
Abstract
Introduction
Hiroshima University, in collaboration with BeRISE Corp, developed a virtual reality-based objective structured clinical examination (VR OSCETM) practice software, as an educational tool to enhance clinical skills. This study aimed to assess the effectiveness of training with VR OSCETM for medical students.
Methods
Twenty medical students participated in this prospective, pre- and post-intervention study. They conducted medical interviews and physical examinations of simulated patients using VR OSCETM and presented their findings. Two instructing doctors assessed and scored their performance based on predefined criteria before and after training. A paired t-test was used to analyze the pre- and post-training scores of five parameters: (a) safety checks, (b) patient care, (c) medical interviews and physical examinations, (d) presentation skills, and (e) overall performance. A questionnaire survey was also administered to assess participants’ perceptions of VR OSCETM.
Results
Post-training scores significantly improved across all parameters compared with pre-training scores (p < 0.01). Scores for (a) safety checks (Pre: 6.0 ± 1.9, Post: 8.6 ± 1.8) and (b) patient care (Pre: 4.6 ± 1.8, Post: 7.8 ± 1.1) were close to the OSCE passing threshold prior to training. Notably, there were remarkable improvements in scores for (c) medical interviews and physical examinations (Pre: 4.1 ± 1.7, Post: 7.3 ± 1.2) and (d) presentation skills (Pre: 3.5 ± 1.3, Post: 7.0 ± 1.6). Scores for (e) overall performance (Pre: 3.8 ± 1.3, Post: 7.2 ± 1.5) mirrored these improvements. The survey indicated that all participants recognized the effectiveness of training with VR OSCETM as a component of OSCE certification preparation.
Conclusion
This study is the first to evaluate the educational impact of VR OSCE™ training in medical students. VR-based training appears to be effective, likely due to its immersive nature. These findings suggest that VR-based digital simulation has substantial potential to enhance medical education.
Keywords
Introduction
Virtual reality (VR) is a technology that creates simulated environments resembling the real world and is widely applied across various fields and industries. 1 The effectiveness of VR as an educational and training tool is well recognized, as it enhances learning by enabling users to become fully immersed in an interactive, virtual environment that closely mirrors the real world. 2 Furthermore, VR facilitates interaction within these virtual settings through specialized headsets, controllers, and hands-on experiential learning. Accordingly, VR is considered highly effective in medical education.3,4 It is used for anatomy education, practicing surgical procedures, and training in cardiopulmonary resuscitation and advanced life support.5-8
Hiroshima University has contributed to these advancements by developing an interventional radiology (IR) simulator that employs a VR system (the VR-IR simulator). 9 The VR-IR simulator serves as a platform for training students to perform IR procedures within virtual environments. Mitani et al 9 reported that the VR-IR simulator has been used to train medical students in endovascular procedures.
We, along with BeRISE Corp, recently co-developed a virtual reality-based objective structured clinical examination practice software (VR OSCETM) (Figure 1A),
10
which is designed as an educational tool to facilitate social distancing. VR OSCETM enables medical students to practice both medical interviews and physical examinations. Tasks include inspection, auscultation of cardiac and pulmonary sounds, and neurological examinations using a percussion device (Figure 1B and C). This software allows learners to select interview items based on the patient’s age, chief complaints, and medical history. Using VR goggles (Pico Neo3), students can engage in a highly realistic and safe virtual environment11,12 to improve their clinical skills through repeated practice. VR OSCETM covers 20 medical scenarios selected according to the foundational diseases outlined in the Model Core Curriculum for Medical Education, as established by the Japan Society for Medical Education.
13
This curriculum ensures that medical students acquire the essential knowledge and skills required for medical practice in Japan. VR OSCETM. (A) Visual representation of the VR OSCETM interface. (B) Simulation of patient interviews within the software. (C) Simulation of diagnostic and physical examination procedures. (D) Scenarios can be freely added or modified using Excel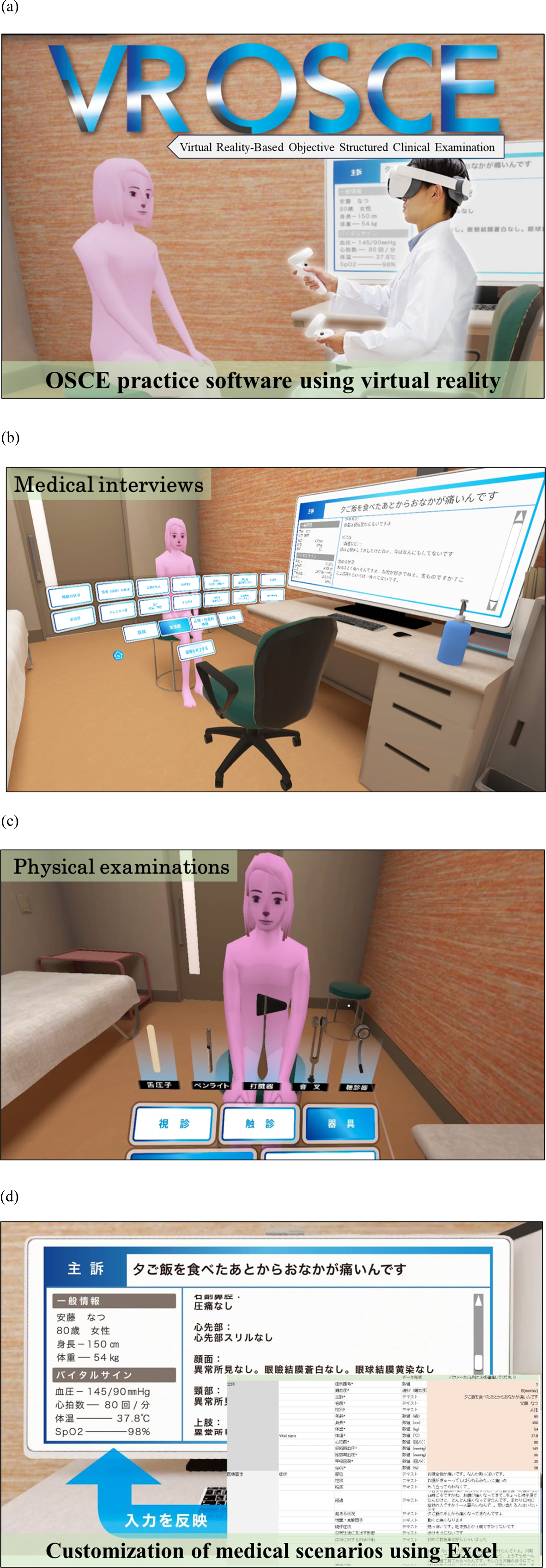
In this study, we assess the effectiveness of VR OSCETM for the clinical training of medical students. By comparing student skill evaluations before and after VR OSCETM training, this study aims to evaluate the impact of VR-based learning on clinical skills development.
Materials and Methods
This prospective, pre- and post-intervention study was designed to evaluate the effectiveness of VR OSCETM and was conducted and reported in accordance with the STROBE statement (Supplementary Material 1). 14 A priori power analysis was conducted using G*Power statistical packages (G*Power Ver. 3.1.9.2, Universität Düsseldorf, Düsseldorf, Germany) 15 for a paired t-test (two-tailed). With an effect size of d = 0.8, an alpha level of 0.05, and a power of 0.80, the minimum required sample size was determined to be 15 participants. 16 Medical students from Hiroshima university who had passed the pre-OSCE in their fourth year and provided written informed consent were eligible for inclusion, while those who failed were excluded. Consequently, twenty fourth- and fifth-year medical students at Hiroshima University were randomly selected and enrolled. Participants received an advanced briefing, and practical training was conducted at the university’s training center. The study spanned the period from April to September 2023. Ethics approval for this study was obtained from Hiroshima University (approval E2023-0030).
The study was structured as follows (Figure 2). VR OSCETM covers 20 medical scenarios categorized into three difficulty levels (A: easy, B: normal, C: hard). First, each medical student randomly selected a scenario, limited to the easiest difficulty level (Level A). Scenarios were randomized using a shuffled list of Level A scenarios. Using VR OSCETM, students conducted medical interviews and performed physical examinations on simulated patients. Students then presented their findings regarding the patients, including differential diagnoses. Through an external monitor, two instructors evaluated their performance based on five assessment criteria using standard OSCE evaluation protocols. Second, a third instructor, distinct from the previous two instructors, provided training using VR OSCETM. During this phase, students engaged in two scenarios at any difficulty level and received feedback from the instructor. Third, students chose another easy scenario that they did not previously complete. They conducted medical interviews once again, performed physical examinations, and delivered presentations. The same two instructors scored this session using the same criteria as those in the initial assessment. Study design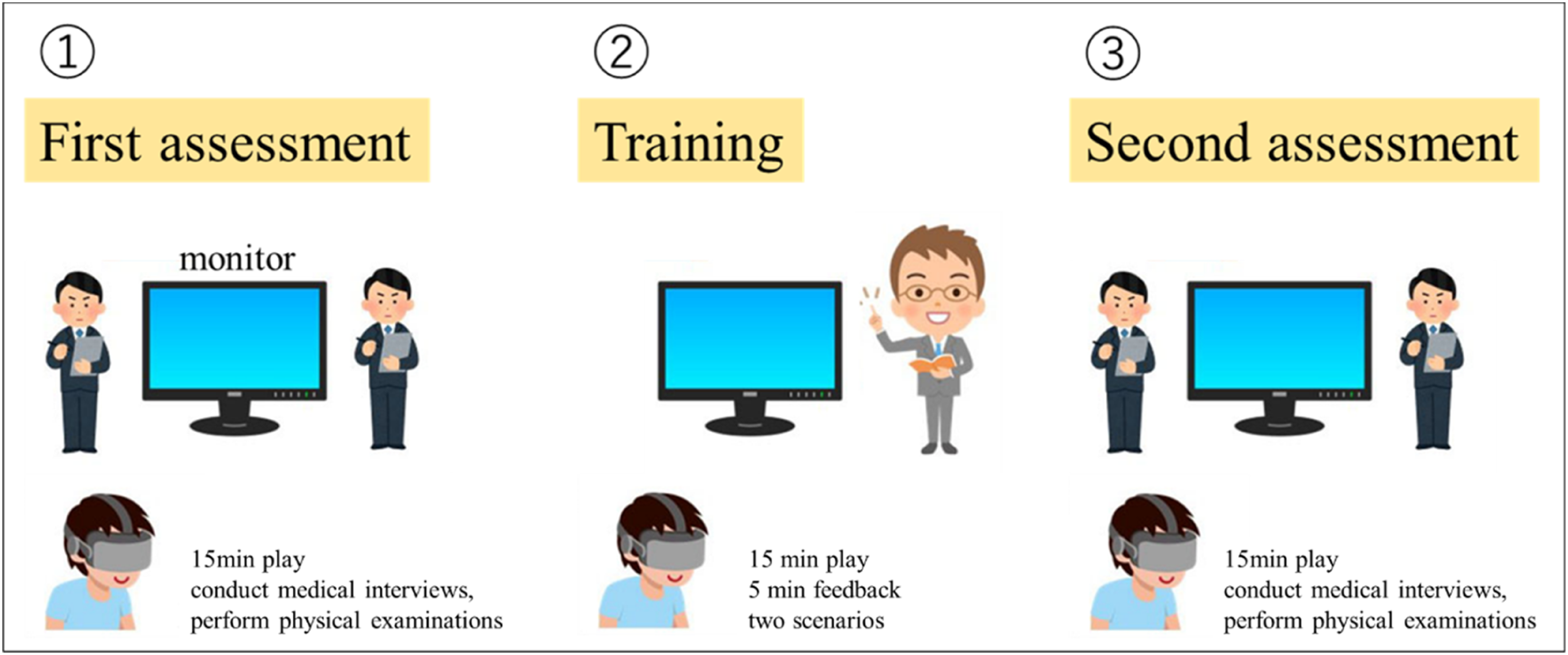
The figure outlines the process in which students conducted medical interviews and physical examinations of simulated patients using VR OSCETM, followed by presentations. Performance was assessed by two instructors via an external monitor (first assessment). After undergoing training on two additional scenarios with a different instructor, students completed another scenario and their performance was re-evaluated by the same instructors (second assessment) as those in the initial assessment.
The following five evaluation criteria were used: (a) safety checks, including patient verification and hygiene; (b) patient care such as greeting and conversation; (c) medical interviews and physical examinations focused on the primary complaint; (d) presentation skills, including differential diagnosis and diagnostic reasoning; and (e) overall performance, capturing general impressions (Figure 3). Evaluation items and criteria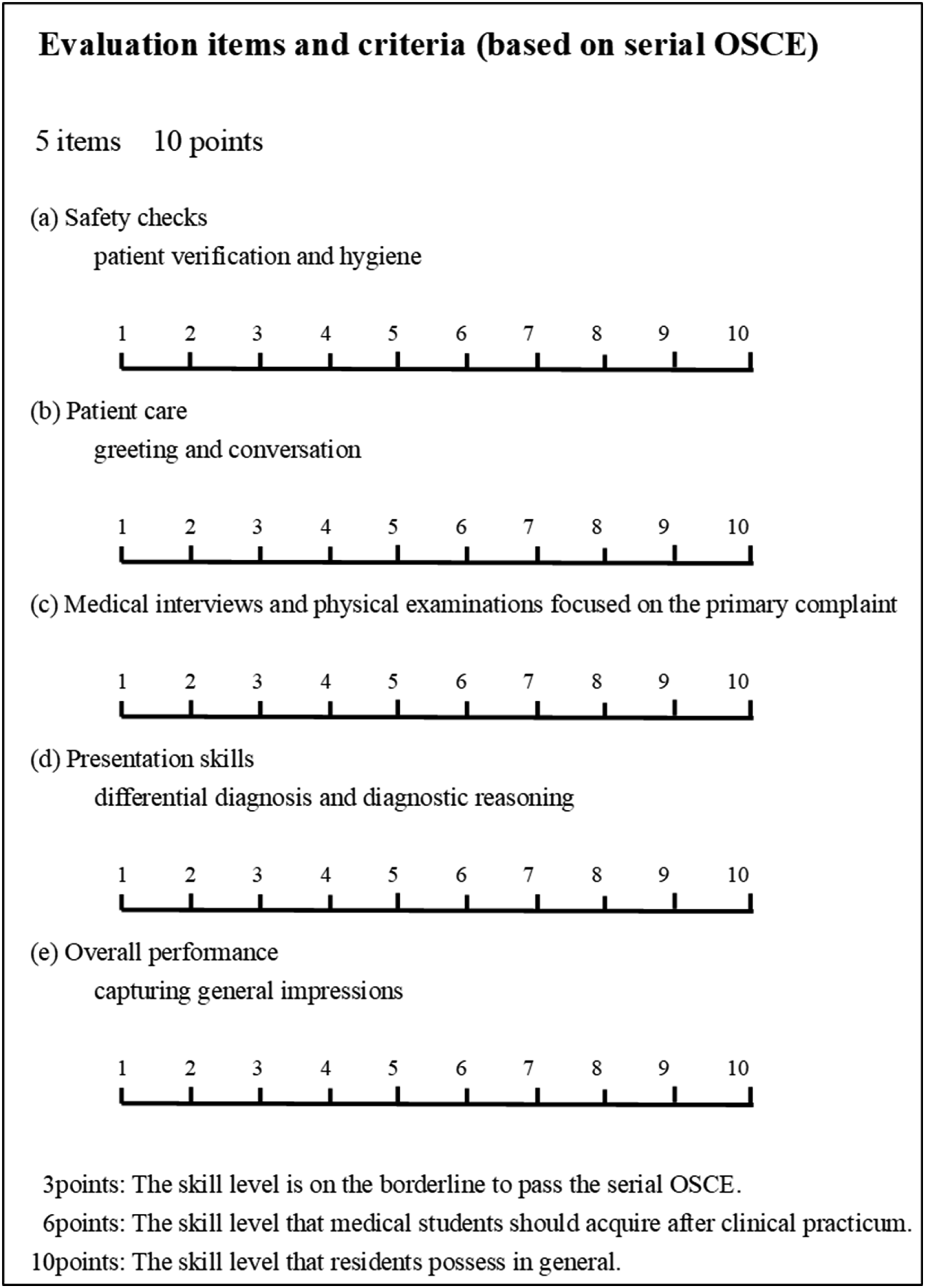
Student performance was assessed based on five evaluation items using serial OSCE assessment criteria.
The evaluation criteria were rated on a 10-point scale, with scores defined as follows: 3 points represent OSCE borderline performance, 6 points represent the OSCE passing threshold, 8 points reflect the proficiency expected at graduation, and 10 points correspond to internship-level competency.
After the second VR session, all 20 medical students were surveyed to evaluate the perceived effectiveness of VR OSCETM. The survey included items rated on a 5-point Likert scale (Questions 1–9) and closed-ended yes/no questions (Questions 10–12) (see Supplementary Figure 1). Any adverse events related to the training were also recorded.
Statistical analysis was performed using R (version 3.2.3; R Foundation for Statistical Computing, Vienna, Austria). Scores before and after training were compared statistically. After confirming normality using the Shapiro–Wilk test, a paired t-test was used to assess differences in each criterion between pre- and post-training evaluations. Statistical significance was defined at p < 0.05 for all analyses.
Results
The results are presented in Figure 4. Scores for (a) safety checks, including patient verification and hygiene (Pre: 6.0 ± 1.9, Post: 8.6 ± 1.8) and (b) patient care such as greeting and conversation (Pre: 4.6 ± 1.8, Post: 7.8 ± 1.1) were close to the OSCE passing threshold prior to training. By contrast, scores for (c) medical interviews and physical examinations focused on the primary complaint (Pre: 4.1 ± 1.7, Post: 7.3 ± 1.2) and (d) presentation skills, including differential diagnosis and diagnostic reasoning (Pre: 3.5 ± 1.3, Post: 7.0 ± 1.6), showed significant improvement. Initially, these scores were below the OSCE borderline performance level but surpassed the passing threshold after training. Scores for (e) overall performance, capturing general impressions (Pre: 3.8 ± 1.3, Post: 7.2 ± 1.5), mirrored these improvements. The increase in post-training scores across all parameters was statistically significant (p < 0.01). Educational effects of VR OSCETM evaluation items included (A) safety checks, including patient verification and hygiene; (B) patient care such as greeting and conversation; (C) medical interviews and physical examinations focused on the primary complaint; (D) presentation skills, including differential diagnosis and diagnostic reasoning; and (E) overall performance, capturing general impressions. VR OSCETM demonstrated significant effectiveness in all areas of education (p < 0.01)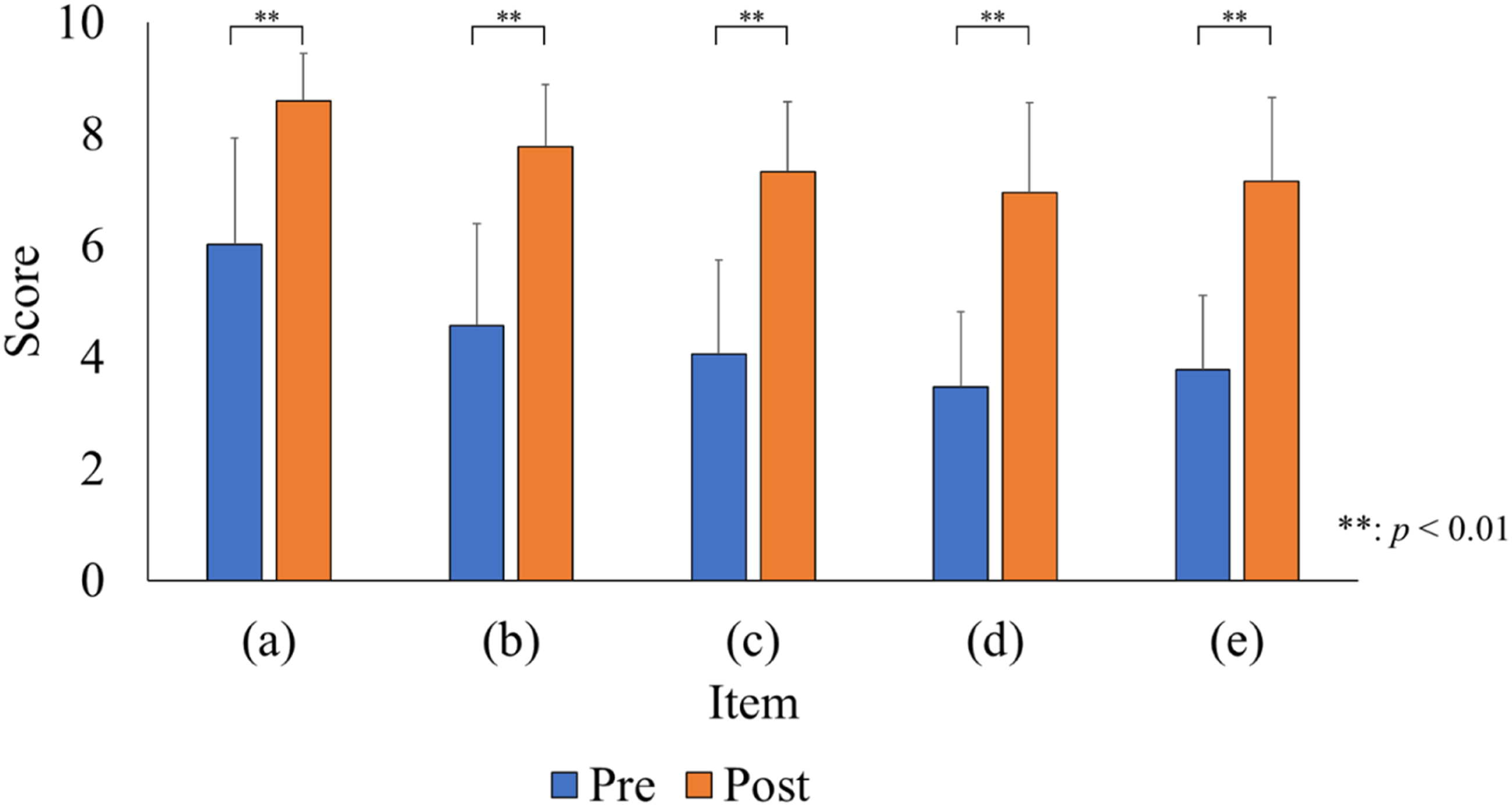
Survey Results of VR OSCETM Evaluation
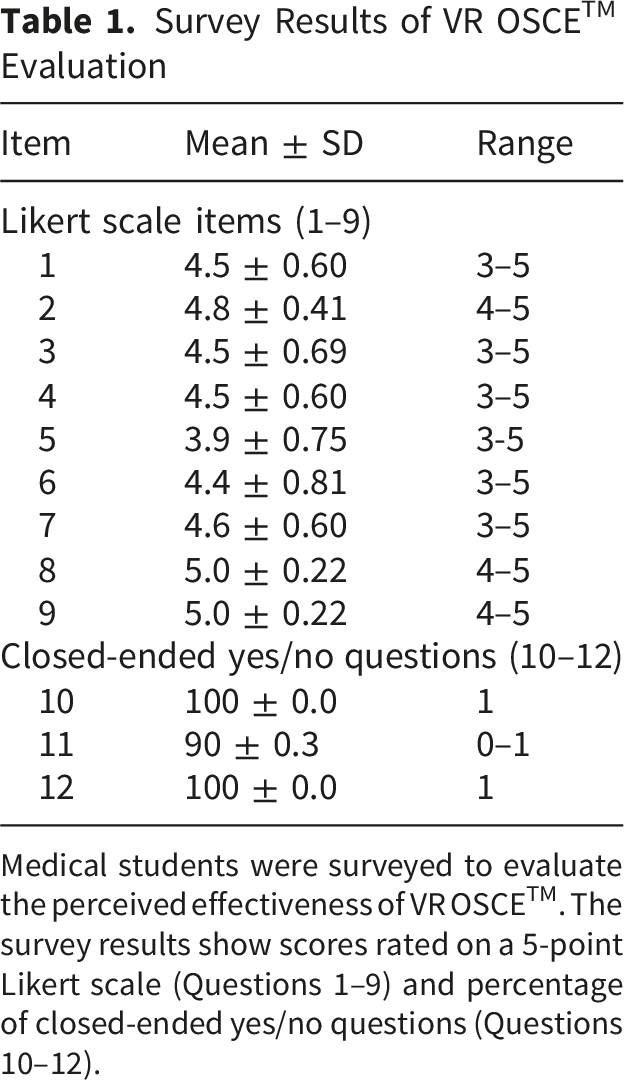
Medical students were surveyed to evaluate the perceived effectiveness of VR OSCETM. The survey results show scores rated on a 5-point Likert scale (Questions 1–9) and percentage of closed-ended yes/no questions (Questions 10–12).
Discussion
The Coronavirus Disease 2019 pandemic, first identified in December 2019, 17 significantly affected medical education, particularly clinical clerkships. To maintain social distancing, 18 opportunities for patient care and bedside teaching were restricted, thereby limiting medical students’ ability to develop essential OSCE examination skills. Tzeng et al 19 reported that the pandemic adversely affected medical students’ clinical training, resulting in diminished OSCE skills and scores. In Japan, medical students must pass a national OSCE following their clinical clerkship to obtain a medical license within a six-year curriculum that includes approximately two years of clinical participation. At our hospital, restrictions similar to those mentioned above reduced students’ opportunities to practice history taking, physical examinations, and medical communication.
As a response, simulation-based education in the medical field has become increasingly significant.20,21 Hiroshima University developed VR OSCETM to address the aforementioned challenges while also minimizing infection risk. VR OSCETM offers a simulated environment in which students can practice medical interviews and physical examinations in a virtual consultation room, providing realistic, repeatable practice opportunities. This study is the first to examine the educational effects of training with VR OSCETM on medical students.
Although students participated in only two VR training sessions with feedback between pre- and post-evaluation, VR OSCETM demonstrated a substantial educational impact (Figure 4). Two main factors likely contributed to this result. The first factor is the immersive nature of VR, which provides a heightened sense of realism and engagement and is beneficial for education.3,4 Although other virtual patient simulators such as Body Interact® have been reported for medical training, 22 VR OSCETM is unique as a VR-based system specifically designed for OSCE training. In fact, many students reported that VR OSCE™ is an effective training tool that allows them to experience real OSCE settings. One student noted, “The VR OSCE provided an environment that closely mirrored real OSCE conditions, including the clinical atmosphere, structured workflow, and sense of time pressure during patient encounters.”
The second factor relates to VR OSCETM’s game-like features. During VR training, patient responses are displayed at a normal conversational pace and diagnostic tools replicate real-life timing. Students must manage their time within the 15-minute limit, navigating the interview and examination under realistic time constraints. This gameplay element enhances motivation and aligns with the growing use of gamification as an effective learning strategy, while also promoting engagement and a constructive competitive environment. 23
The primary feature of VR OSCETM is Excel-based scenario customization (Figure 1D). In contrast to conventional simulation software, which primarily offers preset cases, VR OSCETM enables learners to design and share structured clinical scenarios incorporating differential diagnoses and patient profiles. This customizability facilitates active learning, encouraging students to apply their knowledge and enhancing their educational experience.
This study has some limitations. First, VR OSCETM was developed as practice software aligned with OSCE components and timing constraints, and it currently does not include advanced diagnostic elements such as blood tests or imaging studies. Second, VR OSCETM lacks voice recognition and automated assessment capabilities, making instructor and student feedback essential to optimize learning. Future developments will aim to address these limitations and enhance the software’s functionality. Additionally, this study was limited to VR-based scenarios. We therefore plan a case-control study comparing students trained with VR OSCETM and those without such training, evaluating real OSCE performance using predefined outcome measures, including clinical performance scores, time efficiency, and communication skills.
Although the required sample size based on a priori power analysis was achieved, the small number of participants remains a limitation of this study. Furthermore, since this study was conducted at a single institution, the generalizability of our findings may be limited. The two instructors assessed the same participants during pre- and post-training, which may have introduced recall bias, as familiarity with participants’ prior performance could have influenced subsequent scoring. To address these limitations, future studies should include larger, multi-institutional cohorts to improve generalizability. The use of blinded or independent evaluators may help reduce recall bias, and incorporating objective performance metrics from VR systems could enhance the reliability of assessments.
Conclusions
This study comprehensively evaluated the effectiveness of training with VR OSCETM as a learning tool to enhance clinical skills. The results revealed that medical students who underwent VR OSCETM training demonstrated improved performance in medical interviews and physical examinations compared with that before training. Digital simulation–based education using VR has the potential to transform medical curricula by providing immersive, standardized, and repeatable training environments that enhance clinical skill acquisition, decision-making, and learner assessment.
Supplemental Material
Supplemental Material - Educational Effects of Training with a Virtual Reality-Based Objective Structured Clinical Examination Software
Supplemental Material for Educational Effects of Training with a Virtual Reality-Based Objective Structured Clinical Examination Software by Ryo Touge, Isamu Saeki, Minoru Hattori, Sho Kurihara, Masato Kojima, Yukiko Honda, Eiso Hiyama, Kazuo Awai, Naoko Hasunuma, and Shinya Takahashi in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Educational Effects of Training with a Virtual Reality-Based Objective Structured Clinical Examination Software
Supplemental Material for Educational Effects of Training with a Virtual Reality-Based Objective Structured Clinical Examination Software by Ryo Touge, Isamu Saeki, Minoru Hattori, Sho Kurihara, Masato Kojima, Yukiko Honda, Eiso Hiyama, Kazuo Awai, Naoko Hasunuma, and Shinya Takahashi in Journal of Medical Education and Curricular Development.
Footnotes
ORCID iDs
Ethical Considerations
This study received ethical approval from Hiroshima University (approval E2023-0030) on June 29, 2023.
Consent to Participate
Written informed consent was obtained from all participants prior to participating in this study.
Author Contributions
Conceptualization, I.S.; methodology, M.H., N.H.; software, I.S., S.K.; validation, Y.H.; formal analysis, R.T.; investigation, R.T., I.S., S.K., M.K.; resources, I.S., N.H.; data curation, R.T.; writing-original draft preparation, R.T., I.S.; writing-review and editing, R.T.; visualization, R.T.; supervision, I.S., E.H., S.T.; project administration, I.S., N.H., S.T.; funding acquisition, I.S. All authors have read and approved the final published version of the manuscript, and all authorship requirements have been met.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Ministry of Education, Culture, Sports, Science, and Technology (MEXT) through the “Digital Education Enhancement Plan for Universities and Colleges of Technology” grant. The funders had no role in the study design, data collection, analysis, interpretation of data, writing of the manuscript, or decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VR OSCETM, which is an OSCE practice software incorporating VR, was developed in collaboration with BeRISE Corp. Isamu Saeki, Minoru Hattori, Shinya Takahashi, Naoko Hasunuma, and Kazuo Awai hold patent rights to the know-how licensed by BeRISE Corp. The other authors declare no financial or personal conflicts of interest that could have influenced the outcomes of this study.
Data Availability Statement
The datasets used and analyzed in this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.