
Abstract
Introduction:
Health education plays a critical role in managing congenital anomalies like cleft lip and palate (CL/P). It equips parents with the knowledge and confidence needed for effective care, addressing medical, nutritional, and psychosocial challenges. In Ghana, where CL/P prevalence exceeds the global average and no national health education guidelines exist, initiatives often overlook culturally tailored approaches.
Objective:
To explore health education perceptions and barriers faced by Ghanaian parents of children with CL/P, guided by the social-ecological model at Komfo Anokye Teaching Hospital, Kumasi, Ghana.
Methods:
This qualitative study collected data through face-to-face, in-depth semi-structured interviews. Using criterion-based purposive sampling with maximum variation, parents of children with CL/P who visited the Department of Maxillofacial Surgery at the Komfo Anokye Teaching Hospital in Kumasi, Ghana, were selected. Thematic content analysis was employed to interpret the data and identify themes and subthemes.
Results:
Three themes were identified from analysis of data from 21 parents: 1) social challenges in educational and community settings; 2) inadequate health education information, characterized by overreliance on hospital-based oral instruction with limited availability of written or visual materials; and 3) lack of support facilities, organizations, and government policies beyond the hospital setting. Findings reveal multilevel barriers to effective CL/P health education in Ghana, including knowledge gaps, community stigma, limited organizational support, and absent national policy guidelines.
Discussion:
Addressing multilevel barriers to CL/P health education in Ghana requires culturally appropriate, multilingual materials; community outreach beyond hospitals; and national guidelines to improve outcomes for children with CL/P. Participants, while satisfied with surgical care, highlighted the need for better access to educational materials, stronger support networks, and greater public awareness to improve outcomes for children with CL/P.
Knowledge Transfer Statement:
This study provides important findings to inform community health education programs for parents, training workshops for clinicians on family-centered care, and policy briefs to inform health care leaders. It highlights the need to develop culturally appropriate educational materials to bridge knowledge gaps. Strengthening collaboration between hospitals, schools, and local governments will ensure that improved health education, psychosocial support, and outreach services are integrated into cleft care initiatives, ultimately enhancing outcomes for children with orofacial clefts.
Keywords
Introduction
Congenital anomalies, particularly cleft lip and/or palate (CL/P), present significant public health challenges globally, leading to infant morbidity, mortality, chronic illness, and psychosocial issues (Putri et al 2024; Dai et al 2026). Addressing these requires a multifaceted approach, with health education playing a crucial role in supporting parents in managing the complexities of these conditions (Hlongwa and Rispel 2018). Health education is essential for improving health outcomes by equipping parents with the necessary knowledge and skills to manage the challenges associated with congenital conditions. Children with CL/P often face difficulties in feeding, speech, hearing, and dental health, necessitating specialized care (Costa et al 2019; Sommer et al 2021). Parents frequently experience shock and confusion upon diagnosis, affecting their mental health and coping abilities (Stock et al 2018; Costa et al 2019). Effective health education can alleviate these issues by enhancing awareness, reducing anxiety, and promoting informed decision-making.
Globally, CL/P affects 1 in 700 live births, with a higher prevalence among Asian and American Indian populations (Xu et al 2021). In Ghana, the burden is substantially greater, estimated at 8 per 1,000 live births compared to 1.7 per 1,000 globally, with a Kumasi-based study identifying orofacial clefts as the most common congenital deformity in the region (Agbenorku et al 2013; Bonsu et al 2018). Socioeconomic factors such as low income, malnutrition, and smoking increase CL/P risk, while folic acid supplementation is protective (Ahmed et al 2022; Belcher et al 2022). Since these modifiable periconceptional factors, including folic acid deficiency, smoking, and malnutrition, contribute to CL/P incidence (Ahmed et al 2022; Belcher et al 2022), health education targeting such behaviors during pregnancy has the potential to reduce the occurrence of nonsyndromic CL/P. Support programs, such as the Partners in African Cleft Training (PACT) initiative, have helped train professionals across Ghana, Ethiopia, and Nigeria to enhance local care delivery (Baigorri et al 2021; McCullough and Campbell 2021), although significant gaps in rural health education persist due to geographic barriers, provider training shortfalls, and digital access limitations (Agbenorku et al 2007; Fadeyibi et al 2012).
Despite this, there are no national health education guidelines for families affected by CL/P, leading to delayed treatment-seeking and persistent stigmatization (Bhat et al 2020). Studies indicate that a lack of information during pregnancy and at child welfare centers contributes to delayed access to treatment (Massenburg et al 2016; Vyas et al 2020). The impact of CL/P extends beyond individual families, affecting community dynamics. In West Africa, children with CL/P often face stigmatization and discrimination, while parents experience social isolation and reduced support (Stock et al 2018; Costa et al 2019; Okoye 2019). Community-level health education programs are vital for addressing cultural misconceptions and providing psychosocial support (Hlongwa and Rispel 2018).
Health education also addresses financial and logistical barriers families face in seeking care. Insufficient funds, lack of knowledge, and limited access to resources hinder surgical treatment for CL/P (Massenburg et al 2016). Many affected families in Ghana come from low-income backgrounds, making access to care even more challenging (Donkor et al 2007). Tailored educational initiatives can help families navigate health care systems and access financial assistance (Hakim et al 2021).
This study is grounded in the social-ecological model (SEM) of health, which conceptualizes health behaviors and health outcomes as the product of dynamic interactions across multiple levels: intrapersonal, interpersonal, community, organizational, and policy (Schölmerich and Kawachi 2016). The SEM provides an appropriate theoretical lens for examining health education in the context of CL/P care in Ghana because the barriers to adequate parental knowledge and support operate simultaneously across these levels. At the intrapersonal level, individual parents may lack knowledge about CL/P etiology, feeding management, and psychosocial coping. At the interpersonal level, family dynamics, spousal support, and peer networks shape how parents access and process health information. At the community level, cultural misconceptions, stigma, and social exclusion influence parents’ willingness to seek care and engage with educational resources. At the organizational level, the adequacy of health education delivered by health care providers at facilities such as Komfo Anokye Teaching Hospital (KATH) is critical. At the policy level, the absence of national CL/P health education guidelines in Ghana limits the systematic reach of educational interventions. By applying the SEM, this study moves beyond individual-level explanations of health education gaps to identify leverage points for intervention across all levels of the socio-ecological system.
The purpose of this study was to explore the perceptions of parents of children with CL/P regarding available health education and its role in CL/P management, guided by the SEM. The study addressed 3 research questions:
What are the health education experiences of parents of children born with cleft lip and/or palate in Ghana?
How would parents of children born with CL/P describe available health education and information about their child’s health condition?
How do parents of children born with cleft lip and/or palate perceive care-supportive facilities or organizations, governmental policies, and their coping strategies in Ghana?
Methods
Study Design
This study employed a qualitative design situated within an interpretivist paradigm, which holds that social reality is subjectively constructed through individual lived experiences. This approach was appropriate for exploring the nuanced perceptions of parents of children with CL/P regarding their health education experiences, as it enabled in-depth, semi-structured interviews and a contextually sensitive understanding of their perspectives, satisfaction levels, and identified gaps in existing health education initiatives.
Research team and reflexivity
The lead researcher (A.A.) is a specialist orthodontist with direct clinical experience in CL/P care at KATH, informing both sensitivity to participants’ experiences and the need for careful reflexive management of potential clinical assumptions. Two public health education researchers led the methodological design, a social scientist guided the thematic interpretive approach, and 2 epidemiologists supported data credibility and audit trail maintenance. Reflexive journalling and regular peer debriefing sessions were employed throughout data collection and analysis to identify and manage potential researcher biases, consistent with COREQ checklist domain 1 criteria (Tong et al 2007).
Setting and Participants
The research was conducted at the Multidisciplinary Cleft Care Centre at KATH in Kumasi, Ghana. This center provides comprehensive cleft care, making it an ideal location for assessing educational interventions. Participants consisted of 21 parents attending review appointments or referred for their child’s treatment.
This number was chosen as data saturation was assessed systematically from the 15th interview, with no new codes emerging from the 18th interview onward, and confirmed after the 21st interview, consistent with established qualitative research practice for studies of this scope.
Data Collection
In-depth, semi-structured interviews were conducted in a private room to ensure confidentiality and encourage open discussion. A semi-structured interview guide, developed based on the study objectives and existing literature, was used. The guide was pilot-tested with 3 parents of children with CL/P (who were not included in the main study) to ensure clarity, cultural appropriateness, and relevance of the questions, with minor refinements made based on their feedback. Each session lasted approximately 40 to 60 min and was audio-recorded with participants’ consent for accurate data capture. Interviews were conducted primarily in Twi, the mother tongue of most participants, facilitating smoother communication. Five participants used English, ensuring inclusivity across linguistic groups.
Data Analysis
Data were analyzed using Braun and Clarke’s (2014) systematic 6-phase thematic analysis framework, involving data familiarization, inductive coding, generating and reviewing themes, defining/naming themes, and reporting theme development. Initial open codes were generated from the transcripts and iteratively refined into a standardized codebook. To support multilevel interpretation, emergent categories were mapped to the SEM across the intrapersonal, interpersonal, community, organizational, and policy domains. Data source triangulation (comparing accounts across participants varying in socioeconomic, educational, and geographic backgrounds) and investigator triangulation (independent coding by 3 team members, followed by consensus discussion) of findings enhanced the credibility and reliability of the results.
To ensure analytical rigor and optimize intercoder reliability, 3 analysts independently coded an initial subset of transcripts to pilot the codebook. Coding then proceeded with regular consensus-building sessions, where disagreements were resolved through team discussion and reference to a detailed audit trail. Due to the sensitive nature of the qualitative narratives, including experiences of stigma and specific community references, analysis was conducted using deidentified transcripts to mitigate the risk of participant reidentification within a single-center sample. A summarized coding tree and theme development matrix are provided in Appendix Table 1.
Ethical Considerations
Ethical clearance for the study was granted by the Institutional Review Board of Walden University (Approval No. 04-04-24-0655274) and the Committee on Human Research, Publications, and Ethics at Kwame Nkrumah University of Science and Technology (Approval No. CHRPE/AP/091/24). All participants received comprehensive information regarding the study’s objectives, procedures, and their rights, including the option to withdraw at any stage without consequence. Informed consent was obtained in writing prior to data collection. Participant confidentiality was ensured through data deidentification and secure storage on password-protected systems. The study complied with rigorous ethical standards in alignment with the Declaration of Helsinki and applicable national research regulations.
Evidence of Trustworthiness
A focused research question guided the study to maintain clarity and purpose. Reliable and validated instruments were used to ensure the precision of results. Reflexivity was practiced through continuous self-reflection and maintaining a reflexive journal, minimizing researcher bias. Limitations of the study were acknowledged to enhance credibility. Detailed descriptions of participant selection, data collection, and analysis procedures were provided to ensure contextual understanding. Triangulation of data sources and investigators, member checking conducted in both Twi and English with back-translation to verify accuracy, and stakeholder engagement further strengthened the applicability of findings across different settings. Interview protocols were developed through a thorough literature review and expert consultation to ensure external validity. Dependability was achieved by reaching data saturation, maintaining an audit trail, and seeking peer review to enhance transparency and reliability throughout the research process. Confirmability was ensured by reducing researcher bias through reflexive journaling and grounding all interpretations and conclusions firmly in the collected data, maintaining transparency and objectivity. Intracoder reliability was strengthened through pilot testing of coding procedures and prioritizing familiarity with the research topic to ensure robust and consistent coding practices.
Results
Demographics
The study included 21 participants, the majority of whom were women (20 of 21). Most participants were between the ages of 29 and 38, and a significant number were married (15 individuals). Educational backgrounds varied widely, ranging from primary to tertiary levels. Many participants were engaged in informal employment, such as farming, trading, and hairdressing, while a smaller group worked in the formal sector. Monthly income levels also differed, with most participants (15 of 21) earning below GHS 5,000, pointing to the economic challenges faced by parents. Available from clinical records, the children of participants presented with a wide range of CL/P types, including unilateral cleft lip with or without palate, bilateral cleft lip, and isolated cleft palate. This clinical diversity supports the transferability of findings across different CL/P presentations and care contexts.
Themes
Theme 1: Social Challenges in Educational and Community Settings
Addressing research question 1 (what are the health education experiences of parents of children born with CL/P?), this theme reveals how social and community-level factors such as stigma, discrimination, and limited school support directly shaped parents’ engagement with health education and their ability to advocate for their children’s well-being. These experiences reflect barriers operating at the intrapersonal, interpersonal, and community levels of the SEM. Figure 1 presents a thematic map of this theme, illustrating 2 subthemes: experiences in schools, churches, and communities (subtheme 1.1) and support systems and networks (subtheme 1.2).
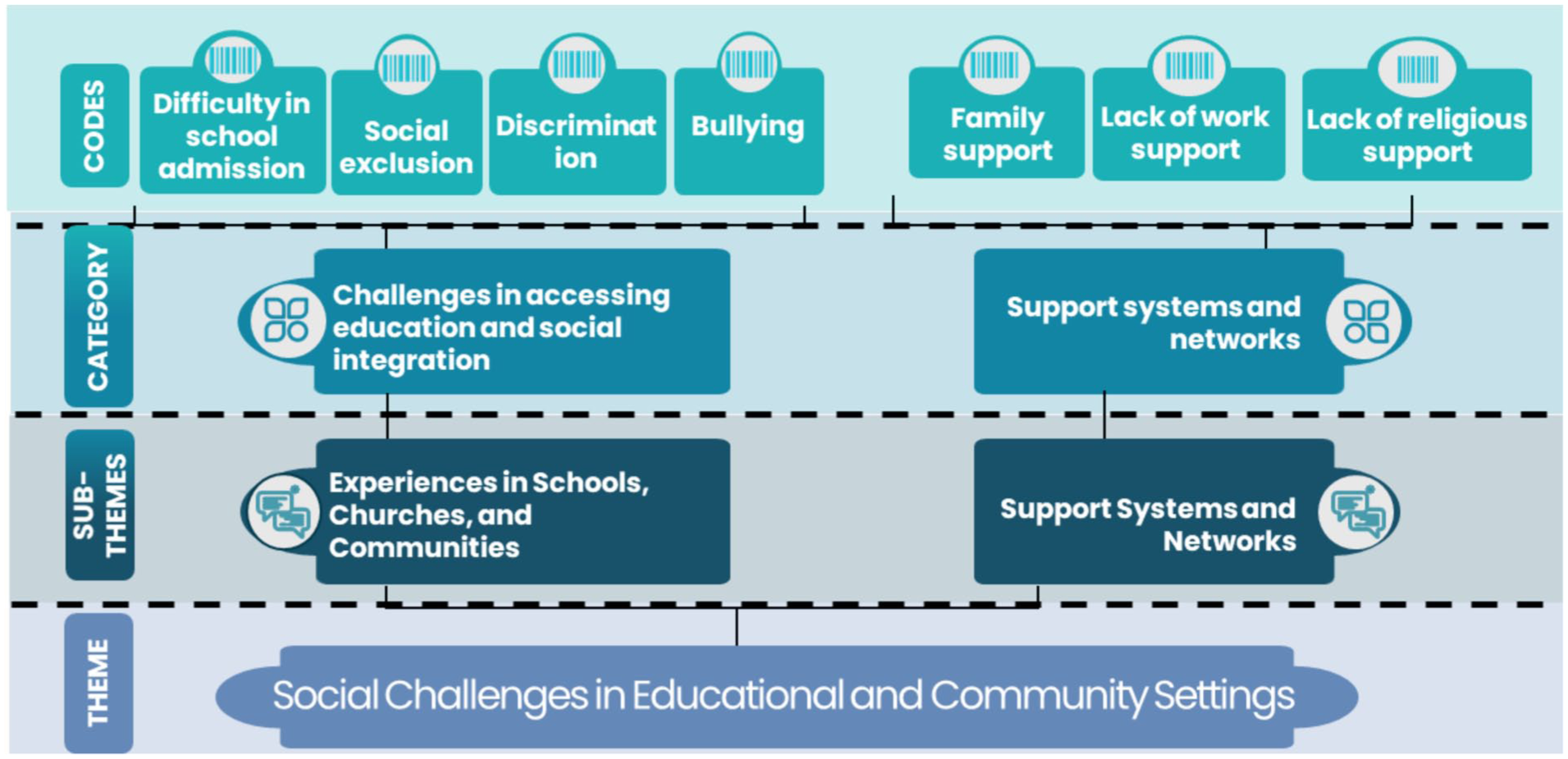
Thematic framework of social challenges and support systems, showing codes organized into categories and subthemes under the theme of social challenges in educational and community settings.
Subtheme 1.1: Difficult experiences in schools, churches, and communities caused by stigma (Fig. 1)
Parents reported difficulties enrolling their children in school due to stigma. Children also experienced bullying from peers. One mother shared, “When she went to school, mates used to tell her, ‘Let us look at your teeth, let us look at your teeth,’ but I told the headmistress of the school who issued a warning to the children to stop doing that” (participant 8).
Another participant recalled, “When he goes into someone’s house, they say to him ‘Go away from here with your crooked mouth,’ It makes me so sad” (participant 4). These experiences of social exclusion were compounded by a lack of understanding and support in school environments, but proactive measures from parents, such as informing teachers, helped reduce these challenges. In communities, social exclusion was common. Despite these challenges, some children excel academically when supported. “Even when they did exams, she was third, so I think she’s doing well” (participant 11), a parent noted, emphasizing the importance of supportive environments.
Subtheme 1.2: Support systems, networks, and social isolation (Fig. 1)
Family support played a crucial role, with one father stating, “I have enough family support, especially from the siblings. They don’t use his condition to intimidate him” (participant 21). However, some parents lacked external assistance. A mother noted, “I don’t have support from anywhere. . . . As for my mom, she’s a pillar of support for me” (participant 20).
Cultural misconceptions and stigma contributed to isolation. Some parents avoided discussing their child’s condition. One participant admitted, “I did not inform my church about my child’s condition. It’s only my pastor who knows” (participant 4), indicating fear of discrimination. Others reported deeply ingrained beliefs about cleft as a curse or supernatural occurrence. One mother stated, “I’ve heard that people say children born like that are children from the waters (nsuo baa); they are not humans” (participant 5). Some parents faced hurtful comments, social isolation, and exclusion from community activities. One mother shared, “For some people, they have never seen a child with a cleft palate, so they do not want us to come near them” (participant 13).
Theme 2: Inadequate Health Education Information
Addressing research question 2 (how do parents describe available health education about their child’s condition?), this theme demonstrates that parents perceived health education as inadequate, inaccessible, and insufficiently comprehensive. These barriers operate primarily at the organizational level (health care provider education practices) and the intrapersonal level (parental knowledge gaps) of the SEM. Figure 2 presents a thematic map of this theme, comprising 2 subthemes: sources of health education and information (subtheme 2.1) and health care accessibility and satisfaction (subtheme 2.2).
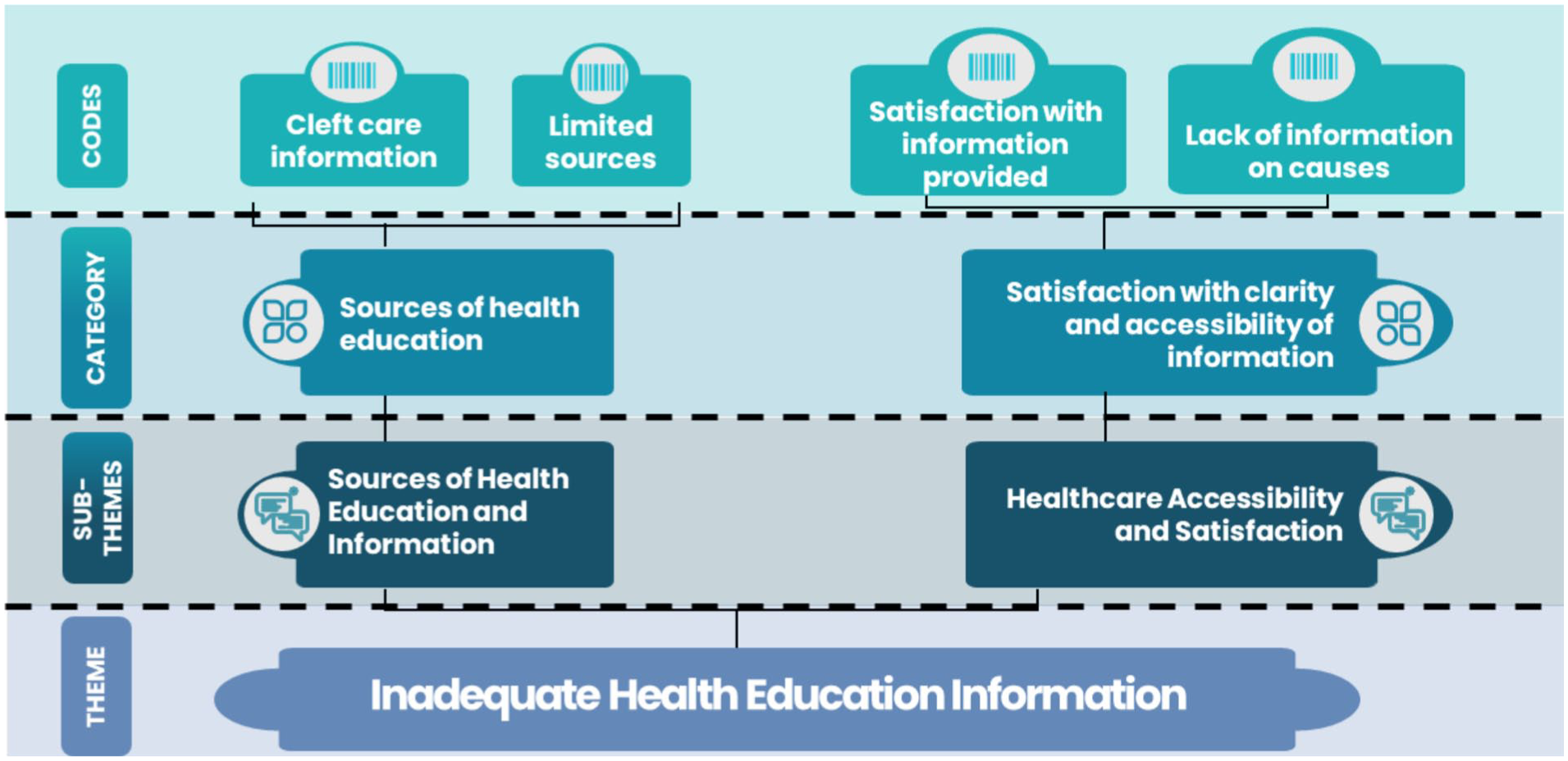
Thematic framework of cleft care information and patient satisfaction, showing codes grouped into categories and subthemes under the theme of inadequate health education.
Subtheme 2.1: Reliance on health services for health education (Fig. 2)
Participants largely depended on health care facilities for information about their child’s condition. One participant remarked, “The only information that I have is what I get from this place” (participant 20). Another mother mentioned, “Apart from here, I do not know of any other place, we are not given any printed material, we are taught everything here orally when we come” (participant 8). This reliance on health care providers as the only source of information underscores the limited availability of alternative resources for parents.
Subtheme 2.2: Health care accessibility and satisfaction (Fig. 2)
While participants expressed satisfaction with the surgical care their children received, many felt that there was a lack of comprehensive and accessible educational information. One mother explained, “I’m not satisfied because I don’t know the cause as of now, whether it was environmental, genetic, or hereditary” (participant 12). Another participant expressed gratitude for the surgical care, stating, “As for what the doctors did if I say I’m not grateful then I’ll be lying. Because when I brought him, he didn’t look like this” (participant 4). Overall, educational support for managing their children’s condition is deemed inadequate.
Theme 3: Perceptions of Support Facilities, Organizations, and Government Policies
Addressing research question 3 (how do parents perceive supportive organizations, governmental policies, and their own coping strategies?), this theme reveals the near-total absence of structured support beyond the hospital setting and the inadequacy of existing policies for CL/P families. These findings reflect organizational and policy-level deficits within the SEM, while identified coping strategies illustrate intrapersonal and interpersonal resilience mechanisms. Figure 3 presents a thematic map of this theme, comprising 3 subthemes: few supportive facilities and organizations (subtheme 3.1), insufficient governmental policies (subtheme 3.2), and coping strategies (subtheme 3.3).

Thematic framework of health care access, policy awareness, and coping mechanisms, showing codes organized into categories and subthemes under the theme of limited support systems and policies.
Subtheme 3.1: Few supportive facilities and organizations (Fig. 3)
Despite appreciating the medical care received, participants expressed frustration with the lack of support organizations and networks. Many were unaware of any community-based support or government policies aimed at addressing the needs of children with cleft lip and/or palate. One participant mentioned, “I have not heard of any support organizations in my area apart from the hospital where I bring my child for treatment” (participant 13). Another also shared, “I have not been anywhere, so I don’t know. This is the only place that I come to” (participant 20). This suggests a need for increased visibility and outreach from support organizations to ensure that parents are aware of the available resources. Support from private and governmental organizations is seen as nonexistent, particularly in terms of providing continuous educational resources and support networks.
Subtheme 3.2: Insufficient governmental policies (Fig. 3)
The effectiveness of governmental policies in addressing the needs of families with children living with cleft lip and/or palate in Ghana is generally perceived as insufficient. While some parents acknowledge the role of health insurance in subsidizing medical costs, there is a lack of targeted policies specifically designed to support these families comprehensively. The lack of awareness about targeted policies was evident, with 1 participant noting, “No, I don’t know of any government policies specifically for children with cleft lips and palate. We just use the national health insurance for the medical bills” (participant 10). Another participant expressed the need for improvement, saying, “As I said initially it’s not enough. More can be done. They are doing their best, but when they are well-resourced, they can do better” (participant 12). A young mother highlighted the financial challenges faced by parents, stating, “Most of the parents with cases like this need support. I had an experience when I had my second surgery. Most of the mothers after surgery face payment challenges” (participant 7). However, others expressed appreciation for the government’s support in covering some health care costs associated with their child’s treatment.
Subtheme 3.3: Coping strategies (Fig. 3)
Common strategies include seeking support from family members, relying on health care providers for information, and finding solace in religious or spiritual beliefs. Despite challenges, many parents developed adaptive strategies to manage emotional and practical aspects of their children’s condition, emphasizing the importance of community and faith-based support. One mother expressed, “I look to God” (participant 4), indicating that her faith provides comfort and strength. The importance of family support was also emphasized: “My family really supports me. I can even leave my child with them and go somewhere. When I go to the farm my mother takes care of him” (participant 15). Another shared, “I have enough family support, especially from the siblings. They don’t use his condition to intimidate him and try their best to support him” (participant 21). Some participants demonstrated resilience by creating explanations for their child’s condition; one said, “When he cries and people ask why, I just tell them that he fell down” (participant 8). These diverse coping mechanisms highlight the role of individual resilience.
Discussion
Summary and Interpretation of Main Findings
This study explored the health education experiences and perceptions of parents of children with CL/P in Ghana through 3 interconnected themes, interpreted through the SEM. Across all themes, findings consistently reveal that parents navigate multiple, compounding barriers to health education, which operate simultaneously at individual, social, organizational, and policy levels, rather than in isolation.
At the intrapersonal and interpersonal levels, theme 1 demonstrates that stigma, cultural misconceptions about the etiology of CL/P, and social exclusion, particularly within schools and communities, profoundly constrained parents’ capacity to seek information, advocate for their children, and engage with available health education. These social barriers are consistent with SEM’s conceptualization of community-level influences on health behavior and align with evidence from comparable West African settings where cultural beliefs linking CL/P to supernatural causes generate stigma that compounds existing health care access challenges (Kimotho and Macharia 2020; Chime et al 2020).
At the organizational level, theme 2 reveals that health education provided to parents was largely confined to verbal instruction at clinical encounters, with no structured written, visual, or digital materials available. This unidimensional, provider-dependent approach left parents without the knowledge needed to understand causal factors, manage feeding and speech difficulties, or address psychosocial challenges independently. The near-total reliance on KATH as the sole source of information reflects a critical organizational gap and mirrors findings by Hlongwa and Rispel (2018) and Bonsu et al (2018) regarding the insufficiency of health education resources for CL/P families in sub-Saharan Africa.
At the policy level, theme 3 identifies the absence of government-supported CL/P education programs, limited awareness of and access to support organizations, and an overreliance on the national health insurance scheme as the primary policy response. In the absence of structured policy support, parents drew upon intrapersonal and interpersonal resilience mechanisms, including faith, family networks, and peer solidarity, as primary coping strategies. Taken together, these findings underscore that effective health education for CL/P in Ghana requires coordinated, multilevel intervention that addresses structural deficits rather than placing adaptive burden solely on individual families.
Clinical, Translational, and Policy Implications
The persistent deficiency in comprehensive national health education campaigns on CL/P in Ghana reflects a broader international challenge in integrating specialized congenital care into primary health care frameworks. This study reinforces the critical need for accessible, detailed educational resources addressing not only medical management, such as surgical care and nutritional needs, but also the psychosocial challenges experienced by parents and caregivers (Hlongwa and Rispel 2018; Belcher et al 2022). While provided surgical outcomes are generally satisfactory, the inadequate availability of health education resources stands in stark contrast, necessitating a paradigm shift in how cleft care is delivered.
Clinically, the reliance on verbal instruction (theme 2) highlights the urgent need to develop multiformat educational materials (pamphlets, videos, digital content) tailored to varying literacy levels. The demographic diversity of participants in this study demonstrates that parents have wide-ranging educational backgrounds; therefore, materials must be comprehensible and useful for all families, from those with limited literacy to those with tertiary education. From a translational perspective, the profound impact of stigma (theme 1) and the demonstrated value of peer support necessitate shifting health education from purely clinical settings into community hubs such as churches, community centers, and district hospitals, particularly in rural regions. Empowering local health care workers and community leaders through training could ensure broader dissemination of essential information. Peer support emerged as a particularly impactful form of education in this study, with many parents reporting that engaging with others facing similar challenges significantly helped them navigate the emotional and practical aspects of raising a child with a cleft. Integrating peer counseling, both in-person and online, could enhance emotional resilience and practical knowledge-sharing (Hlongwa and Rispel 2018; Costa et al 2023).
Policy-wise, addressing the structural deficits identified in theme 3 requires multiagency partnerships between governments and nongovernmental organizations to establish standardized, culturally appropriate health education protocols that can be adapted across different sub-Saharan African contexts. With the increasing availability of smartphones and Internet access, digital platforms offer a powerful means of disseminating educational materials. Mobile apps or websites specifically designed for parents of children with clefts could provide easy access to information, video tutorials, and support networks. Governmental policies should focus on increasing public awareness about CL/P and making educational resources widely available, with partnerships bridging gaps in rural and underserved areas through financial support, educational outreach, and training for local health care workers.
What This Study Adds
To our knowledge, this is the first qualitative study to systematically explore the health education experiences of parents of children with CL/P in Ghana using the SEM framework. By identifying specific multilevel barriers (intrapersonal, interpersonal, community, organizational, and policy) that collectively limit the effectiveness of current health education, this study extends existing literature and provides a theoretically grounded foundation for designing multilevel interventions. The study’s particular emphasis on the vulnerability of parents in rural and low-income settings, where access to health education resources is most constrained, fills a critical gap in the literature. These insights not only are relevant to Ghana but also offer a replicable model for comparable low- and middle-income countries seeking to strengthen cleft care through comprehensive health education.
Limitations and Strengths
While this qualitative study provided valuable insights into the health education experiences of parents and caregivers of children with cleft lip and/or palate in Ghana, several limitations affected trustworthiness. The study’s restriction to KATH in Kumasi limits generalizability, particularly to rural areas with different health care conditions. Selection bias may have occurred, as participants were drawn from those able to access the clinic, possibly excluding caregivers facing financial or logistical barriers. Language constraints, with interviews in Twi and English, may have excluded nonspeakers, and translation could introduce misinterpretations. Despite structured interview guides, researcher bias and recall bias could have influenced the findings. Social desirability bias may have led participants to provide socially acceptable responses rather than authentic accounts. Finally, the predefined interview scope may have limited exploration of broader relevant themes.
Notwithstanding these limitations, this study has several strengths. The use of in-depth, semi-structured interviews in participants’ native language (Twi) ensured linguistic authenticity and minimized communication barriers. The multidisciplinary research team, comprising clinical, public health, social science, and epidemiological expertise, enhanced the credibility and analytical rigor of the findings. The purposive sampling approach with maximum variation ensured a diverse participant group, strengthening the transferability of findings to comparable settings. The application of the SEM provides a replicable theoretical framework for future health education research in CL/P and other congenital conditions in low- and middle-income country contexts.
Future Directions and Recommendations
This study recommends strengthening health education for parents of children with CL/P through improved awareness campaigns, inclusive education, and comprehensive family support. National and localized programs should be expanded to increase public knowledge and dismantle cultural misconceptions. Health care providers must be equipped to deliver comprehensive counseling before and after surgical intervention, supported by clear, literacy-appropriate educational materials and proactive community outreach. Additionally, establishing robust support groups, professional counseling services, and financial aid programs will help families cope with the significant emotional and economic challenges they face. Future research should evaluate the efficacy of parent brochures, pamphlets, digital platforms, community-based peer support models, and multiagency partnerships in improving health literacy and psychosocial outcomes for this population.
Conclusion
This study highlighted the multifaceted health education challenges faced by parents and caregivers of children with cleft lip and/or palate in Ghana. While participants expressed satisfaction with surgical interventions, the pervasive impact of stigma, coupled with inadequate educational resources and support systems, underscores the need for a paradigm shift in cleft care. Moving beyond surgical repair, comprehensive care requires multiagency partnerships to implement accessible, culturally tailored health education, including printed materials and robust psychosocial support networks, ultimately improving the quality of life for affected families and promoting a more inclusive society.
Author Contributions
A.A. Amuasi, contributed to conception and design, data acquisition of data, data analysis and interpretation, drafted and critically revised the manuscript; D. Long-White, J. Saindon, A.O. Crentsil, contributed to conception and design, data acquisition of data, data analysis and interpretation, critically revised the manuscript; E.E. Boham, J.H. Amuasi, contributed to data analysis and interpretation, critically revised the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844261451851 – Supplemental material for Health Education Barriers for Ghanaian Parents of Children with Cleft Lip and Palate: Qualitative Study
Supplemental material, sj-docx-1-jct-10.1177_23800844261451851 for Health Education Barriers for Ghanaian Parents of Children with Cleft Lip and Palate: Qualitative Study by A.A. Amuasi, D. Long-White, J. Saindon, A.O. Crentsil, E.E. Boham and J.H. Amuasi in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is self-funded.
Data Availability
To protect participant confidentiality in this single-center study, raw interview transcripts contain detailed personal narratives and are not available for public deposition. These narratives contain sensitive information that could increase the risk of participant reidentification. Deidentified analytic materials, including the codebook and anonymized quotations, are available from the corresponding author upon reasonable request. Access to full deidentified transcripts for bona fide research purposes may be granted subject to a formal data use agreement and approval by the relevant ethics committees.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.