
Abstract
Background:
Adolescents and young adults (AYA) comprise 50% of sexually transmitted infections (STIs) diagnosed annually. AYA frequently access emergency departments (EDs) for health care. Thus, the ED could be a strategic venue for the diagnosis and treatment of STIs.
Objective:
Cost-effectiveness analysis examining screening strategies for Chlamydia trachomatis and Neisseria gonorrhea (CT/GC).
Design:
Decision analytic cost-effectiveness model.
Setting:
Six pediatric EDs.
Participants:
AYA 15 to 21 y of age seeking acute care at pediatric EDs.
Interventions:
1) Usual care, 2) targeted screening (using a computerized sexual health survey), and 3) universally offered screening.
Main Outcomes and Measures:
Cost in 2024 US dollars and effectiveness measured as STIs detected and successfully treated. Secondary effectiveness outcome metric: quality-adjusted life-years (QALYs). The cost perspective is the direct health care sector, and the time horizon is lifelong.
Results:
Targeted screening was the most effective and most costly (incremental cost-effectiveness ratio [ICER] of $517 per case detected and successfully treated). In a secondary analysis using QALYs lost for long-term complications of untreated CT/GC, targeted screening had an ICER of $23,320/QALY. In this analysis, usual care was dominated, being more costly and less effective than universally offered screening. In subgroup analyses of female versus male, only cohorts using $/QALY, targeted screening remained highly cost-effective for females ($6,389/QALY) compared with universally offered screening but was not cost-effective in males.
Conclusions and Relevance:
Targeted screening is a highly cost-effective strategy for detecting and treating STIs in adolescents seeking pediatric ED care compared with universally offered screening, with an ICER of $517 per case detected and treated. When considering quality of life for female- versus male-only subgroups, screening for males becomes less clear.

Keywords
Highlights
Adolescents and young adults (AYA) comprise 50% of diagnosed sexually transmitted infections (STIs) annually.
AYA frequently access emergency departments (ED) for health care.
We examined the cost-effectiveness of using the pediatric ED as a strategic venue for the diagnosis and treatment of STIs.
We found that targeted screening using a computerized sexual health survey to derive STI risk and provide EHR-embedded clinical decision support was highly cost-effective for detecting and treating STIs in adolescents seeking pediatric ED care compared with universally offered screening.
Introduction
Although adolescents and young adults (AYA) represent only 25% of the sexually active population, they comprise nearly 50% of all diagnosed sexually transmitted infections (STIs). Of the 20 million new cases of STIs each year, 10 million occur among AYA. 1 Failure to diagnose and treat STIs in a timely manner can result in reproductive morbidity, including pelvic inflammatory disease (PID), ectopic pregnancy, infertility, and facilitation of transmission of human immunodeficiency virus (HIV). AYA frequently access emergency departments (EDs) for health care. Furthermore, the ED functions as the primary source of health care for more than 1.5 million AYA.2 –4 Thus, the ED could be a strategic venue for the diagnosis and treatment of STIs.
Despite high rates of STIs among AYA seeking ED care, 5 ED-based STI screening is not yet routine. Given the hectic and nonprivate nature of the ED, STI screening can be challenging. Unlike HIV screening, for which the Centers for Disease Control and Prevention (CDC) recommends universal opt-out screening for all patients ≥13 y in the ED setting, 6 there are currently no CDC recommendations for ED-based Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (GC) screening. Screening for STIs can be offered universally to AYA or to some using a targeted approach based on sexual risk behaviors and/or chief complaint.
As part of a multicenter study at 6 sites within the Pediatric Emergency Care Applied Research Network (PECARN), we conducted a pragmatic trial to assess the clinical and cost-effectiveness of 3 GC/CT screening strategies (usual care, targeted screening, and universal screening) when integrated into routine ED clinical care. During the universally offered screening intervention, STI screening was offered to all participants, and clinical decision support for testing was based solely on the patient’s decision to undergo testing (survey results were not available to clinicians). During the targeted screening intervention, a validated risk score derived from the survey based on patient-reported behavioral data was integrated into the electronic health record to provide clinical decision support for gonorrhea and chlamydia testing. 7 As part of this project, we examined the cost-effectiveness of CT/GC screening strategies for AYA visiting pediatric EDs for acute care. We constructed a decision analytic model using data from the clinical trial combined with literature-based estimates for other key parameters.
Methods
Analyses
Our health economics analysis plan was developed in accordance with the CHEERS 2022 guidelines and follows the conduct recommendations from the Second Panel of Cost-Effectiveness in Health and Medicine. 8 Our base-case analysis examined the incremental cost-effectiveness ratio (ICER) of increasingly more expensive strategies. The ICER reflects cost per infection detected and successfully treated. In a secondary analysis, we calculated the ICER as cost per quality-adjusted life-year (QALY) gained. We performed both deterministic and probabilistic sensitivity analyses. We conducted probabilistic sensitivity analyses using 10,000 iterations of a second-order Monte Carlo simulation, using distributions for most parameter values in the decision model (see online supplement). We performed deterministic sensitivity analyses to examine the impact of parameter uncertainty or variation in settings, such as varying the prevalence of STI in different geographic locations or settings (eg, urban vs suburban vs rural). In addition, we performed subgroup analyses of female- versus male-only cohorts.
Our study population and setting included AYA 15 to 21 y of age seeking acute care at pediatric EDs. We developed a decision analytic model to simulate events and outcomes of 3 CT/GC screening strategies. The comparators included 1) usual care, 2) targeted screening (using a computerized, patient-reported validated sexual health survey [cSHS] to derive STI risk and provide electronic health record–embedded clinical decision support), and 3) universally offered screening (using a computerized survey to assess patient acceptance of STI screening to provide clinical decision support). During targeted screening, a risk score derived from the cSHS was integrated into the EHR to provide clinical decision support (CDS) for CT/GC screening. When high-risk scores were generated, clinicians received CDS that CT/GC testing was highly recommended; at-risk scores generated a CDS that CT/GC testing was recommended; and low-risk scores and those who did not complete the survey did not trigger any CDS. The clinician then discussed the recommendation with the patient. The clinician could choose either to follow the screening recommendation or not. During the universally offered phase, CT/GC screening was offered to all eligible participants. All participants were informed of the CDC CT/GC testing recommendations and given the option on the tablet to accept GC/CT testing. They then completed the cSHS. Results from the cSHS were not available to the clinician. CDS for CT/GC testing was based solely on the patient’s decision to undergo testing. Once again, clinicians could choose either to follow the CDS recommendation or not.
The study perspective was the health care sector, as we did not have information from the companion clinical trial regarding time spent in the pediatric ED for patients in each of the study arms. Travel time to the ED was not relevant, as patients in all study arms had already made a trip to the ED. We used a lifetime time horizon for our analysis, as the late sequalae of STIs in women may last years and occur later in life.
Outcome metrics included costs in 2024 US dollars and effectiveness measured as STIs detected and successfully treated. In a secondary analysis, we used quality-adjusted life expectancy as an outcome. Costs of long-term complications resulting from epididymitis and PID, such as infertility, ectopic pregnancy, and chronic pelvic pain, were discounted at 3% per year.
This study was approved by the University of Utah’s Institutional Review Board using a single institutional review board mechanism for reliance across all participating sites.
Clinical Outcomes of STIs
Precise estimates of long-term sequelae of both CT and GC infections are difficult to determine. An analysis of direct medical costs in the United States estimated that PID develops in 15% of untreated women with either CT or GC infections, while epididymitis develops in 1.5% of untreated men with either STI (see Supplementary Table 3). 9 Recommended treatment for CT is a single 1-g oral dose of azithromycin or 100 mg of doxycycline twice daily for 7 d. 10 Treatment efficacy is 97%. Recommended treatment for uncomplicated GC infections is a single 250-mg dose of ceftriaxone intramuscularly and 1 g of oral azithromycin. 11 Reported cure rates for uncomplicated urogenital infections is 99%. However, STI management and ED follow-up are challenging. Studies have reported loss to follow-up ranging between 8% and 32%. 12 For the secondary analysis using $/QALY, we used data from a study that estimated the lifetime QALYs lost due to chlamydia, gonorrhea, and trichomoniasis in the United States in 2018. 13 For women with long-term complications of untreated chlamydia or gonorrhea, the average discounted loss of QALYs was 2.29, while for men it was 0.006 QALYS (see electronic Supplementary Table 4).
Costs
Major costs for the 3 strategies considered include direct costs of testing and treatment for those diagnosed with infection, along with the costs of sequelae of either untreated or unsuccessfully treated infection including PID and epididymitis (see Supplementary Table 3). Direct costs of screening tests were obtained from the Centers for Medicare and Medicaid Services. 14 Costs of physician services, such as ED visits, were obtained from the Centers for Medicare and Medicaid Services and included professional and facility components.15,16 Costs of additional ED physician time were based on average US salary data for pediatric ED physicians. 17 Costs of long-term complications of STIs were obtained from a study of insurance claims published in 2006. 18 These costs from 1999 and 2000 were inflated to 2024 costs, using the health care component of the personal consumption expenditure for the appropriate years. 19 Drug costs were obtained from the Veterans Administration federal supply schedule. 20
Decision Model
We used a computer program (DECISION MAKER, Boston, MA, USA) to develop a decision analytic model, analyze decision trees, and perform sensitivity analyses. 21 We considered 3 strategies (Figure 1a–c) for a patient population of adolescent males and females presenting to pediatric EDs for acute care visits:
Usual care
Targeted screening
Universally offered screening
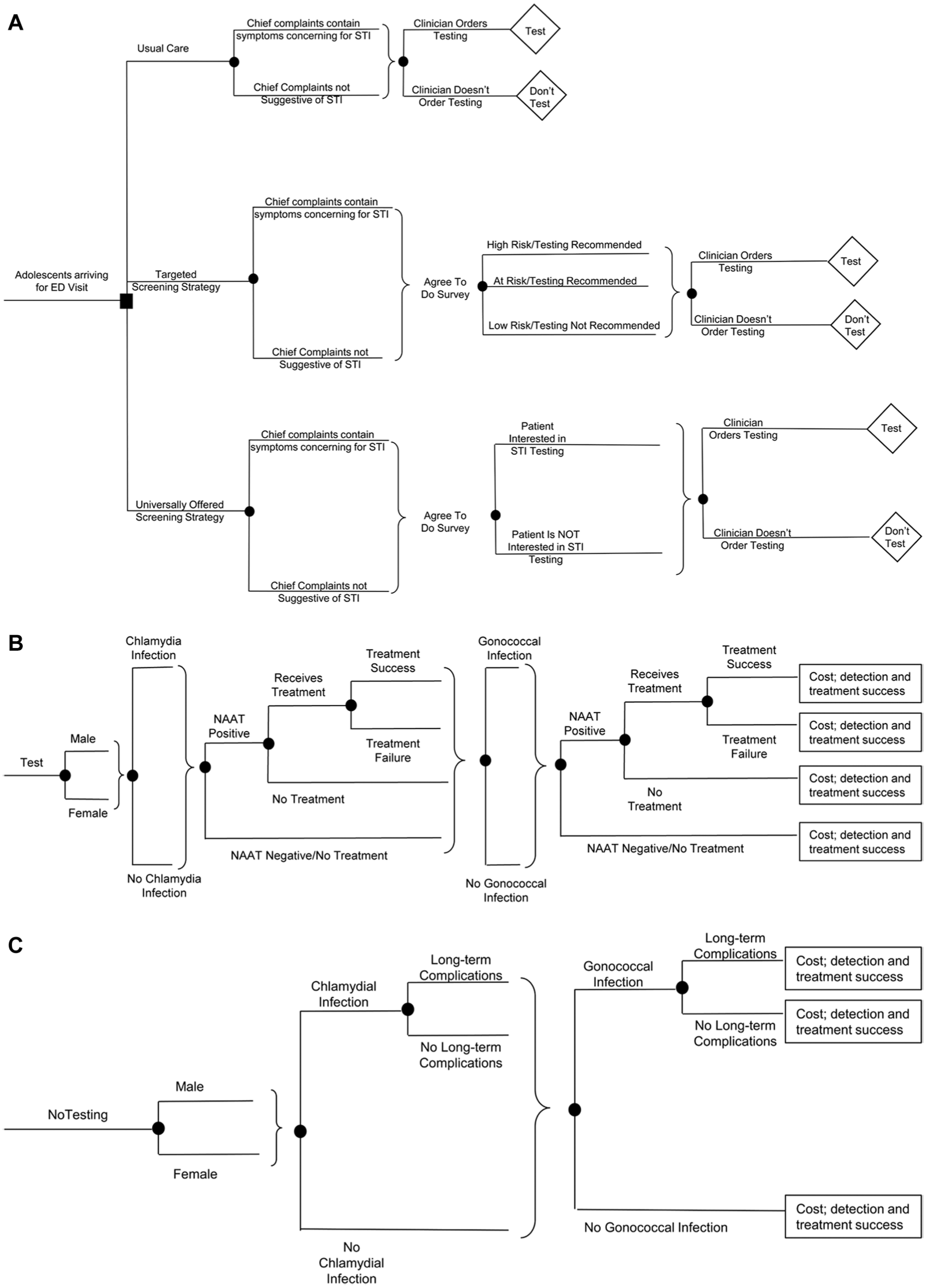
Panel a – The context of the analysis are adolescents between the ages of 15 and 21, seeking acute care at pediatric emergency departments. The 3 strategies shown at the square decision node include: 1) usual care, 2) targeted screening using an STI prediction tool, and 3) universally offered screening. Round nodes represent chance events. In the usual care strategy, patients who have symptoms or are concerned about possible STI undergo testing, represented by the diamond labelled “Test”. In all strategies patients present with chief complaints that are or are not suggestive of an STI. In the Usual Care strategy, clinicians may order or not order STI testing. In the Targeted Screening strategy patients who agree to complete the computerized sexual health survey are risk stratified into one of three groups – high risk, at risk, or low risk. The screening tool recommends to the examining clinician that those who are at high risk or at risk should be tested. The clinician has the option to order testing following receipt of results of STI risk stratification. In the Universally Offered Screening strategy, patients who have completed the computerized sexual health survey may or may not be interested in having STI testing. Once again, the examining clinician may or may not follow through with testing.
Results
Study Parameters
For information on study parameters, see electronic Supplementary Tables 1 through 3.
Prevalence of STIs
CDC data show marked variation in the incidence and prevalence of STIs by age category. Case rates for both CT and GC are highest among AYA between the ages of 20 and 24 y, with roughly similar rates of GC in both females and males, 873.2 and 844.2 per 100,000, respectively. Reported cases of CT are much higher in females than in males, 3,797.8 and 1,680.0 per 100,000 respectively.10,22 If one assumes that AYA who present to pediatric EDs for acute visits reflects the broader population, the estimated probability of STI among patients not specifically seeking attention for STI symptoms is roughly 3.6%. In our PECARN study, the prevalence of CT and GC infection among patients who were tested was 16.4% and 6.4%, respectively. 23 The prevalence of CT and GC among the 14% of patients with a chief complaint including possible symptoms of an STI was 18.9% and 8.3%, respectively, while the prevalence among patients without reported symptoms of an STI was 14.2% and 4.8% respectively. 23 We further calculated the STI prevalence among male and female patients, with and without symptoms of an STI (see Supplementary Table 1). In the targeted screening strategy, we were able to calculate the prevalence of CT and GC across subcategories of patients with and without symptoms of an STI including high risk, at risk, and low risk (as assessed by the survey), as well as among those who rejected the survey or to whom the survey was not offered. To estimate the probability of CT and GC in patients who were not tested, we back-calculated probabilities based on the average prevalence among tested patients in each strategy and the proportion of patients in each strategy tested, so that the overall probability of disease in each strategy was equal to the reported prevalence in CDC data among 20- to 24-y-old AYAs.
Risk estimation
Patients in the targeted screening arm completed a survey that was used to inform an STI risk assessment. The results of this risk assessment were then used to trigger an electronic health record–embedded CDS tool, providing results to clinicians that would inform their decisions to obtain CT/GC testing. As noted above, Supplementary Table 1 reports the probability of CT and GC in each of these risk groups. The probability of patients being at high risk was 58.8% and 24.3%, respectively, among patients with and without symptoms of an STI. Probabilities for the other risk strata are reported in Supplementary Table 2.
Probability of clinicians ordering STI testing
We obtained data on the probability of clinicians ordering STI testing in the usual care and universally offered screening strategies among patients with and without symptoms of an STI (see Supplementary Table 2). In the targeted screening strategy, we further divided patients into the CDS calculated risk groups (high risk, at risk, low risk). Across all these groups, the probability of clinicians ordering testing ranged between 2.0% and 55.2%.
Probability of being interested in STI testing
In the universally offered screening strategy, patients were asked whether they were interested in being tested for an STI (see Supplementary Table 2). As shown in the decision tree model (Figure 1), clinicians were still free to make decisions whether to order testing or not. Twenty-eight percent of patients with symptoms of an STI and 18% of those without symptoms of an STI consented to testing.
Characteristics of urine nucleic acid amplification tests (NAAT)
The CDC-recommended method for testing for CT and GC infection is NAAT of urine specimens. 24 Diagnostic accuracy is relatively good. The specificity for CT and GC is ≥97% (see Supplementary Table 3). The sensitivity for CT ranges between 86% and 00%, while the sensitivity for GC ranges between 91% and 100%.25,26
Summary of Main Results
In the base case (see Table 1), using an overall STI prevalence of 3.6% for a hypothetical ED population of 10,000 adolescent patient visits, universally offered screening was least costly ($244,734), usual care was next most costly ($262,197), and targeted screening was most expensive ($315,026). Universally offered screening resulted in the detection and treatment of 162 STIs. Usual care detected and treated 173 STIs, while targeted screening detected and treated 297 STIs. The incremental cost-effectiveness (ICER) of targeted screening versus universally offered screening was $517 per case identified and successfully treated. Usual care was eliminated by extended dominance, having an ICER greater than that of targeted screening versus universally offered screening. In a population of 10,000 ED patient visits, with an average overall prevalence of 3.6%, the total number of cases is 360. Another way to consider these results is by the proportion of STI patients identified and treated successfully. Thus, universally offered screening results in the detection and successful treatment of 45.0% (162/360) of STIs, while usual care and targeted screening result in the detection and successful treatment of 48.0% (173/360) and 82.5% (297/360) of STIs, respectively.
Results of the Base-Case Analysis.
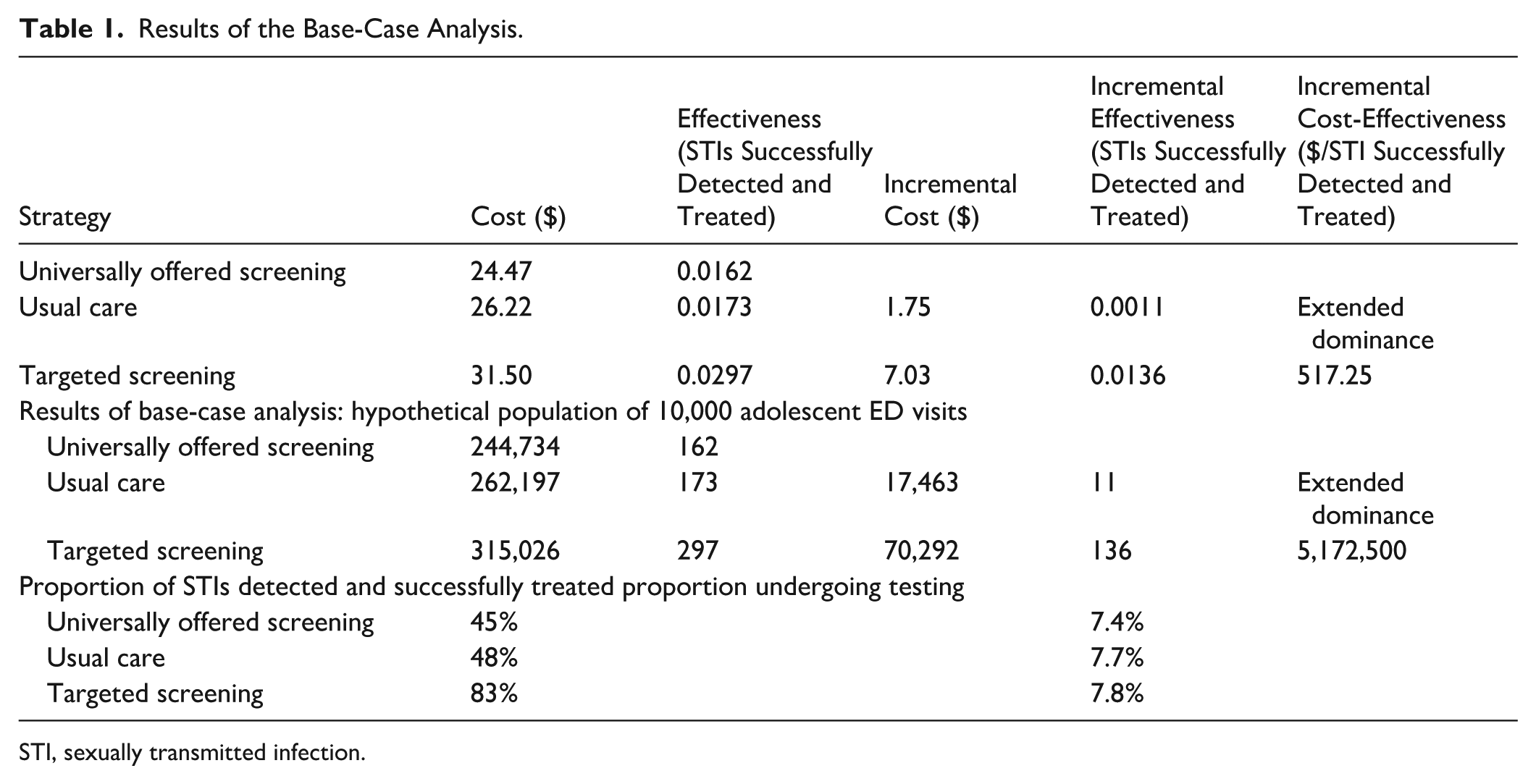
STI, sexually transmitted infection.
We performed a secondary analysis using QALYs lost due to complications of untreated chlamydia or gonorrhea as our outcome metric for effectiveness, rather than cases detected and successfully treated. In this analysis, targeted screening had an ICER of $23,320/QALY gained versus universally offered screening. As in the base-case analysis, usual care was dominated, being more costly and less effective than universally offered screening (see Table 2).
Results of the Scenario Analysis $/QALY.
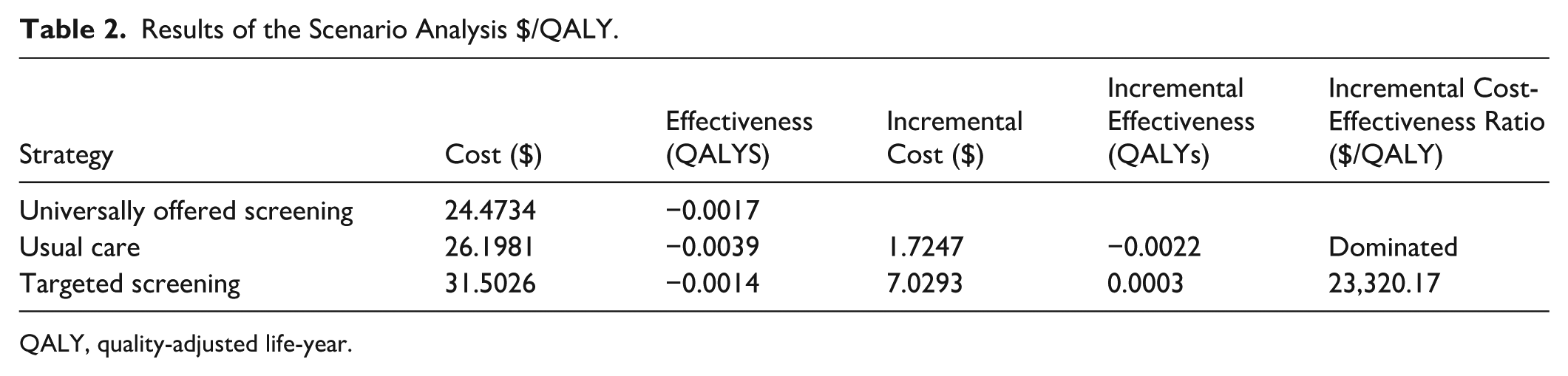
QALY, quality-adjusted life-year.
Deterministic sensitivity and scenario analyses
Key parameters affecting the analysis include the probability of STI, the probability that patients in the universally offered screening strategy are interested in STI testing, and the probability that clinicians order STI testing. Figure 2 shows the ICER for targeted screening versus usual care and universally offered screening as a function of the probability of STI among adolescents coming to the ED. At the base case of STI prevalence of 3.6%, targeted screening is highly cost-effective. However, as the probability of STI decreases, the ICER for targeted screening rapidly increases, making it a less cost-effective strategy in lower prevalence settings. Figure 3 examines the probability that patients in the universally offered screening strategy are interested in STI testing. At the base-case value of 28%, targeted screening is highly cost-effective. However, as this probability increases beyond 58%, universally offered screening becomes a more effective but still costlier alternative to targeted screening. Figure 4 examines the probability that clinicians in the usual care strategy order STI testing. At the base-case probability of 24% for patients with symptoms suggestive of STI and 4% for patients without symptoms of STI, targeted screening is highly cost-effective. However, if the probability that clinicians order STI testing exceeds 42%, usual care becomes more effective, albeit more costly than targeted screening.
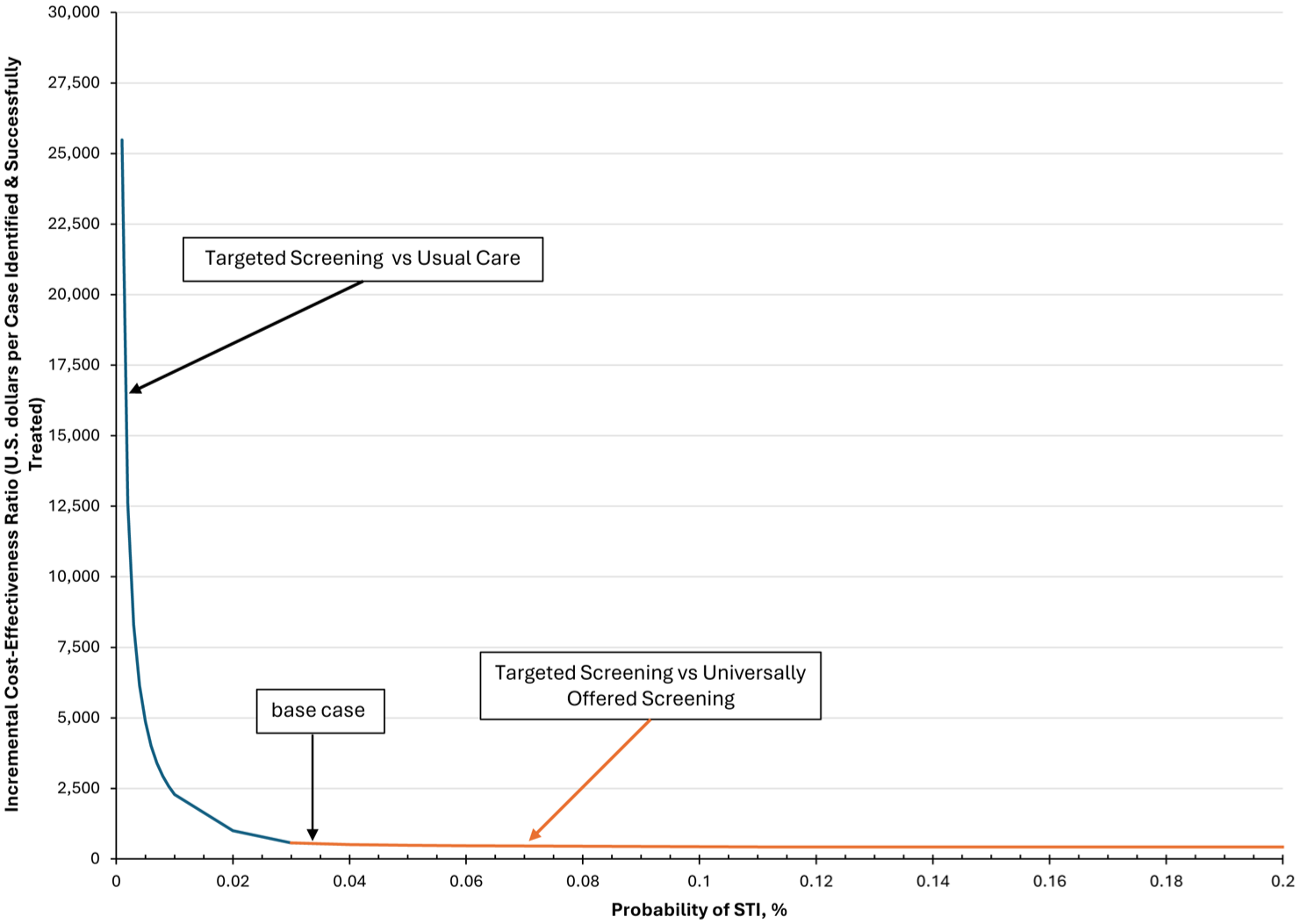
One-way sensitivity analysis of the probability of STI.

One-way sensitivity analysis of probability that patients in the Universally Offered Screening strategy are interested in STI testing.

One-way sensitivity analysis of the probability that clinicians in the usual care strategy order sexually transmitted infection (STI) testing.
We also performed scenario subgroup analyses calculating outcomes for an only female versus an only male population cohort. When considering an only female population, the ICER for targeted screening compared with universally offered screening is $569 per case identified and successfully treated. For a male-only population Universally offered screening becomes more costly and less effective than usual care; thus, the ICER for targeted screening is now calculated compared with usual care at $534. We performed the same subgroup cohort analysis using an outcome metric of QALYs. For a female-only cohort, targeted screening had an ICER of $6,389/QALY compared with universally offered screening. For a male-only cohort, targeted screening was dominated, being more costly and less effective than universally offered screening. While universally offered screening was the most effective strategy, it had an unacceptably high ICER of $5,061,725/QALY compared with usual care. The discrepancy between results using cases detected and successfully treated versus QALYs is likely due to the small impact untreated GC or CT has on males as compared with the impact on females. It is important to note that the analysis using QALYs as the effectiveness outcome does not account for the negative public health impact of untreated STIs.
Finally, we performed a scenario analysis that conservatively assumed that physician staff would spend an extra 15 min of time in discussion with patients for whom they ordered STI testing in the targeted screening and universally offered screening strategies. For this scenario analysis, we did not assume any additional physician or staff costs for the usual care strategy. Using the decision model that calculated the ICER in terms of $/QALY, targeted screening had an ICER of $26,770/QALY versus universally offered screening.
Probabilistic sensitivity analysis
We performed a probabilistic sensitivity analysis using 10,000 iterations of a second-order Monte Carlo simulation (Figure 5). Targeted screening is favored across a wide range of willingness-to-pay (WTP) thresholds above $450 per case detected and successfully treated, while universally offered screening is favored below a WTP of $450. At a WTP of $450, both targeted screening and universally offered screening are cost-effective in 38% of simulations. Usual care is never most cost-effective.

Cost-effectiveness acceptability curve.
Discussion
Adolescents frequently access EDs for health care. We explored the use of ED visits as a strategic venue for the diagnosis and treatment of STIs. We found that targeted screening was the most effective although most costly strategy with an ICER of $517 compared with universally offered screening. In a hypothetical population of 10,000 adolescents, targeted screening and universally offered screening resulted in the identification and successful treatment of 297/360 (83%) and 162/360 (45%), at a cost of $315,026 and $244,734, respectively.
The prevalence of CT/GC is a major factor influencing the effectiveness and cost-effectiveness of screening. Some studies site an increased risk of STI ranging between 2% and 15%, suggesting that those seeking acute care in EDs represent an enriched population with respect to STIs. 12 Other cost-effectiveness analyses have assumed CT/GC prevalence as high as 13.6% for an ED population. 27 We used a conservative estimate of 3.6%, based on surveillance data from the CDC for adolescents between the ages of 15 and 21 y. Such an estimate would, if anything, bias our results against universally offered or targeted screening. We assumed that the prevalence of CT/GC among adolescents using the ED for a variety of acute care issues would mirror the overall population prevalence for this age group. Sensitivity analyses show that the cost per case detected and successfully treated decreases as the prevalence of STIs increases among those seeking ED care. In our analysis, the ICER for targeted screening would decrease to $421 at a prevalence of 13.6%. While almost all of the pediatric EDs in our 6-hospital study see patients up to 21 y of age, prevalence may be lower in EDs that see patients only up to the age of 18 y, as the highest prevalence subgroup of adolescents is between the ages of 20 and 24 y. It is possible that EDs with lower limits on age or in other geographical regions may have a lower prevalence. Thus, decisions about optimal screening strategies could be nuanced to account for prevalence at individual centers. However, the prevalence at a particular center would have to be less than 0.05% before targeted screening would cost more than $50,000 per case detected and treated.
The proportion of patients interested in having STI testing performed in the universally offered screening strategy has a significant impact on its cost-effectiveness compared with targeted screening. In settings where adolescents visiting the ED agree to STI testing at probabilities greater than 58%, universally offered screening becomes more effective than targeted screening and may be a cost-effective alternative depending upon society’s WTP for accurate identification and treatment of STIs in this population. In addition, the effectiveness of usual care is highly dependent upon clinicians ordering urine testing, particularly among patients with symptoms suggestive of STIs. Using data from our own multisite study, only 24% of clinicians ordered such testing for patients with symptoms suggestive of an STI. If the probability of ordering urine testing in the usual care strategy exceeds 42%, usual care becomes more effective than targeted screening but more expensive. The larger this number, the less effective are any screening strategies, as greater proportions of possible cases are detected outside the screening programs. Depending upon society’s WTP for detection and treatment of STIs in this population, usual care might be a cost-effective strategy.
In a probabilistic sensitivity analysis, universally offered screening was a cost-effective alternative if the WTP threshold was less than $450 per case detected and successfully treated. Since there are no clearly defined WTP thresholds for our utility metric of cost per case identified and successfully treated, we performed a secondary analysis in which we used QALYs lost due to long-term complications of untreated chlamydia and/or gonorrhea instead of the effectiveness metric of cases identified and successfully treated. In this analysis, targeted screening was highly cost-effective, at $23,320 per QALY compared with universally offered screening.
We also performed subgroup analyses for cohorts consisting of only females or of only males. Targeted screening remained a cost-effective strategy for both cohorts when using cases detected and successfully treated as an outcome metric. Results were more nuanced when using QALYs as the outcome metric of effectiveness. In these analyses, targeted screening was highly cost-effective compared with universally offered screening for AYA females. However, neither targeted screening nor universally offered screening were cost-effective for AYA males. This is likely due to the smaller burden of untreated CT/GC on males compared with females. Females may suffer numerous impactful long-term sequalae including chronic pelvic pain, tubal infertility, and ectopic pregnancies, while the major longer-term sequela in men is epididymitis. It is important to note that these analyses did not account for the public health burden of asymptomatic, untreated CT/GC and the potential for inadvertent spread of STIs.
The multicenter trial upon which we have modeled our analysis differs from other published cost-effectiveness analyses in several ways. Our study examines screening of both female and male adolescents. Thus, our analysis differs from others that have generally focused on young women.28,29 Some analyses have focused on only the diagnosis and treatment of GC alone, 28 while our study is focused on both CT and GC. Finally, other studies have examined screening in settings with higher described STI prevalence, such as US jails and family planning clinics.29,30
We performed a prior cost-effectiveness analysis using literature-based estimates for base-case parameter values and for the test characteristics of an STI risk prediction algorithm as we awaited the completion of our own clinical trial. 31 In this analysis, both targeted screening and universally offered screening compared with usual care appeared to be cost-effective strategies. Based on data from the completed clinical trial in our 6-site PECARN study, targeted screening performed better and was more cost-effective than in our previous analysis using literature-based estimates. An important limitation and issue complicating the implementation of the screening strategies was the occurrence of the COVID-19 pandemic, which led to staff shortages and, consequently, greatly affected our nursing buy-in and participation. 32 This affected the number of patients who either received or completed the computerized sexual health survey. As a result, the analysis we present uses a “per protocol” subset of patients who were offered and completed the computerized risk assessment. Thus, this analysis provides the cost-effectiveness of targeted and universally offered screening assuming implementation of the computerized sexual health survey was complete. Thus, multicenter studies assessing this real-world intervention with improved rates of uptake are needed to verify whether targeted screening will remain a cost-effective strategy when a larger proportion of patients participate in screening. That being said, in a piecewise linear regression controlling for site as a fixed effect and temporal trends, population-level STI detection rates were higher per 1,000 patient visits during the targeted (adjusted effect 2.59 [95% confidence interval {CI} 2.46, 2.73]) and universally offered (adjusted effect: 1.81 [95% CI 1.67, 1.94]) screening strategies compared with usual care. Similar results were seen in a per protocol analysis. Population-level STI detection rates were higher per 1,000 patient visits in the targeted (adjusted effect 22.11 [95% CI 21.38, 22.84]) and universally offered (adjusted effect: 12.78 [12.04, 13.52]) screening strategies compared with usual care. 23
Additional limitations of our analysis include the lack of a societal perspective and the absence of subgroup analyses by race, ethnicity, rurality, or other demographic factors. Unfortunately, we did not have data from the companion clinical trial documenting the amount of time spent in the ED for each of the 3 screening strategies. However, one might expect that the universally offered screening strategy would take more time in aggregate than the other 2 strategies given the need to discuss screening with all patients rather than the select subgroup identified in targeted screening. Thus, we would anticipate that including additional costs due to time lost in the ED would only strengthen our conclusions by making targeted screening less costly and even more cost-effective compared with universally offered screening. Finally, we included only demographic factors for which we had detailed probabilities and outcomes data in the companion clinical trial. This means we were only able to incorporate sex as a demographic variable in our decision model.
In conclusion, our analysis indicates that targeted screening compared with universally offered screening is a highly cost-effective strategy for detecting and treating STIs in adolescents seeking ED care. However, these conclusions are more tentative when considering the differential effect of untreated CT/GC on quality of life for subgroups consisting of only females or only males. We can still strongly recommend targeted screening as highly cost-effective in terms of both cases detected and successfully treated as well as quality of life for female patients. In subgroup cohorts of only male patients, from the perspective of impact on quality of life, usual care may be the preferred strategy.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683261460886 – Supplemental material for Targeted versus Universally Offered Screening in Pediatric Emergency Departments: Cost-Effectiveness
Supplemental material, sj-docx-1-mpp-10.1177_23814683261460886 for Targeted versus Universally Offered Screening in Pediatric Emergency Departments: Cost-Effectiveness by Mark H. Eckman, Monika K. Goyal, T. Charles Casper, Chella Palmer and Jennifer L. Reed in MDM Policy & Practice
Supplemental Material
sj-docx-2-mpp-10.1177_23814683261460886 – Supplemental material for Targeted versus Universally Offered Screening in Pediatric Emergency Departments: Cost-Effectiveness
Supplemental material, sj-docx-2-mpp-10.1177_23814683261460886 for Targeted versus Universally Offered Screening in Pediatric Emergency Departments: Cost-Effectiveness by Mark H. Eckman, Monika K. Goyal, T. Charles Casper, Chella Palmer and Jennifer L. Reed in MDM Policy & Practice
Footnotes
Acknowledgements
The funder (NICHD) had no role in the design and conduct of this study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Ethical Considerations
This study was approved by the University of Utah’s Institutional Review Board using a single IRB mechanism for reliance across all participating sites (IRB # 00111821).
Consent to Participate
A waiver of written informed consent was provided given that this study was an implementation trial of comparing the implementation of different STI screening strategies into the routine clinical ED workflow.
Author Contributions
Conception and design: MHE, JR, TCC, CP, MKG; analysis and interpretation of the data: MHE, JR, TCC, CP, MKG; drafting of the article: MHE, JR, TCC, CP, MKG; critical revision of the article for important intellectual content: MHE, JR, TCC, CP, MKG; final approval of the article: MHE, JR, TCC, CP, MKG; statistical expertise: MHE, TCC, CP.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by grant R01HD094213 (Goyal/Reed). PECARN is supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS), in the Maternal and Child Health Bureau (MCHB), under the Emergency Medical Services for Children (EMSC) program through the following cooperative agreements: EMSC Data Center (EDC)–University of Utah (UJ5MC30824), GLACiER-Nationwide Children's Hospital (U03MC28844), HOMERUN–Cincinnati Children'’ Hospital Medical Center (U03MC22684), PEMNEWS–Columbia University Medical Center (U03MC00007), PRIME–University of California at Davis Medical Center (U03MC00001), CHaMP node–State University of New York at Buffalo (U03MC33154), STELAR–Seattle Children's Hospital (U03MC33156), and SPARC node–Hasbro Children’s Hospital (U03MC33155). This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US government.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Eckman, Reed, Casper, and Goyal and Ms Palmer have received grant funding from NIH/NICHD R01HD094213 (principal investigators: MKG and JR).
Access to Data and Data Analysis
TCC and CP had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Originality of Content
All information and materials in the article are original.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.