
Abstract
Background
The integration of “Internet+” technologies into medical education has prompted the evolution of traditional teaching models. Case-based learning (CBL), a student-centered approach, is widely used in integrated curricula such as Clinical Pathophysiology & Therapeutics (CPPT). However, the comparative effectiveness of “Internet+” CBL versus traditional CBL in this context remains underexplored.
Objective
To compare the effects of “Internet+” CBL and traditional CBL on teaching satisfaction and perceived learning gains among medical students in a CPPT course, and to provide evidence for educational reform.
Methods
A within-subject comparative survey was conducted among fourth-year undergraduate medical students who had experienced both CBL modalities. The adapted Students’ Evaluations of Educational Quality (SEEQ) questionnaire was used to assess teaching satisfaction and perceived learning gains. Data from 180 valid responses were analyzed using paired t test or Wilcoxon matched-pairs signed rank test.
Results
“Internet+” CBL was rated significantly higher than traditional CBL in overall teaching satisfaction, understanding and application of knowledge, and development of information analysis and teamwork skills. However, the results showed that the “Internet+” CBL modality received higher ratings in terms of learning burden. Both modalities faced challenges in pre-class question initiation and teacher-student interaction.
Conclusion
“Internet+” CBL is associated with higher student-reported learning gains and greater teaching satisfaction among the medical students, albeit with an increased workload. The findings support the adoption of blended CBL approaches in integrated medical curricula and highlight areas for further optimization, such as improving pre-class engagement and interaction.
Keywords
Introduction
Medical education has undergone a paradigm shift over the past decades, moving from traditional instructor-centered lectures to learner-centered approaches that emphasize active participation and lifelong learning.1,2 Traditional classroom-based teaching, while still prevalent, often fails to sustain student engagement and promote deep understanding; studies indicate that students retain only a small fraction of knowledge delivered through passive lectures. 3 In response, educators have increasingly adopted problem-based learning (PBL) and case-based learning (CBL), which situate learning in realistic clinical scenarios and encourage self-directed inquiry.4,5
Clinical Pathophysiology & Therapeutics (CPPT) is the core integrated course of clinical medicine, which covers internal medicine, pathology, pathophysiology, neurology, infectious diseases, surgery, obstetrics, and gynecology. In this study, CPPT employs CBL as its primary instructional strategy, using clinical cases to guide students through the recognition of pathological findings and the development of diagnostic and therapeutic reasoning. 6 CBL, rooted in constructivist learning theory, posits that knowledge is best acquired when learners actively construct meaning through authentic problem-solving. 7
The rapid advancement of digital technologies has given rise to “Internet+” education — a term originating from a 2015 Chinese government policy framework that refers to the integration of Internet technologies with traditional education, which leverages online platforms, massive open online courses (MOOCs), and virtual resources to enhance teaching and learning.8,9 In the context of CBL, “Internet+” modalities incorporate pre-class online questionnaires, case previews, discussion forums, and post-class exercises, enabling more flexible and resource-rich learning environments. Previous pilot studies have suggested that technology-enhanced CBL can improve student engagement and knowledge acquirement.10,11 However, large-cohort studies providing a direct comparison between the “Internet+” CBL and traditional CBL within an integrated curriculum like CPPT remain scarce.
In this study, the CPPT course is delivered in two stages: the first adopts an “Internet+” CBL format with online pre-class activities and post-class reinforcement, while the second employs a traditional CBL format without such digital enhancements (Figure 1). This design offers a unique opportunity to compare the two approaches within the same cohort of students. Understanding their relative strengths and weaknesses is essential for optimizing curriculum design and informing future educational reforms. Therefore, this study aimed to evaluate and compare the effects of “Internet+” CBL and traditional CBL on students’ teaching satisfaction and perceived learning gains in the CPPT course. We hypothesized that “Internet+” CBL would yield higher satisfaction and greater perceived gains in analytical and collaborative skills, but might also increase students’ workload. The findings are expected to provide evidence-based guidance for the integration of digital tools in case-based medical education. Different phases of the CPPT course. CPPT, Clinical Pathophysiology & Therapeutics.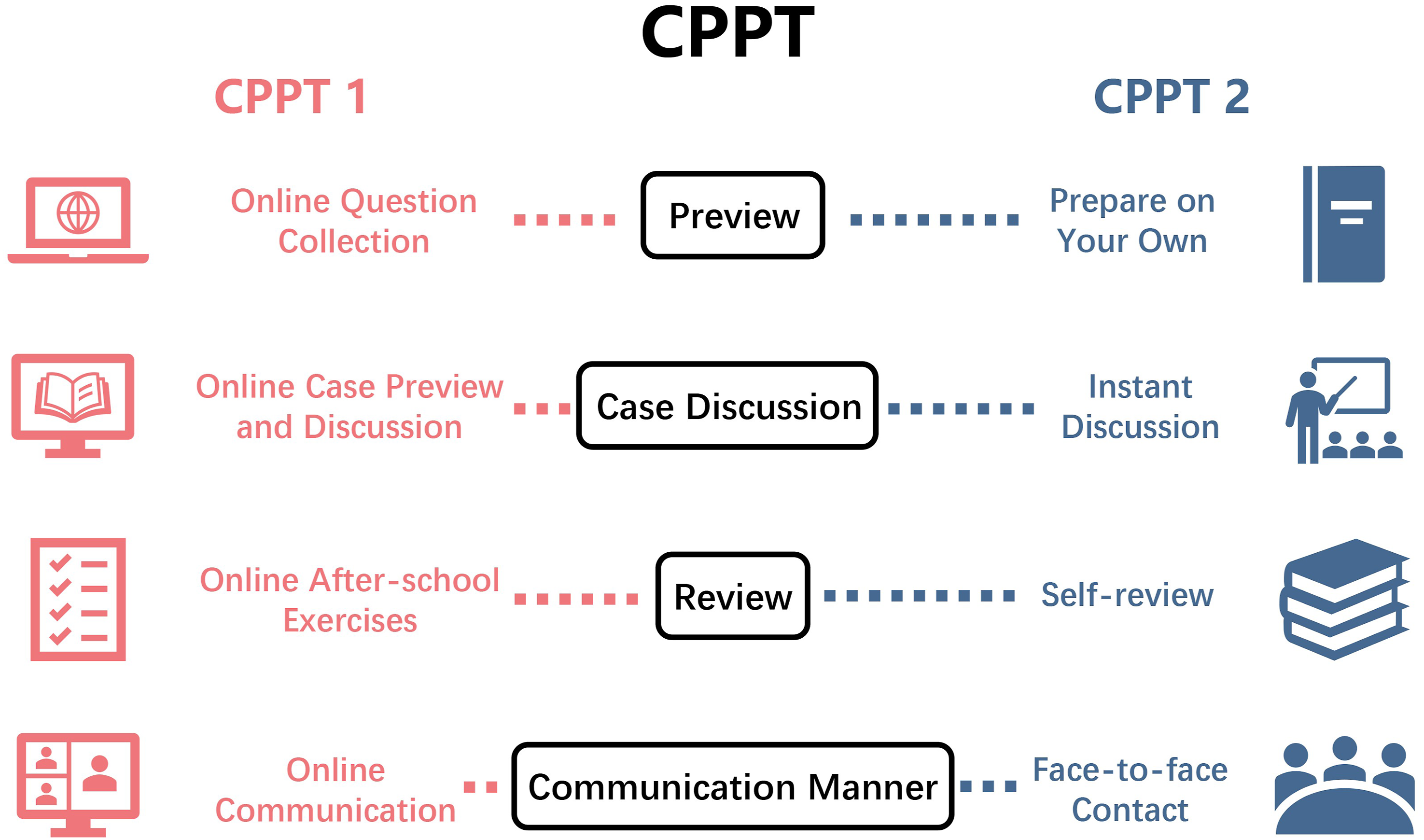
Methods
Ethics Declarations
This study was approved by the Renmin Hospital of Wuhan University Clinical Research Ethics Committee (approval number: WDRY2023-K001). This study adhered to the Declaration of Helsinki. All methods were performed in accordance with relevant guidelines and regulations. All participants provided written informed consent before proceeding with any research activities.
Study Design and Sample Size Calculation
This study is a within-subject comparative survey. The total number of students who met the inclusion criteria was approximately 210. All eligible students were invited to participate, and a total of 180 valid questionnaires were finally obtained, covering 85.7% of the target population, demonstrating good representativeness. A post-hoc analysis based on the primary outcome measure yielded an effect size of Cohen’s d ≈ 0.304. Assuming α = 0.05 and power (1−β) = 0.80, the minimum required sample size was approximately 90. The actual study included 180 paired valid responses, far exceeding the minimum requirement, and the post-hoc power analysis showed 1−β > 0.95, indicating that the sample size was adequate.
Two-Stage CPPT Teaching Modality
The CPPT course was delivered in two sequential stages (Figure 1). In the first stage (CPPT1), the “Internet+” CBL modality was implemented. This modality incorporated the following digital components: (a) pre-class online guiding questions and case previews – before each discussion session, students received a set of guiding questions and electronic case materials via an online platform, which they were expected to review and research independently; (b) electronic pathology slide library – a comprehensive digital library of pathology slides was established, accessible through the university’s learning management system, enabling students to view and study slides at any time using personal electronic devices; and (c) post-class online homework – after each session, students completed a brief online quiz or exercise designed to consolidate their understanding of the key concepts covered in the case discussion. In the second stage (CPPT2), the traditional CBL modality was employed. None of the above online resources were provided. Teaching relied exclusively on face-to-face lectures, paper-based case handouts, and in-class discussions without any digital pre-class or post-class components.
Inclusion and Exclusion Criteria
Fourth-year clinical medical undergraduates from the First Clinical School of Wuhan University were enrolled in this study from July 2022- August 2024. Inclusion criteria were as follows: (a) had completed both phases of the CPPT course in their entirety; (b) agreed to participate voluntarily and provided written informed consent. The main exclusion criteria included: (a) incomplete completion of both phases of the CPPT course; (b) incomplete questionnaire responses or logically inconsistent responses (e.g., identical ratings across all items); or (c) inability to provide informed consent.
Survey Methods
Combined with an evaluation of teaching satisfaction and perceived learning gains, we designed and distributed the “Learning Experience” questionnaire. Questionnaires were distributed and collected using Wenjuanxing (a platform that provides the function of editing and sending questionnaires). Exclusionary questions were set in the questionnaire to ensure that all subjects were medical-related students who had experienced both “Internet +” CBL and traditional CBL teaching modes.
General Information Survey
This includes the age, gender, grade, and major of students.
“Learning Experience” Questionnaire
The questionnaire was adapted to the actual situation based on the students’ evaluations of educational quality (SEEQ), 12 which is used to evaluate students’ learning experience in different teaching modes. It consists of two types of questions: general information, and comparative scoring, which mainly reflect teaching satisfaction and perceived learning gains. Comparative scoring questions had five choices, with one point for “strongly disagree,” two points for “disagree,” three points for “fair,” four points for “agree” and five points for “strongly agree”. 13 We conducted a pilot test on 10 students from the same major who did not participate in the formal study, and made minor adjustments to the questionnaire based on the results. Additionally, five experts with backgrounds in educational research methodology (including one course teaching expert, one medical education researcher, and three instructors) were invited to independently evaluate the content validity of the revised questionnaire. The results showed that the item-level content validity index (I-CVI) ranged from 0.80 to 1.00, and the scale-level average content validity index (S-CVI/Ave) was 0.96, indicating good content validity of the adapted questionnaire. In the formal study, Cronbach’s alpha coefficient of the questionnaire was 0.924, demonstrating excellent internal consistency. This study employed a convenience sampling method, and all students voluntarily participated in the experiment. It should be noted that voluntary participation does not equate to random sampling; therefore, the generalizability of the findings may have certain limitations. In terms of questionnaire content design, all questions were asked twice to obtain student scorings of the two different educational modes.
Statistical Analysis
For continuous variables, data were reported as mean ± SD or P50 [P25, P75] and analyzed by paired t test or Wilcoxon matched-pairs signed rank test. For the count variables, data were presented as percentage or rate. All data were analyzed using the SPSS software program (version 26.0.0, IBM Corp, Armonk, NY), and a two-tailed P < 0.05 was considered significant.
Results
General Information
A total of 190 questionnaires were collected between July 2022 and August 2024, of which 180 were valid, yielding an effective response rate of 94.7%. The respondents were fourth-year undergraduate medical students from the First Clinical School of Wuhan University, including 62 (34.4%) from the five-year clinical medicine program, 72 (40.0%) from the “5+3” integrated program, and 46 (25.6%) from the eight-year program. The age of participants was 20.29 ± 0.81 years, with 56 male (31.1%) and 124 female (68.9%) students. All respondents had completed both phases of the CPPT course and experienced both “Internet+” CBL and traditional CBL modalities.
Comparative Analysis of Teaching Satisfaction
Learning Burden and Pre-class Preparation
Students reported a significantly higher learning burden under the “Internet+” CBL mode compared to traditional CBL (Item 1) (P<0.001). Similarly, online homework was perceived as more burdensome in the “Internet+” group (Item 10). Despite this increased workload, students acknowledged that pre-class exercises enhanced the targeting of teaching (Item 2) (P=0.011) and helped them better understand learning requirements before class discussions (Item 3) (P=0.004). The pre-class case preview was rated as more beneficial for focused learning in the “Internet+” group (Item 5) (P<0.001).
Learning Resources and Guidance
Students perceived that the learning resources provided in the “Internet+” CBL mode (questionnaires, case PPTs, etc.) played a significantly greater guiding role in their studies (Item 6). Online homework was also rated as more effective in consolidating knowledge understanding in the “Internet+” group (Item 8). However, no significant difference was found between the two modes regarding the conduciveness of resources for advance study planning (Item 7).
Alignment With Syllabus and Question Feedback
The electronic pathology slide library in the “Internet+” CBL mode was perceived as better aligned with the teaching syllabus compared to traditional materials (Item 9) (P=0.004). Students also reported that the number of seminar cases better matched the class hours in the “Internet+” mode (Item 12) (P<0.001). However, no significant difference was observed in the timeliness of question feedback through online groups (Item 11). Notably, students’ enthusiasm for asking questions in pre-class collection was low in both groups, with traditional CBL scoring significantly lower (Item 4) (P=0.042).
Comparative Analysis of Perceived Learning Gains
Knowledge Acquisition and Clinical Skills
Compared with the traditional CBL modality, the “Internet+” CBL modality indicated greater improvement in disease diagnosis knowledge (Item 13) (P=0.048), case analysis ability (Item 15) (P=0.019) and pathology image interpretation skills (Item 19) (P=0.011). However, no significant differences were found between the two groups in overall mastery of theoretical knowledge (Item 14), or improvement in clinical thinking (Item 18).
Self-Learning and Collaborative Skills
Students rated the “Internet+” CBL mode significantly higher in enhancing their ability to collect and analyze information through online preview (Item 17) (P=0.036). Online homework was also perceived as more effective in strengthening communication and teamwork skills in the “Internet+” group (Item 20) (P=0.024). No significant difference was observed in the perceived contribution of advance case preview to self-study ability (Item 16) (P=0.217).
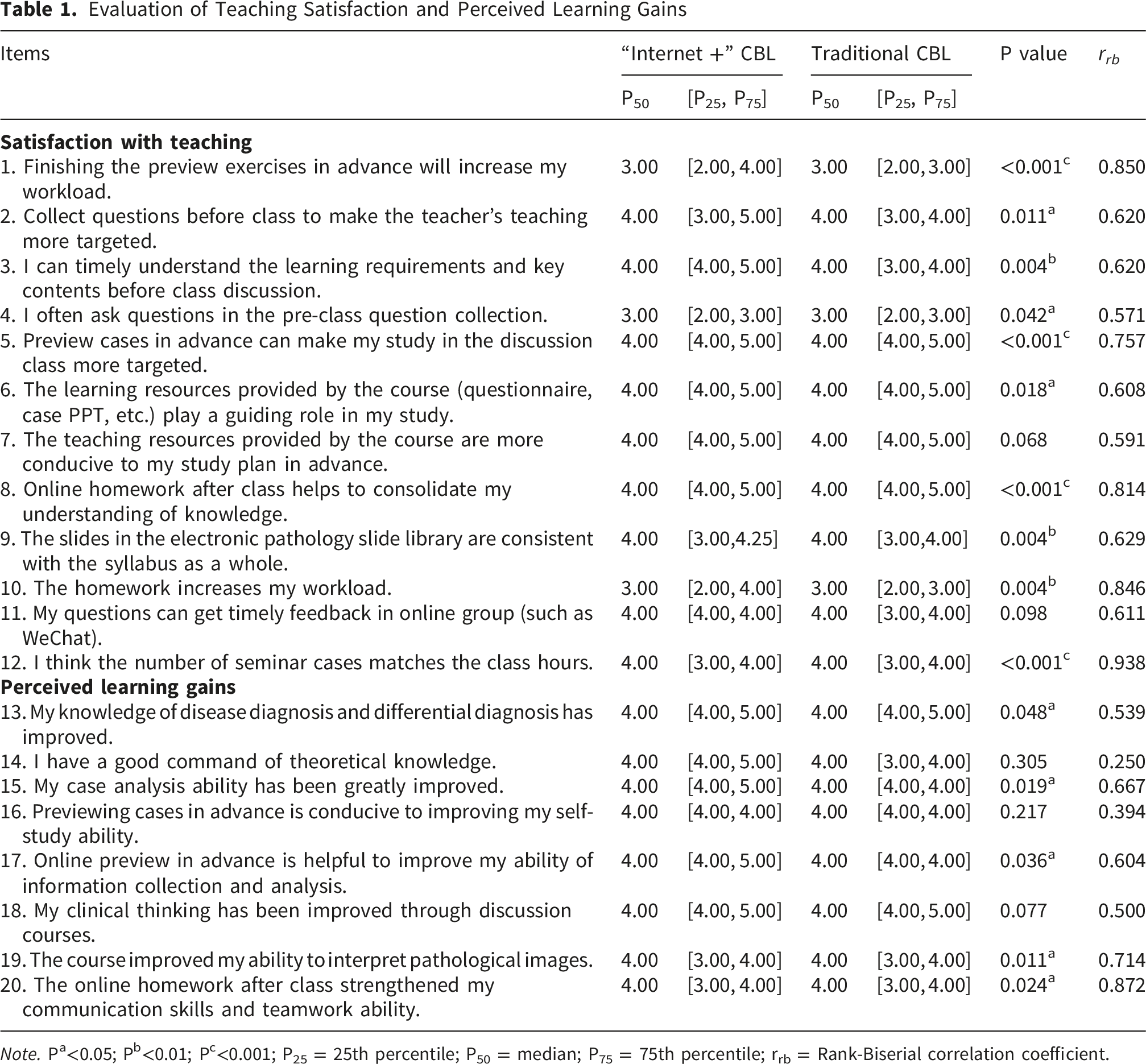
Collectively, regarding teaching satisfaction, “Internet +” CBL is generally better than traditional CBL, but it will increase the learning burden of students. In terms of perceived learning gains, “Internet +” CBL can improve students’ abilities in multiple aspects (Figure 2A-C). Details of the questionnaire are shown in Table 1. Results of the questionnaire research. (A) Comparison of teaching satisfaction in the two groups. (B) Results of perceived learning gains. (C) Average scores of the two groups in terms of teaching satisfaction and perceived learning gains. *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001; ns, no statistical significance. Evaluation of Teaching Satisfaction and Perceived Learning Gains Note. Pa<0.05; Pb<0.01; Pc<0.001; P25 = 25th percentile; P50 = median; P75 = 75th percentile; rrb = Rank-Biserial correlation coefficient.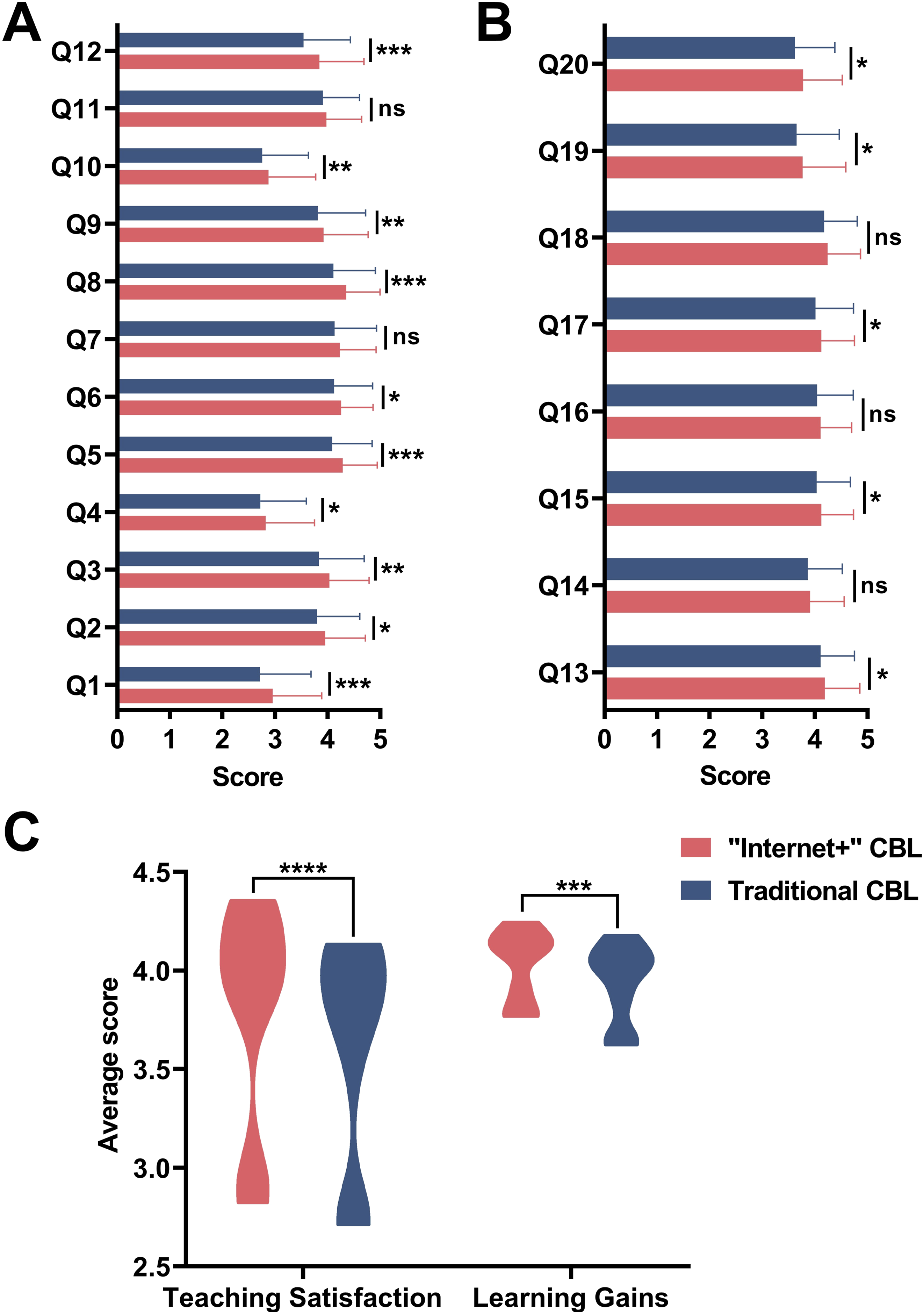
Discussion
Major Findings
This study compared “Internet+” CBL and traditional CBL within an integrated CPPT curriculum, revealing that the technology-enhanced approach significantly outperformed its conventional counterpart in multiple dimensions of teaching satisfaction and self-reported learning outcomes, albeit with an increased perceived workload. These findings align with the growing body of evidence supporting the integration of digital tools into case-based medical education. However, the observed trade-off between enhanced learning experiences and increased student workload warrants careful consideration in curriculum design.
“Internet+” CBL Enhanced Teaching Satisfaction
The superior teaching satisfaction ratings for “Internet+” CBL can be attributed primarily to its structured pre-class components, including online questionnaires, case previews, and targeted exercises. These elements address a fundamental limitation of traditional CBL: the lack of guided preparation. From a cognitive load theory perspective, 14 well-designed pre-class activities reduce extraneous cognitive load by orienting students to key concepts and learning objectives before they engage in complex case discussions. This allows working memory resources to be allocated more efficiently to authentic problem-solving during class, rather than being overwhelmed by simultaneous exposure to new content and clinical reasoning demands. 15
Our finding that pre-class resources enhanced the targeting of teaching (Item 2) and helped students understand learning requirements (Item 3) supports this interpretation. The significantly higher rating for the guiding role of learning resources in “Internet+” CBL (Item 6) further suggests that structured digital materials serve as cognitive scaffolds, helping students navigate the complexity of integrated medical content. This is particularly valuable in courses like CPPT, which synthesize multiple disciplines and require students to integrate basic science knowledge with clinical application.
“Internet+” CBL Improved Self-Reported Learning Outcomes
The “Internet+” CBL modality demonstrated significant advantages over the traditional CBL modality in developing disease diagnosis and differential diagnosis knowledge (Item 13), case analysis ability (Item 15), information collection and analysis skills (Item 17), and pathological recognition (Item 19). These findings resonate with constructivist learning theory, which posits that meaningful learning occurs when learners actively construct knowledge through interaction with authentic problems and resources. The online preview and pre-class questionnaires in “Internet+” CBL transform students from passive recipients of information into active investigators who must gather, evaluate, and synthesize information before entering the classroom.
This preparatory phase likely activates prior knowledge and generates curiosity, creating a “readiness to learn” that enhances the effectiveness of subsequent case discussions. 16 The step-by-step guidance provided by sequenced online resources may also promote the development of metacognitive skills, as students learn to monitor their own understanding and identify knowledge gaps before class. 17 The significant improvement in pathological recognition skills specifically may reflect the advantages of the electronic pathology slide library, which offers high-quality images, annotation capabilities, and self-assessment opportunities that are difficult to achieve with traditional printed atlases.
“Internet+” CBL Cultivated Teamwork Skills
The finding that online homework strengthened communication and teamwork skills (Item 20) more effectively in “Internet+” CBL deserves particular attention. This suggests that technology-enhanced CBL not only facilitates individual learning but also creates new opportunities for collaborative knowledge construction. Online discussion forums and group assignments require students to articulate their thinking, respond to peers’ perspectives, and negotiate shared understanding—processes that are central to the development of collaborative competence. 18 In contrast, traditional CBL often limits collaboration to face-to-face discussions, which may be constrained by time and dominated by more vocal participants. The flexibility of online platforms may also enable more equitable participation, allowing students with different learning styles and communication preferences to contribute meaningfully.
“Internet+” CBL Increased the Learning Workload
Despite its advantages, “Internet+” CBL was associated with significantly higher perceived workload (Items 1 and 10). This finding highlights a critical tension in technology-enhanced education: the same features that enrich learning—additional resources, preparatory tasks, and follow-up exercises—can also increase workload and potentially contribute to student burnout. Importantly, however, students in our study generally considered the workload acceptable, suggesting that the perceived benefits may outweigh the costs. Nonetheless, the higher workload might also reflect factors beyond sheer workload, such as poor calibration of pre-class tasks (e.g., tasks that were too time-consuming or misaligned with students’ available time), suboptimal usability of the online questionnaire platform, or insufficient guidance on how to effectively navigate the pre-class resources. The higher ratings for the guiding role of resources and the perceived relevance of online homework suggest that when using the “Internet+” CBL modality, students may have experienced these tasks as meaningful and instrumental to their learning goals, thereby mitigating the negative impact of increased workload.
Moreover, whether comparable positive effects could be achieved by providing online resources without mandating pre- and post-questionnaires remains unknown. It is possible that optional resources would reduce perceived workload, but may also lead to lower engagement and diminished learning gains for less self-motivated students. Future studies should compare mandatory versus optional designs to determine the optimal balance between structure and flexibility.
Collectively, these findings underscore the importance of thoughtful curriculum design that balances enrichment with feasibility. Strategies to optimize this balance might include: (1) carefully calibrating the number and complexity of pre-class tasks to avoid overload; (2) clearly communicating the purpose and value of each online component; (3) providing flexible deadlines and allowing student choice in some activities; and (4) integrating pre-class preparation with in-class activities to create coherent learning experiences rather than disjointed tasks. 19
Persistent Challenges: Pre-class Questioning and Teacher-Student Interaction
Both CBL modalities faced challenges in stimulating pre-class questions (Item 4) and facilitating timely teacher-student interaction (Item 11). The low enthusiasm for pre-class questioning may reflect several factors: students’ limited prior knowledge of new topics, lack of confidence in formulating questions, or perception that questions will not receive timely responses. The significantly lower scores for traditional CBL in this domain suggest that digital platforms alone are insufficient to cultivate a questioning culture; deliberate pedagogical strategies are needed.
The persistent challenge of teacher-student interaction in both modes highlights a limitation of current “Internet+” implementations. While technology enables asynchronous communication, it may not automatically foster the kind of responsive, dialogic interaction that characterizes effective teaching.20,21 Students’ suggestions—dedicated Q&A sessions, more timely online responses, and increased clinical clerkship opportunities—point toward hybrid solutions that combine the flexibility of online platforms with the immediacy and richness of face-to-face interaction.
Confounding Factors and Study Limitations
Several confounding factors of this study should be acknowledged. First, the two teaching modalities were delivered sequentially, with all students first receiving the “Internet+” CBL format followed by the traditional CBL format. This fixed teaching sequence may introduce an order effect, as students’ evaluations of the second modality could be influenced by their prior exposure to the first. Additionally, maturation effect cannot be excluded, as students may have developed enhanced knowledge or skills over time that systematically affected their ratings. The novelty effect is also possible; students might have rated the “Internet+” CBL modality more favorably simply because it was a new, technology-driven approach, rather than due to its inherent pedagogical superiority. Furthermore, teacher differences or variations in implementation across the two phases may have contributed to the observed differences, as different instructors might have emphasized different aspects or interacted with students differently, even though the syllabus and case materials were standardized. The difficulty of clinical curriculum may also have varied across the two phases of the CPPT course, potentially influencing perceived learning gains and satisfaction independently of the teaching modality. Finally, since the questionnaire was administered after the completion of both phases and data were collected over an extended period, recall bias is possible. Students’ retrospective comparisons may be subject to inaccuracies or influenced by the recency of the second phase.
Furthermore, this study has several additional limitations as follows. Firstly, the questionnaire was adapted from the SEEQ to suit the actual situation and may not address the individual questions and requirements of some students. Secondly, although internal consistency of this questionnaire was high (Cronbach’s α > 0.9), test-retest reliability was not evaluated because the survey was administered only once. Thirdly, the questionnaire did not address emotional aspects, which may also have an impact on students’ experiences. Fourthly, as this was a small sample, single-center study, some of our data are speculative rather than confirmatory. Moreover, the sample was predominantly female (68.9%), reflecting the actual gender distribution in our medical program but potentially limiting the generalizability of findings across genders. Due to the small number of male participants, subgroup analysis by gender was not feasible. Future studies with more balanced gender samples are needed to confirm whether the observed advantages of “Internet+” CBL apply equally to both genders. Finally, this study assessed learning outcomes solely through students’ self-reported perceptions rather than objective measures such as examination scores or clinical performance evaluations. Although perceived learning gains provide valuable insight into learners’ confidence and subjective growth, they do not directly equate to actual knowledge acquisition or clinical competence. The two course phases (CPPT1 and CPPT2) covered different clinical topics, precluding direct comparison of objective academic performance. Future studies should adopt a randomized controlled design within the same course content and include objective tests or standardized clinical assessments to validate these findings.
Conclusion
Collectively, this study demonstrates that “Internet+” CBL offers significant advantages over traditional CBL in the integrated CPPT curriculum, enhancing teaching satisfaction and improving perceived learning gains in case analysis, information processing, and collaborative learning. These benefits are achieved through structured preparation, enriched resources, and flexible engagement opportunities. However, the increased perceived workload associated with “Internet+” CBL requires careful management to ensure that enrichment does not become overload. Overall, “Internet +” CBL builds a brand-new teaching environment with the help of Internet platform and resources, which preliminarily shows potential as a promising direction for the teaching model of clinical competency training, while also providing possible exploratory ideas for future medical educational reforms.
Footnotes
Acknowledgement
We thank all participants for their cooperation and the teachers of the course team for their help.
Authors’ contributions
H.H., J.W., X.W. and Y.C. contributed equally to this work. H.H. and S.W. identified the themes and framework of this study. H.H., J.W., X.W. and Y.C. reviewed literature and drafted the manuscript. X.W. and H.H. designed and distributed the questionnaire. J.W. and J.Z. performed the data recovery and processing. Finally, S.W. reviewed the manuscript and provided suggestions for amendment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Natural Science Foundation of China (No. 82570593), the Natural Science Foundation of Hubei Province (No. JCZRYB202400863), the Fundamental Research Funds for the Central Universities (No. 2042025YXB014), and the Interdisciplinary Innovative Talents Foundation from Renmin Hospital of Wuhan University (No. JCRCYG-2022-001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.