at 1 school versus more than 1 school. The SNs were also classified based on their educational status into those with a bachelor’s degree and lower versus those with a master’s degree and higher. A cumulative response score variable was created for overall knowledge in identifying oral health conditions and selecting appropriate dental referrals by summing all the “correct” responses for the 3 oral health condition scenario questions and the 3 corresponding referral recommendations (cumulative score range: 0 to 6). A higher score would indicate a higher overall knowledge.
We ran descriptive statistics to understand the respondents’ characteristics. Frequencies and percentages were used to describe categorical variables, while mean and standard deviations were used for continuous variables. Bivariate comparisons of SNs’ knowledge of oral health conditions and appropriate dental referrals were tested using chi-square and Fisher exact tests. We used a multivariable-adjusted linear regression analysis to predict higher overall knowledge of SNs in correctly identifying common oral health conditions and appropriate dental referrals. The following variables were included in the model: age (as a continuous variable), race (all other races versus non-Hispanic Whites), ethnicity (Hispanic/Latino versus non-Hispanic/non-Latino), educational status of SNs (bachelor degree and lower versus master degree and higher), number of schools where they work (1 school versus more than 1), and willingness to conduct annual oral health screening for children (yes versus no). We used SAS v9.4 statistical software to run the analyses. We determined that a sample size of 103 was sufficient to run a fixed linear regression model with 7 independent predictors by conducting a priori power analysis with 80% power, ∝ = 0.05, with a medium effect size of 0.15.
Results
Of 1,738 CSNO members, 391 SNs consented to take the survey. All of the responses were collected through the Survey Monkey portal and stored in an in-built database. Of 391 SNs who consented to the study, only 358 completed it, with an overall response rate of 20.6%.
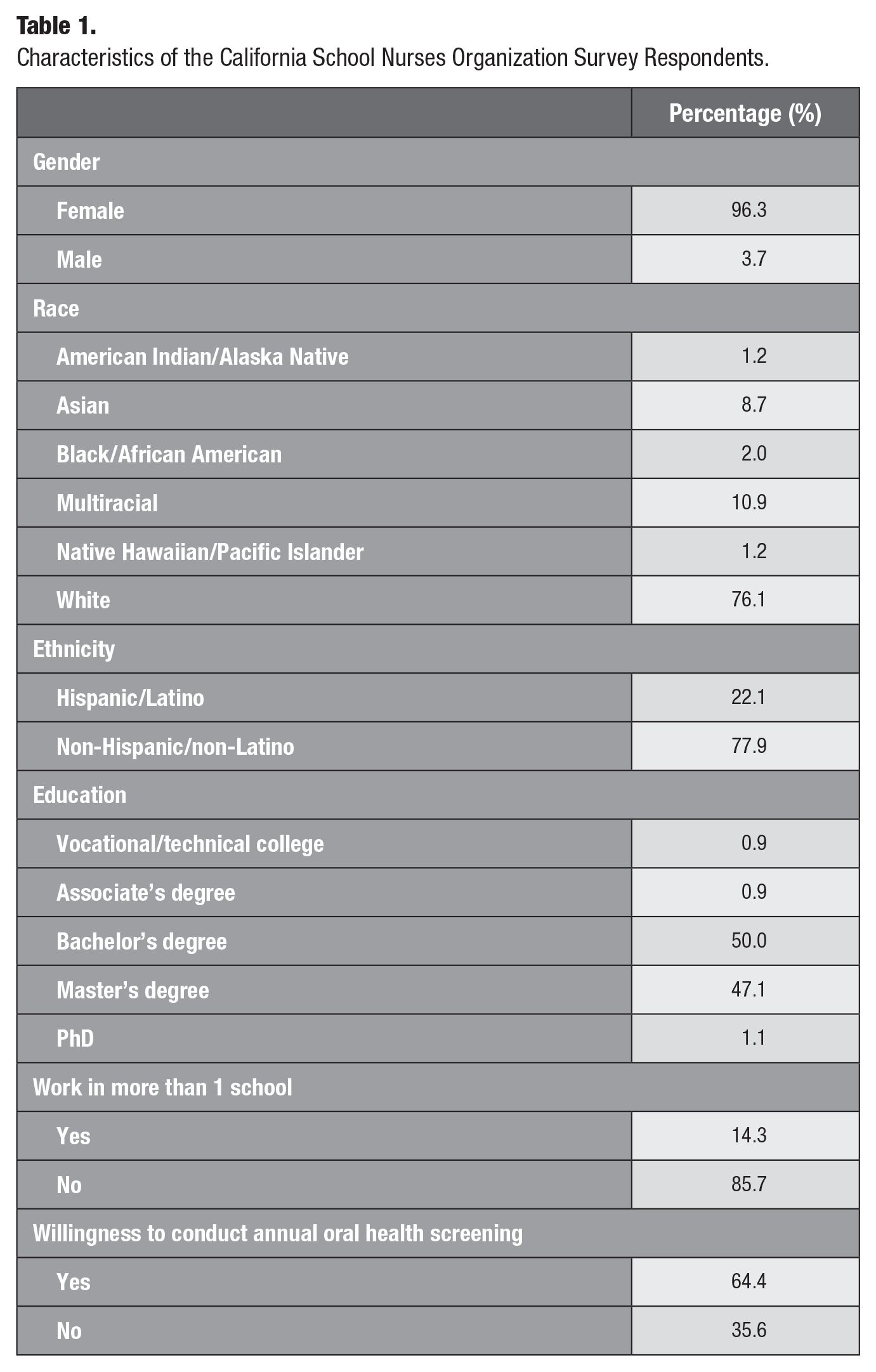
The mean age of the CSNO respondents was 49.0 ± 11.9 y. Most of the CSNO survey respondents were female (96%), White (76%), and non-Hispanic/non-Latino (78%). Almost 50% had attained a bachelor’s degree, and 47% had a master’s degree (Table 1). On average, the SNs responded that they worked at a minimum of 5.3 ± 5.0 schools. Nearly 85% reported working in more than 1 school at a time.
Characteristics of the California School Nurses Organization Survey Respondents.
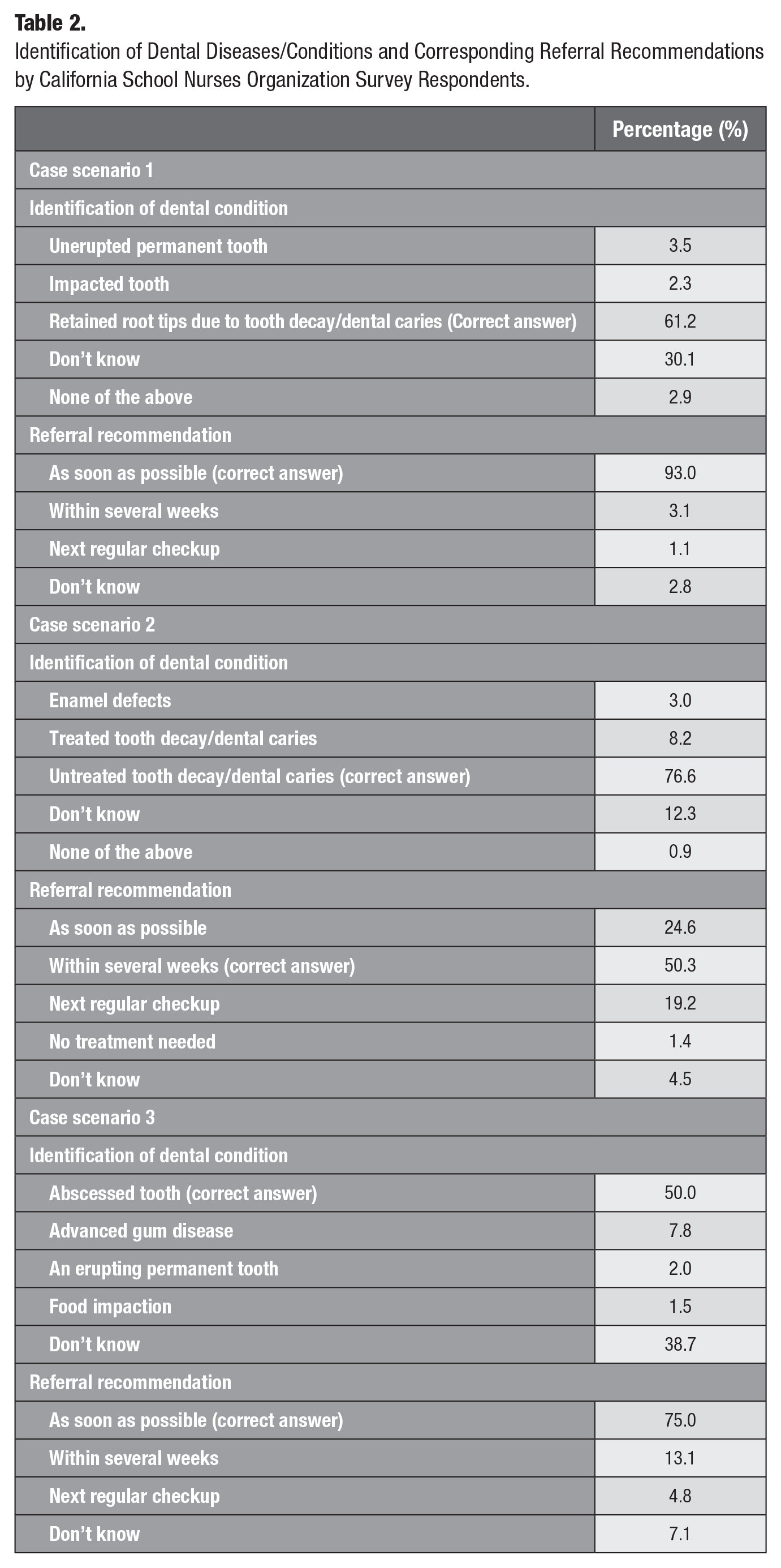
For the first scenario, 61% of SNs correctly identified the condition as “root tips” due to tooth decay. When asked about the appropriate referral recommendation for the condition, 93% of nurses correctly indicated that a child with such a condition be referred to a dental professional immediately. In the second scenario, approximately 77% of SNs correctly identified the condition as “untreated tooth decay,” with only 50% indicating that a child without dental pain visits a dental office within the next several weeks (Table 2). In the third scenario, half of the SNs (50%) correctly identified the condition as an “abscessed tooth,” with most (75%) indicating that such a case should be referred immediately to a dental professional (Table 2). The overall cumulative knowledge score of the SNs was 3.96 ± 1.31.
Identification of Dental Diseases/Conditions and Corresponding Referral Recommendations by California School Nurses Organization Survey Respondents.
When asked if they were willing to perform a simple annual oral health screening for children in the school where they work, almost 64% of SNs expressed the desire to. SNs cited many reasons for not being willing to perform annual oral health screenings. The most cited reasons included needing more time to conduct oral health screenings due to high caseload, understaffing, and insufficient resources. Some other reasons cited included not being formally trained to do oral health screening and therefore not feeling qualified, vision and hearing screenings being a higher priority than oral health, not within the scope of their practice, and already existing dental providers who do screening in schools where they work.
Table 3 and Table 4 show differences in knowledge related to identifying oral health conditions and choosing appropriate dental referrals between different subgroups of SNs. Except for a few significant differences between some subgroups, we saw no major differences in identifying oral health conditions or choosing appropriate dental referrals. Male SNs were significantly more likely to correctly identify root tips than female SNs were (P = 0.02). SNs from White racial backgrounds were significantly more likely to select the correct referral mode for tooth decay with no pain compared with those from other racial backgrounds (P = 0.007). SNs with a master’s degree and higher were significantly more likely to identify the correct referral mode for an abscessed tooth than those with a bachelor’s degree or lower (P = 0.02).
Bivariate Analysis Comparing SNs’ Knowledge of Oral Health Conditions by Key Characteristics.
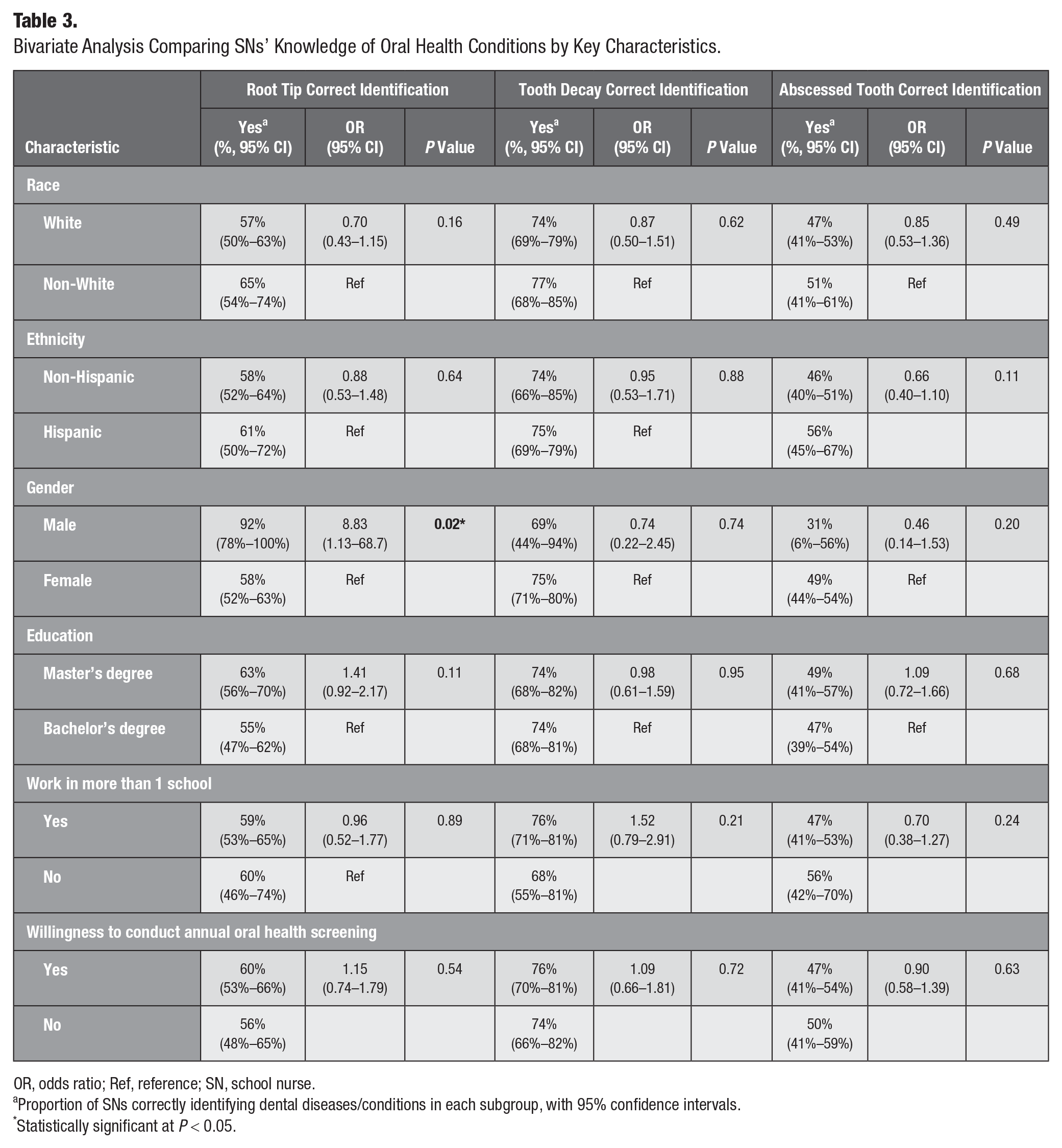
OR, odds ratio; Ref, reference; SN, school nurse.
Proportion of SNs correctly identifying dental diseases/conditions in each subgroup, with 95% confidence intervals.
Statistically significant at P < 0.05.
Bivariate Analysis Comparing SNs’ Knowledge of Correct Referral Modes for Specific Oral Health Conditions by Key Characteristics.
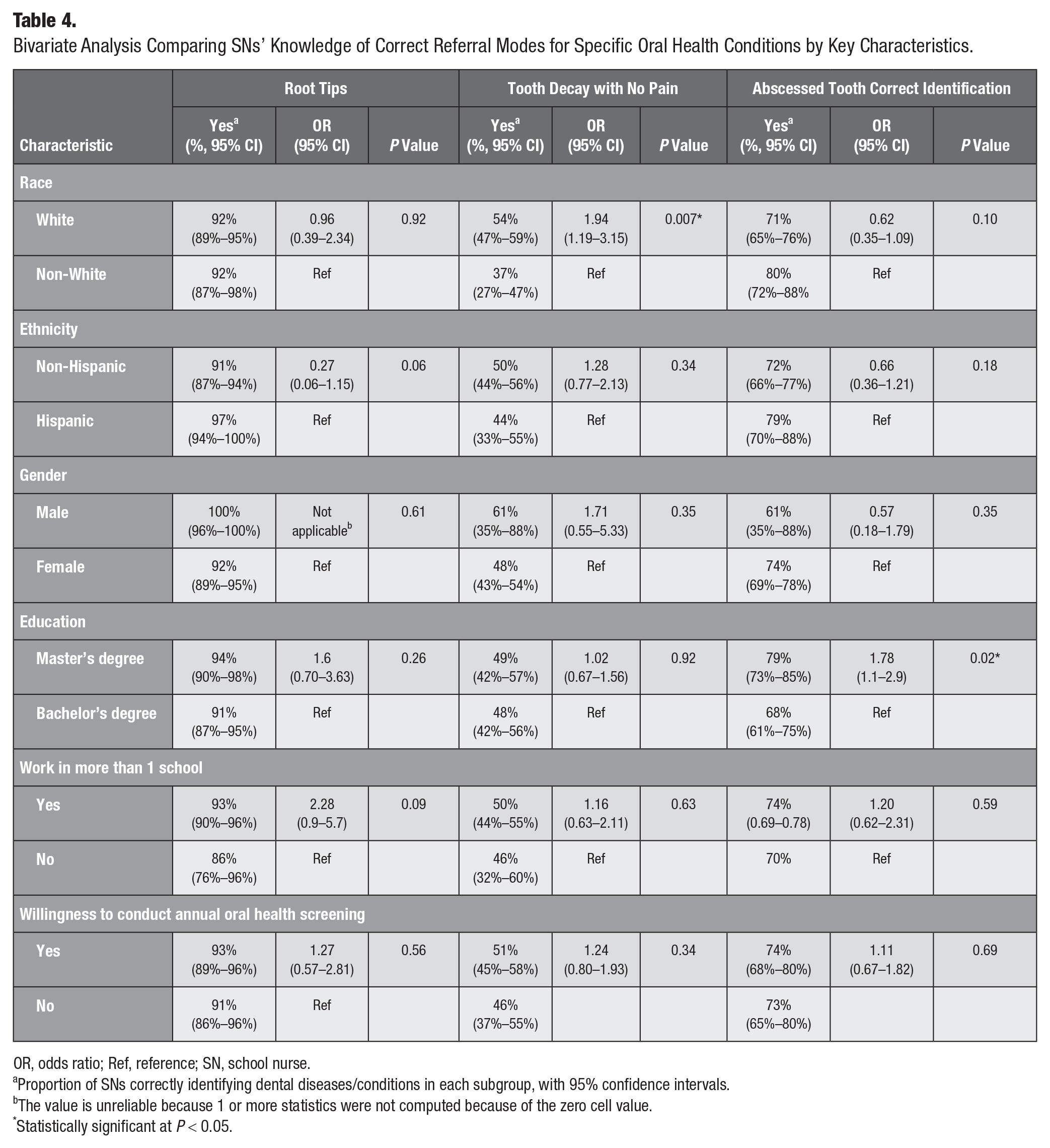
OR, odds ratio; Ref, reference; SN, school nurse.
Proportion of SNs correctly identifying dental diseases/conditions in each subgroup, with 95% confidence intervals.
The value is unreliable because 1 or more statistics were not computed because of the zero cell value.
Statistically significant at P < 0.05.
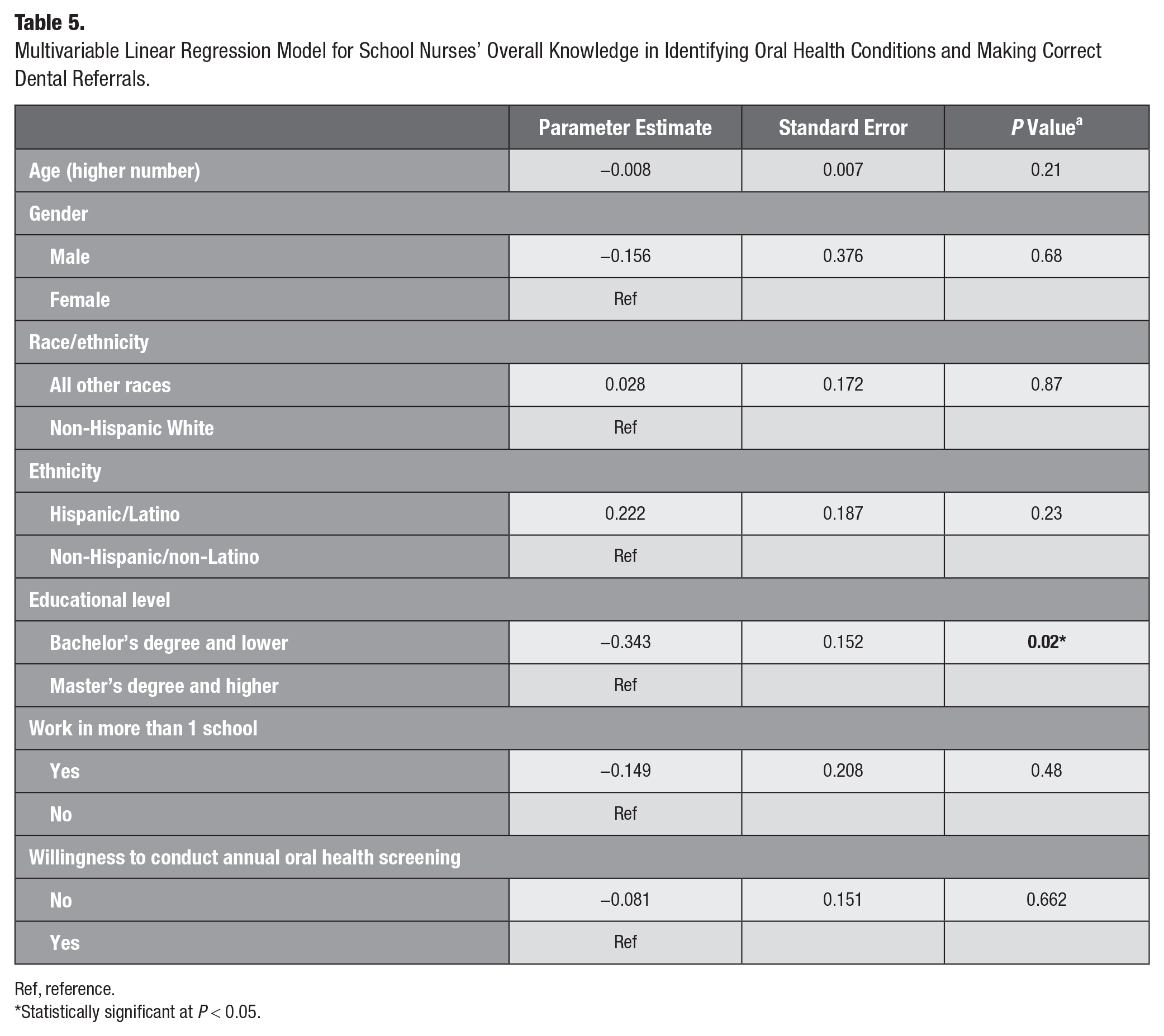
The adjusted linear regression analysis showed that SNs with a bachelor’s degree or lower had significantly lower overall knowledge in identifying common oral conditions and appropriate dental referrals than SNs with a master’s degree or higher by 0.343 points (P = 0.02) (Table 5). No other significant differences in overall knowledge were observed between different subgroups.
Multivariable Linear Regression Model for School Nurses’ Overall Knowledge in Identifying Oral Health Conditions and Making Correct Dental Referrals.
Ref, reference.
Statistically significant at P < 0.05.
Discussion
SNs play an essential role in school health programs by providing many health-related services, including preventive and screening services, health education, and decisions about the health of school children (Magalnick and Mazyck 2008). The NASN advocates for improving the oral health of school children by encouraging SNs to perform oral health prevention, education, and coordination (Buerlein 2010).
One of the strategies recommended in the 2018–2028 California Oral Health Plan is to identify, maintain, and expand community-clinical linkage programs in targeted sites for children, including schools (California Department of Public Health [CDPH], Office of Oral Health 2020). One example of a community clinical linkage program is a school-linked dental program in which screening for dental diseases/conditions, provision of preventive dental care services, and referral and follow-up happen in a school setting (CDPH 2018). Children with high dental care needs are linked with a dental care site where they may receive dental care.
The IOM recommended competencies for nondental professionals, which include recognizing common oral diseases/conditions and referring to dental professionals (IOM and National Research Council 2011), align well with operating school-linked dental programs. For this reason, and because statewide data show that third-grade children in California experience an unusually high prevalence of dental caries (Darise et al. 2021), we conducted this study to determine if members of CSNO are knowledgeable in identifying certain dental conditions and making appropriate referrals for further dental treatment. Adequate knowledge and skills to correctly identify dental conditions and make appropriate dental referrals are crucial to implementing school-linked dental programs. SNs specifically assigned to care for school children’s health can be a great resource in implementing a school-linked dental program because having a dental professional in a school setting is not always feasible and financially sustainable.
Our study showed that SNs’ knowledge of identifying the 3 oral conditions/dental diseases varied, with 50%, 61%, and 77% of SNs correctly identifying an abscessed tooth, root tips, and untreated tooth decay, respectively. The percentages of the appropriate dental referrals chosen for retained root tips, dental caries without pain, and an abscessed tooth were 93%, 50%, and 75%, respectively. These data show that although there may be variations in identifying oral health conditions correctly and choosing appropriate dental referrals, at least 50% of responding SNs correctly identified oral health conditions and appropriate dental referrals. These findings are encouraging because, despite oral health not being their primary health area of focus, at least half of the responding CSNO members knew about dental conditions and appropriate referral recommendations.
The regression analyses showed that SNs’ educational level was the only predictor of their overall knowledge of oral health conditions and appropriate dental referrals. SNs with a master’s degree or higher had significantly higher overall knowledge than those with a bachelor’s degree or lower. This finding is consistent with previous studies, which showed that nursing professionals with higher levels of education also had higher oral health knowledge and literacy than those with lower levels of education (Chan and Hui-Ling Ng 2012; Salamone et al. 2013). Nursing professionals with higher levels of education may update their knowledge by participating in additional training and workshops to keep them informed about their patient’s oral health.
This cross-sectional study has limitations. We did not have access to a statewide sample of SNs in California but only a convenience sample of CSNO members. Therefore, the study findings are not generalizable, which was not the intent of our research. The response rate was approximately 21%, lower than we expected. Recent nursing research shows that the average response rate for online surveys is about 42% (L’Ecuyer et al. 2023). There could be many reasons for nonresponse, including little interest in the focused topic. We did not have access to demographic information for the CSNO members and therefore could not compare those who responded and those who did not. The ASTDD’s Basic Screening Survey (BSS) report provided multiple images for untreated tooth decay, and we chose one of the images to display (ASTDD 2022). SNs could have identified untreated tooth decay correctly had we displayed 1 or more of the other pictures. However, because tooth decay does not appear uniformly on all teeth and may occur on different surfaces, knowing how to identify despite its varied appearances is crucial.
Recent data show that nurses are effective in the prevention of dental caries and oral health promotion (Baginska et al. 2021; Ruff et al. 2024). Our study, although focused on CSNO members, is an excellent addition to existing data on SN’s role in improving children’s oral health. SNs can contribute not only to school-linked dental programs but also to the national oral health surveillance system. SNs have access to millions of school children nationwide and provide health care services to those in need. If SNs are trained and competent in identifying oral health conditions and diseases, as defined by ASTDD, they can contribute to the national oral health surveillance systems by conducting BSS surveys for third graders in schools.
Conclusions
In our study, at least half of the participating SNs accurately identified the dental conditions and chose the appropriate dental referrals. Most respondents were willing to conduct annual oral health screenings for children. SNs with a bachelor’s degree and lower had significantly lower overall knowledge compared with those with master’s degrees and higher. When adequately trained, SNs, a nondental workforce, can effectively assess oral health needs and make appropriate dental referrals for school-linked dental programs.
Author Contributions
C. Neapole, contributed to data interpretation, drafted and critically revised the manuscript; V. Bhoopathi, contributed to conception, design, data acquisition, analysis, or interpretation, drafted and critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of work.
Footnotes
Acknowledgements
We thank the California School Nurses Organization (CSNO) leadership for distributing the survey and the CSNO members for participating.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by generous funding from the University of California, Los Angeles, School of Dentistry.