
Abstract
The COVID-19 pandemic originally necessitated a shift to virtual learning in psychiatric medical education, accelerating the opportunities to enhance medical training with innovative technologies like virtual reality. Virtual reality (VR) simulation enhances education by providing engaging and safe experiential learning opportunities, aiming to bridge the gap between theory and practice. The established framework of rapid design thinking has been used to guide medical innovations during the COVID-19 pandemic, and can continue to support the highly complex and resource intensive nature of VR design and development ongoing. This paper operationalizes a three-step rapid design thinking framework into a stepwise methodology for developing immersive and non-immersive VR simulations for psychiatric education. Key lessons include the importance of early and creative stakeholder engagement, clear terms of reference, rigorous vendor selection using a tailored vendor assessment matrix, utilizing free digital tools for collaboration, emphasizing diversity, equity and inclusion principles and iterative user testing to ensure usability and effectiveness. This study offers a practical guide for educators integrating VR into psychiatric training, demonstrating the value of rapid design thinking in developing and implementing learner-centered solutions swiftly. Future research should explore VR’s accessibility for individuals with disabilities and its long-term cost-effectiveness compared to traditional training methods.
Manuscript
Medical education quickly adapted to new teaching models since the COVID-19 pandemic.1,2 Pivoting to virtual learning and employing simulation methodologies ensured exposure to key clinical situations. Though born out of necessity, studies show these interventions enhance the learning experience.1,3 Given the rapidly evolving technological landscape, educators continue to explore innovative ways to meet complex training needs. 1 One modality that has grown nearly ten-fold in the last five years is virtual reality (VR).4,5 VR refers to an immersive, computer-generated environment designed to replicate real or imagined settings. Through specialized hardware users can interact with and experience these environments in a psychologically safe way as though physically present. 4
VR simulation enhances psychiatric education by engaging learners, offering a safe practice environment, and bridging theory with practice. 5 VR simulations can be immersive, using head-mounted displays and motion controllers, semi-immersive, using a relatively high graphics computing system with a large screen or non-immersive using standard computing or mobile equipment. 6
The immense upfront costs of developing and delivering custom VR simulations necessitate efficient and knowledgeable ways to navigate its development. Rapid design thinking is an established framework that addresses highly complex problems in medical education and has been used to guide medical education innovations. 2 It can incorporate multiple stakeholder perspectives, create space to innovate and accelerate the development of prototypes and allows for iterative change. The steps to design thinking are: (1) Inspiration: gain understanding of the problem and needs by engaging in user-centered research; (2) Ideation: organize the information gathered and identify the problem; and (3) Implementation: putting innovations into practice. 2
To date, based on a literature review, studies of VR development have focused on interviews with Subject Matter Experts (SMEs) to inform design or toolkits that outline key concepts for facilitating the delivering of VR learning experiences.7,8 To our knowledge, there are no papers describing the design and development process specifically for VR simulation in medicine, including psychiatry. Publications outlining VR design and development using established frameworks are needed to support health professions education teams considering these emerging technologies for education and training. This paper operationalizes rapid design thinking into a replicable, stepwise methodology for developing two immersive and non-immersive VR simulations in psychiatric education. The process, decision points, and tools used to support stakeholder engagement, procurement, accessibility, and iterative testing are emphasized. The approach is intended to be adaptable for health professions education teams developing VR simulations under time, budgetary, or resource constraints.
A Rapid Design Thinking Method for Developing Psychiatric VR Simulations
Overview of the Methodological Approach
Rapid design thinking was applied as a structured development methodology with three stages: inspiration, ideation, and implementation. For each stage, the inputs (data sources and stakeholders), activities (tools and decision-making processes), and outputs (development artifacts and usability findings) are specified. Diversity, equity, inclusion, and accessibility considerations are embedded as cross-cutting principles throughout all stages. See Figure 1 for more details. Key steps to rapid design thinking for VR simulations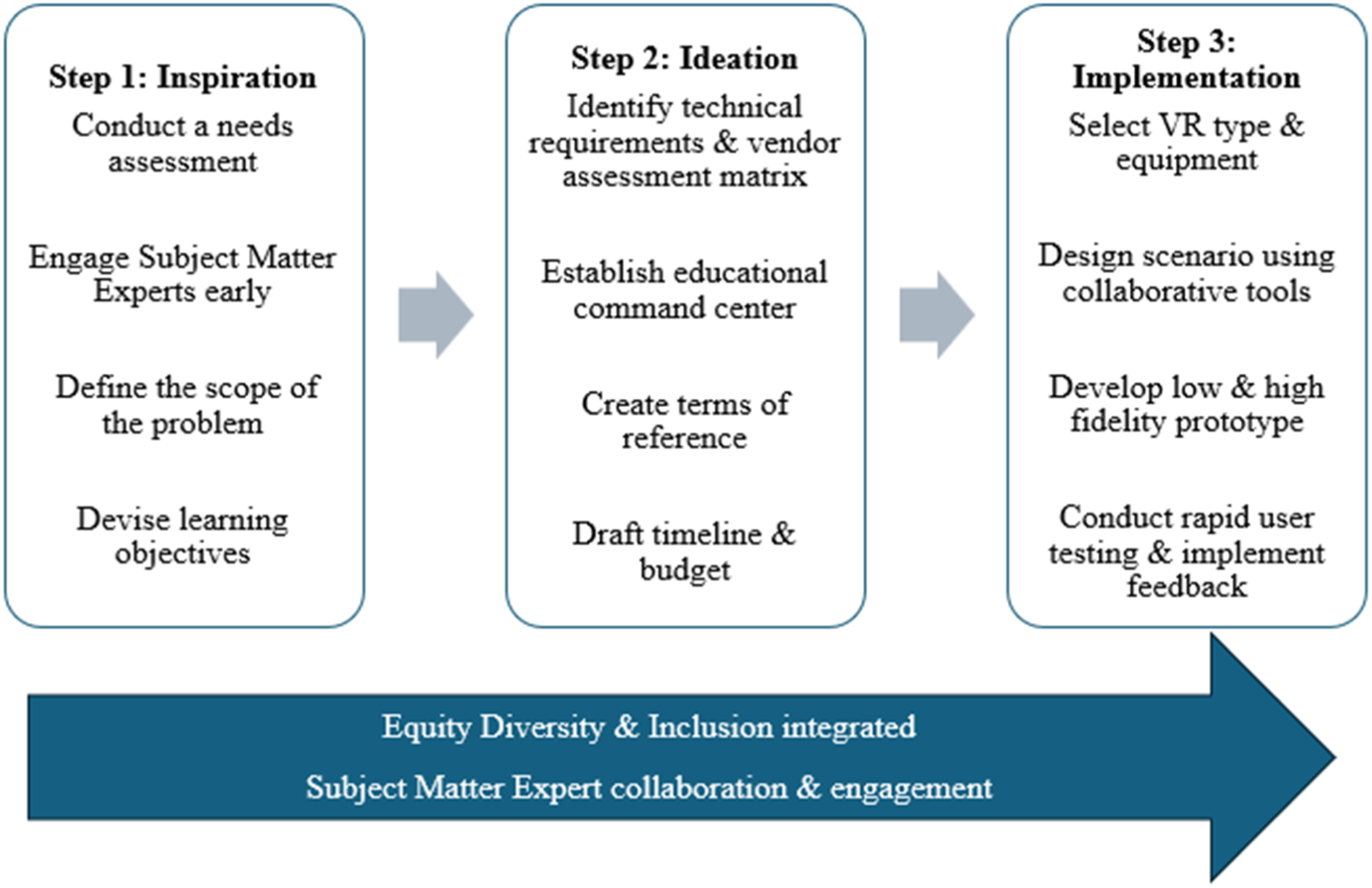
Step 1: Inspiration
The COVID-19 pandemic significantly impacted mental health in Canada, with increased suicidal ideation in frontline workers and marginalized populations. 9 Suicide rates rose to approximately 12 deaths daily, and opioid-related mortality surged by 60%, especially among underserved groups.10,11 Given that nearly half of individuals who die by suicide have contact with a primary care provider in the month prior to death, targeted training in suicide risk assessment is critical to improve early identification and intervention. 12 Similarly, the sharp increase in opioid-related deaths underscores the urgent need for provider education in overdose recognition and response to mitigate preventable fatalities. 11 These findings emphasize an urgent need for enhanced provider training in suicide risk assessment (SRA) and opioid overdose (OO) management.
To address urgent training needs in SRA and OO management, and due to pandemic restrictions, accessible, interactive digital training became a priority. An accredited simulation centre at a major mental health hospital developed VR simulations. The development process began in November 2021 for VR SRA and July 2022 for VR OO and was completed by August 2022 and October 2023, respectively. The intervention was informed by a multi-method needs assessment consistent with continuing professional development best practices, which emphasize triangulating perceived, unperceived, and emergent learning needs. For both SRA and OO simulations, consistent gaps were identified in the application of foundational skills, as well as a need to increase confidence in assessing suicide risk or responding to an opioid overdose. To address these needs, both immersive (using VR headsets and controllers) and non-immersive VR (using standard computing systems) options were created. These formats allow learners to apply foundational skills identified in both needs assessments, while also supporting scalable, remote delivery to reach a broader audience. Gamified VR simulations offer a standardized, repeatable, and innovative training solution.
For the SRA simulation, which was funded by a post-secondary virtual learning grant, the target learner group comprised medical and nursing students. Faculty and clinical staff identified a gap in these learners’ skills in conducting suicide risk assessments. Existing training opportunities were described as either introductory and didactic or advanced and designed for experienced clinicians. No hands-on training opportunity for nursing or medical students to apply foundational skills in suicide risk assessment were identified. A need was therefore identified to provide safe and supportive training environments in which these learners could practice conducting risk assessments before entering the workforce. These gaps informed the creation of learning objectives that focused on application of knowledge, including demonstrating the process of building a therapeutic alliance, conducting a suicide risk assessment to identify risk and protective factors, organizing findings using the 4Ps framework, and appraising which factors are modifiable.
The SRA simulation offered participants an opportunity to conduct SRAs within a clinical setting, engaging with two distinct avatar patients. Each scenario included an avatar preceptor who guided participants through the virtual experience. Training began with a pre-briefing led by the avatar preceptor, introducing participants to the foundational concepts of SRA, including the 4Ps framework: predisposing, precipitating, perpetuating, and protective factors. Participants then interviewed the patient avatars by selecting from a range of pre-written questions designed to uncover both risk and protective factors. Participants categorized the identified factors to assess each patient’s level of suicide risk. Throughout the simulation, feedback was provided via real-time pop-ups, verbal and non-verbal cues from the avatars, and guidance from the virtual preceptor. An additional promotional video shows this in more detail [see Supplemental file 1].
For the OO simulation, the need for opioid overdose response training was identified by clinical staff in a mental health hospital who reported increasing incidences of opioid overdose among patients both in hospital and in the community, as well as through discussions at the hospital’s Quality and Risk Committee. These observations were supported by evidence in the literature and provincial data released during the COVID-19 pandemic. To better understand this need, we reviewed institutional incident reports involving opioid overdose and conducted small-group consultations (approximately 2-3) with interprofessional clinicians, clinical educators, and trainees across undergraduate and postgraduate levels. A literature review on psychiatric emergencies and VR best practices was also undertaken. From these data sources, learning objectives were developed that focused on practicing the steps involved in responding to an opioid overdose in both clinical and community settings. These included assessing a collapse for safety, identifying an opioid overdose and calling for help, administering the required treatment and monitoring the patient’s response, and supporting the patient following an overdose.
The OO simulation was designed to train participants in the effective administration of naloxone, a critical intervention that can temporarily reverse the effects of an opioid overdose, in both clinical and community environments. In the community scenario, participants encountered a young female avatar found unconscious in her bedroom. In the clinical scenario, a male avatar was discovered unconscious in a community clinic bathroom. The training began with participants assessing the scene for safety and identifying any immediate hazards. They then evaluated the avatar for signs of a life-threatening overdose by inspecting key physical indicators such as the pupils, lips, and fingernails. Participants proceeded to administer naloxone: a nasal spray was used in the community setting, while an injectable form was used in the clinical setting. The final stage of the training focused on providing supportive communication and care to the individual until emergency services arrived. An additional promotional video shows this in more detail [see Supplemental file 2].
Step 2: Ideation
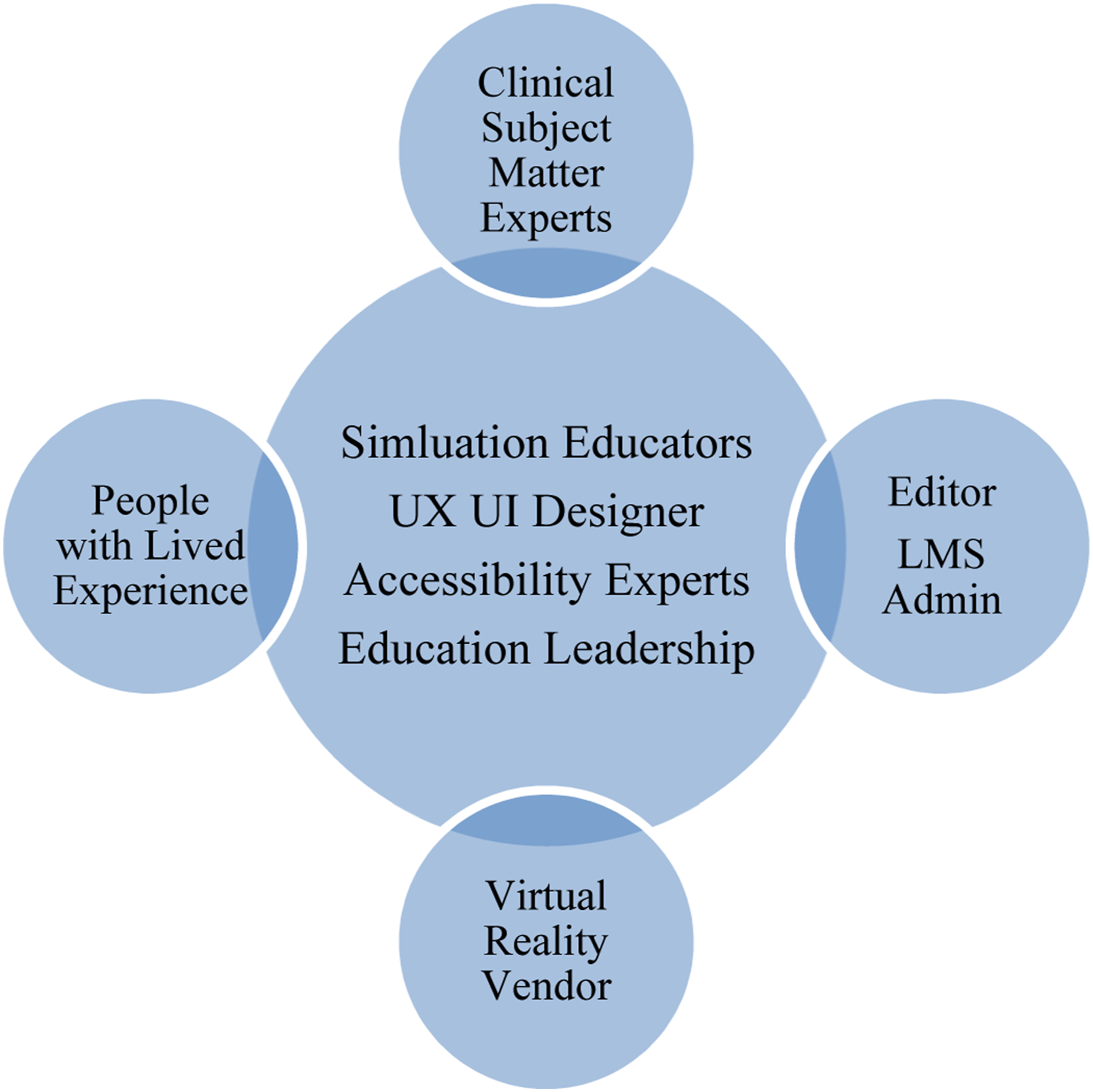
After defining learning objectives and the target audience, engaging stakeholders was critical to ideation. An inclusive “educational command center” brought together key stakeholders with a core team of UX/UI (user experience/user interface) designers, accessibility experts, and simulation educators. This educational command center collaborated regularly with additional experts including people with lived experience (PWLE), clinicians and editors [see Figure 2 for more details]. This structure supported co-design from character profiles to user testing. Clear roles and a jointly developed terms of reference—covering the needs assessment, learning goals, timelines, workflows, and decision-making—enabled effective collaboration. While the hospital provided simulation design expertise, external support was required for VR development. For external vendor selection, the core development team developed a vendor assessment matrix, which specified the following vendor requirements [see Supplemental file 3 for more detail]: 1. Ability to meet technical requirements (e.g. build in a cross-platform game engine, learning management system integration) 2. Ability to meet timeline and budget (e.g. number of simulation scenarios possible in given budget) 3. Ability to ensure sustainable development (e.g. feasibility of revisions post-pilot and ease of use) 4. Possessed knowledge and expertise in VR and UX/UI interface design (e.g. the vendor’s team led development across all stages) Educational command center
Using the vendor assessment matrix was helpful in ensuring the core design team agreed on requirements and enabled objective proposal evaluation and selection. Once the vendor was selected, a service agreement with total cost was agreed upon and signed. The total vendor costs, covered by external grants for VR SRA was $47,080 CAD and for VR OO was $96,180 CAD. The difference in cost across projects can be attributed to the increasing complexity of scenarios for VR OO. Additional costs were covered in-kind by the hospital including staff salaries plus benefits, VR headsets purchased, space, learning management system, licenses, hosting fees and honoraria for subject matter experts/PWLE.
Step 3: Implementation
The educational command center, key stakeholders and vendor collaborated to generate design ideas using low and high-fidelity prototype models including avatar realism, interaction level with the 3D environment and gamification elements. The aim was to enhance user experience while ensuring accurate real-life replication of clinical environments and equipment to minimize cognitive load. 13
It was also important to select the appropriate type of VR equipment for the immersive simulation training. Factors that influenced choice of VR equipment included device specifications (e.g. size, weight) stand-alone versus tethered (i.e. if the headset requires a hardwire connection to a gaming laptop/computer) and cost.
The core design team collaborated with the VR vendor to develop a non-immersive VR version that runs on a standard computer, eliminating the need for a VR headset. This ensures accessibility and affordability, enabling users to engage in VR simulations with their existing device.
Unlike traditional educational modalities, VR requires detailed designing of avatars, scenarios, environments, user interface, script branching, and gamification. Miro™, a free digital collaboration platform, was the virtual space used for all storyboarding, designing of avatars, virtual environments, dialogue, and development of evaluation plans. 14 This virtual platform allowed all stakeholders to collaborate synchronously and asynchronously without creating multiple document versions. Feedback from stakeholders indicated that this facilitated effective collaboration, meeting of tight timelines and the accommodation of different schedules.
Twine™, a free tool for non-linear story design, supported complex avatar conversations in VR scenarios. 15 This branching logic is crucial for conceptualizing psychiatric interviews or patient interactions. The core design team used Twine™ to upload scripts and gather stakeholder feedback on flow and edits. This user-friendly platform fostered collaboration across development stages and effectively captured diverse perspectives.
The key to the implementation stage was rapid prototyping with iterative feedback from stakeholders and target audiences, ensuring that prototypes evolved based on user feedback, improved user experience, while meeting the stated learning objectives. 2 Key stakeholders and target audiences participated in robust iterative user testing processes with timelines that allowed for multiple opportunities for tester feedback, in keeping with a rapid design thinking approach.
The inherent speed and utilitarian principles of rapid design thinking could increase the risk of potentially exacerbating inequities and potentiate bias, if efforts to negate these possibilities are not directly built into the process. This potential risk was addressed by ensuring a compassionate stance and the adoption of a DEI (diversity, equity, inclusion) lens into all stages of development. Specifically, PWLE were key stakeholders and helped ensure a trauma-informed approach that steered the team away from perpetuating biases and stereotypes. For example, for VR SRA, PWLE provided feedback that the patient’s voice did not have enough emotionality in it. This feedback was given to the actor who incorporated it into an updated recording used for that scenario. For VR OO, the process of working with PWLE resulted in a revision to one learning objective focused on supporting the patient after an opioid overdose. The terms of reference, shared goals and values ensured that decisions incorporated diverse perspectives that take into account how power and privilege can taint these processes. While there are currently no approved accessibility standards for VR, we referenced extended reality guidelines and deliberate accessibility adaptations were made to increase accessibility of all VR scenarios. 16 Changes implemented included pre-recorded captions, minimum perceivable text size and minimum color contrast. The team also identified and prioritized the development of a non-immersive version of all VR scenarios, ensuring access for those who cannot tolerate immersive VR, as well as dissemination to remote areas and communities.
The methodology deployed for user testing by the core design team was the Think Aloud method; the user wore a VR headset and mirrored their experience on a larger screen for the facilitator to observe. 17 Non-immersive VR scenarios used video conferencing for a similar interaction. Users shared feedback openly, including thoughts, concerns, and suggestions, while the facilitator noted comments, documented issues, and proposed changes.
Iterative Changes Made During User Testing
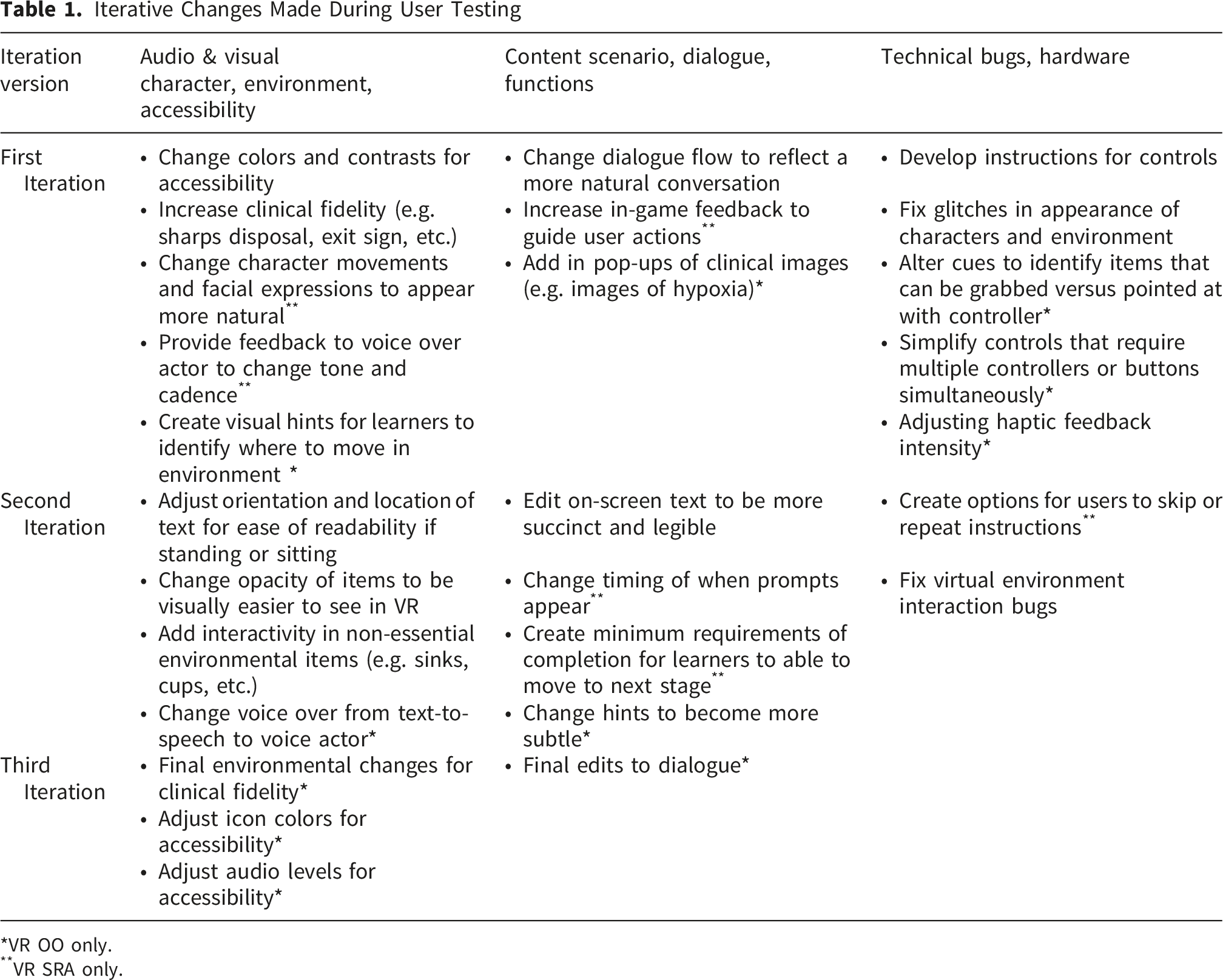
*VR OO only.
**VR SRA only.
Finally, users completed surveys to capture additional anonymous quantitative feedback [see Supplemental file 4]. There were 5 sections included in this user testing survey: demographics, practical relevance, accessibility, overall experience, and achievement of learning objectives. Surveys were developed by the core study team based off Moore’s Outcome Evaluation framework and current extended reality guidelines.16,18 Quantitative questions were measured using either a 5-point Likert scale ranging from ‘strongly disagree (1)’ to ‘strongly agree (5)’ or ‘not at all (1)’ to ‘to a great extent (5)’. Qualitative questions were an open text-box format for users to fill in. IRB/Quality Project Ethics Review approval was obtained prior to commencing VR SRA and VR OO. Participation was voluntary and detailed at the beginning of the surveys was the purpose, confidentiality statement, data storage strategy and informed consent statement.
Participants engaged with either immersive or non-immersive VR formats depending on availability and context. Given the exploratory and methodological focus of the study, outcomes were analyzed across modalities rather than stratified by VR format. No formal comparisons were conducted to assess differential effects between immersive and non-immersive VR, as the study was not designed or powered to examine modality-specific differences. Results therefore reflect aggregated user feedback and outcome measures across both formats.
User testing participants were recruited using a convenience-based sampling approach. Sampling intentionally aimed to include a diverse, interprofessional group representing both experienced clinicians and learners, reflecting the multiple target audiences for which the simulations were designed.
Data Analysis
Descriptive statistics were used to analyze all quantitative data obtained during user testing in IBM SPSS Statistics 27. Thematic analysis was conducted on all open-ended qualitative responses using Braun and Clarke’s six-phase reflexive thematic analysis approach. 19 Two members of the research team independently coded the data and met iteratively to refine codes and develop themes through consensus. 19 Formal inter-rater reliability was not calculated, consistent with reflexive thematic analysis, with rigor supported through iterative review and clear alignment between the themes and participant responses. 19
All steps of this method were done multiple times throughout user testing; VR SRA had 2 iterations of user testing for both immersive and non-immersive scenarios, each lasting approximately 2 weeks. For VR OO, there were 3 iterations, each lasting 2-3 weeks, given its larger project timelines and funding availability.
VR SRA User Testing
Twenty-nine participants took part in the VR SRA user testing. This included 5 Medical Students (17%), 3 Nursing Students (10%), 3 Registered Nurses (10%), 3 Nurse Educators (10%), 3 Social Workers (10%), 2 Physicians (7%), 2 Patient Engagement Facilitators (7%), 1 Psychiatry Residents (3%), 1 Child and Youth Counselors (3%), and 6 (21%) participants who selected ‘other’.
Combining both immersive and non-immersive data, 27 participants (96%) agreed/strongly agreed that this tool was useful for learning how to conduct a SRA (n=28). Furthermore, 26 participants (93%) agreed/strongly agreed that this tool will help them in their practice (n=28). Participants were asked four accessibility questions during this user testing process. The question that received the most negative feedback was: the ‘hit area size’ was easy to access (size of the asset to select). 5 participants (19%) disagreed (n=26), and changes were made accordingly during the user testing process. Overall, all participants (100%) agreed/strongly agree that the training was engaging (n=28) and 24 participants (86%) agreed/strongly agreed that it met their expectations (n=28).
Participants rated the extent to which each learning objective was achieved using a 5-point Likert scale (1 = not at all, 5 = to a great extent). Based on self-reported confidence, 21 participants (75%) indicated that they felt able to appraise which collected factors were modifiable in a patient’s life (n=28). A large majority of participants (27, 96%) reported confidence in organizing collected factors into the P4 Screener categories (n=28). Similarly, 24 participants (96%) reported feeling confident in their ability to identify risk and protective factors through a suicide risk assessment (n=25). Finally, 22 participants (82%) reported confidence in their ability to demonstrate the process of building a therapeutic alliance with a patient (n=27).
VR OO User Testing
Twenty-nine participants took part in the VR OO user testing. This included 6 Registered Nurses (21%), 5 Social Workers (17%), 4 Pharmacists (14%), 3 Physicians (10%), 3 Educators (10%), 2 Occupational Therapists (7%), 2 Behavior Therapy Students (7%), 1 Peer Support Worker (3%), 1 Program Assistant (3%), 1 Behaviour Therapist (3%), and 1 Nursing Student (3%).
Combining both immersive and non-immersive data, 27 participants (93%) agreed/strongly agreed that this tool was useful for learning how to manage an opioid overdose (n=29). Furthermore, 21 participants (72%) agreed/strongly agreed that this tool will help them in their practice (n=29). Participants were asked four accessibility questions during this user testing process. The question that received the most negative feedback was: the labels were clearly visible and easy to read. 5 participants (17%) disagreed (n=29), which was flagged during user testing, and appropriate adjustments were made. Overall, 27 participants (96%) agreed/strongly agree that the training was engaging (n=28) and 26 participants (90%) agreed/strongly agreed that it met their expectations (n=29).
Participants rated the extent to which each learning objective was achieved using a 5-point Likert scale (1 = not at all, 5 = to a great extent). Based on self-reported confidence, 21 participants (81%) indicated that they felt able to assess a collapse for safety (n=26). Similarly, 22 participants (85%) reported feeling confident in their ability to identify an opioid overdose and call for help (n=26). The lowest-rated learning objective was administering the required treatment and monitoring patient response, with 18 participants (69%) reporting confidence in their ability to perform this task (n=26). Finally, 20 participants (77%) reported feeling confident in their ability to support a patient following an overdose (n=26).
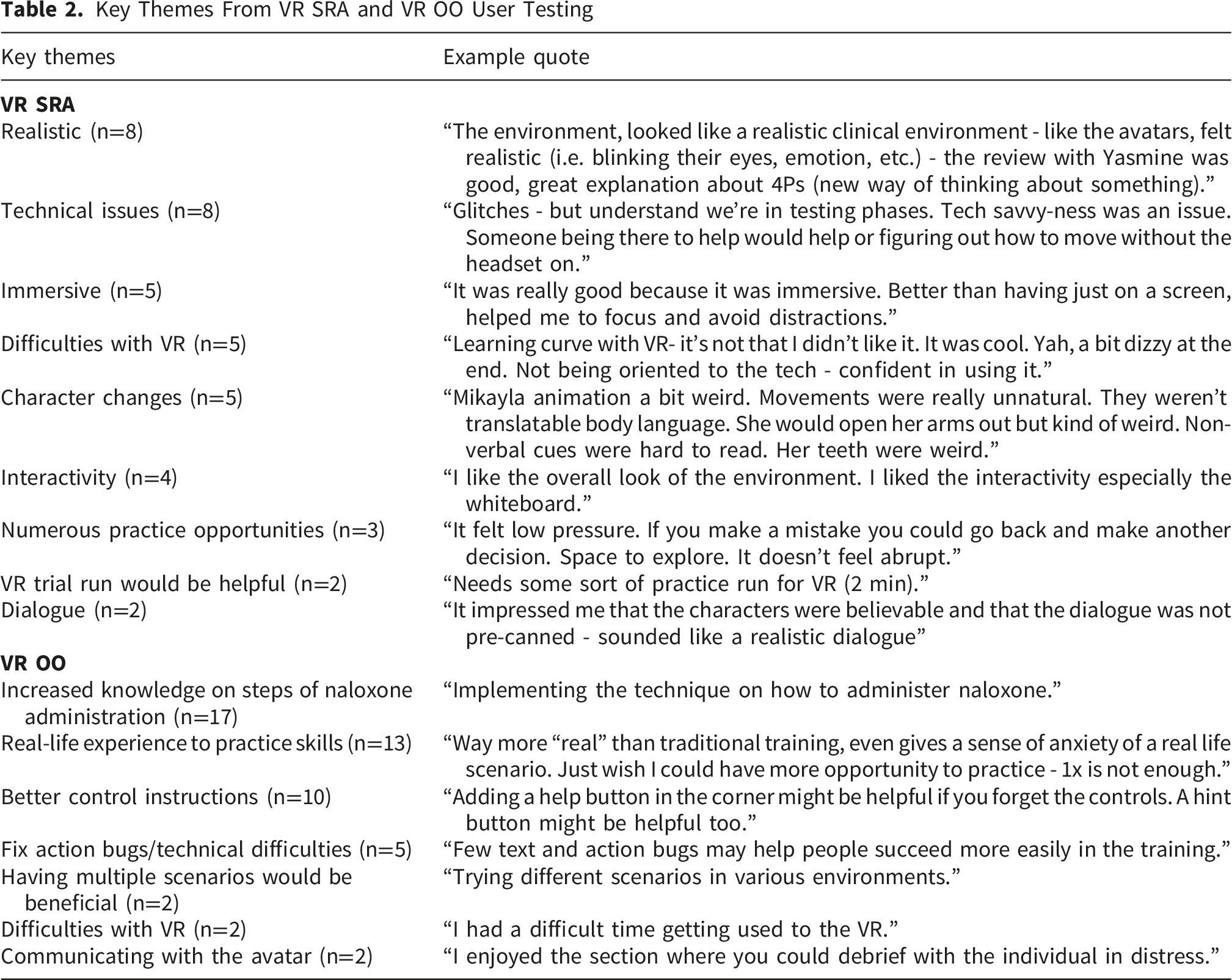
Qualitative Data
Key Themes From VR SRA and VR OO User Testing
In conclusion, the evolving landscape of innovation in medical education holds great promise for immersive and accessible training opportunities, bridging the gap between traditional educational approaches and those enhanced by novel technology. Immersive VR offers an engaging, gamified, and psychologically safe environment where learners can make mistakes, reflect and hone skills through deliberate practice. 20 Prior research suggests that VR-based simulation may offer economic advantages over traditional in-person simulation methods; however, cost-effectiveness was not evaluated in the current study and should be examined in future comparative research.20,21 This paper presents a transferable methodological approach that operationalizes rapid design thinking for VR simulation development in psychiatric education, providing practical tools and decision pathways that educators can adapt to their local contexts.
Using a rapid design thinking approach, both VR SRA and VR OO demonstrated alignment with their intended design and learning objectives based on user testing feedback. User testing showed strong learner reception, realistic scenarios, and a need for support adapting to VR.
Although this project was conducted within a specialized mental health hospital with an established simulation center and embedded UX/UI expertise, several elements of the development approach are readily transferable to institutions with fewer resources. Central to the methodology was the use of rapid design thinking, characterized by iterative prototyping, frequent user feedback, and early testing with representative end users. These processes emphasize structured stakeholder engagement rather than reliance on physical simulation infrastructure. Additional transferable components include the intentional integration of interprofessional perspectives, early incorporation of PWLE input, and the use of structured user testing to refine narrative flow, usability, and perceived realism.
While the full development process benefited from multidisciplinary expertise, the methodology can be replicated at a more modest scale with a defined set of minimum requirements. At a foundational level, institutions would require access to standalone virtual reality hardware, basic technical support for device management and deployment, and subject matter expertise to ensure clinical accuracy and alignment with learning objectives. Although dedicated UX/UI designers and simulation educators enhanced development efficiency and fidelity in this project, similar functions could be fulfilled through external consultants, shared institutional resources, or targeted short-term collaborations. Likewise, content validation does not necessitate a formal simulation center and may be achieved through smaller expert review panels or advisory groups.
Several constraints and limitations should be acknowledged. The custom, avatar-based VR simulation development process may not be generalizable to all types of VR training, and rapid technological advancements could affect its long-term relevance. Additionally, reliance on an external vendor restricted the number of iterative changes due to budgetary constraints, and future modifications would require ongoing financial investment. Other limitations include the single-site design, small sample size, use of a non-validated survey instrument, and the overall cost of VR technology, which may hinder scalability and implementation across institutions. Although this work was developed within a single institutional context, which may limit generalizability, the use of VR partially mitigates this concern by enabling standardized dissemination across settings. These two simulation software programs have been shared with other institutions at local, national, and international levels for download on their own VR headsets, allowing learners in diverse contexts to engage with an identical training experience. Future multicenter studies are needed to formally evaluate implementation and outcomes across different healthcare environments. This study did not include a formal cost or cost-effectiveness analysis; therefore, no conclusions can be drawn regarding the economic impact of the VR simulations. Furthermore, the accessibility of VR for individuals with disabilities has not been evaluated. While accessibility principles informed the design process and several accessibility features were implemented, formal evaluation of accessibility outcomes among users with disabilities was beyond the scope of this study and represents an important area for future research. While limitations inherent in rapid design approaches may arise, these can be mitigated by adopting a compassionate stance and integrating DEI principles throughout the development process. An additional limitation relates to potential selection bias in the user testing sample. Participants who volunteered for the study may have been more technologically comfortable or more positively disposed toward virtual reality–based training than the broader target population. This self-selection may have influenced engagement with the simulations and self-reported outcomes, potentially limiting the generalizability of findings. Future studies should seek to include participants with a wider range of technological familiarity and attitudes toward VR, as well as comparative designs, to better assess acceptability and impact across diverse learner groups.
The creation of VR simulations for psychiatric emergencies is a multifaceted process requiring an array of human and technological resources. Rapid design thinking serves as an effective framework for designing and developing VR simulations, as it gives educators and key stakeholders the ability to innovate and accelerate the development and implementation of prototypes, while maintaining learner-centered solutions. As VR use expands within medical education, this paper offers a practical guide for creating an avatar-based VR simulation in psychiatric training.
Supplemental Material
Supplemental material - Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies
Supplemental material for Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies by Fabienne Hargreaves, Rachel Antinucci, Michael S. B. Mak, Stephanie Sliekers, Ahmed N. Hassan, Sanjeev Sockalingam, and Petal S. Abdool in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental material - Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies
Supplemental material for Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies by Fabienne Hargreaves, Rachel Antinucci, Michael S. B. Mak, Stephanie Sliekers, Ahmed N. Hassan, Sanjeev Sockalingam, and Petal S. Abdool in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental material - Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies
Supplemental material for Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies by Fabienne Hargreaves, Rachel Antinucci, Michael S. B. Mak, Stephanie Sliekers, Ahmed N. Hassan, Sanjeev Sockalingam, and Petal S. Abdool in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental material - Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies
Supplemental material for Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies by Fabienne Hargreaves, Rachel Antinucci, Michael S. B. Mak, Stephanie Sliekers, Ahmed N. Hassan, Sanjeev Sockalingam, and Petal S. Abdool in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental material - Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies
Supplemental material for Using Rapid Design Thinking to Develop Virtual Reality Simulations for Managing Psychiatric Emergencies by Fabienne Hargreaves, Rachel Antinucci, Michael S. B. Mak, Stephanie Sliekers, Ahmed N. Hassan, Sanjeev Sockalingam, and Petal S. Abdool in Journal of Medical Education and Curricular Development.
Footnotes
Ethical Considerations
Ethics approval was obtained through Quality Project Ethics Review from the Centre for Addiction and Mental Health (QPER # 2022_018 and # QPER_66).
Consent to Participate
Participation was voluntary and detailed at the beginning of the surveys was the purpose, confidentiality statement, data storage strategy and informed consent statement.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was financially supported by the eCampusOntario initiative and the Ministry of Health Coping with Covid Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.