
Abstract
Background
Longitudinal clinical experiences (LCEs) represent a broad curricular approach in medical education that emphasizes continuity of care and relationship-building with patients and healthcare teams. In contrast to traditional block-based rotations, LCEs allow students to participate in patient care across time and may include outpatient clinics, patient-following models, and longitudinal integrated clerkships (LICs). LICs represent one well-established model within the broader LCE framework, typically involving simultaneous participation across multiple specialties over months. Given the growing use and variability of longitudinal models in undergraduate medical education, this study aimed to assess the current landscape of LCE implementation, including LICs, across United States medical schools.
Methods
We conducted a comprehensive survey of all accredited allopathic medical schools in the U.S., examining their curricula with a focus on LCEs including LIC implementation. Data was collected on the prevalence of longitudinal clinical programs, types of models used, and average length of programs.
Results
Approximately 64% of medical schools offer some form of LCE. The majority of these programs were mandatory for students (80%), while the rest were offered as an elective option. The programs ranged from being incorporated in exclusively preclinical years, exclusively clinical years, or both. The average length of a longitudinal program was identified to be 24 months. One-third of programs implemented a traditional LIC system, while the rest incorporated longitudinal clinical experiences through a clinic attachment, a patient attachment, or some combination of the two.
Conclusion
There is a trend towards increased adoption and diversification of longitudinal clinical education with LIC models and other LCEs in U.S. medical schools. When compared to a previous analysis, schools are integrating LCEs earlier. This shift reflects growing recognition of the benefits of longitudinal experiences in medical education. Future research should focus on long-term outcomes of longitudinal programs, strategies for overcoming implementation challenges, and standardization.
Keywords
Introduction
Longitudinal clinical experiences (LCEs) represent a broad curricular approach in medical education that emphasizes sustained clinical engagement, continuity of care, and relationship-building with patients and healthcare teams over time. LCEs have been an evolving product of the medical education system since its development over the past 100 years as an alternative to traditional block-based education. 1 Rather than organizing clinical learning exclusively through short, discipline-specific blocks, LCEs allow students to participate in patient care across extended periods and in a variety of clinical settings. These experiences may include longitudinal outpatient clinics, patient-following models, specialty-specific tracks, continuity-based preclinical experiences, or more comprehensive longitudinal integrated clerkships (LICs). Longitudinal clinical experiences have been associated with improved continuity of care exposure, enhanced clinical confidence, and stronger professional identity formation among medical trainees.2,3 Among these experiences, the LIC curriculum represents a widely adopted structure that focuses on integrating multiple specialties of medical care over a more continuous timeline.
The traditional medical school curriculum adopted by most medical schools today has its roots dating back to the early 20th century. 4 As medicine evolved into various specialties each with its own board certification, the block rotation curriculum was born. The concept focused on building upon two years of preclinical textbook coursework by spending 4–8 weeks in each specialty for a year as a third-year medical student. This model provides structured exposure to core disciplines and remains widely used. However, critics have noted that short, specialty-specific blocks may limit continuity with patients, supervisors, and clinical teams. 5 In response, many medical schools have incorporated longitudinal models to better integrate clinical learning across time, specialties, and care settings.
Within the broader LCE framework, longitudinal integrated clerkships represent one of the most established and clearly defined models. LICs typically involve students participating in multiple specialties simultaneously over several months, often with repeated engagement with the same patients, preceptors, and clinical environments.6-10 These programs may be mandatory or elective and have been implemented across rural, community, and urban settings, demonstrating adaptability to different institutional and healthcare contexts. By emphasizing sustained engagement, LICs seek to promote continuity-based clinical competencies, integrated clinical reasoning, and patient-centered care. 11
Although LICs are an important example of longitudinal clinical education, many schools implement LCEs that do not meet the full structure of an LIC. These may include weekly outpatient continuity clinics during preclinical coursework, longitudinal patient panels, early clinical immersion experiences, or longitudinal tracks layered onto traditional block rotations. Some curriculum models introduce students to direct patient care early in medical school, reflecting a broader shift toward earlier and more continuous clinical exposure. 12 This transition has also occurred alongside other curricular reforms, including problem-based learning and integrated approaches to clinical education.13,14 As a result, LCEs may vary substantially in timing, duration, specialty integration, required participation, and curricular structure.
Longitudinal models may offer several educational benefits, including stronger relationships with clinical supervisors, improved interprofessional learning, and greater opportunities for patient advocacy. Interprofessional cooperation has been linked to improved patient outcomes, and longitudinal clinical models may help students develop more meaningful relationships with members of the healthcare team.15-18 These experiences allow students to follow patients across encounters, clarify complex medical information, and participate more actively in care coordination. 19 However, LCE implementation can also present logistical challenges, including scheduling across clinical sites, coordinating longitudinal supervision, and balancing continuity experiences with existing curricular requirements. 20
Given the growing use and variability of longitudinal models in undergraduate medical education, this study aimed to explore the current landscape of LCE implementation across medical schools in the United States. Specifically, we sought to characterize the extent of LCE adoption, describe common curricular structures, and identify national trends in longitudinal clinical programming. In this analysis, LCEs were examined broadly, with LICs considered one subset within the larger category of longitudinal educational models.
Methods
Study Design
This study utilized a descriptive, cross-sectional design to evaluate the presence of longitudinal clinical experiences (including LICs) across all allopathic medical schools in the United States. The dataset was compiled through the collection of publicly available information. Sources included medical school websites, program descriptions, online brochures, and published literature. The study aimed to identify the prevalence of Longitudinal programs, their structure, duration, goals, and key features. For this review, an LIC was operationally defined as a clinical curriculum in which students participate in multiple rotations simultaneously over an extended period, while mastering required clinical competencies. Longitudinal clinical experiences were defined as curricular opportunities where students participate in the comprehensive care of patients over time or develop continuing relationships with patients and preceptors. These LCEs include preclinical continuity clinics, patient-panel assignments without integrated multi-discipline clerkship requirements, and were reported separately from LICs.
Search Strategy
A comprehensive search was conducted from September 1, 2024 to November 1, 2024 to identify all accredited allopathic medical schools in the U.S. This was primarily completed using the Association of American Medical Colleges (AAMC) database. For each school, official websites were reviewed to identify information related to their specific curriculum and program features. Those with LIC programs or similar LCE training models were documented accordingly.
Inclusion & Exclusion Criteria
All accredited allopathic medical schools in the United States listed at the time of the search were eligible for screening. Schools were included at the institutional level if they were U.S.-based, Liaison Committee on Medical Education (LCME)-accredited allopathic medical schools with publicly available curriculum information accessible through official school or program sources. Osteopathic medical schools, international medical schools, and non-accredited institutions were excluded.
At the program level, curricular models were included in the detailed analysis if publicly available information indicated the presence of either: (1) a longitudinal integrated clerkship, defined as a longitudinal clinical curriculum in which students participate in multiple disciplines simultaneously over an extended period while meeting core clinical competencies or (2) a longitudinal clinical experience, defined as a longitudinal patient care and/or preceptor continuity experience that did not fully meet LIC criteria. Programs were excluded from detailed program-level analyses if no longitudinal component was identified, if the available description was insufficient to determine whether the experience met LIC or LCE criteria, or if the experience was clearly a traditional block rotation without a longitudinal continuity component. Schools without identifiable LIC or LCE offerings were retained in the institutional prevalence analysis but were not included in analyses of program structure or duration.
Data Extraction
Data were extracted by five independent reviewers using a standardized Excel sheet. Institution name, location, accreditation status, and initial year of accreditation were collected. Each program was assessed for the presence of a longitudinal clinical program (LIC or LCE). This data was stratified into three categories: 0 longitudinal clinical programs, 1 longitudinal clinical program, or 2+ longitudinal clinical programs. If applicable, the name of the LIC program was documented. Programs were determined to have an LIC if they had a curriculum aspect that met Worley’s comprehensive LIC definition of a long-term program covering multiple specialties simultaneously. 10
Programs meeting LCE criteria (longitudinal patient or faculty experiences), or those meeting Worley’s definition of amalgamative or small-scale LIC curricula were categorized separately. Those with an LIC or LCE available were further evaluated. Information on the participation requirement (mandatory vs. elective) of the program was identified. The specific structure of program was documented as it fit into one of three categories: Traditional LIC, Clinic Attachment Only, or Patient and Clinic Attachment. The length of the program and if it existed in preclinical years, clinical years, or both was recorded. Finally, the presence or absence of longitudinal program goals on the institutions’ websites were documented. Discrepancies between reviewers were resolved through discussion and consensus. Consensus was reached through repeat review of the original publicly available institutional materials to ensure that final classifications reflected the most accurate interpretation of the source data. Institutions were not contacted directly, as the study was designed to assess LIC program characteristics based on information available in the public domain using a standardized and reproducible methodology.
Analysis
Descriptive statistics were used to analyze and summarize the data. Specific datapoints explored included the proportion of schools with longitudinal clinical programs, the average length of programs, and the type of LIC or LCE model implemented. Results were displayed in graphic and narrative formats to allow for an accessible and comprehensive descriptive overview.
Results
Program Qualities
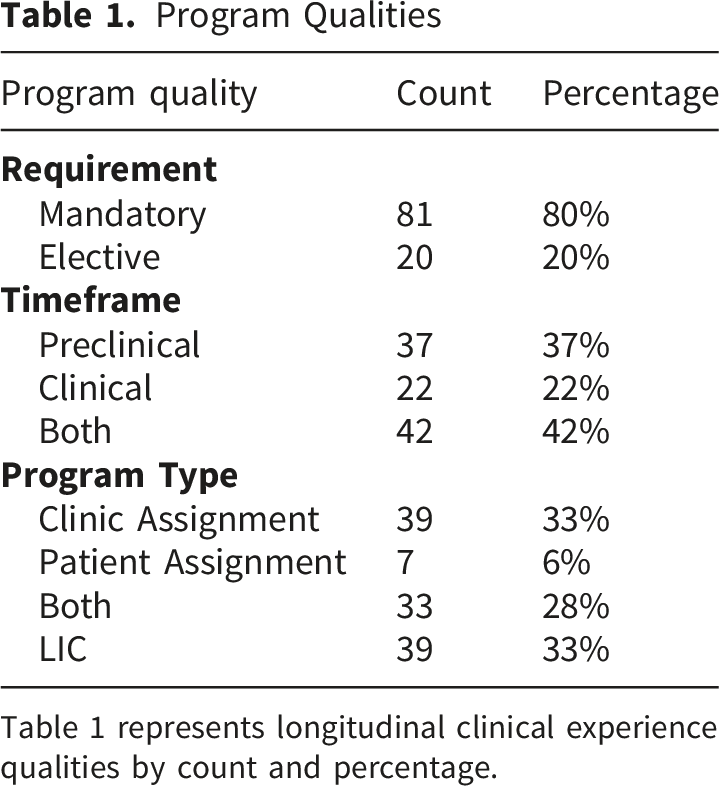
Table 1 represents longitudinal clinical experience qualities by count and percentage.
A little over one-third (37%) of programs implemented a longitudinal clinical experience in the preclinical years (typically the first and second years of medical school). Approximately 22% had LIC/LCE options in clinical years (typically the third and fourth years of medical school). While 42% had structured longitudinal opportunities throughout both the preclinical and clinical years (Table 1). A traditional LIC model refers to continuous clinical experiences where students work with different specialties throughout each week. Alternative LCE model refers to those with an elective LCE curriculum or clinical assignments in their first/second years of medical school. For example, a few programs offer specific tracks, often in primary care, that incorporate longitudinal patient care experiences. When exploring the type of program available at each institution, one-third had a clinic assignment option. This was typically structured as one session every other week with a local primary care clinic. Only 6% of programs had students assigned to a specific patient as the extent of their longitudinal patient care experience. Thirty-three (28%) had both a clinic and a patient assignment. Finally, 39 (33%) programs evaluated had incorporated the traditional Longitudinal Integrated Clerkship curriculum (Table 1).
With regards to length of these programs, the average length was 24months, and the median length was 18 months. The program lengths ranged from 2 to 48 months long (Figure 1). Six of the programs ranged were 6 months or less (6, 6%). Thirty institutions had a program that ranged from 6 months to 1 year (30%). Fourteen ranged from 12 to 18 months (14%). Fourteen ranged from 18 to 24 months (14%). One ranged from 24 to 30 months (1, 1%). Eleven ranged from 30 to 36 months (11%). Twenty-four ranged from 42 to 48 months (24%). Number of programs by average length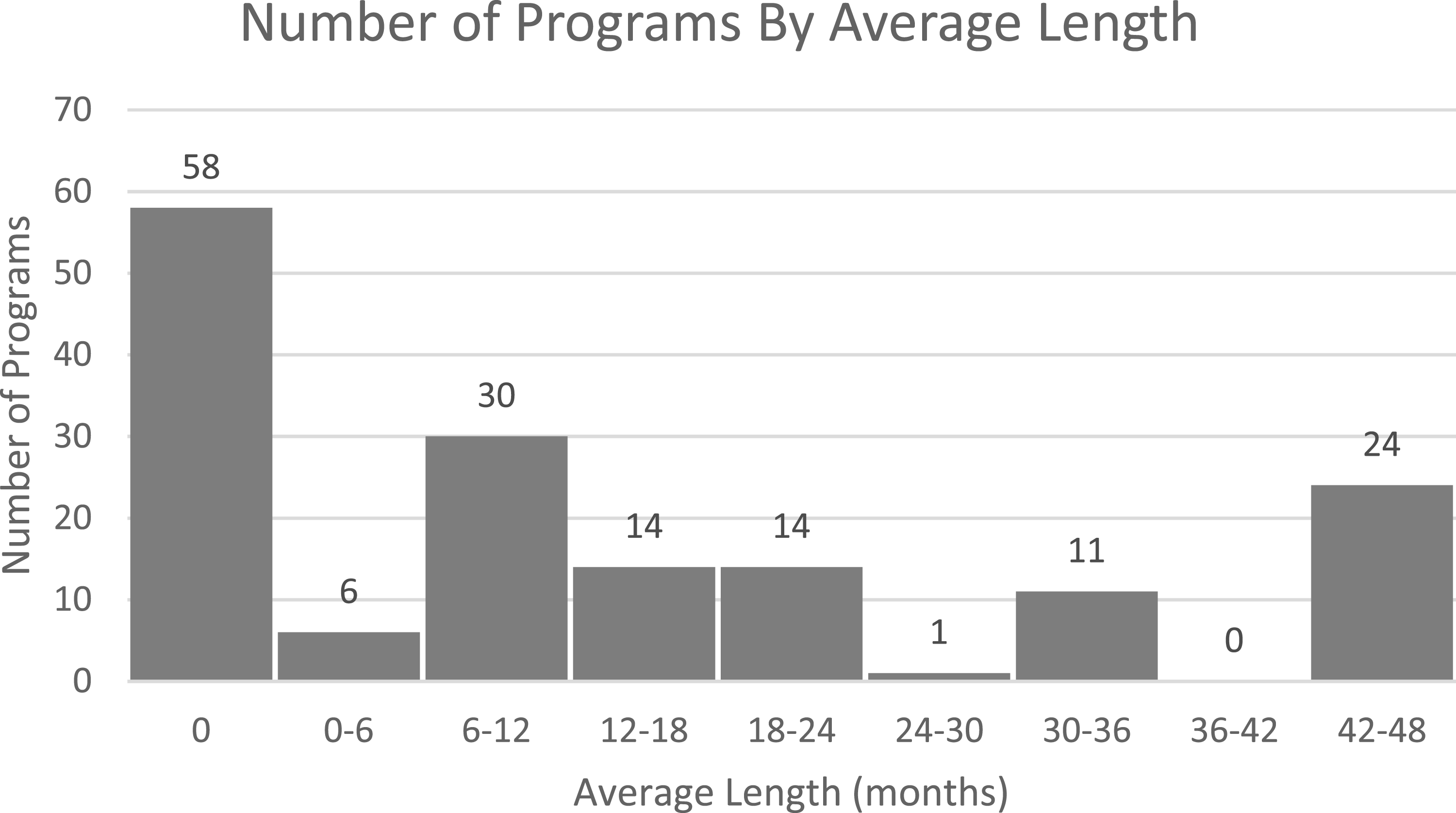
Discussion
The findings of this study reveal that longitudinal clinical experiences are increasingly being adopted across allopathic medical schools in the United States, with 101 institutions offering some form of LIC or LCE. A previous review identified 69 allopathic medical schools offering longitudinal clinical programs as of August 2014, whereas the present study identified 101 schools offering longitudinal clinical experiences, representing a notable increase in institutional adoption over time. 21 It is important to note that since August of 2014 to November 2024, there was an increase from 137 to 158 U.S. allopathic medical schools. However, there was still a 14% increase in the proportion of medical schools utilizing a longitudinal clinical curriculum over this time period (50% vs 64%). Although the number of longitudinal programs increased compared to prior reports, it remains unclear whether this growth is driven primarily by expansion of traditional LICs or by broader adoption of alternative longitudinal clinical models. There has been a substantial increase in the number of allopathic medical schools implementing some form of longitudinal clinical experience for medical students in the past seven years.
These programs vary significantly in structure, with some schools integrating longitudinal clinical experiences into the first two years of medical education, others in the final two years, and some spanning the entire four years. Additionally, some are mandatory, while others are offered as an elective. The models of longitudinal clinical programs range from emphasizing patient or clinic attachments, to the traditional LIC structure. This diversity reflects the adaptability of the longitudinal model to different institutional goals.
The variability in longitudinal curriculum implementation identified in this study highlights the flexibility of the model to meet the needs of different institutions and student populations. For example, programs that integrate LCEs into the first two years of medical school may provide students with early exposure to clinical practice and thus reinforce basic science learning through connecting theory to practice. Conversely, programs that focus on the final two years may allow students to consolidate their clinical skills and prepare for board exams and residency in a more immersive and realistic environment. 9
Despite its many benefits, the LIC model is not without challenges. Implementing LICs and LCEs requires significant institutional commitment, including the allocation of resources for faculty development, curriculum design, and administrative support. 22 Additionally, the success of LICs/LCEs depends on the availability of clinical sites and preceptors who are willing to engage in longitudinal teaching relationships. 23 These challenges may explain why some institutions offer these longitudinal experiences as elective rather than mandatory programs.
Limitations
The reliance on publicly available information and self-reported data from institutions could introduce inaccuracies, particularly for programs that are newly established or undergoing changes. This approach is also vulnerable to information bias from incomplete, outdated, or inconsistently reported website content, as well as publication/visibility bias in which schools with well-established or highly promoted longitudinal curricula may be more likely to feature programs prominently online. Because program details were derived from web-based sources, some LIC/LCEs may have been misclassified or missed entirely if descriptions were limited, archived, or not publicly accessible. In addition, the absence of primary-source validation (direct confirmation with curriculum deans or LIC program directors) limits our ability to verify program status (active/inactive), structure, and whether experiences are mandatory versus elective. Although direct institutional outreach might have clarified select discrepancies, we did not pursue program-by-program confirmation because response rates and the level of detail provided would likely vary across schools, introducing differential ascertainment and reducing the standardization and reproducibility of the data collection process. As a result, classifications were based uniformly on publicly available sources, which may not fully capture internal curricular details or recent programmatic changes. Additionally, the study does not explore the quality or outcomes of these specific LIC/LCE programs, such as student satisfaction, clinical performance, or long-term career impacts, which limits the ability to draw conclusions about the effectiveness of different longitudinal models. The study focuses exclusively on allopathic medical schools, excluding osteopathic and international institutions, which may limit the generalizability of the findings. In particular, the exclusion of osteopathic (DO-granting) schools likely yields an incomplete picture of longitudinal clinical training nationally and may underestimate the prevalence and diversity of longitudinal models in the U.S. These limitations highlight the need for further research, including qualitative studies and longitudinal assessments, to provide a more comprehensive understanding of LIC programs in the U.S.
Conclusion
The growing adoption of longitudinal clinical curricula in allopathic medical schools in the United States reflects the recognition of its potential to enhance medical education. The variability in implementation observed in this study underscores the adaptability of the LIC model to different institutional contexts and educational goals. By providing students with opportunities for continuity of care, authentic clinical experiences, and strong mentoring relationships, LICs and LCEs can play a critical role in preparing future physicians to meet the complex demands of modern healthcare. Future research should explore the long-term outcomes of LIC graduates, including their performance in residency and their ability to provide patient-centered, value-basedcare.
Footnotes
Authors’ Contributions
AE, AS, CB, JM, and WS performed data collection from medical school curriculum websites, analyzed the data, constructed figures, and were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data used and analyzed in this study is publicly available.