
Abstract
Introduction:
Oral health is a crucial yet neglected aspect of the global health and development agenda. Although oral diseases affect almost half of the world’s population, they receive little attention and public investment by policymakers, undermining progress toward the Sustainable Development Goals (SDGs).
Objective:
The study aimed to 1) analyse the SDG framework through an oral health lens, identifying links across goals and targets, and 2) quantify the reduction in oral disease burden required by 2030 under a counterfactual status quo projection and 2 policy benchmark scenarios: one-third reduction of noncommunicable disease prevalence aligned with SDG target and 10% reduction based on the World Health Organization Global Oral Health Strategy & Action Plan (GOHAP) target.
Methods:
A systematic content analysis was conducted on the UN resolution “Transforming Our World: The 2030 Agenda for Sustainable Development.” Linkages were categorised across 4 dimensions: disease burden, determinants, system integration, and policy alignment. The Global Burden of Disease data were used to model a counterfactual status quo projection using the compound annual growth rate (CAGR) (2015–2019), disaggregated by World Bank income groups. “Improvement ambition,” representing potential preventable disease burden, was calculated as the difference between the status quo projection and each target.
Results:
Oral health was directly or indirectly linked to all 17 SDGs and 37 of 169 SDG targets, particularly SDGs 3, 4, 6, and 10. Achieving the SDG-aligned target could avert 981 and 649 million cases of caries of permanent teeth and periodontal disease, respectively, by 2030. Even with the GOHAP target of a 10% reduction, 373 and 272 million cases could be averted, respectively.
Conclusion:
Oral health is linked to the SDGs through shared risk factors and determinants with implications for equity and global development. The “improvement ambition” metric provides a practical tool for policymakers to benchmark progress and guide investments during this decisive decade.
Knowledge Transfer Statement:
Integrating oral health into SDG-aligned policy could avert up to 981 million cases of permanent caries and 649 million cases of periodontal disease by 2030. Even achieving the WHO Global Oral Health Action Plan target would prevent hundreds of millions of cases globally. Our “improvement ambition” metric helps policymakers and researchers benchmark progress toward Universal Health Coverage, noncommunicable disease prevention, and health equity, highlighting that excluding oral health results in losses in health, productivity, and social progress.
Keywords
Introduction
Oral health is a significant blind spot in the global health agenda. Despite affecting nearly half the world’s population, oral diseases remain largely absent from national health priorities and global health investments. This neglect has serious consequences, not only for individuals but for the success of international development frameworks. As the world approaches 2030, the promise of the Sustainable Development Goals (SDGs) is at risk, and oral health is a litmus test for whether that promise can be fulfilled.
Over 3.5 billion people have untreated oral conditions, with preventable diseases such as caries, periodontitis, and tooth loss continuing to rise (Bernabe et al 2025). Yet oral diseases are not explicitly acknowledged across the 17 SDGs and their 169 targets (United Nations General Assembly 2015). This disconnection is more than a missed opportunity; it undermines the goals themselves. From poverty and nutrition to education, employment, and health equity, oral diseases exert silent but significant pressure on development outcomes (Peres et al 2019). Without addressing them, progress on SDG 3 (health); SDG 1 (poverty); SDG 4 (education); SDG 6 on water, sanitation, and hygiene (WASH); and SDG 10 (inequality) will not be fully achievable (Winkelmann et al 2023; Listl and Bärnighausen 2025).
In response to decades of neglect, the World Health Organization (WHO) adopted a historic resolution on oral health in 2021, followed by the development of the Global Oral Health Strategy & Action Plan, 2023–2030 (GOHAP) (World Health Assembly 2021; WHO 2024). GOHAP provides a strategic roadmap for improving oral health worldwide by integrating it into primary health care, universal health coverage (UHC), and population-level interventions. The plan’s global monitoring framework also includes a global disease reduction target, aiming for a 10% relative reduction in the prevalence of major oral diseases by 2030, using 2023 as a baseline (WHO 2025). Although less ambitious than the one-third reduction target of SDG 3.4 for noncommunicable diseases (NCDs), this marks the first time for over 2 decades that oral diseases have been clearly tied to a measurable global goal in WHO policy (Fédération Dentaire Internationale 1982).
These parallel targets—SDG 3.4 and GOHAP—provide the foundation for this article’s analytical approach. Setting disease reduction goals has long been used in global health to drive investments, track progress, and benchmark accountability. Yet for oral health, the magnitude of what could be achieved remains poorly understood.
This article combines 2 novel contributions. First, it offers a systematic content analysis of the SDG framework through an oral health lens by mapping where and how oral health aligns with sustainable development. Second, it quantifies the “improvement ambition”: the number of cases (for caries of deciduous and permanent teeth, edentulism, and periodontal disease) that could be prevented if oral health were truly improved in line with the SDGs and the GOHAP targets. The target scenarios include 1) the SDG target of a one-third reduction in prevalence for NCDs and 2) the GOHAP target of a 10% reduction. The findings show that oral health is not only relevant to the SDGs but also indispensable to achieving them.
Methodology
This study employed a 2-pronged analytical approach to examine the relationship between oral health and the SDGs and to estimate the scale of missed progress under current trajectories.
Content Analysis of the SDG Framework
We conducted a comprehensive and systematic content analysis of the official United Nations (UN) resolution “Transforming Our World: The 2030 Agenda for Sustainable Development,” including the preamble, overarching vision, all 17 goals, and their 169 associated targets (United Nations General Assembly 2015). The objective was to identify direct and indirect linkages between the SDGs and oral health, based on explicit language around health, social and commercial determinants, system integration, and implementation mechanisms.
The 4 analytical dimensions—namely, disease burden, determinants, system integration, and policy alignment—were defined drawing on established frameworks, including the common risk factor approach, the social determinants of health, and WHO frameworks on UHC.
An initial classification of each SDG across these dimensions was conducted by a lead author with expertise in global oral health policy, applying a 3-level relevance rating (strong, moderate, limited). Classification was based on the presence, explicitness, and multidimensionality of oral health linkages within the SDG text (for detailed definitions of the rating scale, see Table 1).
Summary highlights of SDG–Oral Health links.
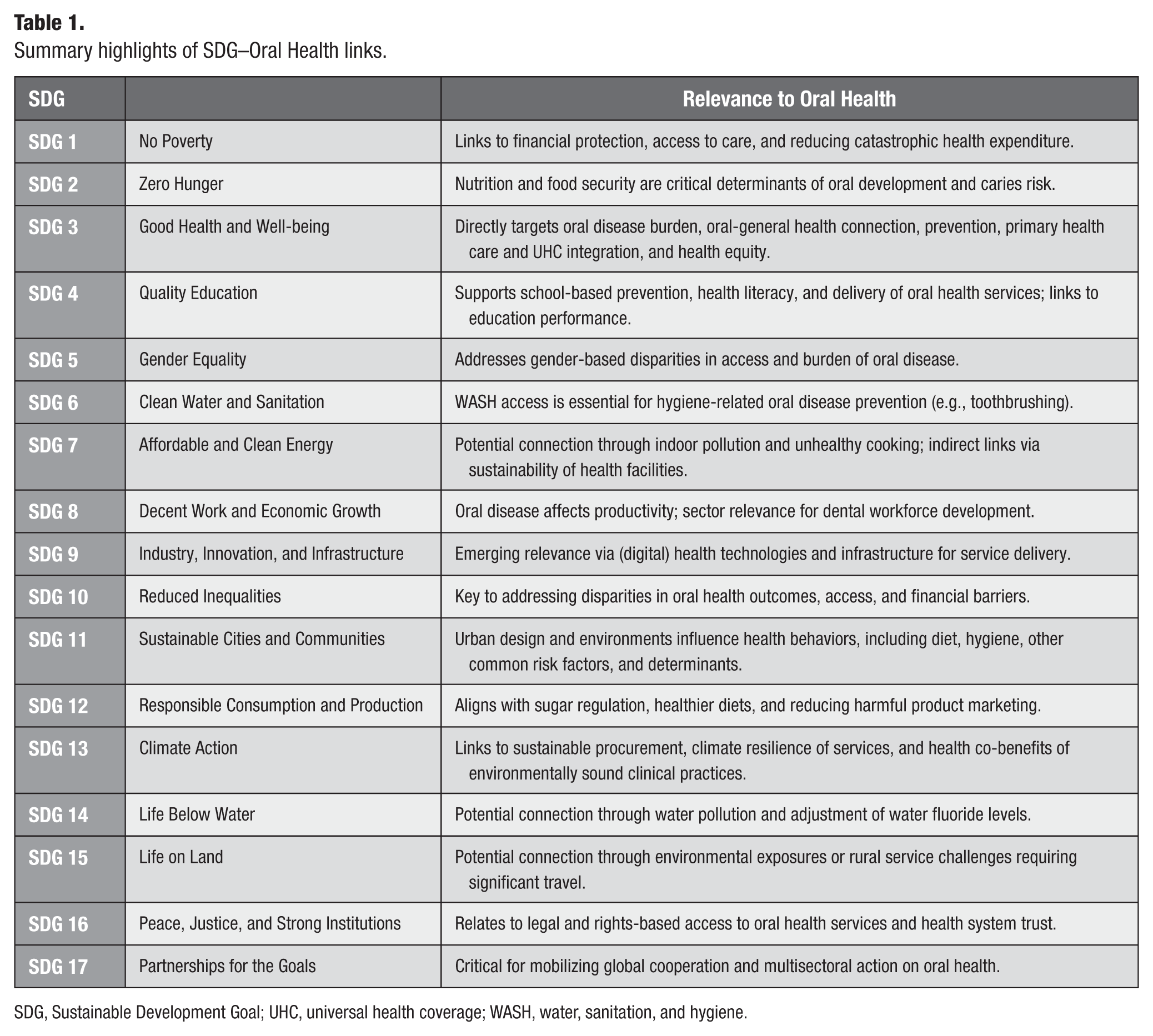
SDG, Sustainable Development Goal; UHC, universal health coverage; WASH, water, sanitation, and hygiene.
The full classification was subsequently reviewed by all coauthors using a shared analytical matrix. Discrepancies in interpretation were discussed and resolved through consensus, with reference to the original SDG language and the predefined analytical dimensions. For clarity and advocacy purposes, the results of this analysis were later visualised as a heatmap, categorising each SDG on a 1 to 3 scale across the 4 analytical dimensions. This approach represents a structured, theory-informed content analysis designed to identify policy-relevant linkages rather than a quantitative coding exercise.
Each SDG was categorised based on a 3-level scoring system (strong, moderate, or limited alignment). Classification into strong, moderate, or limited alignment was based on 3 criteria: 1) the presence of explicit or implicit references relevant to oral health, 2) the clarity and strength of the linkage, and 3) the extent to which multiple analytical dimensions were addressed within a given SDG. SDGs demonstrating clear and multidimensional connections were classified as strong, those with partial but meaningful linkages as moderate, and those with indirect or limited relevance as limited.
All coauthors independently reviewed the full-resolution text to extract relevant references. These included 1) links to disease outcomes such as NCDs, UHC, and malnutrition; 2) references to determinants such as hygiene, education, inequality, and WASH; and 3) institutional pathways relevant to oral health integration. Extracted references were consolidated into a comprehensive matrix that grouped linkages by SDG and relevance dimension. Discrepancies were resolved through discussion and consensus.
For clarity and advocacy purposes, the results of this analysis were later visualized as a heatmap, categorizing each SDG on a 1 to 5 scale across 4 dimensions: Disease Burden, Determinants, System Integration, and Policy Alignment.
Modeling Counterfactual Scenarios for Disease Burden
To estimate the potential impact of achieving global oral health targets, we projected case numbers for 4 major oral conditions—caries of permanent teeth, caries of deciduous teeth, edentulism, and periodontal disease—under 3 scenarios:
Scenario 1: Status quo (counterfactual)—assuming continuation of current trends based on the compound annual growth rate (CAGR) observed between 2015 and 2019 using Global Burden of Disease (GBD) data (Institute for Health Metrics and Evaluation 2019)
Scenario 2: SDG-aligned—applying a 33.3% reduction in prevalence from 2015 levels by 2030, consistent with SDG target 3.4 on premature NCD mortality
Scenario 3: GOHAP-aligned—applying a 10% reduction in prevalence from 2023 levels by 2030, aligned with the WHO Global Oral Health Action Plan (2023–2030)
The projections were conducted at the global level and disaggregated across World Bank income groups (low, lower-middle, upper-middle, and high income). The improvement ambition was defined as the absolute difference in projected case numbers between the status quo and each target scenario for each disease.
Data were extracted from the Global Burden of Disease Study (Institute for Health Metrics and Evaluation 2019) and expressed in millions of cases. A geometric growth model was used for future projections, assuming a constant Compound Annual Growth Rate (CAGR) (United Nations 1956).
The status quo projection assumed a constant annual proportion change. The used geometric growth model can be discretely expressed as

where Pt = projected cases after t years, P0 = baseline cases, r = CAGR, and t = number of years from baseline.
CAGR for each oral condition and each region was calculated using the case numbers of 2015 and 2019, shown as follows:

Finally, N2030 (status quo) was calculated using

Results were compiled in tabular and graphical formats for each disease and income region.
Results
Oral Health across the SDGs
The content analysis identified that all 17 SDGs show some degree of relevance to oral health, with direct or indirect connections found in 37 of the 169 official SDG targets. These linkages were analyzed across 4 dimensions: Disease Burden, Determinants, System Integration, and Policy Alignment. The full content mapping is provided in Appendix Material 1.
Results are presented in the heatmap (Fig. 1), with key examples summarized in the highlight table (Table 1).
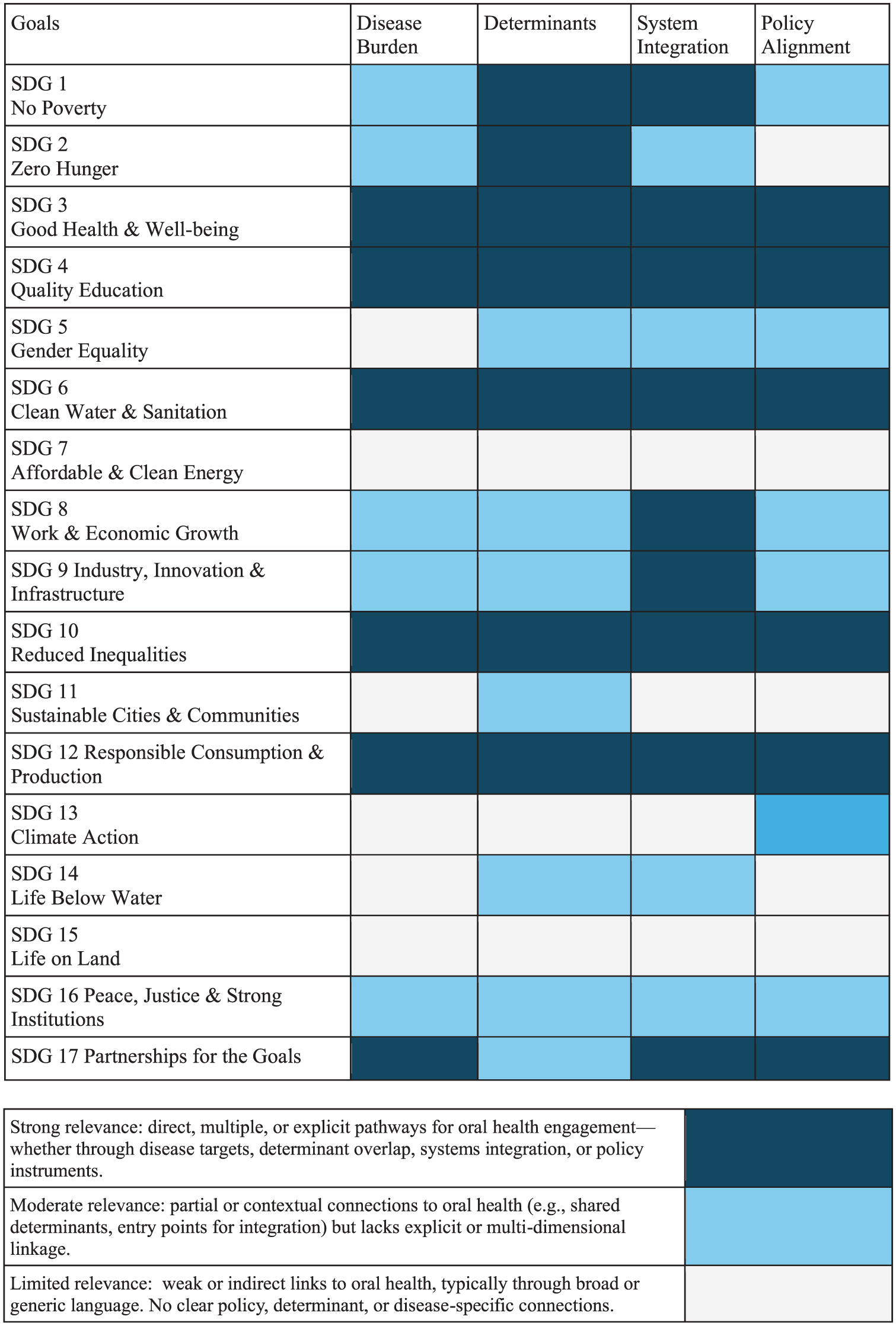
Scoring of oral health links with Sustainable Development Goals.
Four SDGs demonstrated strong and multidimensional relevance to oral health:
SDG 3 (Good Health and Well-being) had the most robust alignment. Targets 3.4 (NCD mortality), 3.8 (UHC), and 3.a (tobacco control) provide clear entry points for oral disease prevention and integration into broader health strategies.
SDG 4 (Quality Education) is linked through the impact of untreated oral disease on education performance, through WASH infrastructure in schools enabling preventive hygiene behaviors like supervised toothbrushing, and through general education levels as a determinant of health.
SDG 6 (Clean Water and Sanitation) is linked through its role in promoting hygiene, access to fluoridated water, and safe clinical environments in schools and health facilities.
SDG 10 (Reduced Inequalities) relates to the social gradient in oral disease burden and access to care, highlighting how income, geography, and other structural inequities shape oral health outcomes.
Three SDGs were assessed as having moderate alignment, with partial but meaningful links across multiple dimensions:
SDG 1 (No Poverty) and SDG 8 (Decent Work and Economic Growth) connect through the financial consequences of untreated oral diseases, including catastrophic health spending, reduced employability, and productivity losses; including poverty as a general determinant of health and disease.
SDG 2 (Zero Hunger) relates to oral health through the bidirectional association between diet, caries risk, and malnutrition, particularly in vulnerable populations such as children and older adults.
SDG 12 (Responsible Consumption and Production) is relevant via the commercial determinants of oral health, especially the production and marketing of sugar, tobacco, and alcohol.
SDG 17 (Partnerships for the Goals) supports the development of multisectoral strategies, financing, and accountability mechanisms for oral health.
Nine additional SDGs were classified as having limited but noteworthy relevance to oral health:
SDG 5 (Gender Equality) highlights disparities in access to oral health services and disease burden by gender, including maternal oral health.
SDG 9 (Industry, Innovation, and Infrastructure) includes emerging relevance through digital oral health technologies and expanded infrastructure for care delivery.
SDG 11 (Sustainable Cities and Communities) reflects the role of housing, urban design, and transport in shaping exposure to oral health risks and access to care.
SDG 13 (Climate Action) and SDG 12 (again, in the environmental context) are relevant in relation to mercury phase-down in dental materials and broader sustainable, environmentally sound practices.
SDG 14 (Life Below Water) and SDG 15 (Life on Land) may be indirectly linked through environmental policies affecting fluoride levels in water sources or exposure to pollutants.
SDG 16 (Peace, Justice, and Strong Institutions) touches on the governance, regulatory, and rights-based aspects of access to oral health services.
Figure 1 presents the comparative scoring across all goals, Table 1 provides a synthesized overview of SDG relevance to oral health, and Appendix Material 1 contains the full qualitative content analysis of the SDG resolution text.
Quantifying the Missed Disease Reductions
By 2030, achieving the SDG-aligned target of one-third prevalence reduction (Table 2 and Fig. 2A) would lead to the following:
Projected Case Numbers and Estimated Reductions across 4 Oral Diseases and World Bank Income Groups.
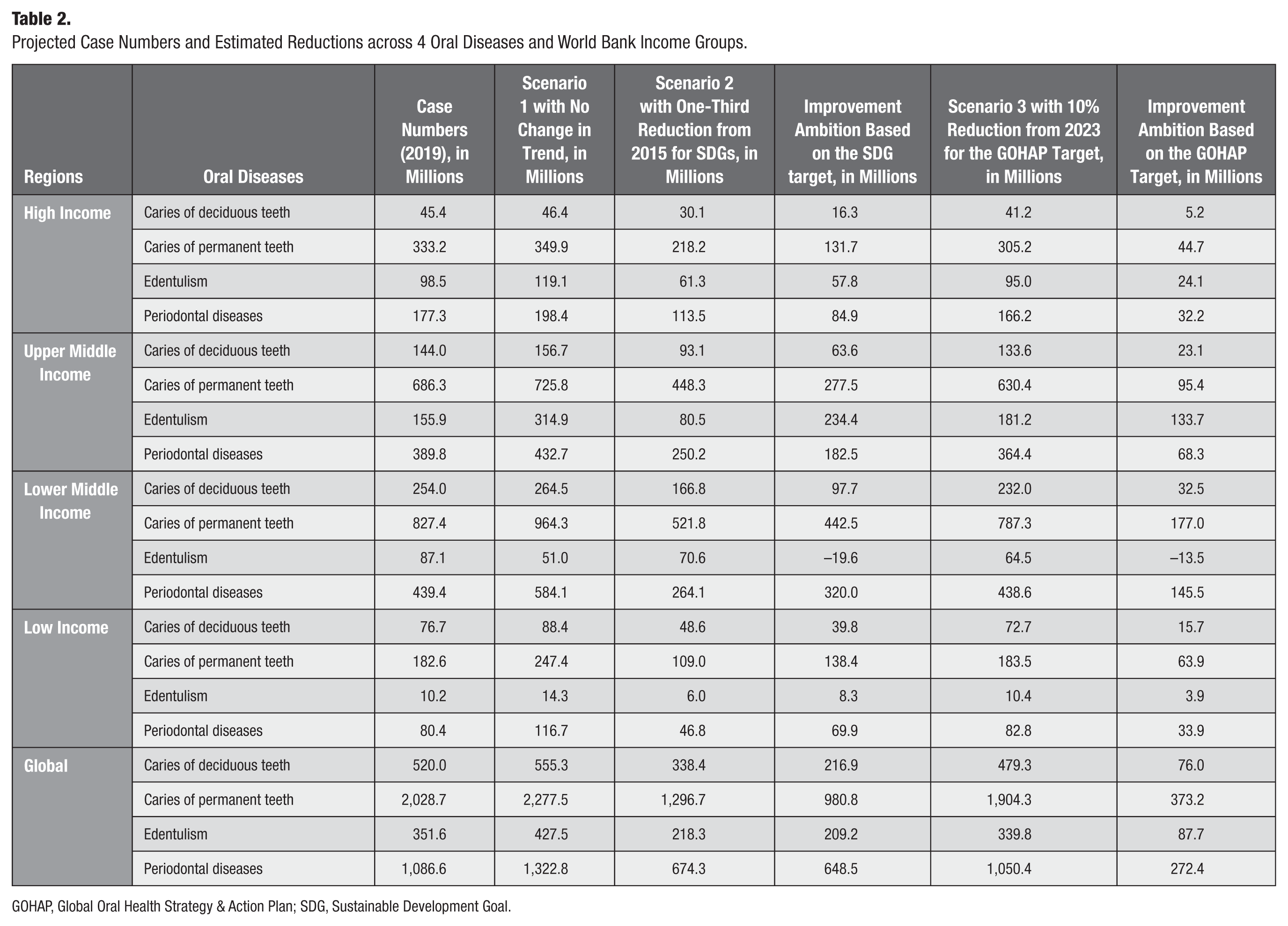
GOHAP, Global Oral Health Strategy & Action Plan; SDG, Sustainable Development Goal.
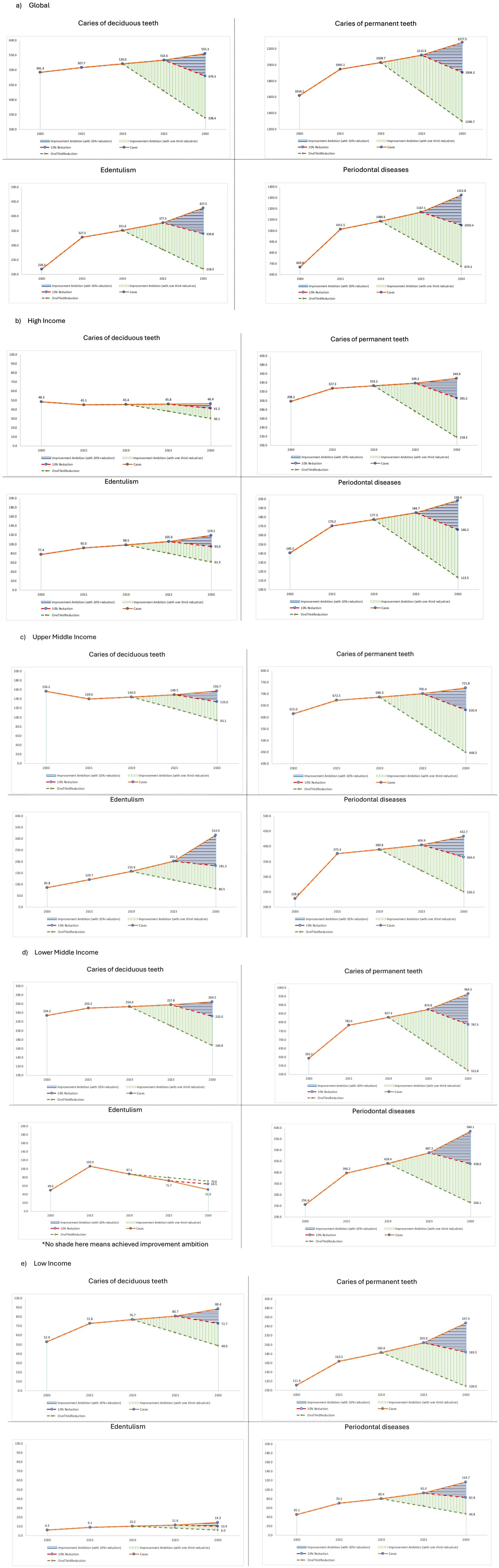
Oral disease burden projections from 2000 to 2030.
981 million cases of caries in permanent teeth
649 million cases of periodontal disease
217 million cases of caries in deciduous teeth
209 million cases of edentulism
Achieving the more conservative GOHAP-aligned target of a 10% reduction (from a higher projected baseline of 2023), disease reductions (Table 2 and Fig. 2A) would remain substantial:
373 million cases of permanent caries
272 million cases of periodontal disease
88 million cases of edentulism
76 million cases of deciduous caries
The case reductions under the GOHAP scenario reflect cumulative increases in projected burden under the status quo and changes in the realized target, highlighting the scale of action required to meet them.
Regional variation reveals stark disparities:
Low-income countries face over 40% projected growth in permanent caries by 2030 without intervention. Even a 10% reduction could prevent over 100 million cases across all 4 conditions (Table 2 and Fig. 2E).
Lower-middle-income countries exhibit the highest absolute number of preventable cases, especially for permanent caries and periodontal disease. Under the SDG scenario, the combined improvement ambition exceeds 750 million cases (Table 2 and Fig. 2D).
Upper-middle-income countries are on track for a near doubling of edentulism, indicating urgent needs for rehabilitative services and preventive aging strategies (Table 2 and Fig. 2C).
High-income countries show more stable incidence levels, with smaller absolute reductions but meaningful gains in periodontal disease and permanent caries prevention (Table 2 and Fig. 2B).
Full case projections and reduction estimates by disease and World Bank income groups are provided in Table 2 and Figure 2, which include the SDG and GOHAP scenarios and quantify the scale of improvement ambition under each target (Fig. 3A, B).

Heatmaps for improvement ambition.
Discussion
Despite decades of declarations, resolutions, and reform calls, oral health remains structurally sidelined from the mainstream of global health and development agendas. This study quantifies the cost of that exclusion in terms of missed disease reduction, while also demonstrating that integrating oral health into SDG implementation frameworks would be both feasible and overdue.
By systematically mapping how oral health relates to SDG targets, we show a broad and meaningful intersection with the 2030 agenda. Oral health is relevant to all 17 goals and 37 of the official 169 targets. The alignment is strongest with SDG 3 (health), SDG 4 (education), SDG 6 (WASH), and SDG 10 (inequality) but extends to areas such as nutrition, economic productivity, sustainable consumption, and governance. This is consistent with parallel frameworks on the commercial and social determinants of oral health, as well as the common risk factor framework, but has not, until now, been applied systematically to the SDG framework itself.
Our modeling adds a second layer: it estimates the gap between the current trajectory and 2 global targets: 1 defined under the SDG umbrella (a 33.3% reduction in NCDs) and 1 under the Global Oral Health Action Plan (a 10% reduction in oral disease prevalence). The results are striking: if oral health were included in these global efforts and fully implemented, this would avert up to 981 million cases of permanent caries and 649 million cases of periodontal disease by 2030. These figures transform political invisibility into epidemiological urgency.
Although oral diseases affect people across all regions and income groups, the burden and the opportunity for improvement are far from evenly distributed. By applying both the SDG and GOHAP targets across World Bank income groupings, our analysis reveals stark regional disparities in disease burden, projected trends, and potential reductions. These differences underscore the urgent need for context-specific strategies and for a more equitable distribution of attention, resources, and accountability within global oral health efforts. It also demands evaluation and reflection on currently available interventions and investments, and whether those are adequate.
Across all 4 disease categories, the case numbers are projected to increase substantially in low- and middle-income countries (LMICs) under the status quo. For instance, by 2030:
Permanent caries cases are expected to grow by over 40% in low-income countries, with similar trends in lower-middle-income settings.
Periodontal disease is projected to increase sharply, especially in lower-middle-income regions, where growth between 2015 and 2019 already exceeded 10%.
Edentulism is rising fast in upper-middle-income countries, where a near doubling is projected by 2030 if current trends persist.
When comparing target scenarios to the counterfactual projections, the concept of improvement ambition highlights not only the scale of the challenge but also the moral geography of missed potential:
In low-income countries, a 10% reduction (GOHAP) would prevent over 100 million cases of oral disease by 2030.
In lower-middle-income countries, improvement ambition is even higher, especially for periodontal disease and permanent caries, where the gap between trend and target exceeds 750 million cases combined under the SDG scenario.
In high-income countries, the ambition remains significant, but the relative gains are smaller, reflecting both plateauing incidence and historically greater access to care.
These findings demonstrate that the burden of inaction is disproportionately borne by LMICs, where oral health services are least available and the health system capacity to respond is weakest. If left unaddressed, this will not only deepen global health inequalities (SDG 10) but also undercut progress on SDG 1 (poverty), SDG 3 (health), and SDG 8 (economic productivity). In this context, the GOHAP target of a 10% reduction may be more politically achievable than the SDG-aligned 33.3% benchmark, but both require levels of action and investment not yet visible in most countries.
Several studies have made the case that oral health is relevant to the SDGs, arguing that oral health is linked to the broad development outcomes defined in the SDGs (Benzian and Listl 2022; Huang and Chang 2022; Abodunrin et al 2023; Benzian 2023; Benzian and Mathur 2023; Folayan et al 2023a, 2023b; Sun et al 2023; Crystal et al 2024; Folayan et al 2024a, 2024b; El Tantawi et al 2024a, 2024b). These publications contributed to greater awareness, but none have attempted a comprehensive mapping of SDG linkages combined with scenario modeling of disease reduction.
Our study builds on and extends this work by introducing an analytical framework that merges content analysis with burden projections. In doing so, we move from rhetorical recognition to quantifiable benchmarks and accountability. The concept of “improvement ambition” offers a new framing for global oral health: a way to articulate both the scale of the challenge and the opportunity for impact. Much like the “lives saved” framing in maternal and child health, improvement ambition quantifies what is possible, not just what is happening. It allows policymakers and advocates to benchmark progress, model return on investment, and align oral health action with global accountability frameworks. It converts an abstract policy target into a measurable implementation gap. For policymakers, the metric can be used to identify how far current trajectories are from agreed or aspirational targets, which conditions contribute most to the gap, and where the largest preventable burden lies by income group or country. This makes it useful for prioritizing action within national oral health strategies, NCD plans, UHC benefit package design, school health programs, WASH-linked prevention, and investment cases. Rather than simply reporting disease burden, the metric asks a more policy-relevant question: how much disease could be avoided if current trajectories were shifted toward agreed benchmarks?
For researchers and monitoring agencies, the metric can be updated as new GBD estimates, national oral health surveys, or administrative data become available. It can also be disaggregated by age, sex, socioeconomic position, geography, or service coverage, where data permit. In this way, “improvement ambition” is not intended as a precise forecast but as a transparent planning and accountability tool. It can help track whether oral health policies are narrowing the gap between projected burden and global targets, and whether progress is occurring equitably across populations.
This framing is especially powerful because it converts a passive absence (oral health not being included) into an active shortfall: cases that could have been averted, inequalities that could have been reduced, and costs that could have been avoided. These ambitions vary substantially across regions and income groups, revealing not only global urgency but also the need for tailored strategies.
Governance, Advocacy, and the SDGs
This study highlights a central paradox: oral health is highly relevant to the SDGs, with strong potential for disease reduction, yet progress remains negligible. This reflects deeper structural and political, institutional, and historical dynamics that have shaped both the SDG architecture and the trajectory of oral health advocacy.
When the SDGs were adopted in 2015, they were shaped through a highly political, consensus-driven process. Sectors with coordinated advocacy, strong institutional allies, and clear political asks secured visibility (Hickmann et al 2023). Oral health lacked all three. There was no unified constituency, no embedded presence in global negotiations, and no strategic framing aligned with the broader development agenda.
Since then, progress has been made. The WHO resolution on oral health (2021), the Global Oral Health Status Report (2022), and the GOHAP (2024) signal growing institutional recognition (World Health Assembly 2021; WHO 2022, 2024). But these gains remain fragmented. Oral health continues to be underrepresented in national health strategies, financing frameworks, and global accountability systems.
Critically, oral health advocacy has not yet achieved the level of “issue salience” seen in other global health fields (Wlezien 2005). Unlike HIV, maternal health, or UHC, oral health lacks broad coalitions, civil society engagement, and political entrepreneurship. Its claims remain technically valid but politically peripheral (Shiffman 2009; Benzian et al 2011; Shiffman and Shawar 2022).
The absence of indicators has compounded this marginalization. Without metrics, there is no mandate; without a mandate, there is neither funding nor accountability. Global financing tends to favor issues with clear metrics, wide coalitions, and demonstrable cross-sector impact; oral health has not yet met these criteria in the SDG era. To change this, oral health must move from technical consensus to political strategy. Integration into SDG implementation will require stronger coalitions, clearer narratives, and meaningful participation in governance and financing platforms, not as an add-on, but as essential to equitable health and development.
Policy Implications for SDG-Aligned Oral Health Action
The findings point to several practical steps for moving oral health from rhetorical inclusion to measurable SDG implementation. First, oral health should be framed as a marker of social progress, equity, and health system performance rather than as a narrow dental service issue (Listl and Bärnighausen 2025). Second, essential oral health services should be integrated into UHC benefit packages, primary health care, school health platforms, and essential medicines and technologies lists (Listl et al 2021; Christian et al 2023). Third, oral health should be embedded in SDG-aligned national planning processes, including voluntary national reviews, NCD strategies, WASH programs, nutrition policies, and primary health care reforms. Fourth, countries and global agencies should strengthen integrated surveillance by including oral health indicators in national health information systems and global monitoring frameworks. Fifth, investment cases should explicitly link oral health to productivity, poverty reduction, educational participation, and human development. Finally, oral health advocacy needs broader multisectoral coalitions that connect dental public health with education, WASH, nutrition, NCD prevention, aging, disability, and equity movements. These steps would align oral health more closely with the governance and accountability mechanisms that shape SDG implementation.
Limitations
Several limitations must be acknowledged. The SDG mapping relies on interpretive reading of policy language and does not represent a systematic meta-analysis of empirical data. The scoring system used in the heatmap is illustrative, based on a structured, theory-informed framework and expert judgment rather than formal qualitative coding procedures. While this approach enables a nuanced interpretation of policy language, it may introduce subjectivity in the categorization of linkages despite the use of predefined dimensions and consensus-based validation.
The disease projections are based on a continuation of past growth rates and do not model more complex interactions such as changes in population age structure, access to care, or health system responses. The underlying GBD estimates are modeled with uncertainty, particularly in low-income settings with sparse primary data. Nonetheless, the combination of content analysis with scenario modeling provides a robust foundation for the conclusions drawn and fills a gap in the global oral health evidence base. Finally, this is a broad analysis using global data, primarily for policymaking and advocacy, and quantifies the gap between projected burden and policy benchmarks. This is not an analysis to evaluate the current public or global health programs.
Conclusion
Oral health remains both a glaring omission and a strategic opportunity within the 2030 Sustainable Development Agenda. This study demonstrates that oral health is deeply interwoven with the SDGs—not only through its burden and shared risk factors but also via its relevance to systems integration, equity, and human development. By quantifying what could be achieved through alignment with global targets, we show that millions or even billions of cases could be prevented by 2030. These figures are not merely epidemiological abstractions; they represent tangible improvements in quality of life, productivity, and health system efficiency. The introduction of a clear improvement ambition offers a new way to frame progress and mobilize accountability in a space that has long lacked both.
The next 5 years are critical. Achieving the promise of the SDGs will require oral health to be embedded within UHC, NCD prevention, WASH, nutrition, education, and equity agendas—not as an add-on but as part of mainstream health and development policy. If oral health continues to be excluded, global health and development goals will remain incomplete (Benzian et al 2025). But with strategic integration and political will, oral health can become a powerful lever for delivering on the SDGs’ central promise: health and well-being for all by 2030.
Author Contributions
M.R. Mathur, S.S. Syed, D. Nagrath, H. Benzian, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript; S. Listl, contributed to conception, data interpretation, drafted and critically revised the manuscript; V.K. Mishra, contributed to conception, data analysis, drafted the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work, ensuring integrity and accuracy.
Supplemental Material
sj-docx-1-jct-10.1177_23800844261455290 – Supplemental material for Oral Health and the SDGs: Unlocking Missed Potential for Global Health Gains
Supplemental material, sj-docx-1-jct-10.1177_23800844261455290 for Oral Health and the SDGs: Unlocking Missed Potential for Global Health Gains by M.R. Mathur, S. Listl, S.S. Syed, D. Nagrath, V.K. Mishra and H. Benzian in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not required for this study.
Data Availability
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.