
Abstract
Purpose
While traditional medical education emphasizes real patient interactions, practical and ethical constraints require alternatives, such as simulated patients (SPs) or virtual patients (VPs) in virtual reality. This study investigates medical students’ experiential perceptions across different simulation formats within the same undergraduate medical curriculum, using a newly developed modality-spanning questionnaire.
Methods
A prospective cross-sectional study was conducted with 486 medical students across four curricular courses with differing educational content and objectives (two SP-based and two VP-based courses). A study-specific questionnaire applicable across both simulation formats captured “experience of presence” (‘embodiment’, ‘involvement’, ‘coherence’) and “experience of learning” (‘experience of competence’, ‘tension’, ‘acquisition of skills’, ‘enthusiasm’). Exploratory and confirmatory factor analyses were used to examine internal structure and psychometric properties of the questionnaire.
Results
Analyses indicated a stable internal structure with good sampling adequacy (Cronbach’s α = 0.82 for “experience of presence” and α = 0.66 for “experience of learning”). While overall perceived learning did not differ between simulation formats, format-specific experiential profiles emerged. SPs were rated higher for “experience of presence”, particularly regarding ‘involvement’ (M = 4.05 vs. 2.62), whereas VPs scored higher for ‘coherence’ (M = 4.50 vs. 3.98). Within learning-related dimensions, SPs were associated with greater ‘tension’ (M = 3.57 vs. 2.71) and ‘acquisition of skills’ (M = 4.66 vs. 4.24), while VPs elicited higher levels of ‘enthusiasm’ (M = 4.57 vs. 4.03; all p < 0.001).
Conclusion
This study provides insights into how medical students experience presence and learning across different simulation formats within an authentic curricular setting. While SPs appear to foster emotional engagement and perceived skill acquisition, VPs may particularly support spatial orientation and motivational aspects. Applying a single questionnaire across content-diverse courses and modalities may support educators in strategically aligning simulation formats with specific educational objectives and guiding the targeted development of curricula.
Keywords
1. Introduction
Simulation provides a safe and controlled alternative when practical or ethical constraints make interactions with real patients challenging. 1 When thoughtfully designed and aligned with educational goals, simulations help prepare students for the complexities of medical practice, enhance their confidence, and refine their skills. 2 A key challenge in clinical training is balancing hands-on experience with patient safety and ethical considerations. Simulation offers a structured, error-tolerant environment in which students can develop clinical skills without compromising patient well-being. Medical education simulations use selected scenarios, specific equipment, simulated patients (SPs), or virtual patients (VPs) to replicate real-life clinical settings. Both formats require significant investments: SP simulations demand personnel and logistic coordination, while virtual reality (VR) simulations require technological infrastructure and setup as well as development time.
SPs are trained actors who realistically portray specific symptoms or health conditions. 3 This enables students to take a history and perform physical examinations in a controlled setting, often conducted on-site in dedicated learning spaces. The approach helps learners to develop their communication and interpersonal skills, 4 while receiving structured feedback on their clinical and professional performance. 5 However, their implementation can be logistically demanding, particularly with large student cohorts. VPs, also resource-intensive, albeit in a different way given the often substantial programming costs for development, involve computer-based scenarios designed to mimic individuals with a medical condition. 6 Head-mounted displays immerse the students in a VR environment, with VPs programmed to respond to the students’ actions, providing feedback and enabling students to practice decision-making. 7 VR environments can often be accessed flexibly, facilitating self-paced learning. 8 Despite these advantages, technological limitations, such as the reduction in face-to-face communication and VR side effects, may reduce their effectiveness. 9
Regardless whether utilizing SPs or VPs, the goal remains to engage students deeply in the learning activity. In this context, the terms presence and immersion are frequently used. 10 Presence refers to a psychological state in which users feel situated in the simulated/virtual environment. 11 Immersion, primarily used as a technical term in VR research, describes the experience of being completely absorbed in a medium. 12 It also refers to the technological features of a system, such as sensory fidelity and interactivity, which enhance the feeling of being present. 13 However, this study did not evaluate these technological aspects of immersion, focusing on subjective student experiences across different simulation formats instead. Thus, presence is used to denote the subjective experience of students during the simulation. 14
Importantly, learning in simulation-based medical education is shaped not only by cognitive processes but also by learners’ emotional and motivational states.15-17 Building on these observations, learning experiences can be described along dimensions such as perceived competence, skill development, as well as emotional and motivational involvement. In contrast to presence, which reflects learners’ subjective sense of being situated and involved within the simulated environment, the experience of learning refers to learners’ perceptions of competence development, challenge, and motivational engagement during the learning process. In simulated learning environments, these experiential aspects may influence both how learners perceive training activities and how they engage with them.18-21 Although conceptually distinct, experiences of presence and learning are closely interrelated and may jointly shape the perceived effectiveness of simulation-based training. 22 Thus, an approach that explicitly considers cognitive, emotional and motivational aspects may not only offer a more comprehensive understanding of students’ perception but also contribute to enhancing the educational effectiveness of simulation formats. In particular, self-report instruments are well suited to capturing experiential dimensions such as presence, emotional involvement, and motivation that are not directly accessible through objective performance measures. When rigorously developed and psychometrically examined, they provide valuable insights into learners’ subjective experiences across simulation formats. 23
Previous research on simulated and virtual patient–based formats demonstrates considerable heterogeneity in study designs and outcome measures. Many studies compare VPs with traditional instructional approaches rather than directly contrasting different simulation modalities with one another. 24 As a result, there is limited evidence on how students perceive and engage with different simulation formats, and no clear consensus exists regarding differences in experiences of presence or learning processes across formats. 25 This underscores the need for systematic and comparable measurement approaches to capturing learners’ perceptions in simulation-based training. To address this, well-designed self-report questionnaires represent a practical and feasible means to assess learners’ perceptions across different simulation formats. At the same time, research conducted under authentic curricular conditions may provide important insights into how such experiences manifest in real-world educational practice, capturing the contextual and situated nature of learning processes. 26 However, this comes with the inherent challenge that simulation modality and instructional content are often intertwined and comparisons between simulation formats should be interpreted as exploratory. The present study is thus best understood as a proof-of-concept for a modality-spanning instrument designed to capture these experiential dimensions across diverse simulation-based learning contexts.
Against this background, the present study had the following aims: (1) To design a context-specific questionnaire assessing students’ “experience of presence” and “experience of learning” across different simulation formats; (2) To explore how students’ experiences of presence and learning manifest across various simulated and virtual patient–based formats, including an examination of their underlying factor structure; and (3) to identify specific strengths and weaknesses in each format and to discuss implications for the targeted use and further development of simulation formats in medical education.
2. Methods and Materials
2.1. Ethics and Data Protection
The local institutional review board concluded that the study did not qualify as biomedical or epidemiological research (Ethics ID 20210824 01). Students received full information on the study and their participation was voluntary. Data were collected anonymously using the EvaSys® platform (Lüneburg, Germany), with informed consent from all participating medical students. Neither participation (including lack thereof), nor the responses to the questionnaires had any consequence on the academic progress of students. Data were processed and stored in accordance with current data protection laws.
2.2. Study Design, Simulation Training, and Participants
The prospective cross-sectional study was conducted over two semesters (winter 2021/2022 and summer 2022) at a medical school in Germany offering a standard six-year undergraduate curriculum. All eligible students enrolled in four clinical courses were invited to participate in an online survey evaluating their simulation-based training experiences. Accordingly, sample size was determined by curricular cohort sizes and subsequently evaluated for adequacy in factor analyses. No additional exclusion criteria were applied, except for the VR-based emergency training course, for which only students who actively participated in the simulation scenarios were included in the analysis. Supplement 1 provides an overview of the simulation courses, learning objectives, and student activities.
This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies. 27
2.2.1. Course 1: History Taking With SPs Using Physical Simulation
Fifth-semester students (third year) attended the “basic practical and communication skills in surgery and medicine' course, comprising six two-hour sessions. This study analyzed data from the history-taking sessions with SPs, during which each student practiced for 10 minutes and received 20 minutes of feedback. Data from both semesters were included.
2.2.2. Course 2: Breaking Bad News With SPs in a Physical Simulation, Delivered Remotely via Videoconference
Seventh-semester students (fourth year) attended the “interdisciplinary oncology' module, which included lectures, seminars, and a communication course. They conducted telemedicine-style follow-ups with SPs to practice delivering bad news using a six-step model. Each student had a ten-minute interaction followed by 20 minutes of feedback. Sessions were held online via Zoom (Zoom Video Communications, San Jose, California, USA) in winter 2021/2022 and in person at the Teaching Clinic in summer 2022.
2.2.3. Course 3: Management of Emergency Cases Using VR Simulations With VPs
Tenth-semester students (fifth year) participated in fully immersive VR-based emergency training as part of their clinical rotations in internal medicine. During the two weeks, they attend four mandatory sessions, including one course using STEP-VR (Version 0.11 beta), an established VR system at our medical school. 28 Student assistants conducted 120-minute small-group sessions (eight to ten students). This was followed by a 60-minute debrief with a consultant of internal medicine. 28 Owing to time constraints, only three to four students per group actively participated in managing, diagnosing, and treating a critically ill patient presented through a VP scenario. Only these active participants were included in the study. VR sessions were held in person in the Teaching Clinic during both semesters of the study.
2.2.4. Course 4: Management of an Oncology Case Using VR Simulations With VPs
Sixth-semester students (third year) attended this module as a part of “internal medicine”, which included case-based lectures and bedside teaching. An additional fully immersive VR course on pancreatic cancer featured 40 minutes of individual sessions, during which students interacted with a VP, reviewing the medical history, diagnosis, and treatment. 29 This VR system was also already established at the medical school. Sessions took place in the Teaching Clinic in winter 2021/2022 only.
2.3. Development of the Questionnaire and Data Collection
The questionnaire was designed to measure students’ experiences of presence and learning across different simulation formats, ensuring its applicability in diverse instructional settings. It was tested in four courses (history taking, breaking bad news, emergency management, and oncology case management) to evaluate its robustness across various teaching environments. All variables captured students’ self-reported experiences and perceptions rather than objective learning outcomes. Throughout this manuscript, “experience of learning” refers to students’ perceived learning-related experiences rather than objective learning outcomes.
Items were adapted from established questionnaires including the Measurement, Effects, Conditions – Spatial Presence Questionnaire (MEC-SPQ) 30 and the Igroup Presence Questionnaire (IPQ), 31 supplemented with new items to capture presence and immersion in medical education. These new items were created based on expert consensus among medical educators and clinical instructors. The first section included 16 items: nine adapted from the MEC-SPQ, 30 six from the IPQ, 31 and one from the Flow Short Scale, 32 covering different aspects such as attention allocation, spatial awareness, and suspension of disbelief. The second section contained 17 items: three from the MEC-SPQ, 30 two from the Perceived Stress Questionnaire (PSQ), 33 three from the Intrinsic Motivation Inventory (IMI), 34 two from a questionnaire on interactive learning environments, 35 one from the Perceived Stress Scale (PSS-10), 36 and six newly developed items. This section assessed content, learning challenges, perceived competence, and motivation. All items utilized a five-point Likert scale (1 = “strongly disagree” to 5 = “strongly agree”, with an option to abstain.
After each course, students completed an online survey via the platform EvaSys (Lüneburg, Germany). They provided demographic information (age, gender), prior work experience in the medical field, and familiarity with gaming (asked during evaluation of the courses with VPs). Session dates and case details were recorded to identify and account for any anomalies. 37
The primary outcomes of the study were students’ self-reported experiences of presence and learning. The primary independent variable was simulation format (simulated patients vs. virtual patients).
2.4. Statistical Analysis
Survey data were exported and screened in Microsoft Excel 2021 (Microsoft Corporation, Redmond, WA, USA). Statistical analyses were conducted using IBM SPSS Statistics 28.0 (IBM Corp., Armonk, NY, USA) and R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) with RStudio version 2022.07.2 (Posit Software, Boston, MA, USA). Missing values were treated as absent without imputation. Descriptive statistics included mean (M) and standard deviation (SD). Group differences were assessed using the Welch-test and chi-square test, selected for their suitability to the data scale.
The psychometric properties of the questionnaire were evaluated. The minimum sample size for confirmatory factor analysis (CFA) typically ranges from 100 to 200 for simple models, but can be significantly higher for more complex models or those with weaker factor loadings.38,39 A maximum-likelihood exploratory factor analysis (EFA) was performed on the winter 2021/2022 dataset, while the summer 2022 dataset was used for CFA. 40 EFA criteria included a significant Bartlett’s test (p < 0.05), a Kaiser-Meyer-Olkin (KMO) coefficient > 0.50, factor loadings > 0.30 (without double loadings) and communalities (λ) > 0.40. The Kaiser-Guttman rule was applied, retaining factors with eigenvalues greater than 1. 41 Internal consistency was assessed using Cronbach’s alpha 42 with values ≥ 0.73 = high and ≥ 0.64 = adequate. 43 Factor correlations were analyzed with Pearson’s coefficient.
For “experience of presence”, missing values were excluded via listwise deletion to ensure complete datasets. In “experience of learning”, pairwise deletion was used to maximize the sample size. 44 CFA model fit was evaluated using a comparative fit index (CFI) > 0.95, root-mean-square error of approximation (RMSEA) < 0.06, and standardized root-mean-square residual (SRMR) < 0.08. 45
Known-groups validity was assessed to determine whether the questionnaire could differentiate between the two simulation formats. 46 Differences between SP and VP simulations were analyzed using the Welch-test, which is robust to violations of normality assumptions. 47 Owing to the large sample size, only highly significant results were considered (p < 0.001). 48
3. Results
3.1. Descriptive Statistics of Participants
Of 852 students enrolled in all four courses, 486 participated in this study. Of these, 317 participated in simulations with SPs and 169 in simulations with VPs. The overall sample was deemed representative of the student body at the medical school: the participants were 23.7 ± 3.5 years old and 67 % were female.
Participant Characteristics Stratified by Simulation Format
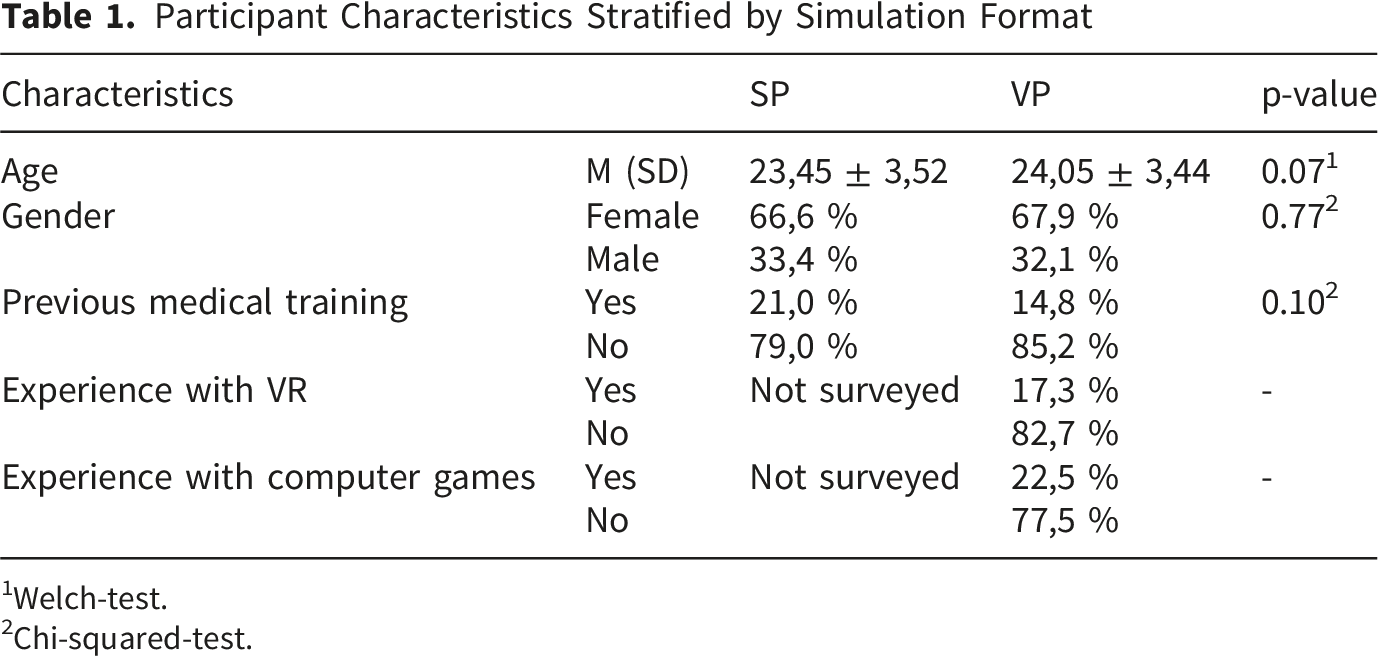
1Welch-test.
2Chi-squared-test.
3.2. Analysis of Questionnaire Items and Psychometric Evaluation
Table 1 outlines the final questionnaire items. Two constructs (denoted with “”) and their corresponding factors (denoted with ‘’) were identified. The construct “experience of presence”, with a Cronbach’s alpha of 0.82, comprised three factors: ‘embodiment’, which captures the participants’ feeling of being an active part of the simulation; ‘involvement’, reflecting the degree to which the simulation commands attention and creates a sense of realism and emotions; and ‘coherence’, determining the authenticity and consistency of the simulation setting. For the construct “experience of learning”, with a Cronbach’s alpha of 0.66, four factors were identified: ‘experience of competence’, detailing students’ self-assessment of their ability; ‘tension’, encompassing nervousness and challenges faced during the simulation; ‘acquisition of skills’, measuring perceived knowledge and skill enhancement; and ‘enthusiasm’, indicating the students’ motivation and engagement with the task. The internal consistencies of the two constructs were determined to be high and adequate, respectively.
Descriptive Results of the Refined Questionnaire Items Along With the Respective Constructs as Identified in the CFA, n = 486
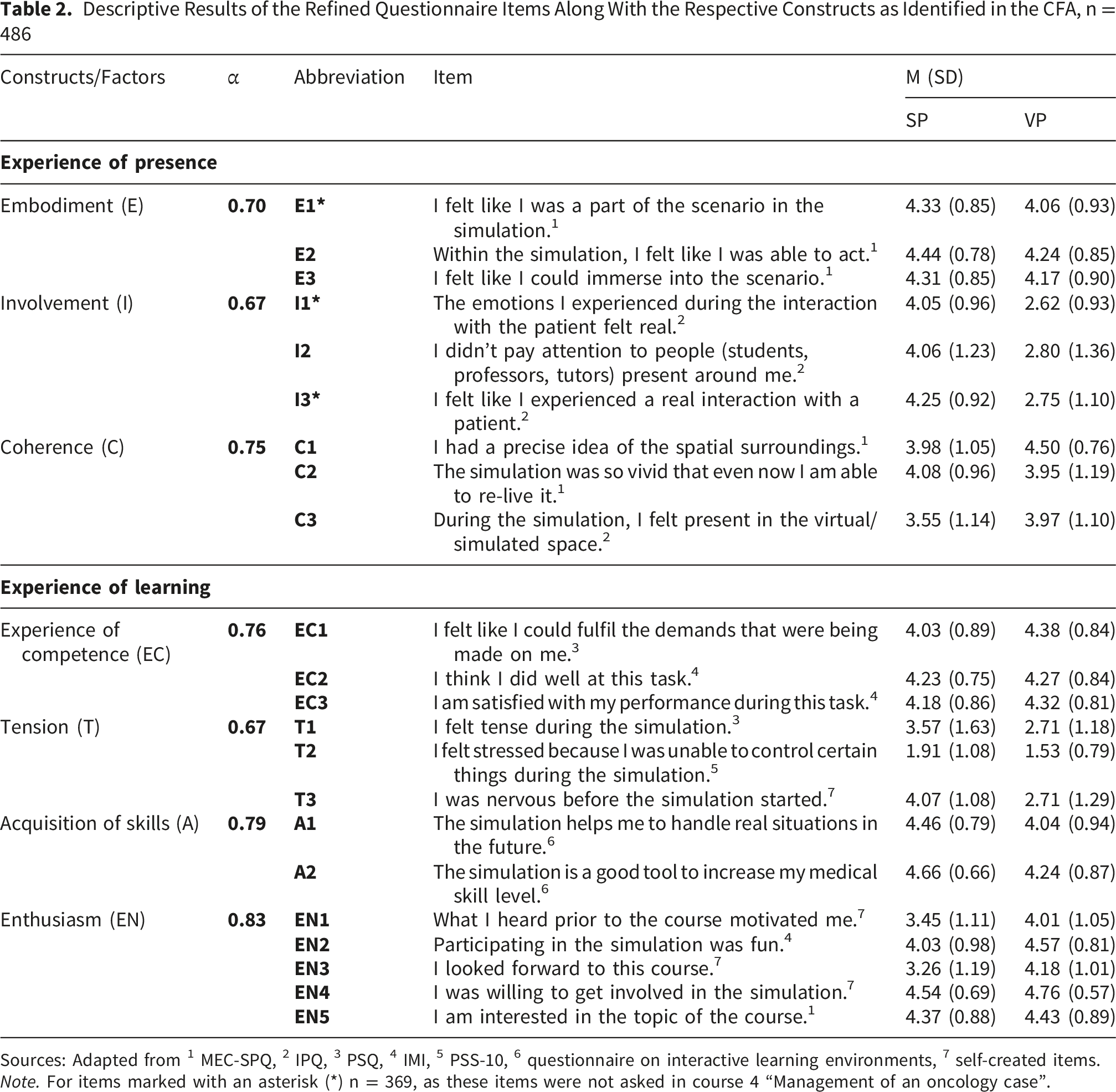
Sources: Adapted from 1 MEC-SPQ, 2 IPQ, 3 PSQ, 4 IMI, 5 PSS-10, 6 questionnaire on interactive learning environments, 7 self-created items.
Note. For items marked with an asterisk (*) n = 369, as these items were not asked in course 4 “Management of an oncology case”.
3.3. Format-Related Differences
Differences between simulation format scores were measured using the refined questionnaire (Figure 1). The comparisons revealed significant differences between SP and VP conditions, thereby supporting the instrument’s known-groups validity. Overall, SPs received significantly higher ratings for the construct of “experience of presence”, particularly due to their significantly higher scores in ‘involvement’. This may suggest a greater emotional and cognitive engagement. Conversely, VPs scored higher for ‘coherence’, indicating a greater perceived consistency and realism of the simulated environment. ‘Embodiment’ was rated comparably for both formats, suggesting that participants felt equally active and present in both simulation settings. Box-plot illustrations of the constructs “experience of presence” and “experience of learning” with their factors, with the significance of the differences indicated between the course formats using SPs and VPs. The box plot features a horizontal mean line within each box, with the box itself representing the interquartile range (IQR) of the middle 50% of scores, and whiskers extending to depict the overall data range up to 1.5 times the IQR. n. s. = not significant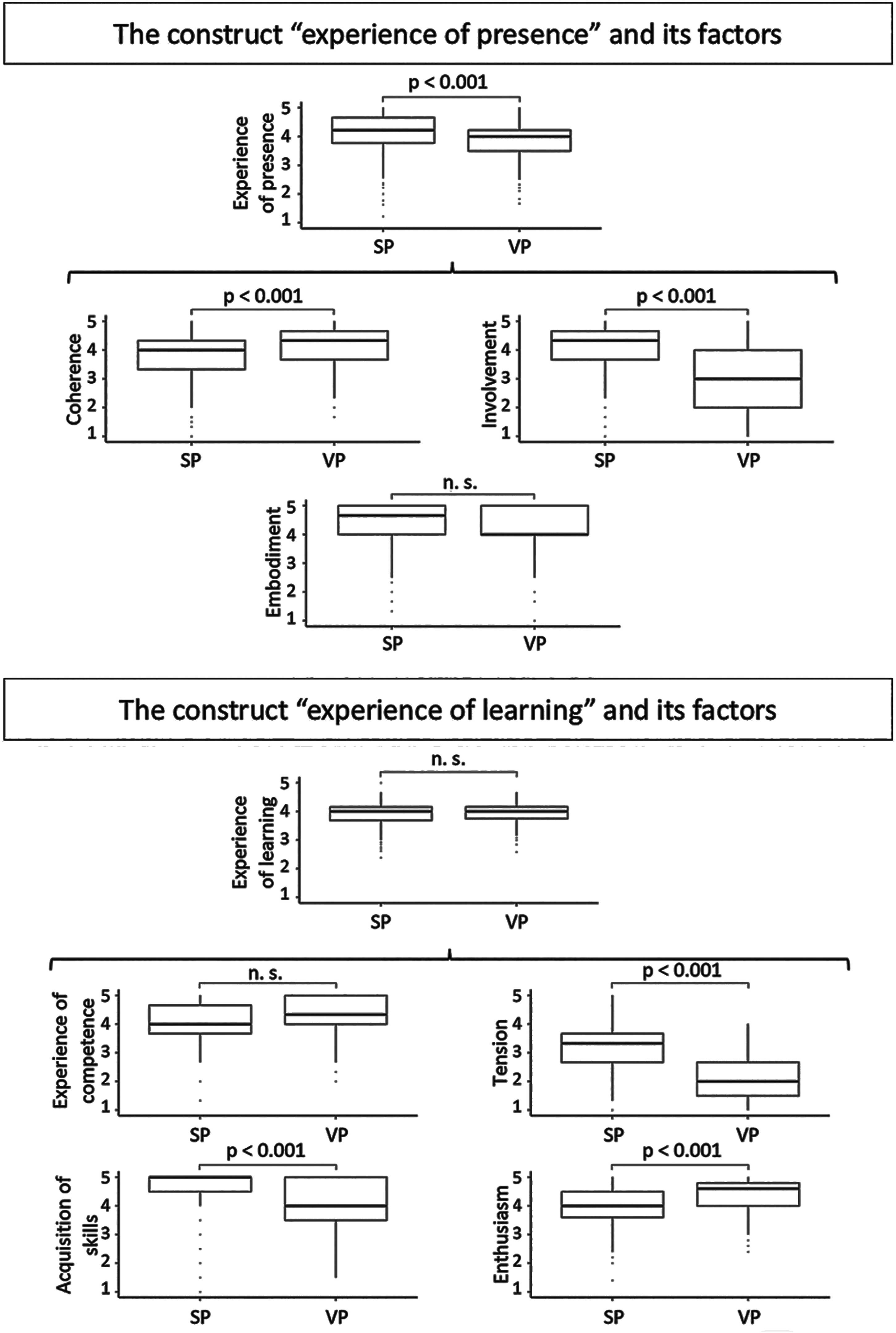
Taken together, the construct “experience of learning” was comparable across both simulation formats. However, when examining the individual factors, only the ‘experience of competence’ yielded similar ratings in both groups. SPs led to significantly higher levels of ‘tension’ and ‘acquisition of skills’, whereas VPs elicited significantly greater ‘enthusiasm’.
4. Discussion
Our cross-sectional study, conducted over two semesters and across four curricular courses, provides a broad perspective of simulation-based training within the degree course in medicine in Würzburg. The development of a new questionnaire was essential for capturing experiences of presence and learning across different simulation formats, as commonly used instruments are often modality-specific and thus limit meaningful comparison between physically and virtually mediated learning environments. 50 The new questionnaire focuses on shared experiential dimensions applicable to both SP and VP simulations. By adapting items from established instruments (e.g., IPQ, MEC-SPQ) to the clinical context and supplementing them with newly developed items, we provide initial evidence supporting the questionnaire’s reliability and internal validity. This was reflected by consistent factor structures and satisfactory psychometric properties demonstrated through exploratory and confirmatory factor analyses.
4.1. Evaluation of SPs
The SPs received higher ratings for the overall “experience of presence”, particularly in terms of ‘involvement’. This can be attributed to the minimal environmental setup, which resulted in greater emphasis on interaction with the SP. Emotional engagement is known to play a key role in shaping learning experiences by influencing attention, memory, and motivation. 51 Research on practicing physicians has revealed that positive emotions and involvement contribute to a more comprehensive diagnostic process, as well as quicker and more creative problem-solving. 52 Furthermore, simulation methods that evoke emotional and embodied experiences appear to influence the development of empathy positively. 53
We found that ‘tension’ levels were significantly higher in simulations using SPs. Previous work suggests that moderate levels of challenge and tension can enhance learner engagement and increase the perceived meaningfulness of training experiences, consistent with the Yerkes-Dodson law, which posits an optimal level of arousal for performance, 54 although the relationship between stress and learning outcomes remains complex and context-dependent. 55 While productive tension may stimulate effort and contribute to a sense of achievement, 56 negative emotions such as fear, boredom, or frustration can impair concentration and hinder learning both in face-to-face57,58 and virtual settings. 59 In our study, students reported moderate to high levels of excitement accompanied by minimal perceived loss of control in both simulation formats, suggesting that experienced tension largely remained within a manageable and potentially facilitative range.
Students rated the SPs higher in terms of ‘acquisition of skills’, indicating that they perceived this format as relevant for future professional practice and as a useful tool to develop required competencies, especially in communication and interpersonal skills. This aligns with research demonstrating that goal orientation enhances academic achievement by directing students’ energy and focus. 60 However, learners may not always accurately define their own learning objectives, which might influence their self-assessment of progress. 61
4.2. Evaluation of VPs
VPs scored higher on ‘coherence’ compared to SPs, likely due to the realistic representation of the environment afforded by VR-technology, which gave students the feeling of being on site. Studies highlight the potential of VR to improving students’ understanding of surgical procedures and anatomical structures, as well as in fostering spatial awareness. 62 Additionally, VR enables students to familiarize themselves with specific clinical environments, facilitating readiness for actual clinical scenarios and preparation for real-world placements. 63 In our study, this was exemplified by the STEP-VR system, which replicates key spatial and functional elements of the emergency department at the local university hospital to provide an immersive preparatory learning experience for students. Research comparing in-situ simulations (conducted in a real clinical setting) with off-site simulations (training rooms) demonstrated that in-situ training can facilitate superior organizational learning. 64 With particular regard to spatial orientation and environmental familiarity, VR may therefore represent a promising approach to approximating selected aspects of in-situ simulation, especially in contexts where on-site training is logistically constrained.
Another notable finding was the higher levels of ‘enthusiasm’ reported in VP simulations compared to SPs. This aligns with studies revealing that students using VR for subjects such as neuroanatomy reported greater motivation and enjoyment compared to traditional paper-based methods, although this did not necessarily translate into better learning outcomes. 65 However, motivation and enthusiasm-related factors do play a crucial role in performance. VR simulations can foster motivation and enthusiasm among students, contributing to greater engagement and potentially more effective learning processes. 66 Additionally, self-efficacy has been identified as an important predictor of performance. 67 Enthusiasm may not only enhance engagement but also strengthen self-efficacy, thereby promoting deeper involvement and sustained effort in the learning process. 68
Despite such immersive potential, VR appears less effective at fostering ‘involvement’ and realistic patient interactions, raising the question of how much empathy VR (as an environment) can truly elicit in simulations. Studies on this topic have yielded mixed results: while VR has been shown to enhance emotional empathy (automatic responses to others’ emotions), its effect on cognitive empathy (conscious understanding of another’s feelings) remains inconclusive. 69 Moreover, increasing immersion in VR does not necessarily lead to greater emotional engagement. 70 To enhance user ‘involvement’, further research is needed, particularly focusing on advancements in VR technology 71 such as speech interaction and authentic facial and gestural responses of VPs.
Our findings indicate that neither simulation format is inherently superior with respect to students’ reported experiences. Instead, each format offers distinct advantages that vary according to the learning context and educational goals. This underscores the importance of intentionally aligning simulation-based teaching methods with specific learning objectives. SPs may be particularly effective for training communication and interpersonal skills, especially in emotionally or relationally complex scenarios, while VPs can support structured clinical decision-making and spatial orientation within recognizable clinical environments. Future curriculum development could benefit from an integrative approach that strategically employs both SPs and VPs, leveraging their respective strengths to optimize learning outcomes.
4.3. Methodological Considerations
We conducted our study under authentic curriculum conditions, consistent with realistic evaluation principles. 72 Within this pragmatic design, the findings are best interpreted in light of the interplay between simulation modality and instructional content. Rather than artificially controlling variables or randomizing students, which would have compromised standardized teaching, we embedded our questionnaire into mandatory simulation-based training. Although each simulation format targeted distinct clinical objectives, our primary aim was to assess the tool’s applicability across multiple courses. By enrolling 486 of the 852 students from various semesters, we leveraged the natural diversity of medical education, thereby enhancing the ecological validity and practical relevance of our findings. However, as a drawback of this pragmatic approach, both simulation modality and instructional content varied simultaneously: SP-based scenarios focused more strongly on communication and empathy, whereas VP-based scenarios emphasized procedural and spatial aspects. This may explain why SPs were associated with higher emotional involvement, while VPs were associated with higher ratings of coherence and spatial realism. Prior research suggests that direct interpersonal interaction fosters affective engagement,73,74 whereas technology-mediated environments may preferentially support cognitive and procedural learning. 75 This overlap between modality and instructional content makes it difficult to attribute observed differences in learners’ experiences exclusively to the simulation format itself – reflecting a well-established trade-off in research design. 76 While controlled, explanatory studies aim to isolate causal effects under standardized conditions, pragmatic approaches prioritize ecological validity and the applicability of findings to real-world practice.76,77 Our study can be positioned towards the pragmatic end of this continuum, as it captures how simulation-based teaching is implemented within an existing curriculum. Accordingly, the findings should be interpreted with caution when drawing modality-specific conclusions.
Moreover, in line with contemporary instructional design models, the simulation formats were embedded at different stages of the curriculum to align with the underlying learning objective.64,78 Consequently, participants varied in their level of clinical experience, which may have influenced their perceptions: The VR-based emergency training took place in the fifth year, when students had already gained exposure to real clinical environments, potentially enabling a more differentiated evaluation of spatial realism and coherence. In contrast, SP-based communication courses were positioned before extensive patient contact, where emotionally salient interactions may be perceived as particularly novel and intense, contributing to higher involvement. Additionally, the uneven distribution of participants across courses may have introduced minor imbalances in exposure, although no systematic bias was evident in the descriptive analyses. Overall, these factors suggest that sample composition, learners’ developmental stage, and prior experience should be considered when interpreting the results.
4.4. Strengths and Limitations
Questionnaire-based studies often face limitations such as subjectivity, low response rates, and the potential for socially desirable answers. 79 In our study, voluntary participation may have introduced a potential self-selection bias, and differences in course content between SP and VP simulations could have influenced the results. Additionally, since participants were from a single institution, their perceptions of instructional topics and teaching staff may have thus been shaped by location-specific factors. Simulation-based training was integrated into the curriculum from the first year onwards, allowing for the progressive development of students’ skills. VR was introduced later in the clinical phase as an extension of prior simulation experiences. However, this study focused on students’ perceptions of the teaching method itself, rather than their discipline-specific expertise, which naturally evolves throughout their education.
EFA and CFA rely on specific assumptions regarding data distribution, which may not always align with real-world conditions. The interpretability of the results therefore depends on the quality and reliability of the underlying measurement instrument. To mitigate this, we included students from different semesters and curricular stages to ensure heterogeneous representation, and conducted a rigorous psychometric evaluation using exploratory and confirmatory approaches. Additional research is necessary to assess the questionnaire’s generalizability and applicability across different institutional contexts. In particular, incorporating objective learning measures (e.g. pre–posttest assessments) could enable direct comparisons of identical SP and VP simulation scenarios and strengthen the interpretation of the instrument’s explanatory value. Such approaches may help to examine the relationship between subjective experience and performance outcomes.
As discussed above, the pragmatic design limits the disentangling of modality and content-related effects and requires cautious interpretation of comparative findings. Future studies using more controlled designs and standardized scenarios across modalities would be needed to address this limitation more directly. At the same time, such approaches presuppose that comparable learning objectives, particularly communication-focused scenarios, can be implemented in VR-based environments, which remains challenging at the current stage of development.
Although this study did not aim to validate a measurement instrument formally, the exploratory data provide initial evidence supporting aspects of construct validity within established validity frameworks.23,80 Specifically, the consistency of item functioning and the stability of the factor structure contribute to internal structure evidence, while systematic associations observed across simulation formats may offer preliminary insights into generalization and construct interpretation.
In addition to didactic considerations, practical factors such as cost and scalability also influence implementation decisions. In our study, we did not directly compare the costs of SPs and VPs. However, we do acknowledge that cost considerations play a central role in implementation decisions and may influence scalability and sustainability. 81 Despite recent reductions in hardware costs, the acquisition of VR equipment and the development of VR scenarios continue to represent substantial financial investments for institutions, currently limiting broader scalability. Existing cost-effectiveness analyses in emergency medical training suggest that these initial expenses may be offset over time by the savings made not having to fund consumables and SP costs.82,83
5. Conclusion
This study introduces a modality-spanning questionnaire to assess medical students’ experiences of presence and learning in simulation-based training. As a proof-of-concept, the findings should be interpreted with appropriate caution. Our results suggest that SP and VP simulations offer complementary experiential strengths rather than one format being universally superior. SPs were associated with greater emotional involvement and perceived skill acquisition, whereas VPs were associated with higher ratings in coherence, enthusiasm, and structured clinical reasoning. These observed patterns should be interpreted in light of the pragmatic study design, precluding causal attribution to the simulation modality alone.
These results underscore the importance of aligning simulation formats with specific educational objectives. Applying a single questionnaire across multiple courses highlights the value of systematically capturing experiential dimensions that complement objective learning outcomes. An integrative curricular approach that strategically combines SP and VP simulations may therefore support both emotional engagement and spatially oriented learning experiences in medical training.
Supplemental Material
Supplemental Material - Students’ Experiences of Presence and Learning Across Simulated and Virtual Patient Formats: A Cross-Sectional Study
Supplemental Material for Students’ Experiences of Presence and Learning Across Simulated and Virtual Patient Formats: A Cross-Sectional Study by Hanna Brecheisen, Joy Backhaus, Nina L. Zerban, Tobias Mühling, Alexander Hann and Sarah König in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to all the students who participated in this study. Furthermore, we would like to thank Andrew Entwistle for his assistance with proofreading the manuscript.
Ethical Considerations
The local institutional review board (Ethikkommission der Universität Würzburg) reviewed the study and determined that it did not qualify as biomedical or epidemiological research (Ethics ID 20210824 01). All study procedures were conducted in accordance with relevant institutional guidelines and regulations. Data were collected anonymously, and all data handling complied with applicable data protection laws.
Consent to Participate
All participating medical students received comprehensive information about the study and provided written informed consent prior to participation. Participation was entirely voluntary, and neither participation nor non-participation, nor responses to study questionnaires, had any impact on students’ academic progress.
Consent for Publication
Not applicable, as no individual person’s data or personal details are included in this publication.
Author Contributions
Hanna Brecheisen and Sarah König were responsible for the development of the questionnaire, the conception and execution of the study, as well as drafting and revising the manuscript. Joy Backhaus was in charge of the statistical evaluation and played a key role in both drafting and revising the results. Nina Luisa Zerban, as coordinator of the SP program in Würzburg, assisted in evaluating these courses by administering the surveys. Tobias Mühling and Alexander Hann contributed to data collection and offered valuable feedback to the study design. All authors approved the submitted manuscript and agreed to be accountable for the research work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tobias Mühling was involved in the development of the STEP-VR emergency training software and has a familial relationship with the managing director of OrangeWhip Interactive, which later acquired the software. All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset utilized in this study is available from the corresponding author on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.