
Abstract
Background
Clinical reasoning is a complex process that plays a crucial role in order to solve the patients’ problems. Our aim was to compare AI competences to the physicians’ competences in clinical reasoning.
Methods
We performed a meta-analysis under the guidelines of the AMSTAR (version 2). All eligible articles were retrieved from Pubmed, Embase and Cochrane databases. The articles included were rated according to the MMERSQI scores. Binary diagnostic accuracy was used as the primary outcome. Continuous performance scores were considered as secondary outcome in order to avoid excluding studies using continuous scores instead of concordance rates. The Review Manager software 5.4 (free version) was used to conduct this meta-analysis. The OR with the 95% CI were calculated for studies reporting binary accuracy. The SMD with the 95% CI were calculated for studies using continuous scores. Q test and I2 statistics were carried out to explore the heterogeneity among studies. P value <0.1 for q test or I2 value >50% represented substantial between study heterogeneity. A random-effects model was used. Subgroup analyses were performed to explore the potential sources of heterogeneity if necessary. Publication bias was assessed using the funnel plot analysis.
Results
Considering the studies using binary scores and comparing odds ratios, 1609 clinical vignettes were used to compare the different LLM to the human clinical reasoning. The combined OR reached 0.65 with 95% CI [0.38, 1.12]. No significant difference between both groups was observed (p=0.12). When considering studies using continuous scoring systems, the combined standard mean difference reached 0.08 with 95% CI [-0.19, 0.35]. No significant difference between both groups was observed. In order to explain the heterogeneity that was noticed, we performed a sub-group analysis taking into account the nature of the clinical cases (real-world or published), the LLM system used (Chat-GPT v4) and the expertise of the respondants (novices or experts). The heterogeneity was observed in all subgroups excluding the subgroup of the studies using binary scoring systems and comparing LLM’s scores to novices’ scores. The combined OR reached 0.62 with 95% CI [0.35, 1.1]. No significant difference was observed between both groups (p=0.1) and the heterogeneity I-square was evaluated to 0% and Tau2 to 0.00.
Conclusion
Even if this meta-analysis showed the absence of difference between AI and human clinical reasoning, these reaults have to be taken with caution because of the important heterogeneity that wasn’t resolved by subgroup analyses.
Introduction
Artificial intelligence (AI) has modified the medical practice. Earlier technology innovations extended physicians’ senses without altering how they think. AI acts directly on the cognition process itself. Generative artificial intelligence technologies can mimic human cognition. They can improve clinicians’ and students’ performance of some tasks. AI has been reported in many fields and specialties including radiology, pathology, urology, etc….1-5 In the field of medical practice, AI use has been reported as a useful tool of medical learning and medical teaching. In medical learning, AI use has been reported in medical research, medical writing, self-learning follow-up, understanding and creating concepts. In medical teaching, it has been reported as a useful tool for creating vignettes, virtual patients, multiple clinical questions, for history taking teaching.6-9 Clinical reasoning is a complex process implicating 2 systems: a rapid and intuitive system, mostly used by experts, and a hypothetico-deductive-based system mainly used by novices and used by experts to correct the intuitive system errors.10-14 Clinical reasoning is based on different steps: information gathering, hypothesis testing, differential diagnosis management and diagnostic refinement based on emerging evidence. Practicing clinical reasoning is also based on using the Bayesian theory calculating the probability of a particular disease per evidence.
AI has been used to solve health problems and for clinical results with discordant reports. Some authors reported that AI outperformed the human clinical reasoning competences.15-18 Other authors reported that AI was inferior to physicians in the domain of clinical reasoning.19-21 On the other hand, some authors reported that AI can improve human competences without outperforming them.8,9,22-25
Our aim was to compare the AI clinical reasoning competences to the physicians’ clinical reasoning competences based on a systematic review of the literature with a meta-analysis.
Methods
Data Source and Search
This meta-analysis was conducted under the guidelines of the AMSTAR (Version 2). 26 To retrieve all eligible articles, PubMed, Embase databases and Cochrane Library were comprehensively searched with limitation to French and English language. The search medical subject heading (MeSH) terms employed for literature retrieval included: Comparison of artificial intelligence OR generative artificial intelligence OR Artificial intelligence agents OR artificial intelligence multi-agents AND clinical reasoning in medical education. The reference list of eligible articles was also independently searched by 2 authors (MM, MZ) to obtain other valuable sources. According to inclusion criteria, titles and abstracts of all retrieved publications were screened and judged by the 2 same authors.
Study Selection Criteria
To be qualified for inclusion in this meta-analysis, articles must comply with all the following criteria: The articles were original articles consisting of cohort studies or case control studies, articles compared the AI-based clinical reasoning to human-based clinical reasoning. This comparison has to be based on the results of human experts’ results. The major exclusion criteria were as follow: qualitative studies, studies without a comparison to the expert reference test, technical reports, studies with no case reports, published protocols, comments or letters with invalid data. Studies with insufficient data or without data enabling to calculate the Odds ratios or the standard means were excluded. Studies with duplicate data reported in other studies and reviews weren’t included.
Data Extraction and Quality Assessment
Two investigators independently reviewed all the articles and extracted data from the selected articles: first authors’ name, publication year, scoring methods of the clinical reasoning competences (binary or continuous), number of the vignettes (cases) studied, characteristics of the vignettes (real-world vignettes, published cases, created cases), number of doctors, qualifications of the doctors included (experts, residents, specialties). Experts are defined as qualified medical specialists or general practitioners (GPs) who have completed their formal education, training, and certification, and are no longer in a training period. Novices were defined as students in training and still tutored. Any disagreements were solved by discussion and consensus between the 2 reviewers.
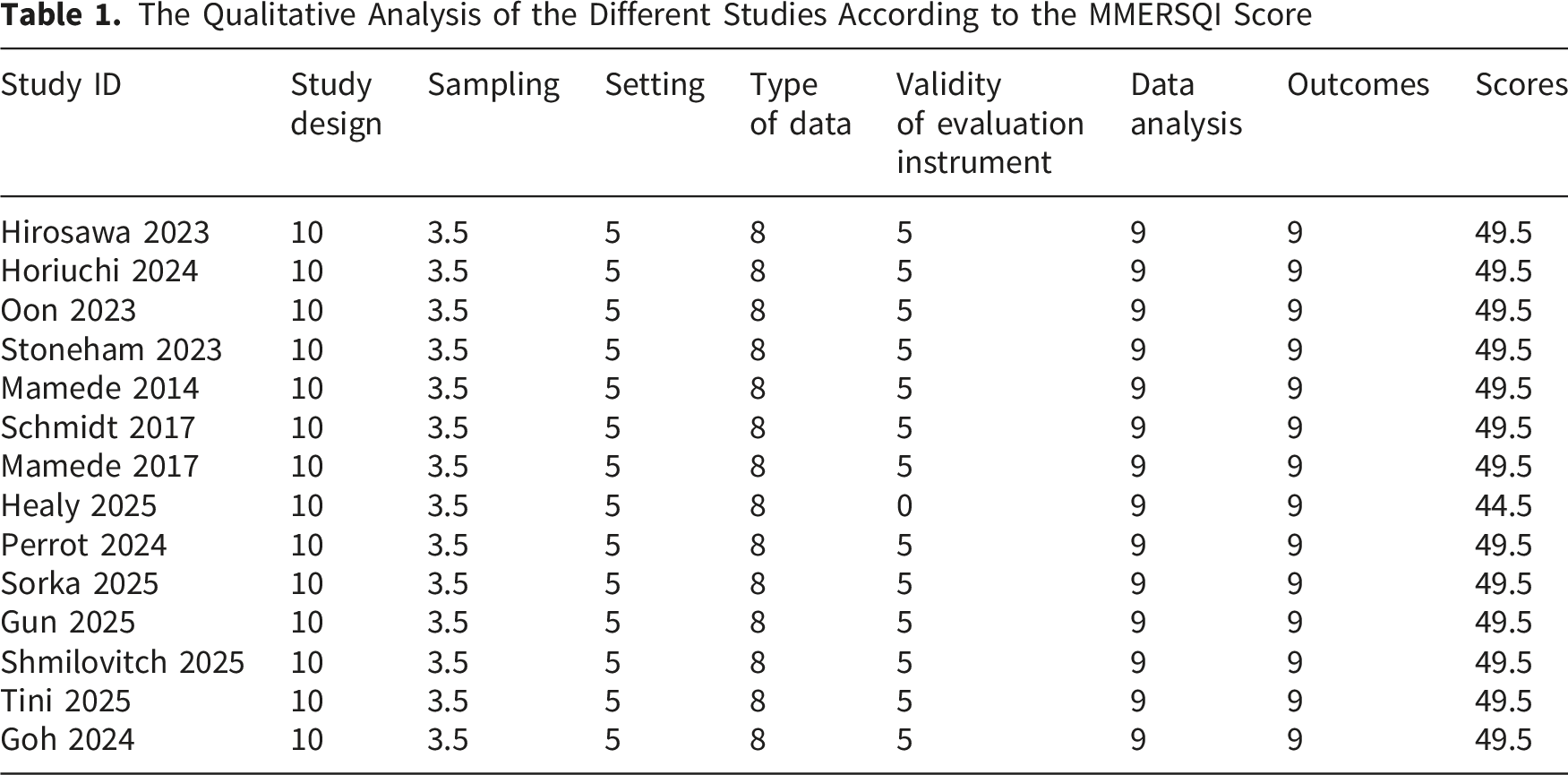
The articles included were rated according to the Modified Medical Education Research Study Quality Instrument (MMERSQI) scores. 27 The scoring criteria consisted of 6 items: the study design, the sampling, the setting, the data type, the validity of the evaluation instrument, the data analysis and the outcomes. The scores ranged between 23.5 (min) and 100 (max).
Outcomes
Binary diagnostic accuracy was used as the primary outcome. Continuous performance scores were considered as secondary outcome in order to avoid excluding studies publishing continuous scores. This methodological choice was justified to avoid ruling out potential important articles dealing with continuous scoring systems.
Statistical Analysis
We used the Review Manager software 5.4 (free version) to conduct this meta-analysis. The odds ratio with the 95% confidence intervals were calculated for studies reporting binary accuracy. Studies publishing continuous scores weren’t excluded. The standard mean differences with the 95% confidence intervals were calculated. When standard mean differences weren’t directly reported, Hedges g was calculated from available summary statistics or derived from confidence intervals, standard errors or test statistics. Continuous performance scores were considered as secondary outcome. Using Odds Ratio (OR) for binary data was considered more appropriate when dealing with studies comparing concordance rate between human clinical reasoning and AI clinical reasoning. On the other hand, Standardized Mean Difference (SMD) was more appropriate to for studies using a continuous scoring system.
The number of clinical cases or vignettes was used instead of the number of evaluators. Even if LLM represent a single system, their performance was assessed across multiple cases or vignettes. - Heterogeneity assessment: Q test and I2 statistics were carried out to explore the heterogeneity among studies. P value <0.1 for q test or I2 value >50% represented substantial between study heterogeneity. A random-effects model was used. Subgroup analyses were performed to explore the potential sources of heterogeneity if necessary. - Publication bias: Publication bias was assessed using the funnel plot analysis. - The reporting of this study conforms to the PRISMA 2020 statement
28
- PROSPERO registration record: 1276673 - Conflict of interest: No conflict of interest was reported by the authors - Funding sources: No funding sources were reported by the authors
Results
Search Results
We retrieved 150 records. For example, the MESH search using this equation: (“comparison”[All Fields] OR “comparisons”[All Fields]) AND (“human s”[All Fields] OR “humans”[MeSH Terms] OR “humans”[All Fields] OR “human”[All Fields]) AND (“clinical reasoning”[MeSH Terms] OR (“clinical”[All Fields] AND “reasoning”[All Fields]) OR “clinical reasoning”[All Fields]) AND ((“artificial intelligence”[MeSH Terms] OR (“artificial”[All Fields] AND “intelligence”[All Fields]) OR “artificial intelligence”[All Fields]) AND (“clinical reasoning”[MeSH Terms] OR (“clinical”[All Fields] AND “reasoning”[All Fields]) OR “clinical reasoning”[All Fields])) on pubmed highlighted 74 records. This strategy was also used when using the other databases. After reviewing the titles and abstracts, 9 records were excluded due to language limit and unrelated studies. By reviewing full-text articles, we excluded further 127 records, leaving 14 eligible articles. Figure 1 represents the flowchart of the literature review. The flow chart showing the search strategy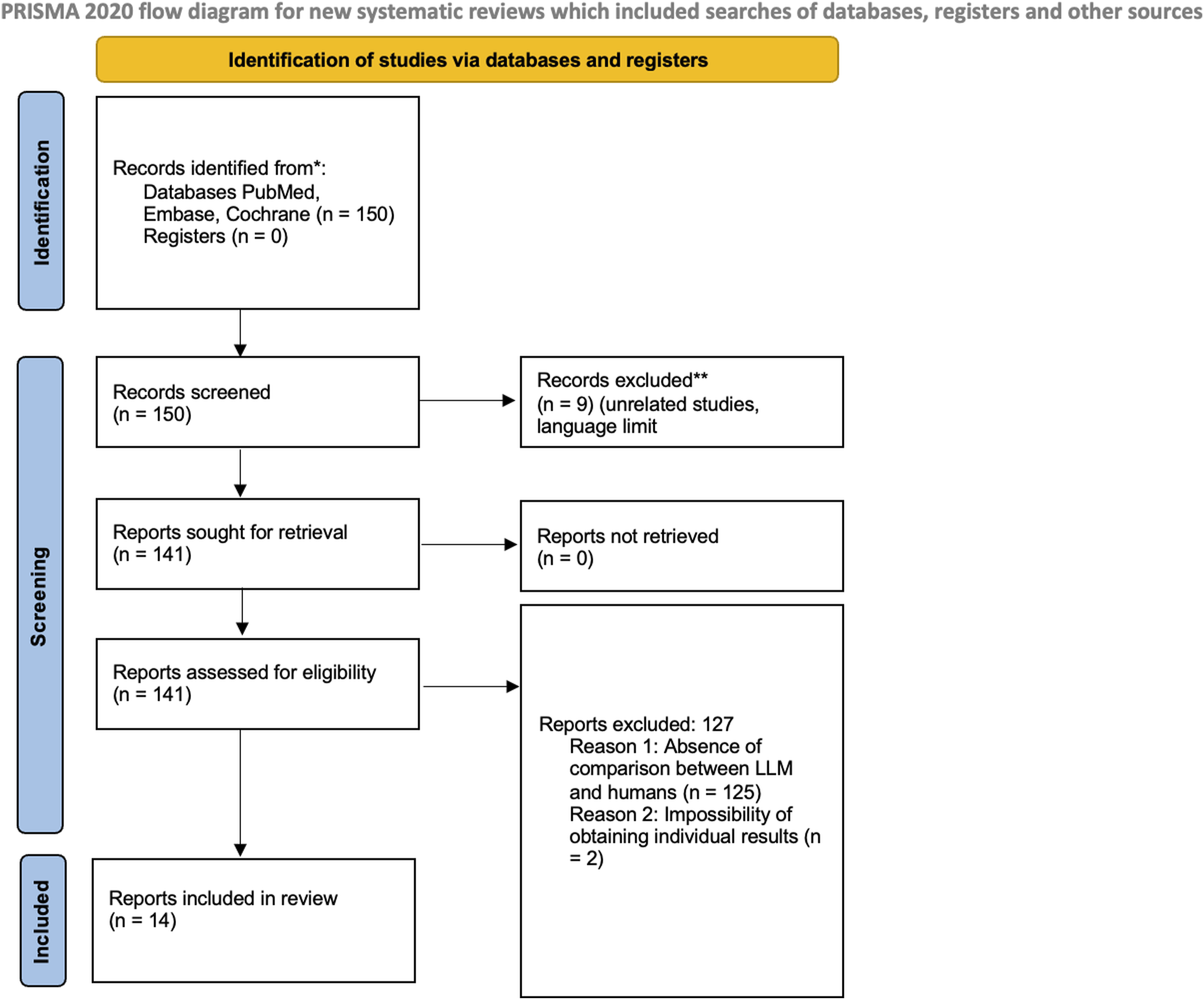
Qualitative Assessment Results
The Qualitative Analysis of the Different Studies According to the MMERSQI Score
Descriptive Results
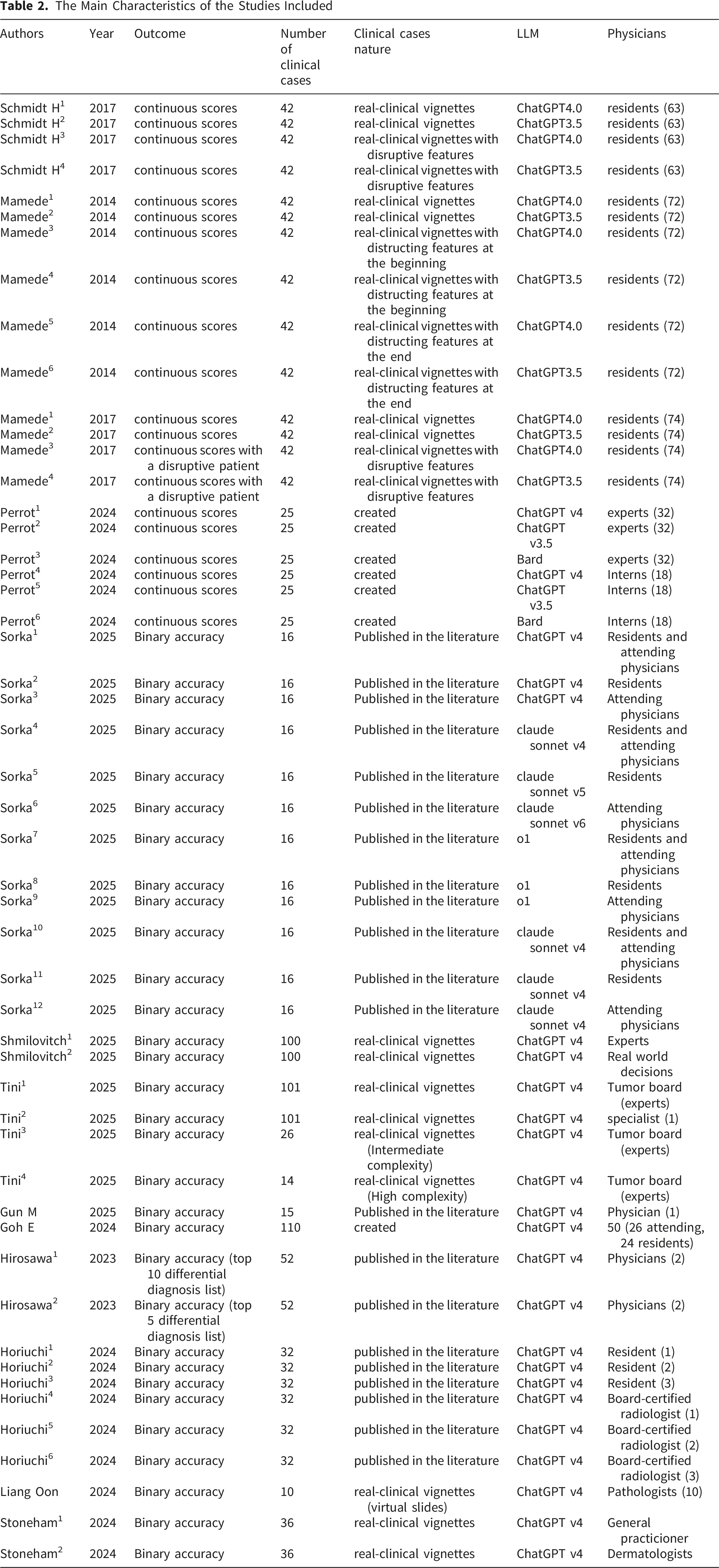
Five articles reported continuous scoring and 9 articles described binary scoring system.20-22,29-35 Among the articles using continuous scores, the article published by Schmidt, et al (2017) was considered as 4 studies. 36 This was due to the fact that the authors compared the human clinical reasoning among residents to 2 LLM systems (chatGPT V4 and chatGPT V 3.5). Besides, the authors included cases with disruptive features.
The manuscript of Mamede et al (2014) was considered as 6 studies. 37 The authors compared the human clinical reasoning among residents to 2 LLM systems (chatGPT V4 and chatGPT V 3.5). Besides, the authors included cases with disruptive features at different times of the process: at the beginning and at the end. The article of Mamede et al. (2017) was considered as 4 studies. 38 This was due to the fact that the authors compared the human clinical reasoning among residents to 2 LLM systems (chatGPT V4 and chatGPT V 3.5). Besides, the authors included cases with disruptive features. The manuscript of Perrot and coworkers was considered as 6 studies. 29 The authors used 3 different LLM (ChatGPT V4, V3.5, Bard) and they compared experts’scores and interns’ scores to the LLM’s scores.
Nine manuscripts used a binary method of scoring and the different odds ratios were calculated. The manuscript published by Sorka and coworkers was considered as 12 studies. 32 The authors used 3 LLM (ChatGPT V4, claude sonnet and o1). Besides, they compared the scores of the LLM to the residents, the attending physicians and the global scores. 30
The manuscript of Schmilovitch and colleagues was considered as 2 studies. The authors compared the LLM scores to the experts’ scores and real world decisions. 31
The manuscript published by Tini and colleagues was considered as 4 studies. The authors used real-world clinical vignettes in addition to vignettes of high and intermediate complexity. Besides, the authors assessed the scores of experts and specialists. 22 The vignettes are defined as revealing symptoms with the clinical history, the laboratory investigations and the patients’ management. The vignettes were considered real when they corresponded to real records in opposition to created or published ones. Published vignettes are usually different from real ones because the information judged as unuseful or unnecessary for the diagnosis are almost always deleted for publication purposes.
The manuscript published by Hirosawa and coworkers was considered as 2 studies. 32 The authors compared the scores of LLM to physicians using a binary method comparing the concordance in the top 5 differential diagnoses suspected and in the 10 differential diagnoses suspected. 32 The manuscript publised by Horiuchi and colleagues was considered as 6 studies. The authors compared the LLM’s scores to 3 different residents and 3 different board certified radiologists. 33 The article published by Stoneham and coworkers was considered as 2 studies because the authors compared the LLM’s scores to general practitionners and dermatologists. 35
The Main Characteristics of the Studies Included
Meta-Analysis Results
We analysed the results of the studies using continuous scores and binary scores separately. This was due to the fact that we need to compare standard means in the former ones and Odds ratios in the later ones.
Considering the studies using binary scores and comparing odds ratios, 1609 clinical vignettes were used to compare the different LLM systems to the human clinical reasoning. The combined Odds ratio reached 0.65 with 95% CI [0.38, 1.12]. No significant difference between both groups was observed (p=0.12). The heterogeneity I-square was evaluated to 77% and Tau2 to 1.46 (Figure 2A). The Funnel plot applied to all the studies included reflected no publication bias. (A) The forest plot illustrating the comparison between LLM systems and physicians in studies using binary scores, (B) The Funnel plot of the studies included highlighting the absence of publication bias, (C) the forest plot illustrating the comparison between LLM systems versus physicians in studies using continuous scores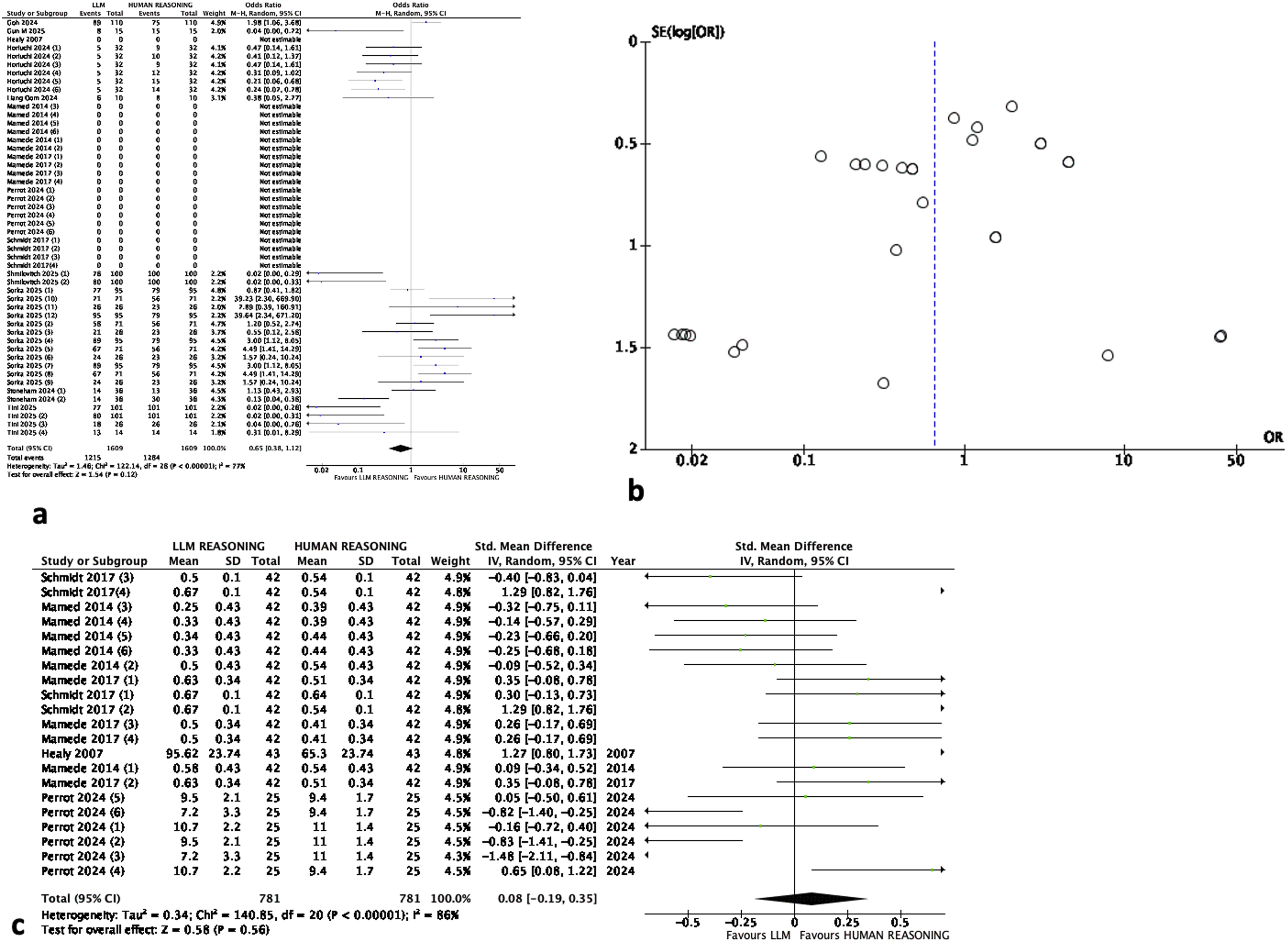
Considering the studies using continuous scores and comparing standard means differences, 781 clinical vignettes were used to compare the different LLM to the human clinical reasoning. The combined standard mean difference reached 0.08 with 95% CI [-0.19, 0.35]. No significant difference was observed between both groups (p=0.56). The heterogeneity I-square was evaluated to 86% and Tau2 to 0.34 (Figure 2C).
Sub-Group Analysis
Facing this heterogeneity, either in studies using binary method or those using continuous scores, we performed a sub-group analysis based on the nature of the clinical cases or vignettes (real-world or published), the LLM used (Chat-GPT v4) and the expertise of the respondants (novices or experts).
Considering the studies using binary scoring methods:
The studies using real clinical cases presented a combined Odds ratio reached 0.09 with 95% CI [0.02, 0.35]. A significant difference between both groups was observed in favour of LLM (p=0.0005). The heterogeneity I-square was evaluated to 74% and Tau2 to 2.72 (Figure 3A). Subgroup analysis of binary studies assessing (A) real-world clinical vignettes, (B) published or created vignettes, (C) the use of ChatGPT V4, (D) novices versus LLM scores, (E) experts versus LLM scores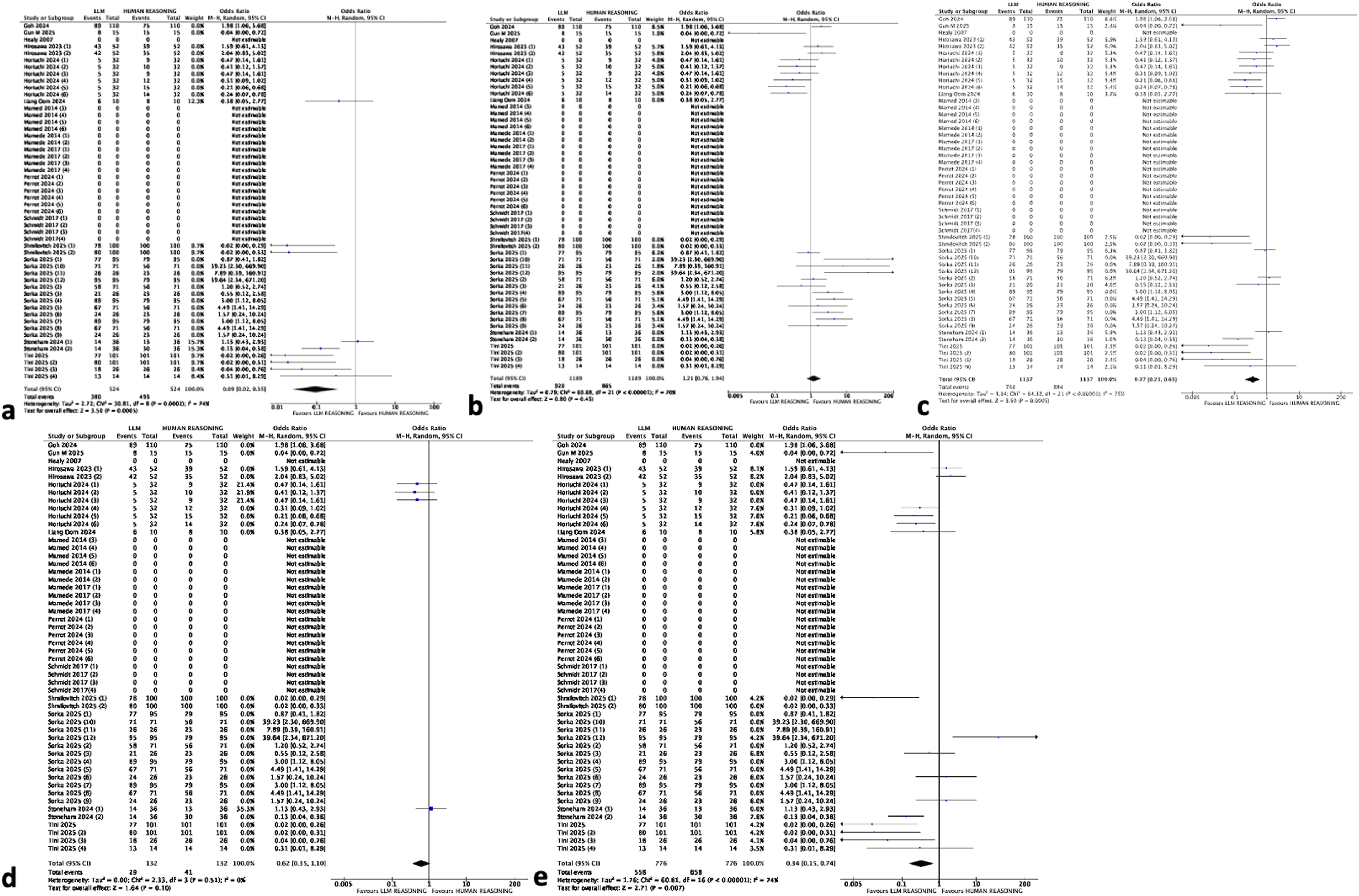
The studies using published or created clinical cases presented a combined Odds ratio reached 1.21 with 95% CI [0.76, 1.94]. No significant difference was observed between both groups (p=0.43). The heterogeneity I-square was evaluated to 70% and Tau2 to 0.79 (Figure 3B).
The studies using ChatGPTv4 presented a combined Odds ratio reached 0.37 with 95% CI [0.21, 0.65]. A significant difference between both groups was observed in favour of LLM (p=0.0005). The heterogeneity I-square was evaluated to 75% and Tau2 to 1.14 (Figure 3C).
The studies comparing LLM’s scores to novices’ scores presented a combined Odds ratio reaching 0.62 with 95% CI [0.35, 1.1]. No significant difference was observed between both groups (p=0.1). The heterogeneity I-square was evaluated to 0% and Tau2 to 0.00 (Figure 3D).
The studies comparing LLM’s scores to experts’ scores presented a combined Odds ratio reaching 0.34 with 95% CI [0.15, 0.74]. A significant difference between both groups was observed in favour of LLM (p=0.007). The heterogeneity I-square was evaluated to 74% and Tau2 to 1.76 (Figure 3E).
Considering the studies using continuous scoring methods:
The studies using real clinical cases presented a combined standard mean difference reaching 0.19 with 95% CI [-0.07, 0.46]. No significant difference between both groups was observed (p=0.16). The heterogeneity I-square was evaluated to 81% and Tau2 to 0.21 (Figure 4A). Subgroup analysis of continuous scores studies assessing (A) real-world clinical vignettes, (B) published or created vignettes, (C) the use of ChatGPT V4, (D) novices versus LLM scores, (E) experts versus LLM scores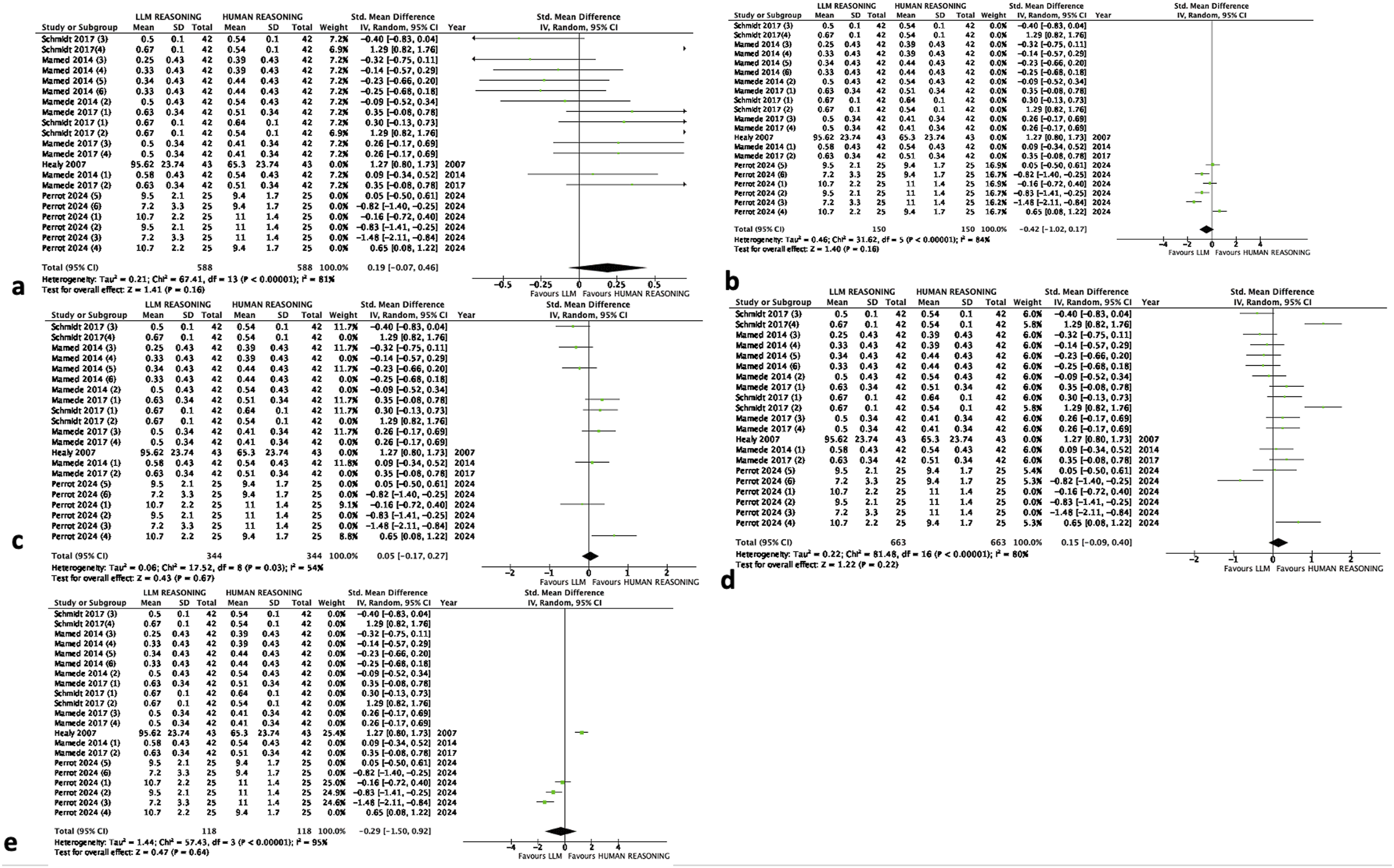
The studies using published or created clinical cases presented a combined standard mean difference reaching -0.42 with 95% CI [-1.02, 0.17]. No significant difference was observed between both groups (p=0.16). The heterogeneity I-square was evaluated to 84% and Tau2 to 0.46 (Figure 4B).
The studies using ChatGPTv4 presented a combined standard mean difference reaching 0.05 with 95% CI [-0.17, 0.27]. No significant difference between both groups was observed (p=0.67). The heterogeneity I-square was evaluated to 54% and Tau2 to 0.06 (Figure 4C).
The studies comparing LLM’s scores to residents or interns’ scores presented a combined standard mean difference reaching 0.15 with 95% CI [-0.09, 0.40]. No significant difference was observed between both groups (p=0.22). The heterogeneity I-square was evaluated to 80% and Tau2 to 0.22 (Figure 4D).
The studies comparing LLM’s scores to experts’ scores presented a combined standard mean difference reaching -0.29 with 95% CI [-1.50, 0.92]. No significant difference between both groups was observed (p=0.64). The heterogeneity I-square was evaluated to 95% and Tau2 to 1.44 (Figure 4E).
Discussion
This meta-analysis highlighted the difficulty to compare human clinical reasoning to LLM clinical reasoning because of the important heterogeneity. Considering the studies using binary scores and comparing odds ratios, 1609 clinical vignettes were used to compare the different LLM to the human clinical reasoning. The combined Odds ratio reached 0.65 with 95% CI [0.38, 1.12]. No significant difference between both groups was observed (p=0.12). When considering studies using continuous scoring systems, the combined standard mean difference reached 0.08 with 95% CI [-0.19, 0.35]. No significant difference between both groups was observed. These results couldn’t be taken into account because of the importance of the heterogeneity in both types of studies. We performed a sub-group analysis taking into account the nature of the clinical cases (real-world or published), the LLM system used (Chat-GPT v4) and the expertise of the respondants (novices or experts). Using real-case-vignettes is very important because when dealing with clinical reasoning, physicians have to rule out many information reported by the patients that aren’t relevant for the diagnosis and these irrelevant information are almost always deleted from created or published vignettes creating a limitation of the assessment of the information gathering step during the clinical reasoning process. We considered “experts” all specialists or board certified specialists and “novices” all interns or residents included.
The heterogeneity was observed in all subgroups excluding the subgroup of the studies using binary scoring systems and comparing LLM’s scores to novices’ scores. The combined Odds ratio reached 0.62 with 95% CI [0.35, 1.1]. No significant difference was observed between both groups (p=0.1) and the heterogeneity I-square was evaluated to 0% and Tau2 to 0.00. The strengths of this meta-analysis consist of including all kind of studies, those using binary scoring systems and those using continuous tests. Clinical reasoning has many definitions in the literature. These definitions differ according to the different learning theories. Cognitivist view considers clinical reasoning as an intracerebral process used to analyze a patient’s problem in order to make a medical decision and to provide the proper treatment plan. 39 On the other hand, anthropologist view considers clinical reasoning as an out-from-the-skull process necessitating a collaborative inter-professional activity enhanced by the material environment or what is called ‘situativity’. 40 These different views are consensual concerning the complexity of the definition of the clinical reasoning. Clinical reasoning definition can’t be limited to the only diagnostic accuracy because finding the right diagnosis may be hazardous. Clinical diagnosis is a multi-step process including problem characterization, hypothesis generation, pattern recognition, hypotheses validation according to diagnostic tests interpretation with differential diagnosis and diagnostic verification.41,42 All these steps have to be assessed in order to validate human clinical reasoning. AI clinical reasoning has progressed over the last decade. The first-generation AI systems were mainly black boxes systems programmed to find a diagnosis based on the Baysian theory. These systems included versions 3, 3.5 of chat-GPT, Bard, Claude Sonnet. 30 New-generation models such as version 4 of chat-GPT are based on pattern recognition and a mimicking process of the human clinical reasoning.20,22,31-33 The comparison between human clinical reasoning and AI clinical reasoning was in favor of humans within studies using old models and favouring AI in studies using new-generation models. This can’t be supported because of the important heterogeneity observed. Zhuang and colleagues, published a preliminary real-world clinical validation study of a multi-modal reasoning agent. 43 The authors reported a comparable diagnostic accuracy between multi-model agent and opthalmology residents, an outperformance in treatment planning with mitigated errors through structured reasoning highlighting the need for domain-specific AI tools. This study couldn’t be included in our meta-analysis because of the absence of individual results. The version 4 of Chat-GPT was reported as being able to analyze pattern and was assessed as a potential modulator in this meta-analysis. because it is considered as a developed LLM according to many authors.4,33,44-53 The use of new generation models wasn’t a potential modulator according to the subgroup analysis. The concept of pattern mimicker of LLM has also been debated in the literature because even if LLM have this potential it can’t be available with the multiplicity of epidemiological context in the different countries of the world or the patients’ bihaviours or the economic context37,38,54-56
The subgroup analysis highlighted only the role of including non experts as a potential modulator. When comparing LLM systems to novices there was no significant difference. This results could seem disappointing because in studies including experts, the results in both kind of studies highlighted a significant difference in favour of LLM systems and we expect experts to be superior or at leat equal to LLM systems. Even if the heterogeneity ruled out the possibility of considering the expertise as a modulator, this result seems contradictory with the results reported in the literature. In fact, many authors reported that LLM could outperform students in training but not experts. Even the expertise has to be defined. In this study, we considered as experts all specialists but expertise depends on the years of practice and this varies in the different studies and could explain the heterogeneity observed in the experts subgroups. According to some authors, experts difference with novices relies on the veracity of the initial hypotheses during the clinical reasoning process.
In this meta-analysis, we studied the impact of using real-world clinical reasoning. This is explained by the fact that clinical reasoning couldn’t be assessed without taking into account the reality of the context. Published or created cases or vignettes simulate reald-world practice. Our results highlighted a significant different in favour of LLM in binary studies and no significant difference between both group in studies using continous scores. We excluded the context as a potential modulator because of the important heterogeneity in both types of studies. These results are disappointing because they point out that the LLM systems could be more efficient in real-world context in comparison to physicians. Many authors discussed the competences of LLM systems because they aren’t customized to answer to the conditions of clinical settings.
The major limitations of this meta-analysis consist of the inability to assess the sources of heterogeneity and the absence of explanations to the disappointing results concerning the role of the expertise or the adapatbility of the LLM systems to the real-world clinical settings.
Even if, we highlighted the role of including residents or internes as modulators in binary studies, the sub-group results including the experts seem disappointing and remain unexplained. The definition of expertise adopted by the authors may seem quite simple because expertise is also related to the years of experience after graduation and it is also related to different competences according to the different speciaties. On the other hand, there is no consensus about the number of years of experience to define expertise because of individual cognitive differences that can explain different expertise levels of physicians with similar years of experience.
Conclusion
Due to fundamental methodological limitations and unmanageable heterogeneity, this meta-analysis cannot provide a definitive answer to the research question regarding superiority of AI to humans in domain of clinical reasoning. It showed substantial heterogeneity across studies, which limited the interpretability of the pooled results. Although subgroup analyses were performed, they do not fully resolve this issue. The research question (“Can AI reasoning replace human reasoning?”) is a deep qualitative-philosophical-clinical question and choosing a quantitative method requires more studies using binary scoring system and focusing on the importance of the expertise or the use of real-world clinical vignettes to answer to the question related to the comparison of LLM clinical reasoning to human clinical reasoning. Besides, future research should look at process-oriented benchmarks rather than just the final diagnosis because clinical reasoning isn’t just about finding the accurate diagnosis but it is about a kind of chain-of-thought.
Footnotes
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Mona Mlika. The first draft of the manuscript was written by Mona Mlika, Majdi Zorgati, Imen Ben Ismail and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.