
Abstract
Background
One in four US children live in immigrant families, and 16% of US children live in poverty. To provide optimal medical care for these populations, additional knowledge and skills are needed. It is unknown whether residency training is adequately preparing physicians to care for these populations. We surveyed pediatric residents to understand if training on the needs of children in immigrant and low-income families was associated with self-reported preparedness and plans to care for these populations.
Methods
A cross-sectional survey was conducted in a large midwestern pediatric residency. Questions related to resident demographics, exposure to specific curricular components, future career plans, and residents’ report of feeling prepared to care for children in immigrant families and children in low-income families. Data were analyzed using descriptive statistics and Fisher’s exact test.
Results
Of 158 potential responses, 96 completed surveys were analyzed (61% response rate). Residents had been interested in training programs that would allow them to care for children in immigrant families (76%) and children in low-income families (93%). Most residents (89%) felt prepared to care for children in low-income families. Fewer residents (59%) felt prepared to care for children in immigrant families. Exposure to global health lectures (p = 0.04) and cultural humility training (p = 0.02) and other global health topics was associated with residents reporting feeling prepared to care for children in immigrant families. Residents whose future career plan included care for children in immigrant families or international populations were more likely to be exposed to elective global health training opportunities.
Conclusion
Pediatric residents are interested in caring for children in low-income and immigrant families. Exposure to specific global health and cultural humility training sessions was associated with feeling that residency prepared them to care for children in immigrant families and implementation of similar training into residency programs should be considered to improve care for immigrant families in the US.
Introduction
In recent decades, the proportion of immigrants and refugees has grown, accounting for nearly 14% of the United States (US) population. 1 One in four children in the US are immigrants or the children of immigrants.2,3 Over 40% of immigrant children live in low-income households, 3 compared to 16% of all US children.4,5 Children in immigrant families and children living in poverty represent important overlapping demographic groups who face many challenges related to social drivers of health, including barriers to healthcare access, discrimination, and economic instability.
Global health education may imply relevance only to international clinical care, however locally diverse populations can also benefit when physicians have global health training. Training experiences that include global health education and cross-cultural care have been associated with measurable improvement in trainees’ preparedness to care for diverse and underserved populations. Residents who participated in global health tracks or pathways demonstrate greater self-reported knowledge, skills, and attitudes toward caring for marginalized populations than national comparison cohorts. 6 Similarly, training in culturally appropriate care has been linked with higher patient satisfaction 7 and trainees with greater cross-cultural education and clinical exposure to underserved communities report increased comfort caring for populations with limited English proficiency,6,8 and other social vulnerabilities. 9
Residency training in pediatrics must prepare physicians to provide equitable, high-quality care to children of all backgrounds. While resident trainees report enjoyment in caring for immigrant and refugee patients, they also describe a lack of confidence and knowledge regarding the health and care of these populations.10,11 Even prior to residency, many graduating medical students note limited exposure to instruction on culturally sensitive care and care for immigrants and refugees, leaving them feeling underprepared to care for diverse patient populations. 12 This gap persists beyond training, with up to one third of practicing pediatricians and subspecialists reporting discomfort caring for immigrants and refugees. 13 The American Academy of Pediatrics (AAP) has highlighted the importance of incorporating education on cultural humility and the care of children in immigrant families within pediatric residency programs. 14
In response to these needs, our pediatric residency program developed and integrated global child health-focused educational components into the core curriculum with the goal of preparing all pediatric residents to care for diverse patient populations. Using Kern’s six-step model for curriculum development, this survey assesses resident needs in global health training (step 2) and collects evaluation and feedback (step 6) related to the implemented curriculum. 15 In this study focusing on questions related to evaluation and feedback, we examined whether exposure to global child health educational activities was associated with residents’ perceived preparedness to care for children in immigrant families and those in low-income families. We also explored residents’ self-reported initial interest in and future career plans to care for these populations as well as factors associated with career intentions.
Methods
Setting and Participants
This cross-sectional survey study took place at a large free-standing children’s hospital located within the midwestern region of the US. Both pediatric residents and combined pediatric residents who were enrolled in residency at the time of the survey were targeted for recruitment in the spring of 2021. Combined residency programs included residents in Medicine-Pediatrics, Pediatrics-Psychiatry-Child Psychiatry, Emergency Medicine-Pediatrics, Child Neurology, and Neurodevelopmental Pediatrics programs, all of whom participate in the general pediatric graduate medical curriculum. All eligible participants who were in enrolled pediatric residency training at our institution in March of 2021 were included. Medical trainees who were students, participating in pediatric fellowships or other residency programs outside of pediatrics at the time of the survey were excluded from the study. The Institutional Review Board (IRB) at the associated university provided exempt approval for this study (IRB Protocol # 10479).
Study Procedures
A survey aimed at understanding the experiences of residents exposed to the program’s global health (GH) curriculum was distributed to all categorical and combined pediatric residents (a total of 158 residents) via email using a Research Electronic Data Capture (REDCap) platform hosted at Indiana University in March 2021. 16 As an exploratory study to understand needs, attitudes, and experiences related to GH and a GH curriculum, this survey aimed to include all eligible trainees and a sample size calculation was not done. The survey was initially sent on March 15, 2021, via email with a link to the anonymous survey. To improve resident participation and reduce non-response bias reminders were sent via email and group text every 1-2 days over a 2-week period, and a $5 gift card incentive was provided to residents who included their email address on completion of the survey. Participation was voluntary, and participants completed an electronic participant agreement via REDCap prior to moving forward with the survey. Participants were asked to complete the survey within 10 days (by March 26, 2021); however, responses were open for a full 2 weeks. . The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist was utilized to review the reporting, and is available as a supplementary file (Supplement 1). 17
Survey Content
The survey used for this study was guided by global health-focused questions from the AAP Annual Survey of Graduating Residents questionnaires 18 and a prior survey of residents on the quality of their global health education in Wisconsin. 19 The annual AAP graduating questionnaire is a widely used questionnaire which is developed by experienced researchers based on literature review and is pilot-tested by pediatric residents. The Wisconsin survey was validated by several faculty members. 19 Using these source documents, the survey was developed by the study team with modifications to adapt questions to our curriculum. 20 Survey questions evaluated resident demographics and priorities used in selecting potential residency programs. Questions also evaluated current plans for specialization, location of future practice, and populations each resident plans to care for after training. The survey asked residents about their current feelings of if residency had prepared them to care for children in immigrant families, as well as children in low-income families. Exposure to curricular components during and prior to residency training was also assessed. Before implementation, the instrument was reviewed by faculty members with expertise in survey development (MSM, SLC), and was iteratively pilot tested by three pediatrics residents in the 158 member study population (2% of the study population), with refinement of questions based on feedback. Given the exploratory nature of this assessment, the team did not seek to validate the survey. The survey used is available for review as part of the supplemental materials (Supplement 2). The survey was administered via REDCap. 16
Programming and Curriculum Focused on Global Child Health Training
Global Child Health Curriculum Components
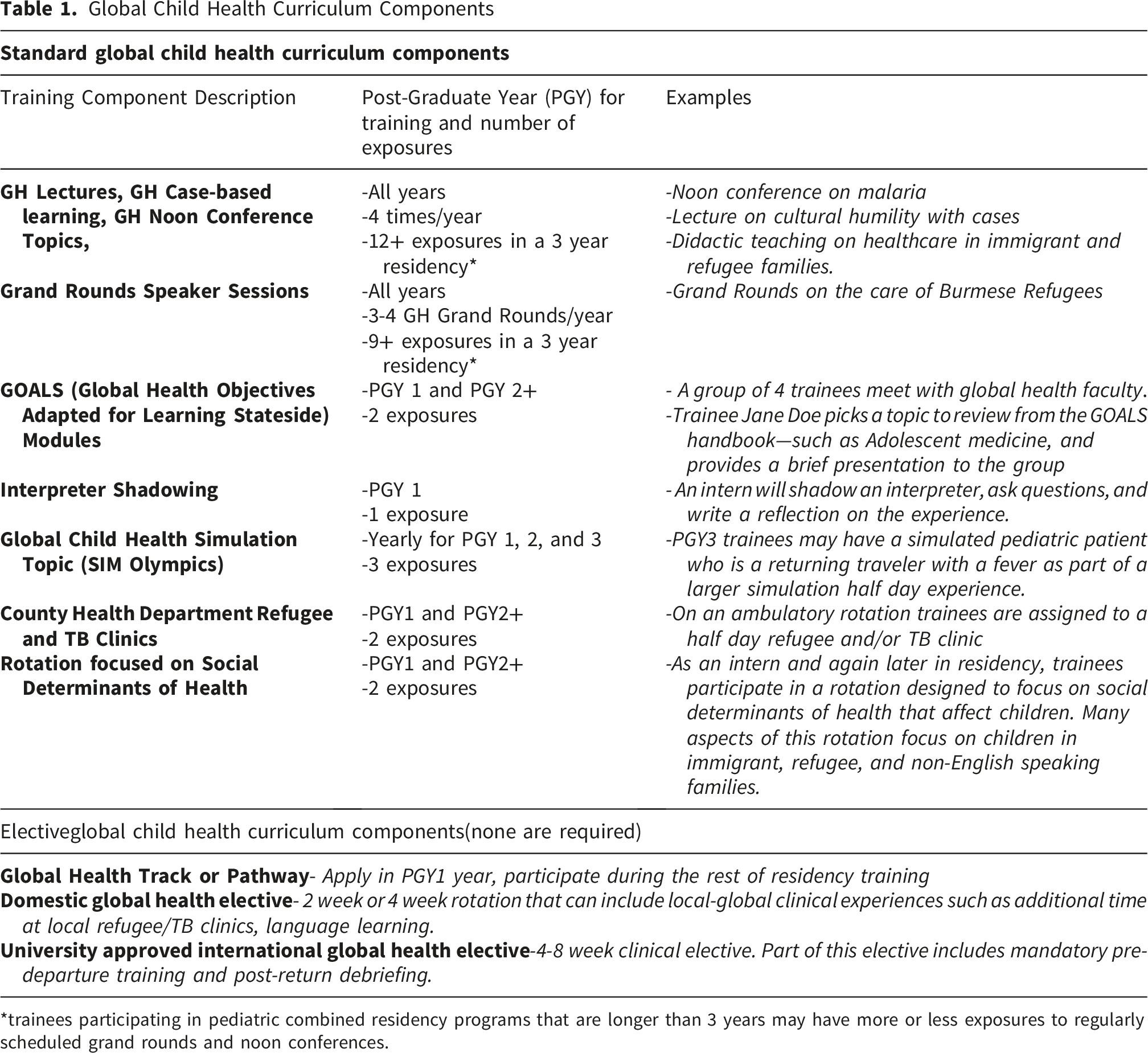
*trainees participating in pediatric combined residency programs that are longer than 3 years may have more or less exposures to regularly scheduled grand rounds and noon conferences.
Lecture and Conference Based Learning
The pediatric residency program hosts a noon conference session that occurs four weekdays per week consisting of 45-minute didactic sessions and a 30-minute clinical case. As part of the global health curriculum, quarterly noon conferences would cover the following topics: Health care of immigrant or refugee children and their families, Epidemiology of infant and child mortality in developing countries, Socioeconomic determinants of global child health, Diagnosis and management of malnutrition in developing countries, Diagnosis and management of common pediatric tropical diseases, Ethical issues in working or volunteering in developing countries, International child health policies, initiatives, and guidelines, Health care delivery systems in developing countries, and Preparation for responding to humanitarian emergencies. In addition, the Department of Pediatrics hosts hour-long weekly Grand Rounds sessions that are attended by trainees as well as faculty. Approximately four Grand Rounds sessions per year are dedicated to global health related topics. While attendance is not mandatory, trainees are strongly encouraged at all noon conferences and weekly Grand Rounds.
Small Group Learning-Self-Directed GOALS Modules
All pediatrics and combined program residents complete a self-directed learning module on a pediatric global health topic of their choice using the Global Health Objectives Adapted for Learning Stateside (GOALS) modules, 21 followed by a group debriefing session. For the GOALS module, residents select one set of objectives in pediatric global health and spend between 2-5 hours on individual self-directed learning reviewing the provided materials. The GOALS debriefing sessions are precepted by faculty with experience in global health. The GOALS discussion lasts between 1-2 hours depending on the number of residents participating each month. The GOALS sessions are part of the standard curriculum and occur twice during residency—once during the intern year, and again later in residency. A list of topics that can be selected for discussion as part of the GOALS modules and a link to access the official GOALS manual is included in the supplemental material [Supplement 3].
Experiential Learning—Interpreter, Simulation and Clinical Experiences
An interpreter session is a standard experience for all categorical and combined first year residents in their pediatric ambulatory rotation, comprised of direct observation of an in-person Spanish language interpreter followed by a written reflection on ways to optimize care for non-English speaking patients that is submitted online.
Simulation-based experiences are part of an annual simulation didactics program completed by all pediatric and combined program residents in their first, second, and third years of training. During the simulation sessions, one encounter is focused on objectives related to a “global health” communication focused scenario—caring for immigrant patients with specific concerns or troubleshooting barriers when utilizing a medical interpreter.22,23 Each simulation session lasts about 20-25 minutes including the simulated patient encounter and a guided debriefing with dedicated global health faculty. Over their residency training program, residents should experience a total of three different global health related simulation cases. Lastly, residents on their ambulatory rotation are scheduled to attend a half day of clinic at the county health department’s clinic for recently arrived refugees.
Optional Global Health Training
Optional activities include participation in domestic or international global health electives and clinical experiences at the public health department, such as spending time in the tuberculosis clinic. Residents can apply to and join the interdisciplinary global health pathway (formerly called the global health track), which provides a multi-year focus on training targeted towards those who plan to practice globally as part of their career.
Data Analysis
Study data were collected and managed using REDCap electronic data capture tools hosted at Indiana University. 16 Only those surveys with 75% or more of the survey completed were included in the analysis. By using this threshold, records with very few responses overall were excluded before analysis, and only records that included responses to both the demographic section of the survey and the key ‘preparedness’ outcome questions were included. Data analysis was performed using R 4.4.3. 24 Demographic data was summarized using descriptive statistics. Results of 6-point Likert-scale questionnaire data were summarized using frequencies. Fisher’s exact test was used to examine associations between curriculum exposures and outcomes such as future plans to care for children in low-income families, children in immigrant families, international populations abroad, and perceived preparedness to care for children in immigrant families, and children in low-income families. To assess directionality and calculate effect sizes, unadjusted odds ratios and 95% confidence intervals were calculated. In order to obtain the odds ratios and confidence intervals needed to evaluate effect size, exposure to each curricular component was re-coded as a binary variable: residents who participated in a curricular component either before or during residency were classified as “exposed” to the educational activity, and those who did not participate either before or during residency were classified as “not exposed.” Blank responses on the exposure variables were treated as “not exposed’ in the analysis. In similar fashion, perceived preparedness outcomes were dichotomized into “prepared” (Strongly Agree or Moderately Agree), and “not prepared” (all other responses). As this study is part of an exploratory evaluation of an educational curriculum, a sample size was not calculated prior to the study, a sensitivity analysis was not performed, adjustment for confounding was not performed, and no subgroup analyses or interaction terms were examined in the analysis. Alpha was set at 0.05.
Results
Demographic Information
Of the 158 potential respondents, 112 (71%) surveys were initiated within the study time frame. On review of data, 7 surveys were initiated but completely blank, 4 surveys included answers to some or all of part 1, 3 surveys included answers up to some or all of part 2, and 2 surveys included some questions in part 3 but did not reach the questions related to perceived preparedness. These 16 surveys were eliminated and were not included in the analysis. One incomplete survey that answered 92.5% of questions including answers to questions regarding preparedness and demographic questions was included in the analysis. This resulted in 96 resident responses included in the analysis (61% response rate).
Demographics
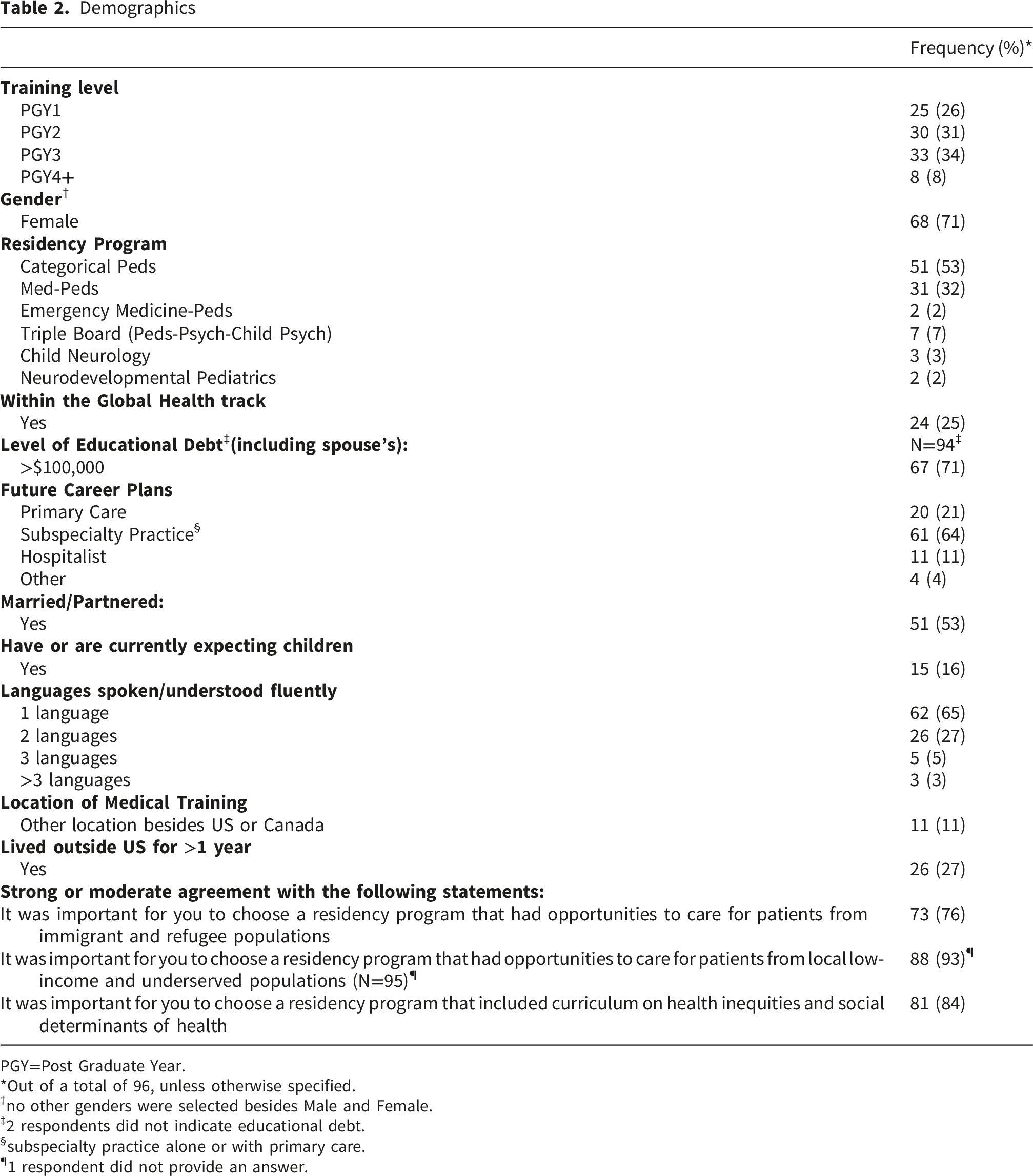
PGY=Post Graduate Year.
*Out of a total of 96, unless otherwise specified.
†no other genders were selected besides Male and Female.
‡2 respondents did not indicate educational debt.
§subspecialty practice alone or with primary care.
¶1 respondent did not provide an answer.
Before Residency
When reflecting on their goals prior to starting residency, most residents reported seeking residency programs with opportunities to work with children from low-income families (93%) and children in immigrant families (76%). In addition, most residents (84%) were interested in formal curriculum training on health inequities and social drivers of health when assessing residency programs (Table 1). Many reported that prior to residency they had experienced some formal global health (58%), cultural competency/humility training (72%), and 41 (43%) had been on personal or informal global health medical electives, with 36 (38%) reporting participation in university-approved international medical electives. Fewer residents had domestic global health experience (29%) or had shadowed a medical interpreter prior to residency (13%).
Self-Reported Preparedness for Clinical Care of Children in Low-Income and/or Immigrant Families
Preparedness to Care for Different Population Groups
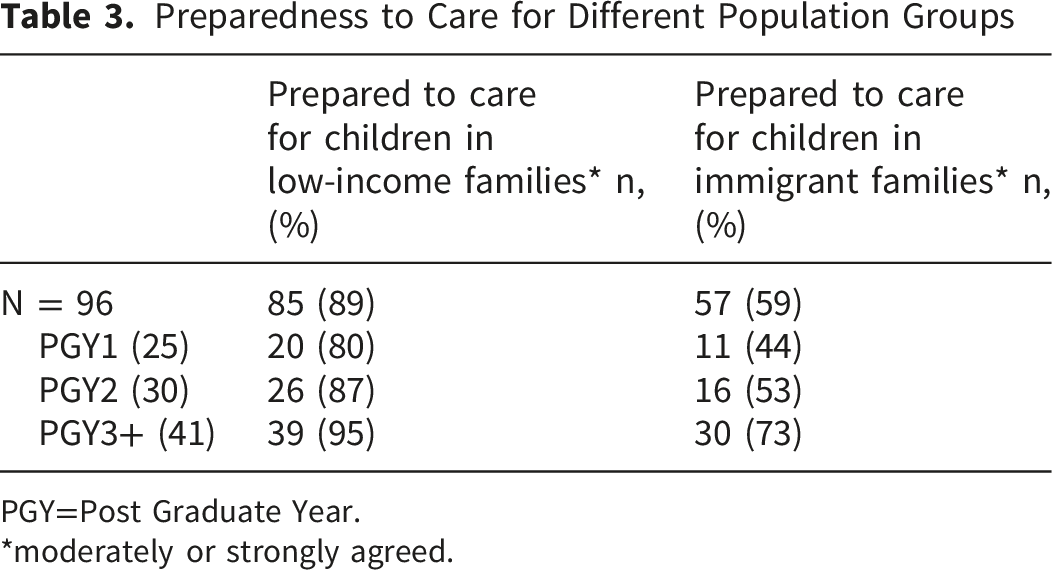
PGY=Post Graduate Year.
*moderately or strongly agreed.
Association of Curricular Components and Perceived Preparedness
Curricular Components or Other Exposures and Relation to Perceived Preparation to Care for Populations
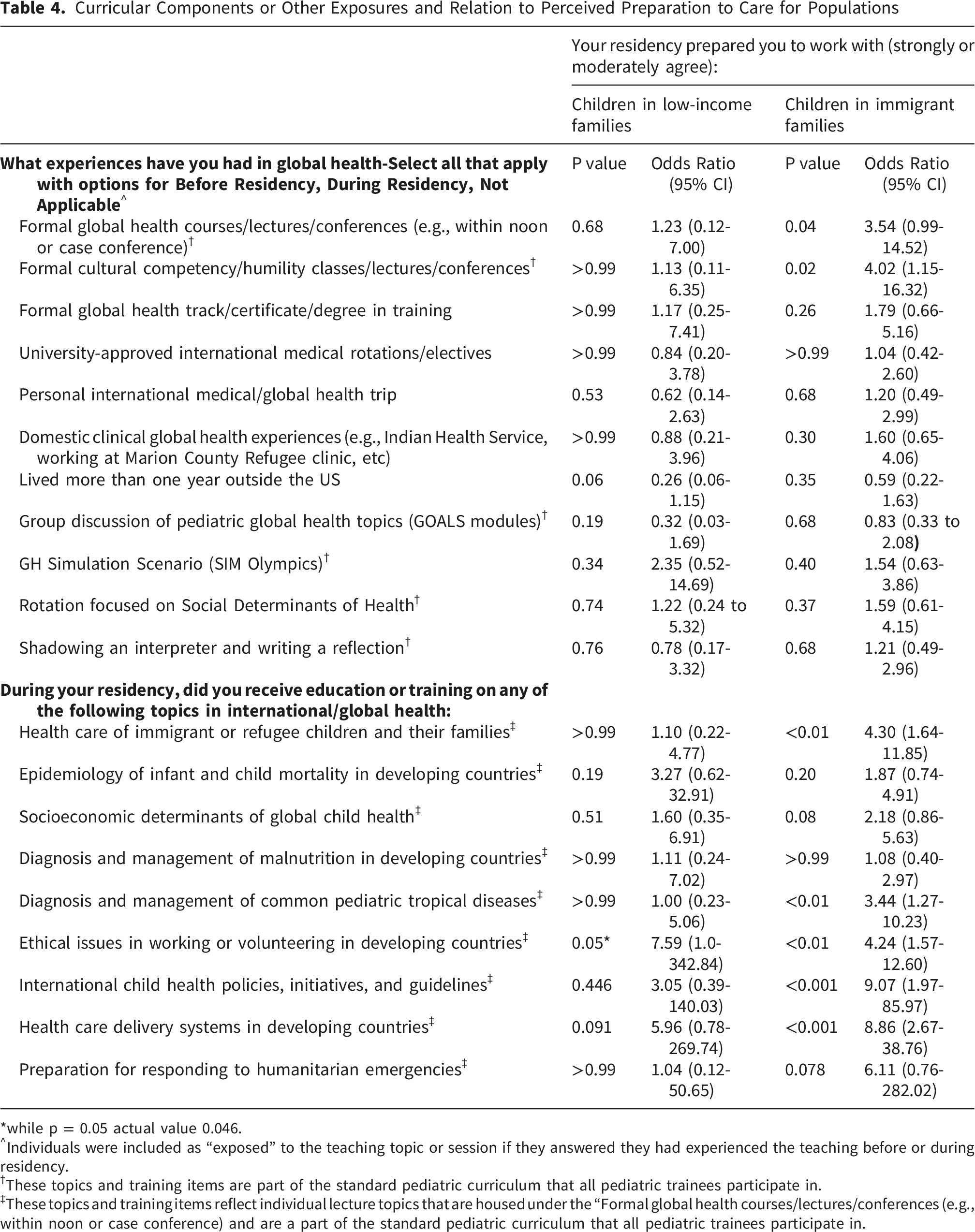
*while p = 0.05 actual value 0.046.
^Individuals were included as “exposed” to the teaching topic or session if they answered they had experienced the teaching before or during residency.
†These topics and training items are part of the standard pediatric curriculum that all pediatric trainees participate in.
‡These topics and training items reflect individual lecture topics that are housed under the “Formal global health courses/lectures/conferences (e.g., within noon or case conference) and are a part of the standard pediatric curriculum that all pediatric trainees participate in.
Self-Reported Future Plans for Clinical Practice After Residency
When asked about their career plans, 66% of residents indicated they plan to care for children in immigrant families locally, while 95% indicated plan to care for children in low-income families, and 40% of residents indicated spending time caring for an international population while working abroad. Three residents indicated that they do not plan to work for any of the three populations.
Association of Curricular Components and Future Plans for Clinical Practice
Residents were surveyed regarding their future plans for clinical practice, and associations between these future plans and exposure to global health educational training and topics were examined. For individuals planning to care for low-income and underserved communities no significant association to global health training and topics was identified.
Curricular Components or Other Exposures and Relation to Future Practice Plans
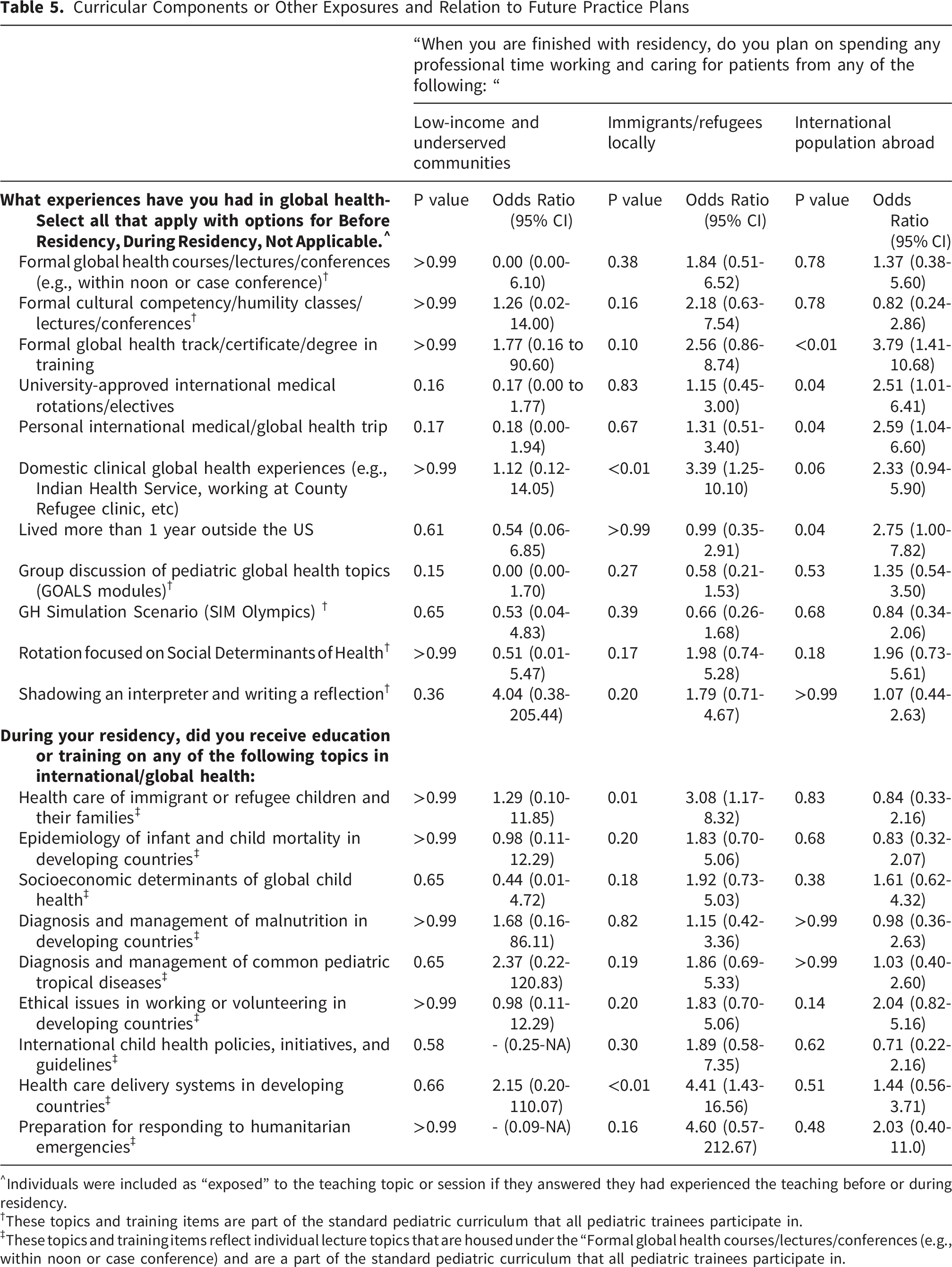
^Individuals were included as “exposed” to the teaching topic or session if they answered they had experienced the teaching before or during residency.
†These topics and training items are part of the standard pediatric curriculum that all pediatric trainees participate in.
‡These topics and training items reflect individual lecture topics that are housed under the “Formal global health courses/lectures/conferences (e.g., within noon or case conference) and are a part of the standard pediatric curriculum that all pediatric trainees participate in.
Individuals who self-reported future plans to care for international populations abroad were more likely to have lived more than one year outside the United States (OR = 2.75, 95% CI [1.00-7.82], p = 0.04) and to report exposure to global health track or certificate training (OR = 3.79, 95% CI [1.41-10.68] p < 0.01), global health electives that were either university sponsored (OR = 2.51, 95% CI [1.01-6.41], p = 0.04) or personally sponsored (OR = 2.59, 95% CI [1.04-6.60], p = 0.04) (Table 5).
Discussion
Pediatric residents in our program expressed interest in caring for and learning about children in immigrant and low-income families. More than half of the residents agreed their training prepared them to care for children in immigrant families, and nearly all reported their training prepared them to care for children in low-income families. Exposure to global health-related lectures and topics such as health care delivery systems in developing countries, care of immigrant and refugee children, cultural humility training, and international child health policies was associated with greater perceived preparedness to care for children in immigrant families.
Caring for children in immigrant families requires medical knowledge and understanding of the unique social and structural challenges these families face.13,14,25 Our results align with prior studies showing that targeted education on immigrant and refugee health improves trainees’ preparedness6,12,13 and knowledge6,26 to care for immigrant and culturally diverse populations. This study extends the existing literature by evaluating the self-perceived impact of integrating GH education into the core residency curriculum for all residents, not just individuals pursuing a designated GH track. Residents with pre-existing interest in GH may naturally seek out such content, but by embedding these topics within required coursework, our program aimed to ensure all trainees develop foundational competence and confidence in caring for immigrant and underserved populations. This approach supports the goal of preparing a pediatric workforce equipped to care for increasingly diverse communities.
We observed that residents who reported exposure to global child health and immigrant-focused training components were more likely to report that their residency prepared them to care for children in immigrant families. While our study design cannot establish causality, these associations reinforce prior work demonstrating that focused education on immigrant health improves physician preparedness.6,8,12,13,26 Importantly, by including children in low-income families as a comparison group, we identified a meaningful difference: while nearly all residents felt prepared to care for children in low-income families, fewer felt prepared to care for immigrant families. This disparity highlights an opportunity for continued curricular refinement to strengthen training around immigrant and refugee health.
Our findings also reveal important insights into the relationship between educational exposures and residents’ future career intentions. Exposure to some-though not all-curricular components was associated with residents’ reported plans to work with children in immigrant families. We also noted that when planning to care for specific groups, trainees reported more exposure to optional and elective portions of the GH education opportunities. Residents who plan to care for children in immigrant families report exposure to domestic global health experiences. For those who plan some clinical work internationally, exposures to global health pathways and international experiences such as personal or university approved global health electives were more likely reported. In planning to care for different groups the link to elective experiential training warrants further study to understand how specific curricular elements influence or are influenced by long-term professional goals.
We evaluated exposure to a range of curricular components encompassing didactic, discussion-based, and experiential learning opportunities, including shadowing interpreters, simulation sessions, and global health electives. Previous studies have shown that trainees prefer experiential learning such as direct clinical care and immersive experiences when developing culturally responsive care skills. 11 Pediatricians with international experience were more likely to report high levels of comfort in caring for children who were immigrants or refugees than those without such experience. 27 In our study, experiential opportunities, such as GH simulation sessions, a rotation focused on social determinants of health, and domestic/international global health experiences were not associated with perceived preparedness to care for immigrant or low-income populations, although several of these experiences were associated with plans to work internationally. These findings may reflect selection bias, as residents who pursue elective GH experiences often enter training with pre-existing interests and motivations related to global or underserved care. Furthermore, while experiential training is important and desired, it can be hard to ensure all trainees have equitable exposure to the clinical care of diverse patients during their residency training. Guides and curriculum components developed by the American Board of Pediatrics and the AAP exist for those hoping to integrate more global health training into their general pediatric training curricula.28,29 For our trainees, additional evaluation of the impact of specific components of GH training are needed, but our results support that didactic, discussion, and case-based training may help augment clinical exposures and other experiential learning during graduate training.
Limitations
As a single center, exploratory evaluation conducted as a cross-sectional survey, findings are subject to recall bias both for curricular exposures and self-perceived preparedness, and questions related to future career plans may or may not be actualized after resident graduation. When asking residents their agreement with the statement “your residency prepared you to work with immigrant/refugee populations” we did not define “prepared,” which limits reproducibility and generalizability. Furthermore, single survey items may not fully capture the complexity of clinical preparedness. The vast majority of residents self-reported feeling prepared, which may result in a ceiling effect limiting the ability to detect meaningful differences in the preparedness outcomes. The cross-sectional exploratory nature of the survey did not include follow up with further GH training, and a small sample size without a prior sample size calculation limits statistical power and results in wide confidence intervals for many comparisons. Bivariate analyses were used, so potential confounders were not adjusted for, and a formal statistical correction was not completed.
Additionally, because this study was conducted during the Covid-19 pandemic, trainees’ perception of international work may have shifted in response to travel restrictions and risks, with changing worldwide GH priorities. As a single-institution survey, our findings may reflect local context or self-selection bias as residents drawn to our program, which has access to a long-standing international partnership for GH electives and a GH pathway, may already have higher interest in and prior exposure to GH, immigrant health and the care of underserved populations and be more willing to complete the survey. This can also limit generalizability. Our survey is an exploratory study aimed to gather data about our trainees’ interest and experiences with GH and GH training. In line with this, our survey was pilot tested, but not validated, nor was a sensitivity analysis completed on the data. Despite these limitations this study contributes to the literature by evaluating the perceived impact of GH curricular components among all pediatric residents, not just those enrolled in GH tracks. Future research should longitudinally examine the impact of individual curricular components on objective measures of cultural competence and preparedness as curricula and needs evolve.
Conclusion
As the number of children in immigrant families and low-income families rises,1,2,4,5 graduate medical education must prepare trainees to delivery equitable care for all populations. Caring for culturally and socially diverse populations requires both knowledge and experience. While prior studies have shown that GH training benefits self-selected participants, our study demonstrates that integrating global health, immigrant and refugee health, and cultural humility content into core residency education for all trainees is associated with greater perceived preparedness to care for immigrant families. Pediatric residency programs should continue to evaluate and refine curricular components to ensure that every trainee graduates prepared to provide compassionate, culturally responsive, and effective care to immigrant, refugee, and low-income populations.
Supplemental Material
Supplemental Material - Caring for children in immigrant families and children in low-income families: a cross-sectional survey of pediatric residents
Supplemental Material for Caring for children in immigrant families and children in low-income families: a cross-sectional survey of pediatric residents by Palka R. Patel, Mitali Thanawala, Feenalie Patel, Christina Knight, Jocelyn Mineo, Shaina M. Hecht, Scott L. Coven and Megan S. McHenry in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Caring for children in immigrant families and children in low-income families: a cross-sectional survey of pediatric residents
Supplemental Material for Caring for children in immigrant families and children in low-income families: a cross-sectional survey of pediatric residents by Palka R. Patel, Mitali Thanawala, Feenalie Patel, Christina Knight, Jocelyn Mineo, Shaina M. Hecht, Scott L. Coven and Megan S. McHenry in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Caring for children in immigrant families and children in low-income families: a cross-sectional survey of pediatric residents
Supplemental Material for Caring for children in immigrant families and children in low-income families: a cross-sectional survey of pediatric residents by Palka R. Patel, Mitali Thanawala, Feenalie Patel, Christina Knight, Jocelyn Mineo, Shaina M. Hecht, Scott L. Coven and Megan S. McHenry in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgements
The authors wish to thank the Indiana University School of Medicine pediatric residents who participated in the survey. We would like to thank and give acknowledgement to Dr. Bobbi Byrne who helped review the curriculum and study design, JangDong Seo who contributed to early statistical analysis, Addison Montroy who contributed majorly to revisions in the statistical analysis, and to Melissa Thomas for her review and editing.
Ethical Considerations
This study was deemed exempt by the IRB at Indiana University (IRB# 10479).
Consent to Participate
This study was deemed exempt by the IRB at Indiana University (IRB# 10479). Prior to initiating the electronic survey a participant agreement statement was utilized to obtain written voluntary informed consent from participants.
Author Contributions
MT, FP, CK, SLC, SMH, and MSM conceptualized the needs assessment. SLC and MSM provided guidance to survey design. MT, FP, CK, SLC, and SMH administered the survey and reviewed initial results. JM conducted statistical analysis. PRP was a major contributor in writing the manuscript, with MSM and SMH reviewing and providing feedback. All authors read and approved of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through internal research funds from Dr. Megan S. McHenry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset analyzed during the current study is available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.