
Abstract
Background
This cross-sectional study examined whether anxiety and depression symptoms decrease as medical students progress through training (suggesting adjustment disorder) or persist (suggesting chronic conditions), while identifying associated risk factors, including student debt burden and treatment effectiveness.
Methods
We surveyed medical students (years 1-4) at VHS-ODU using a sociodemographic questionnaire and validated screening instruments (GAD-7 for anxiety and PHQ-9 for depression) via RedCap from September to November 2024.
Results
Among 126 students, Scores were higher in Years 2–3 than in Years 1 and 4, but differences by year were not significant (GAD-7 p=0.055; PHQ-9 p=0.352). Students with a prior mental-health diagnosis had higher symptoms (GAD-7 8.09 vs 4.31; PHQ-9 10.18 vs 4.72; p≤0.001). Among those with a prior diagnosis, scores did not differ by current treatment category (GAD-7, p = 0.900; PHQ-9, p = 0.263). Higher student-loan balances were associated with higher scores (descriptive only; group Ns were unavailable for testing).
Conclusion
Medical schools should prioritize proactive screening and timely access to care, bolster support during clinical training, and address financial stressors; longitudinal studies are needed to test whether such changes reduce symptom burden.
Introduction
Meta-analyses estimate depression prevalence among medical students at 27-28% globally, with anxiety affecting approximately 34%, rates 2-5 times higher than those of age-matched peers. 1 These patterns are consistent across geographic regions and persist despite increased awareness and institutional wellness initiatives.
The trajectory of symptoms across medical school years remains a topic of debate. If symptoms primarily reflect adjustment disorder — a time-limited response to stressors that resolves within 6 months — we expect improvement as students acclimate. However, persistence or worsening would suggest chronic conditions (major depression or generalized anxiety) requiring different interventions. 2
With MDD and GAD, there is often a long and consistent history of anxiety and depression symptoms. However, those with AD only experience their symptoms in times of stress or change, when they have difficulty coping with a specific, triggering life event, and these symptoms are usually resolved within months. We therefore surveyed medical students across all four years at VHS-ODU with three objectives: (1) test whether mental health symptoms decrease with progression through medical school (supporting adjustment disorder) or persist/increase (supporting chronic conditions), (2) assess whether students with pre-existing conditions receiving treatment show better outcomes than untreated peers, and (3) identify demographic and academic correlates of symptom severity, with financial burden emerging as a key finding rather than a planned objective.
Methods
Reporting Guidelines
This study follows the Equator guidelines and conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplementary File 1).
Study Design and Setting
This cross-sectional survey was conducted from September 1 to November 1, 2024, among medical students at Virginia Health Sciences (VHS) at Old Dominion University (ODU). The study was approved by the VHS Institutional Review Board Protocol (IRB #24-06-XX-0151).
Study Population
All medical students enrolled in the MD program at VHS-ODU were eligible (approximately 600 students across four years). The survey remained open throughout the 2-month study period. Of 600 eligible students, 126 responded to the survey (21% response rate).
Eligibility Criteria - Inclusion
Students actively enrolled in the VHS-ODU MD program during September-November 2024.
Exclusion
(1) Leave of absence, (2) studying abroad, (3) self-reported chronic disabling medical conditions. REDCap screening automatically excluded ineligible participants before survey access. Our exclusion of students with chronic medical conditions aimed to isolate stressors specific to medical training; however, it likely results in a meaningful underestimation of the overall mental health burden, as chronic physical illness is strongly associated with elevated anxiety and depression. 3 Students with chronic conditions represent a vulnerable subpopulation who may face compounded challenges while managing their health alongside rigorous training. This limits the generalizability of our findings to the full medical student population. Future research should specifically examine mental health in this understudied group.
Procedures
The Student Affairs Office distributed survey invitations via the institutional email system. After electronically informed consent, participants accessed the survey via REDCap, a secure web-based platform. Participation was voluntary and anonymous, and the survey took approximately 15-20 minutes.
Measures
The survey assessed: • Sociodemographic variables: age, gender, race/ethnicity, parental income, relationship status • Academic variables: year in school, employment status, clinical rotation stress, examination concerns (Step 1, Step 2, clinical exams) • Financial variables: student loan balance (categorized: none, <$100,000, $100,000–199,999, $200,000–299,999, ≥$300,000) • Mental health variables: prior diagnoses, current treatment status (none, medication, counseling, both), barriers to care • Outcome measures: GAD-7 for anxiety (0–21 scale, ≥10 indicates moderate-severe); PHQ-9 for depression (0–27 scale, ≥10 indicates moderate-severe)
The item assessing additional pressure during clinical rotations asked students whether they experienced increased stress specifically during their clinical training compared to pre-clinical years, with response options of Yes/No/No change. This allowed us to capture the qualitative shift in stressor types as students transition from the classroom to patient care settings.
The GAD-7 is a validated 7-item anxiety screening tool 4 with a specificity of 82%. 5 The PHQ-9 is a validated 9-item depression screening tool 6 with scores ranging from 0 to 27; a score of 10 or higher indicates moderate to severe depression (sensitivity, 89%; specificity, 88%). 6
Statistical Analysis
We calculated descriptive statistics for all variables. Continuous outcomes (GAD-7 and PHQ-9 scores) were compared across year groups using a one-way ANOVA with Tukey’s HSD for post hoc pairwise comparisons. Categorical variables were compared using chi-square tests or Fisher’s exact tests when expected cell counts were <5. Given the exploratory nature of this single-institution study, we report exact p-values without formal adjustment for multiple comparisons. Findings should be interpreted as hypothesis-generating rather than confirmatory. We calculated Cohen’s d effect sizes to quantify the magnitude of observed differences, as effect sizes provide meaningful information independent of the sample size and statistical significance. No prior sample size calculation was performed; we employed a census approach, inviting all 600 enrolled medical students to participate. Post-hoc power analysis using G*Power 3.1 indicated 80% power to detect large effect sizes (d>0.8) but only 50% power for medium effects (d=0.5), limiting our ability to detect small-to-moderate differences across subgroups. Analyses were performed using SPSS version 31.
Ethical Considerations
The study was approved by the IRB (protocol #24-06-XX-0151). Participation involved minimal risk. Data was collected anonymously via REDCap and will be retained in accordance with institutional policy for 7 years. Participants reporting suicidal ideation received automatic resources and crisis hotline information.
Results
Participant Characteristics by Academic Year
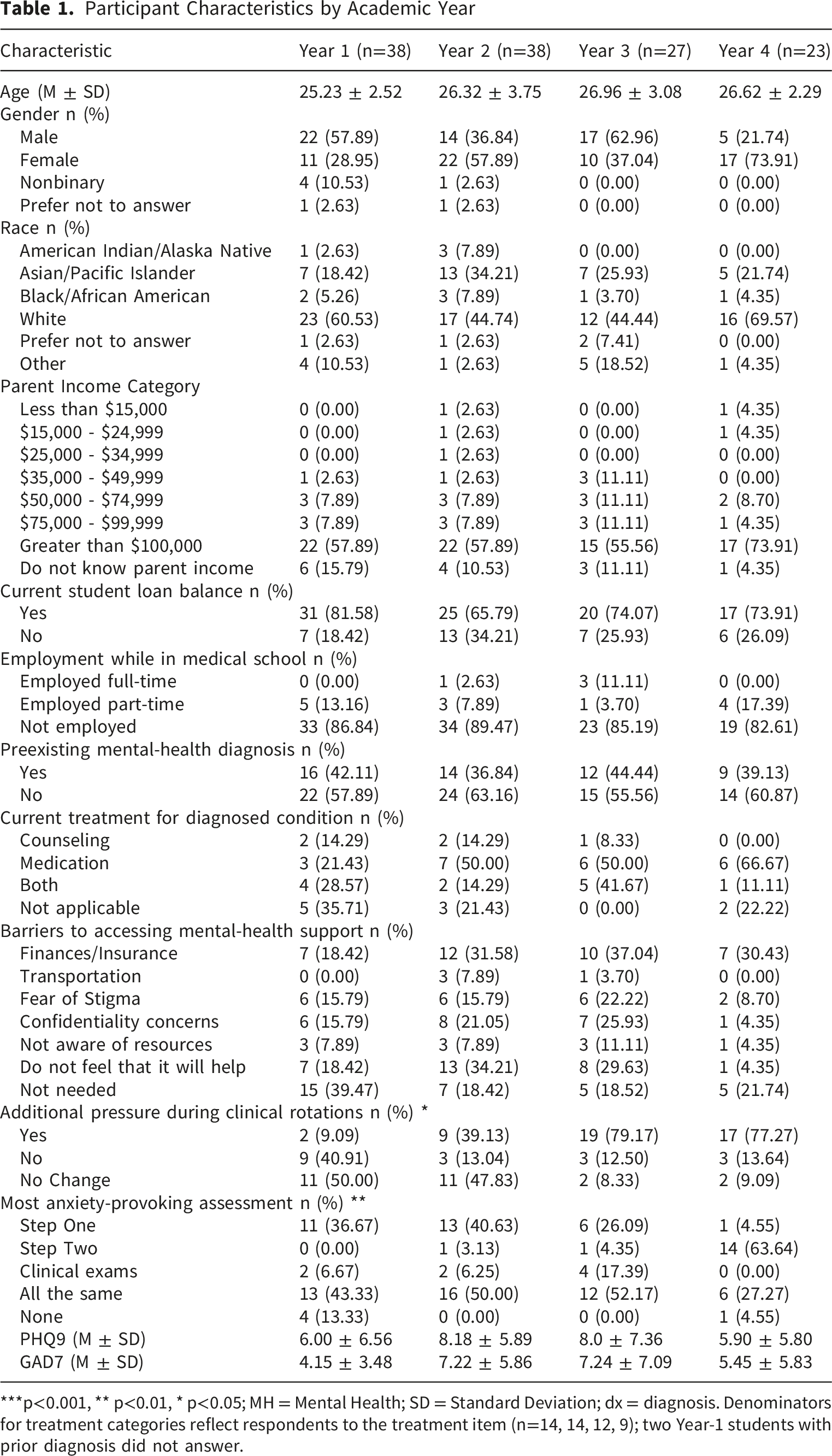
***p<0.001, ** p<0.01, * p<0.05; MH = Mental Health; SD = Standard Deviation; dx = diagnosis. Denominators for treatment categories reflect respondents to the treatment item (n=14, 14, 12, 9); two Year-1 students with prior diagnosis did not answer.
Symptom Scores Across Key Factors
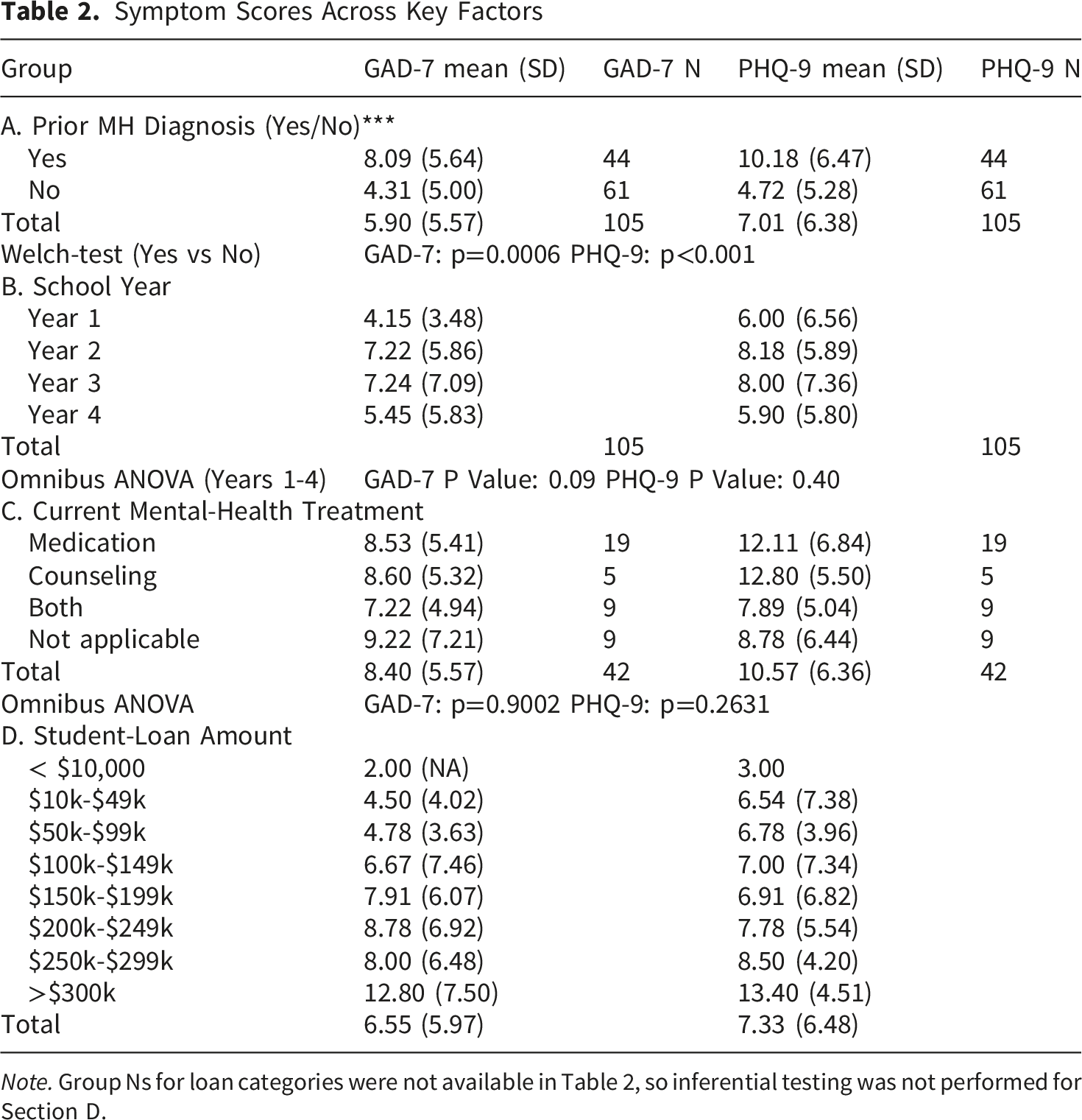
Note. Group Ns for loan categories were not available in Table 2, so inferential testing was not performed for Section D.
Mean PHQ-9 scores were 6.00 (Year-1), 8.18 (Year-2), 8.00 (Year-3), and 5.90 (Year-4). Mean GAD-7 scores were 4.15, 7.39, 7.22, and 5.45 across Years 1–4, respectively (Table 2; Figure 1A-B). The pattern suggests higher symptoms in Years 2–3 and lower symptoms in Years 1 and 4; however, omnibus tests were not statistically significant (GAD-7: F(3,101) = 2.61, p = 0.09; PHQ-9: F(3,101) = 1.10, p = 0.40) (Table 2; Figure 1). Symptom scores by year (A|B). (A) GAD-7 and (B) PHQ-9 means by Year 1–4 with 95% CIs. Sample sizes per year are shown in Table 2. Instruments: GAD-7 range 0–21; PHQ-9 range 0–27; higher scores indicate greater symptom burden. Omnibus ANOVA: GAD-7 F(3,122) = 2.61, p = 0.0546; PHQ-9 F(3,122) = 1.10, p = 0.352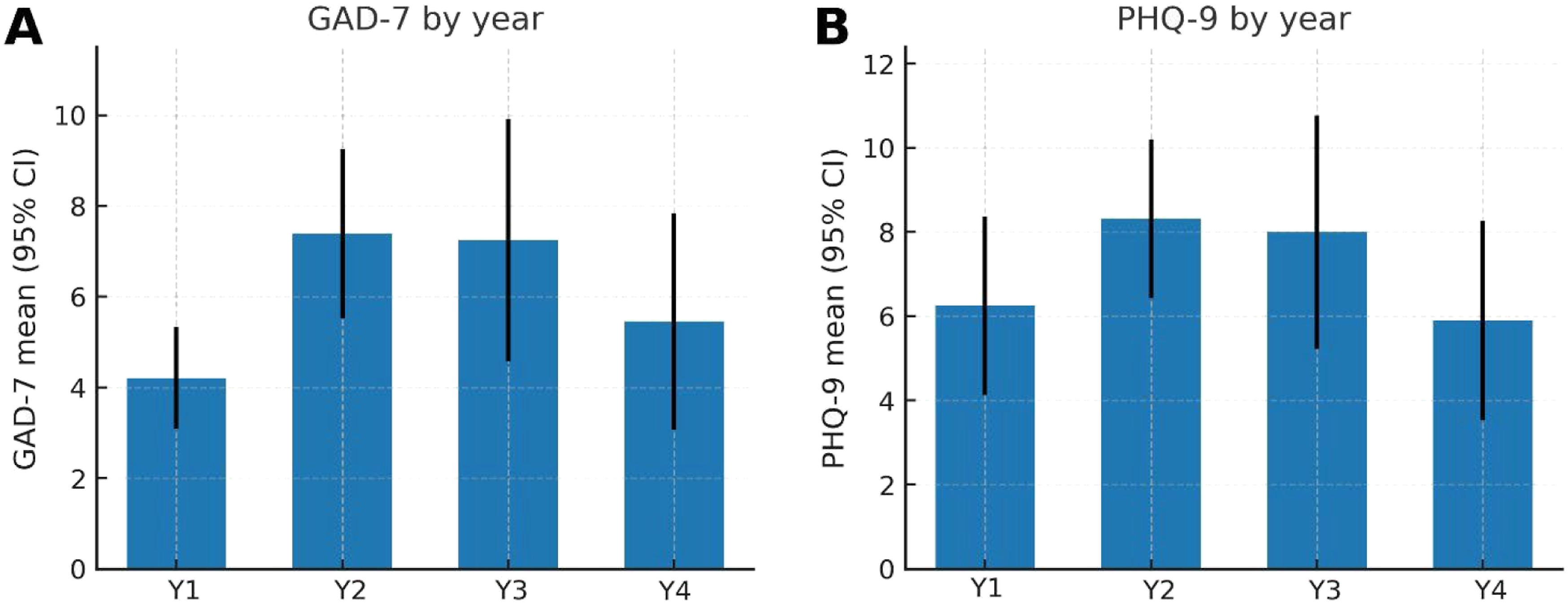
Students reporting a prior diagnosis had higher mean scores than those without a diagnosis: GAD-7, 8.09 vs. 4.31, and PHQ-9, 10.18 vs. 4.72 (Table 2; Figure 2A-B). Welch’s t-tests showed statistically significant differences for both scales (GAD-7: t(85.8) = 3.55, p=0.0006; PHQ-9: t(80.9) = 4.60, p<0.001) (Table 2). Within the subgroup with a prior diagnosis, mean scores were similar across self-reported treatment categories (medication-only, counseling-only, both, not applicable). GAD-7 means ranged from 7.22 to 9.22, and PHQ-9 means ranged from 7.89 to 12.80 (Table 2). Omnibus tests were not significant (GAD-7: F(3,38) = 0.19, p=0.9002; PHQ-9: F(3,38) = 1.38, p=0.2631) (Table 2). Symptom scores by prior mental health diagnosis (A|B). (A) GAD-7 and (B) PHQ-9 means with 95% CIs among students with vs without a prior diagnosis. Welch’s t-tests: GAD-7 t(85.8) = 3.55, p = 0.0006; PHQ-9 t(80.9) = 4.60, p < 0.001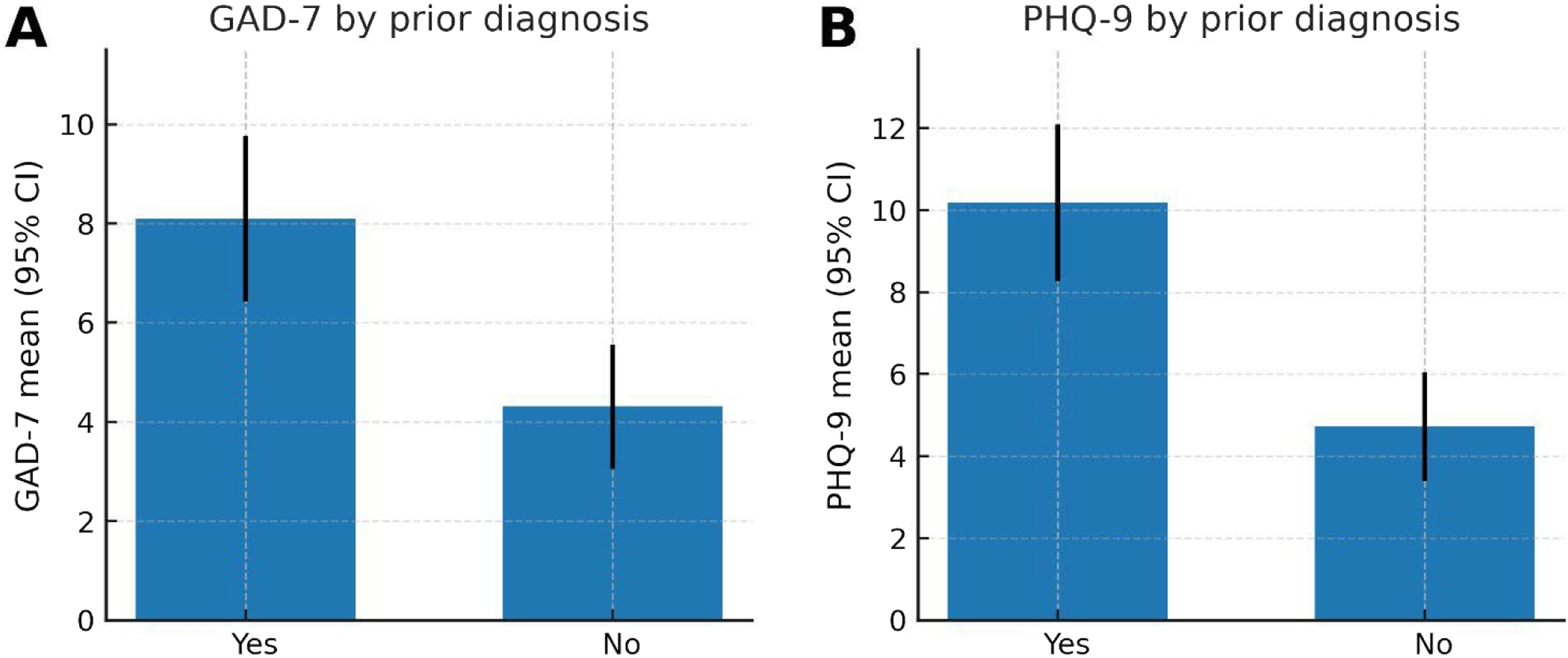
A higher current loan balance was associated with higher mean symptoms (Table 2; Figure 3A-B). PHQ-9 means rose from 3.00 (<$10k) to 13.40 (>$300k); GAD-7 means rose from 2.00 to 12.80 across these strata. Group Ns for loan categories were not available in Table 2, so inferential testing was not performed. Symptom scores by current student loan balance (A|B). (A) GAD-7 and (B) PHQ-9 means across self-reported loan strata. Error bars show SD because group counts are not available in Table 2; provide Ns to display 95% CIs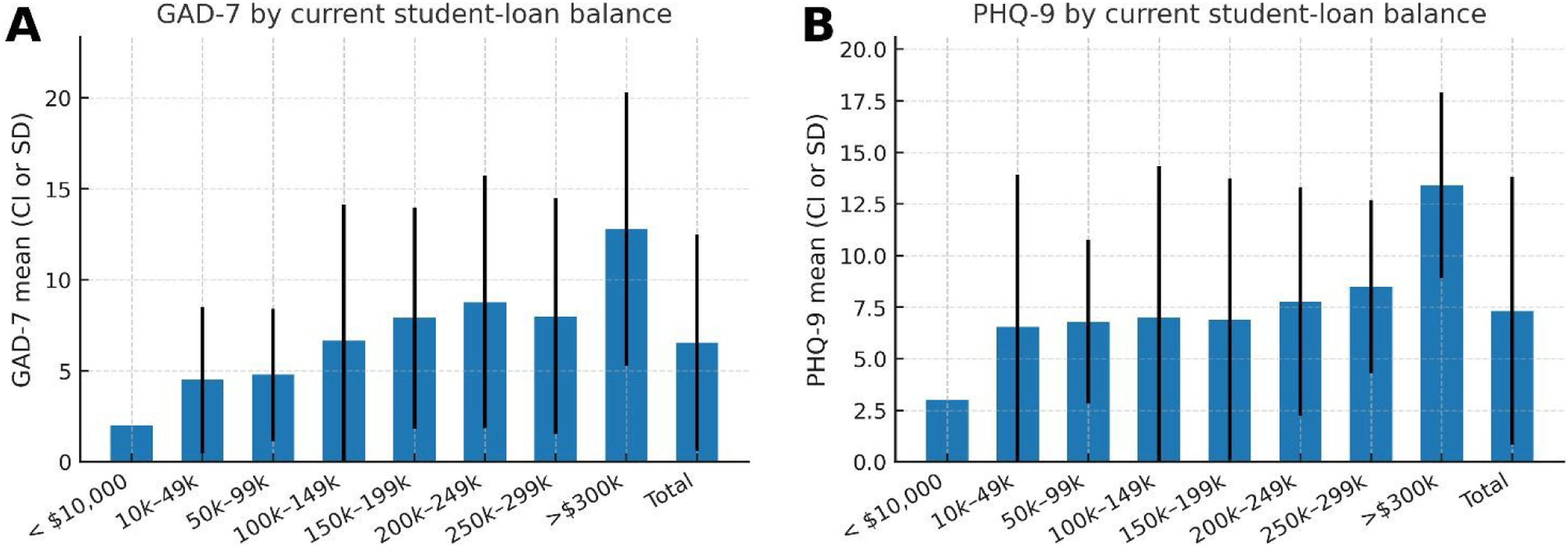
Perceived additional pressure during clinical rotations increased in the clinical years: 9.09% (Year-1), 39.13% (Year-2), 79.17% (Year-3), and 77.27% (Year-4) reported “Yes” (Table 1; Figure 4A). The most anxiety-provoking assessment shifted by year (Table 1; Figure 4B): Step 1 was most common in Year-1 (36.67%); All the same was most common in Year-2 (50.00%) and Year-3 (52.17%); and Step 2 dominated in Year-4 (63.64%). Clinical stressors by year (A|B). (A) Additional pressure during rotations (Yes/No/No change) by year and (B) most anxiety-provoking assessment by year. Values are percentages using year-specific denominators (Table 1). Presented descriptively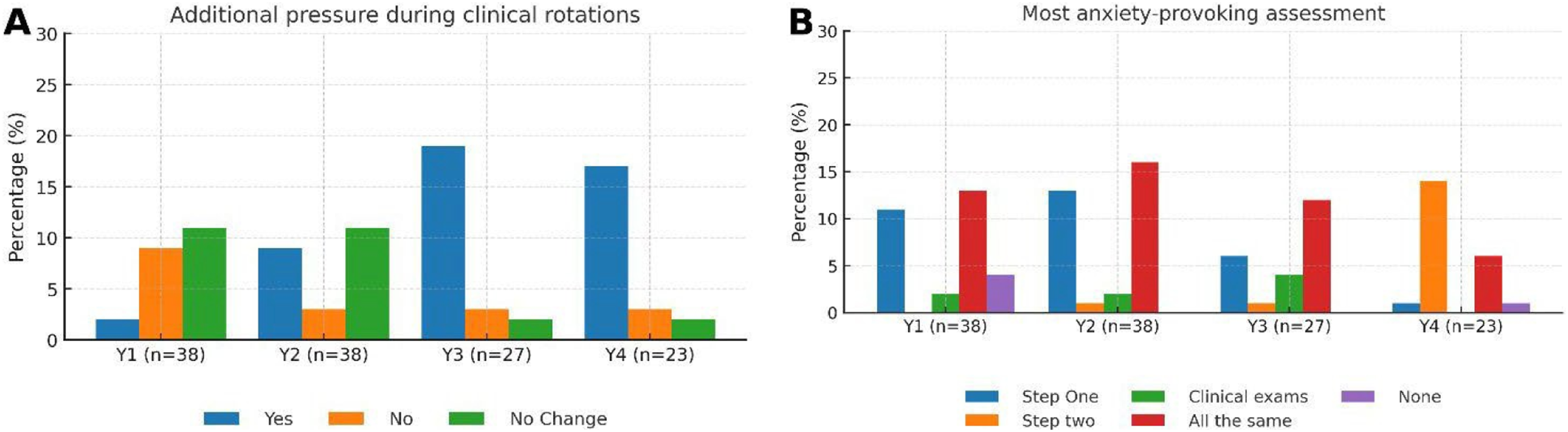
Discussion
Our cross-sectional analysis of mental health symptoms among medical students at VHS-ODU reveals patterns that warrant serious consideration from medical educators and administrators. The prevalence rates we documented, with 23.8% of students screening positive for moderate to severe depression and 18.3% for anxiety, aligns closely with the global estimates reported in a comprehensive systematic review. 1 That analysis of 43 countries found a 27% prevalence of depression and 11% prevalence of suicidal ideation among medical students. This consistency between our single institution findings and international data suggests that the challenges we observe reflect systemic issues within medical education rather than isolated institutional problems. A more recent meta-analysis by Quek et al 7 examining 69 studies with 40,348 medical students globally found an anxiety prevalence of 33.8% (95% CI: 29.2–38.7%), substantially higher than general population rates. The COVID-19 pandemic has further exacerbated these challenges, with Lin et al 8 reporting 45% anxiety prevalence among medical students during the pandemic period.
We initially hypothesized that mental health symptoms would decrease as students progressed through their training, consistent with an adjustment disorder pattern, where symptoms typically resolve within six months of stressor onset. 2 Our data did not support this hypothesis. Mean GAD-7 scores increased from 4.15 in the first year to 7.22 in the second year and 7.24 in the third years, though these differences did not reach statistical significance (p=0.09). PHQ-9 scores showed a similar pattern, rising from 6.00 in the first year to 8.18 in the second year. While our cross-sectional design and sample size limit definitive conclusions about trajectories, this pattern suggests that medical school presents successive waves of stressors rather than a single adaptable challenge. Longitudinal research supports this interpretation. Carrard et al 9 followed 1,595 students across a 6-year curriculum and found that emotional exhaustion peaks in year 2 and again in year 6, with different types of stressors affecting different training phases. Silva et al 10 identified three distinct trajectories in their longitudinal cohort: 68.5% never developed depression, 19.7% showed persistent depression, and 11.8% demonstrated recovery patterns.
The slight improvement observed in fourth-year students (GAD-7: 5.45, PHQ-9: 5.90) could reflect genuine adaptation, increased autonomy during sub-internships, or survivor bias among those who successfully navigated earlier challenges.
Students with pre-existing mental health diagnoses faced particularly severe challenges. These students reported significantly higher symptom burdens compared to those without prior diagnoses, with a mean GAD-7 scores of 8.09 versus 4.31 (p<0.001) and PHQ-9 scores of 10.18 versus 4.72 (p<0.001). Perhaps most concerning was our finding that the current treatment status was not associated with symptom levels. Among students with prior diagnoses, those receiving medication, counseling, both interventions, or no treatment reported similar symptom severities (GAD-7, p = 0.900; PHQ-9, p = 0.263). This suggests that standard mental health interventions, while potentially effective in other settings, may be insufficient to counteract the intense demands of medical training. Klein and McCarthy 11 found similar patterns in their narrative review, noting that mindfulness interventions failed to improve anxiety, depression, quality of life, or resiliency among medical students. MacLean et al 12 argue that the medical school environment itself remains the primary barrier to effective treatment, with traditional interventions failing to address the root causes adequately.
The relationship between student loan burden and psychological distress presents another critical concern. Students carrying debt exceeding $300,000 reported mean GAD-7 scores of 12.80 and PHQ-9 scores of 13.40, indicating symptom ranges approaching severe levels. These scores were more than double those of students with minimal debt (GAD-7: 2.00, PHQ-9: 3.00 for those with less than $10,000 in loans). Although we were unable to perform formal statistical testing due to insufficient group sizes across loan categories, the 33 descriptive patterns are striking. Previous systematic reviews have documented similar associations, noting that high medical student debt affects not only mental health but also academic performance and specialty choice, potentially steering students away from primary care fields where physician shortages are most acute. 13 While this association emerged from exploratory analysis rather than a priori hypothesis testing, the magnitude of the relationship warrants urgent attention. The dose-response pattern we observed, with symptoms nearly doubling from the lowest to the highest debt categories, suggests that financial stress may amplify the psychological burden of medical training in clinically meaningful ways.
The cross-sectional design prevents us from establishing causal relationships or tracking individual trajectories through medical school. Our exclusion of students with chronic medical conditions, while methodologically sound for isolating medical school-specific effects, likely leads to an underestimation of the overall mental health burden. Additionally, the GAD-7 and PHQ-9 are validated screening instruments with good sensitivity and specificity. Still, they cannot establish clinical diagnoses of anxiety or depression disorders, which require comprehensive evaluations by qualified professionals. Our prevalence estimates, therefore, reflect symptom burden rather than diagnosed disorders. While these tools are widely used in medical student populations for research purposes, readers should interpret our findings as indicators of psychological distress requiring further clinical assessments rather than definitive diagnoses. Research on medical students with chronic conditions remains limited, with Jain 14 noting that equitable access remains elusive for disabled students who face additional stigmatization affecting disclosure and mental health. Meeks et al 15 explicitly identify this as an understudied area, with limited longitudinal data on the success of this population. Additionally, our sample size of 126 students limited statistical power, particularly for subgroup analyses examining treatment effects and loan burden associations. A prior power calculation was not conducted, which we acknowledge as a methodological limitation; however, our census sampling approach (inviting all eligible students) represents the maximum feasible recruitment for this single-institution study. This was one limitation of this study.
These findings carry important implications for medical education reform. The persistence of elevated symptoms across training years, and the apparent ineffectiveness of current treatments within the medical school context suggest that conventional wellness initiatives are inadequate. Recent systematic reviews support this assessment. Bennett-Weston et al 16 conducted a meta-review of 13 systematic reviews encompassing 94 studies and 17,616 students. They found that 11 reviews were rated “critically low” quality, while only 2 were rated “low” quality, with limited evidence for the effectiveness of interventions. Da Silva et al 17 found only small effect sizes for mindfulness interventions (SMD = 0.29) in their meta-analysis of eight RCTs. Meaningful reform requires addressing structural factors, including evaluation systems that perpetuate competition, the hidden curriculum that often prioritizes endurance over health, and the financial burden that compounds academic stress. For students with pre-existing mental health conditions, our data indicates that current support systems are failing to provide adequate protection against medical school stressors. These students may require enhanced monitoring, prophylactic treatment intensification during predictable high-stress periods, and specialized support programs that recognize their vulnerability while supporting their professional development.
Future research should prioritize longitudinal designs that track individual students from matriculation through graduation and into residency. Such studies could distinguish between actual developmental patterns and cohort effects while identifying critical periods for intervention. Qualitative research exploring students’ lived experiences could illuminate the mechanisms underlying our quantitative findings and identify protective factors among those who maintain well-being despite challenges. Most importantly, we need rigorous evaluation of structural interventions such as expanded pass-fail grading, debt relief programs, and protected time for mental health care without academic penalty. Successful examples exist: Slavin et al 18 documented remarkable improvements at Saint Louis University following comprehensive reforms, including pass-fail grading, curriculum reduction, and learning communities, with depression rates dropping from 27% to 4% and anxiety declining from 56% to 14%. Bloodgood et al 19 found that pass-fail students at Mayo Medical School experienced significantly less stress than their traditionally graded peers, while maintaining equivalent USMLE Step 1 scores.
Our findings contribute to growing evidence that mental health challenges among medical students reflect systemic issues rather than individual vulnerabilities. The combination of persistent symptoms across years, ineffective treatments for at-risk students, and the amplifying effect of financial stress reveals fundamental tensions within medical education. We teach the importance of mental health while creating environments that undermine it. We emphasize evidence-based practice while maintaining traditions that lack empirical support for their educational value. These contradictions between stated values and institutional practices suggest that addressing the mental health crisis in medical education will require more than incremental adjustments. Instead, it demands a fundamental reexamination of how we train physicians and what costs we are willing to accept that process.
Conclusion
This study contributes important data to the growing body of evidence documenting mental health challenges among medical students worldwide. Our findings at VHS-ODU, with 23.8% of students screening positive for clinically significant depression and 18.3% for anxiety, mirror the prevalence rates reported across medical schools globally, confirming that these challenges reflect systemic issues within medical education rather than institution-specific factors. By openly examining these patterns, our institution demonstrates a commitment to understanding and addressing student well-being.
Our analysis revealed three critical patterns that align with broader trends in medical education research. First, students with pre-existing mental health conditions showed elevated symptoms throughout training despite treatment, suggesting that standard therapeutic approaches require adaptation for the unique demands of medical education. Second, the association between higher student debt and increased symptom severity underscores how financial pressures interact with academic stress, a challenge facing medical students nationwide as education costs continue to rise. Third, the intensification of stress during clinical years, reported by nearly 80% of students in clinical training, reflects the complex transition from classroom to patient care that medical educators nationwide are working to improve.
These findings position our institution to contribute meaningfully to national efforts addressing medical student well-being. Potential areas for leadership include implementing routine mental health screening at matriculation and key transition points, with automatic referral pathways for students scoring above clinical thresholds. For students carrying debt exceeding $200,000, targeted financial counseling coupled with mental health support could address the compound stressors we identified. The dramatic increase in perceived pressure during clinical years suggests the need for structured transition programs, protected wellness time during rotations, and re-evaluation of subjective evaluation methods that may exacerbate anxiety.
Our study has limitations that should guide interpretation and future research. The cross-sectional design captures only a snapshot of student experiences, and the 21% response rate, while typical for medical student surveys, may not fully represent all student perspectives and could be one of the limiting factors for this study. Longitudinal studies tracking students from matriculation through residency would provide valuable insights into symptom trajectories and critical intervention points. Additionally, qualitative research exploring students’ experiences and coping strategies could inform more targeted support programs.
The consistency between our institutional findings and international data underscores that medical students’ mental health is a shared challenge that requires collaborative solutions across medical education. By documenting these patterns and contributing to the evidence base, institutions like ours can help drive systemic improvements that benefit students everywhere. The path forward requires an honest assessment of current practices, a willingness to implement evidence-based reforms, and a commitment to creating training environments that support both professional development and personal well-being. Through such efforts, medical education can better align its practices with its values, producing physicians who are not only clinically competent but also psychologically healthy and prepared for sustainable careers in medicine.
Supplemental material
Supplemental material - Mental Health Among Medical Students at VHS-ODU: A Cross-Sectional Survey
Supplemental material for Mental Health Among Medical Students at VHS-ODU: A Cross-Sectional SurveyMental Health Among Medical Students at VHS-ODU: A Cross-Sectional Survey by Foroozan Afsharchi, Joshua F. Edwards, Kailash S. Ram, Jingru Haung, Valicia Hale, and Ismail El Moudden in Journal of Medical Education and Curricular Development.
Supplemental material
Supplemental material - Mental Health Among Medical Students at VHS-ODU: A Cross-Sectional Survey
Supplemental material for Mental Health Among Medical Students at VHS-ODU: A Cross-Sectional SurveyMental Health Among Medical Students at VHS-ODU: A Cross-Sectional Survey by Foroozan Afsharchi, Joshua F. Edwards, Kailash S. Ram, Jingru Haung, Valicia Hale, and Ismail El Moudden in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgements
The authors thank the medical students of Macon & Joan Brock Virginia Health Sciences at Old Dominion University (VHS-ODU) who participated in this study. We are grateful to the Office of Student Affairs at VHS-ODU for facilitating survey distribution; Dr. Allison Knight for her collaboration in coordinating student wellness resources and supporting participant access; the VHS-ODU Institutional Review Board for ethical oversight; the Research and Infrastructure Services Enterprise (RISE) at VHS-ODU for statistical and infrastructure support; and the Office of Medical Student Research with student outreach. The authors also acknowledge the broader VHS-ODU community for supporting research on student well-being.
Ethical Considerations
This study was approved by the IRB committee at VHS-ODU, protocol #24-06-XX-0151. Also approved by Student Affairs at VHS-ODU.
Author Contributions
Funding
This research received no external funding. Institutional resources used in the conduct of the study , including REDCap data infrastructure, IRB administration, and distribution support from the Office of Student Affairs at Macon & Joan Brock Virginia Health Sciences at Old Dominion University , were provided in-kind.
Declaration of Conflicting Interests
The authors declare the following potential non-financial interests: F.A. serves as Director of Student Health at VHS-ODU, the institution from which study participants were recruited; J.F.E. serves as Director of Medical Student Research at the same institution; I.E.M. serves as Assistant Director of Data Sciences and Analytics within the Research and Infrastructure Services Enterprise at the same institution and provided statistical oversight for this study; K.S.R., J.H., and V.H. were enrolled medical students at VHS-ODU during the conduct of this study. These institutional roles motivated the research question but did not influence data collection, analysis, or interpretation, as participation was anonymous and the analytic dataset contained no identifiers. The authors declare no financial conflicts of interest with respect to the research, authorship, or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.