
Abstract
Background
Access to human tissue for medical education is becoming increasingly limited due to ethical, legal, and financial challenges. In this context, three-dimensional (3D) printing has emerged as a promising alternative, yet its educational impact requires systematic evaluation. This review assessed the effectiveness and methodological quality of 3D printed models (3DPMs) in medical education.
Methods
A systematic review was conducted following PRISMA guidelines. PubMed, Web of Science, and Scopus were searched through December 2024 for intervention studies (randomized controlled trials, single-group designs, non-randomized comparisons) employing 3DPMs among medical students, residents, or physicians. Quality was appraised using the Medical Education Research Study Quality Instrument (MERSQI), and educational outcomes were categorized by Kirkpatrick levels.
Results
Sixty-seven studies (5,329 participants) were included. At Kirkpatrick Level 1 (Reaction), 71.6% reported high learner satisfaction; 85.1% demonstrated significant knowledge/skill improvements (Level 2), and 56.7% observed concurrent gains. Only two studies assessed behavioural change (Level 3), and none evaluated patient or healthcare outcomes. The mean MERSQI score was 12.01 ± 1.95, indicating predominantly moderate quality; 69.8% were randomized trials. Fused deposition modeling was the most common printing technology, and the heart was the most frequently printed organ. Cognitive strategies underpinned nearly all interventions.
Conclusions
3DPMs consistently enhance satisfaction and knowledge in medical education, and there is growing evidence of skill transfer. However, higher-level behavioral and patient outcomes remain largely unexplored, and the quality of existing studies is predominantly moderate. Future research should focus on advanced Kirkpatrick levels and employ more rigorous designs to fully validate the educational benefits.
Keywords
Introduction
Modern medical education depends on diverse educational resources including cadaveric dissection, anatomical models, simulation tools, and digital media as fundamental components for developing students’ clinical competencies. 1 Access to these resources is a significant challenge for many medical schools, not only for financial reasons, but also for various other reasons, including ethical, legal, and cultural. Especially, the access to human tissue is faced with many limitations that create serious problems for medical educators in some countries and cultural circles. However, the development of Three-dimensional (3D) printing has created a new learning and teaching tool for medical education.2,3
3D printing is an additive manufacturing technique that turns a digital 3D model into a physical object. 4 Guided by computer instructions, material is deposited in successive layers, building up the item until it precisely replicates the on-screen blueprint. Common printing materials include strong nylon, gypsum, aluminum, textile-based substances, and polylactic acid (PLA). 5 3D technology is related to visualization, a two-dimensional (2D) image can be seen as a flat object, while a 3D image provides a deeper effect and challenges our brains to better understand. 6
This technology is used in various fields including architecture, mechanical engineering and design. Although 3D printing entered medical sciences in the mid-1980s, 7 its widespread adoption in medical education is recent. Dingyuan Jiang et al reported that annual publications on this topic remained low1-6 before 2010, accelerated from 2016 to a peak of 34 in 2019, plateaued during 2020–2021, then resumed growth to a high of 46 in 2024. Cumulative publications rose from 1 in 2010 to 302 by 2025. 8 3D printing technology is often used for clinical purposes, allowing doctors and surgeons to perform more accurate reconstructions of eye disorders, 9 cerebral arteriovenous malformation, 10 and tibial plateau fractures, 11 also, with these models, doctors and surgeons can explain the patient’s illness well and improve the doctor-patient relationship and increase the patient’s trust in the treatment process. 10
The applications of 3D printing models have been investigated in most systematic reviews, primarily in surgery, whereas the impact of their use in medical education has received little attention. Thus, a comprehensive and systematic study must investigate the effects of 3D printing on different levels of medical education. We conducted a systematic review to answer 2 research questions • Q1: What is the impact of 3D printing interventions in medical education? • Q2: What is the quality of 3D printing intervention studies in medical education?
Methods
This systematic review was conducted to evaluate the impact of 3D printers on medical education. The report follows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist, which provides a standardized framework for reporting systematic reviews and meta-analyses. The study protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) (Registration Number: CRD420261386915, Date: 05 May 2026).
Data Sources
The Web of Science, PubMed, and Scopus databases were searched for articles published through December 23, 2024. In addition, the reference lists of included studies and conference proceedings were screened. We contacted the authors of the included articles to obtain further information.
Search Strategy
The search strategy was built around four main conceptual blocks: (1) educational activities, (2) medical education domains, (3) 3D printing technology, and (4) target learner populations. The following free-text terms and controlled vocabulary were used across databases (adjusting syntax for each platform, e.g., PubMed, Web of Science, and Scopus). For the education block, the terms included “Training”, “Learn”, “Teach”, “Education”, combined with domain-specific terms such as “Medical education”, “Basic science”, “Clinical skill”, “Clinical competence”, and “Surgery”. For the technology block, we used “3D printing”, “three-dimensional printing”, “additive manufacturing”, and “3D printed”. For the learner population, we searched for “Medical student”, “MD student”, “Undergraduate”, “Postgraduate”, and “Physicians”. In databases that support thesaurus searching, MeSH terms (e.g., “Education, Medical”, “Printing, Three-Dimensional”, “Students, Medical”) were exploded and combined with title/abstract field searches. All four blocks were combined with the Boolean operator AND.
Inclusion and Exclusion Criteria
Inclusion criteria encompassed all full-text studies that investigated the impact of 3D printing in medical education. This included intervention studies such as randomized controlled trials, single-group posttest-only designs, single-group pretest and posttest designs, and non-randomized studies with two groups.
Exclusion criteria were applied to review and meta-analysis studies, letters to the editor, observational studies without educational intervention, case reports, case series, qualitative studies, and studies focused on non-medical education populations (such as dentistry and nursing).
Study Selection
All retrieved records were imported into the Document Manager (EndNote X7). After removing duplicate entries, the titles and abstracts of the literature records were screened by two authors (MB and AS) independently, based on preestablished inclusion criteria from the PICOS framework, to exclude clearly irrelevant records. Following this, the full texts of the remaining records were examined in detail to select those that met the inclusion criteria. In the event of a divergence during the literature selection process, the final decision was made through consultation with the third author (EJ).
Inter-rater agreement during title/abstract screening was assessed using Cohen’s kappa coefficient, yielding a value of 0.87 (95% CI: 0.82–0.92), indicating near-perfect agreement. Disagreements occurred for 47 of 1,770 screened records (2.7%). Full-text review disagreements involved 12 of 91 reports (13.2%). The third author (EJ) was consulted for arbitration on 8 occasions (0.45% of screened records) to resolve persistent disagreements, primarily concerning the applicability of the educational intervention criterion.
Data Extraction
Two reviewers (S.B. and F.E.) independently extracted data from each eligible study using a standardized, pre-piloted extraction form. Any disagreements were resolved through discussion until consensus was achieved; if necessary, a third reviewer (AS) was available for arbitration. The following information was collected from each article: • First author (year of publication) • Country where the study was conducted • Target group (e.g., medical students, residents, fellows) • Study design • Number of participants • Anatomical region or organ(s) featured in the 3D printed model (3DPM) • Type of 3D printer • Type of printing material • Pedagogical strategy employed • Kirkpatrick level(s) of educational outcome • Domain(s) assessed (e.g., knowledge, skills, attitudes) • Main finding(s)
After extraction, the data were collated and synthesized to address the review questions.
Quality of the Studies
The quality of the studies was assessed using a checklist called the Medical Education Research Quality Instrument (MERQI). 12 This checklist includes 10 items categorized into 6 different domains, with each item having a unique set of answers that yield specific scores. Each item can receive a maximum score of 3. The total points can range from a minimum of 4 to a maximum of 18. Based on the authors’ agreement, scores between 5 and 9 indicate low quality, scores from 10 to 14 indicate moderate quality, and scores above 15 indicate high quality for the articles.
Definition
To identify the pedagogical and andragogical approaches best suited for 3D printing in medical education, it is necessary first to define the learning domains. The three learning domains—cognitive, affective, and psychomotor—describe what learners should be able to do or how they should change as a result of instruction. These domains inform pedagogical design. In contrast, the Kirkpatrick Evaluation Model serves a different purpose: it provides a framework for measuring the effectiveness of instruction across four levels (Reaction, Learning, Behavior, Results). For example, a single educational intervention could thus be designed using cognitive domain principles while being evaluated using Kirkpatrick Level 2 (knowledge gain). These frameworks are complementary.
Cognitive Domain
This domain encompasses learning skills related to mental processes and thinking. It follows a hierarchy in which learners process information, build understanding, apply knowledge, solve problems, and conduct inquiry. Bloom’s taxonomy describes six levels of increasing cognitive complexity: knowledge, comprehension, application, analysis, synthesis, and evaluation. 13
Affective Domain
This domain addresses educational objectives concerned with attitudes, emotions, interests, and values. It is organized into five sub-domains that represent a progression of internalization: (1) Receiving, (2) Responding, (3) Valuing, (4) Organization, and (5) Characterization (13).
Psychomotor Domain
This domain focuses on physical skills, reflex actions, and interpretive movements. It involves the physical encoding of information and the coordinated use of gross and fine muscles to express or interpret concepts. Dave’s (1975) taxonomy structures this domain into five levels: (1) Imitation, (2) Manipulation, (3) Precision, (4) Articulation, and (5) Naturalization. 13
Kirkpatrick Evaluation Model
The Kirkpatrick pyramid is a globally recognized method for evaluating training and learning outcomes. It assesses programs across four levels:
Reaction: the degree to which participants find the training favorable, engaging, and relevant;
Learning: the degree to which participants acquire the intended knowledge, skills, attitudes, confidence, and commitment;
Behavior: the degree to which participants apply what they learned in their actual practice;
Results: the targeted organizational or performance outcomes that occur as a result of the training. 14
Results
Study Characteristics and Kirkpatrick-Level Outcomes
The 67 included studies encompassed 5,329 participants (undergraduate medical students, residents, and attending physicians; one study did not report participant numbers) (Figure 1). Overall, the vast majority demonstrated favorable educational outcomes with 3DPMs. At Kirkpatrick Level 1 (Reaction), 48 studies (71.6%) reported enhanced learner satisfaction and engagement; learners consistently rated 3D printed materials as superior to 2D images, atlases, and even cadaveric or plastinated specimens in terms of realism and ease of understanding. Knowledge and/or skill improvements (Level 2, Learning) were documented in 57 studies (85.1%), with most showing that 3DPM groups outperformed traditional teaching controls on post-test scores, knowledge retention, and spatial anatomical comprehension. Concurrent improvements in both reaction and learning were observed in 38 studies (56.7%). Only two studies addressed behavioural outcomes (Level 3, Behaviour): one study combined behaviour with knowledge acquisition,
15
while another evaluated reaction, learning, and behavior simultaneously, marking the only study to cover three Kirkpatrick levels.
16
These two investigations respectively demonstrated enhanced bronchoscopy skills with improved procedural safety, and better preoperative planning aligned with clinical standards. No study assessed patient or healthcare outcomes. While the majority of findings favored 3D printing, a few comparisons showed equivalent results between models and alternative methods, suggesting that 3DPMs are at least as effective as existing educational tools. Collectively, these results provide strong evidence for the educational value of 3DPMs across diverse learner populations and anatomical topics. PRISMA flow diagram of the systematic review and meta-analysis selection process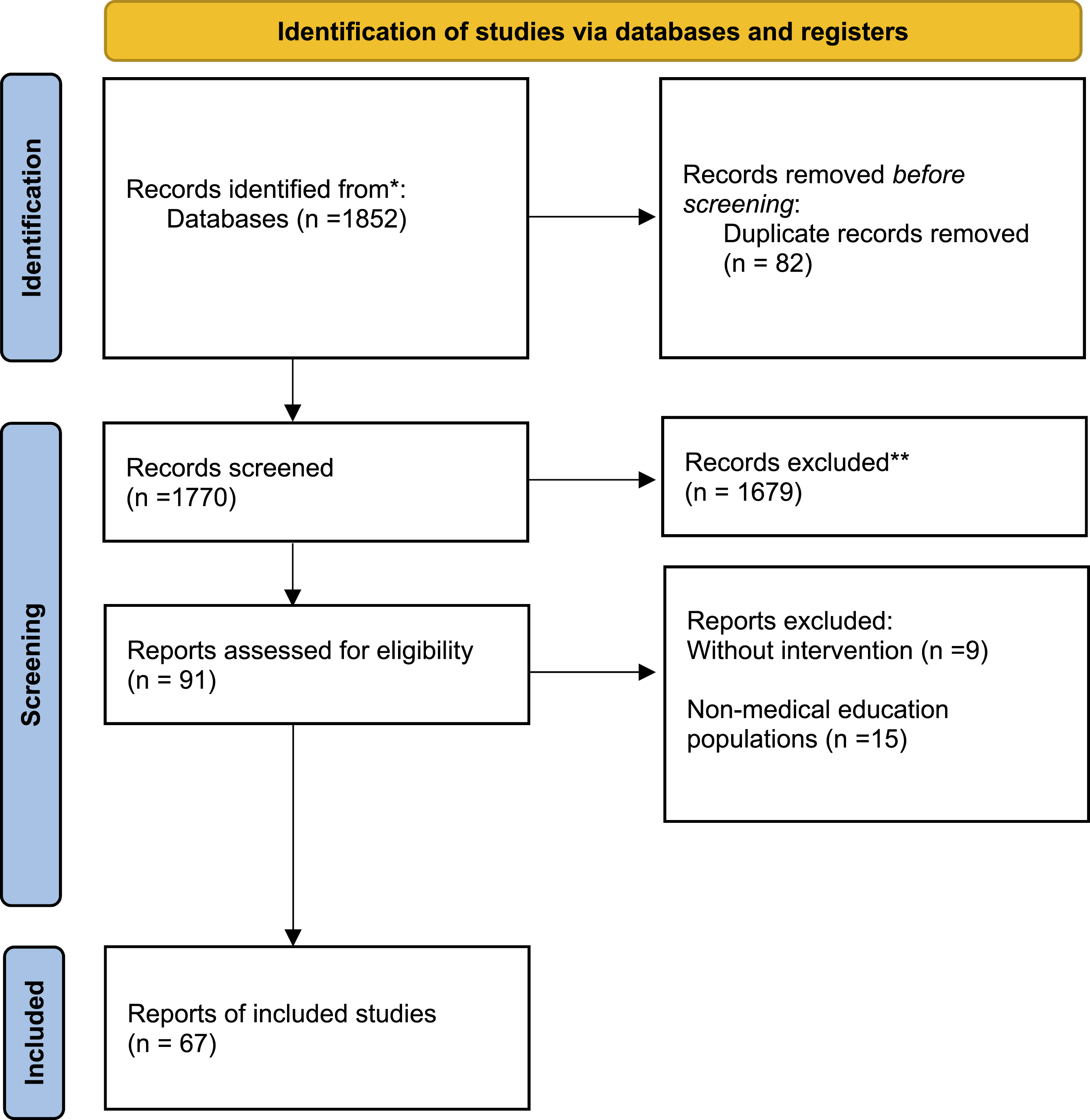
Geographical Distribution
The USA contributed the largest number of studies (n = 25), followed by China (n = 13) and Singapore (n = 5). Asian countries together provided 23 studies (including Japan, Turkey, Kuwait, South Korea, and Iran with one each). European contributions included 3 studies from the United Kingdom, 2 each from Italy, France, and Switzerland, and single studies from Spain, Germany, Ireland, and Greece. Canada and Australia contributed 3 and 2 studies, respectively, while Brazil and New Zealand had one each. Two studies were multinational: Yoo et al (2017) 17 (USA, Canada, South Korea) and AlAli (2018) 18 (Kuwait, United Kingdom).
Subject Areas and Printed Organs
Characteristics of the 67 Included Studies
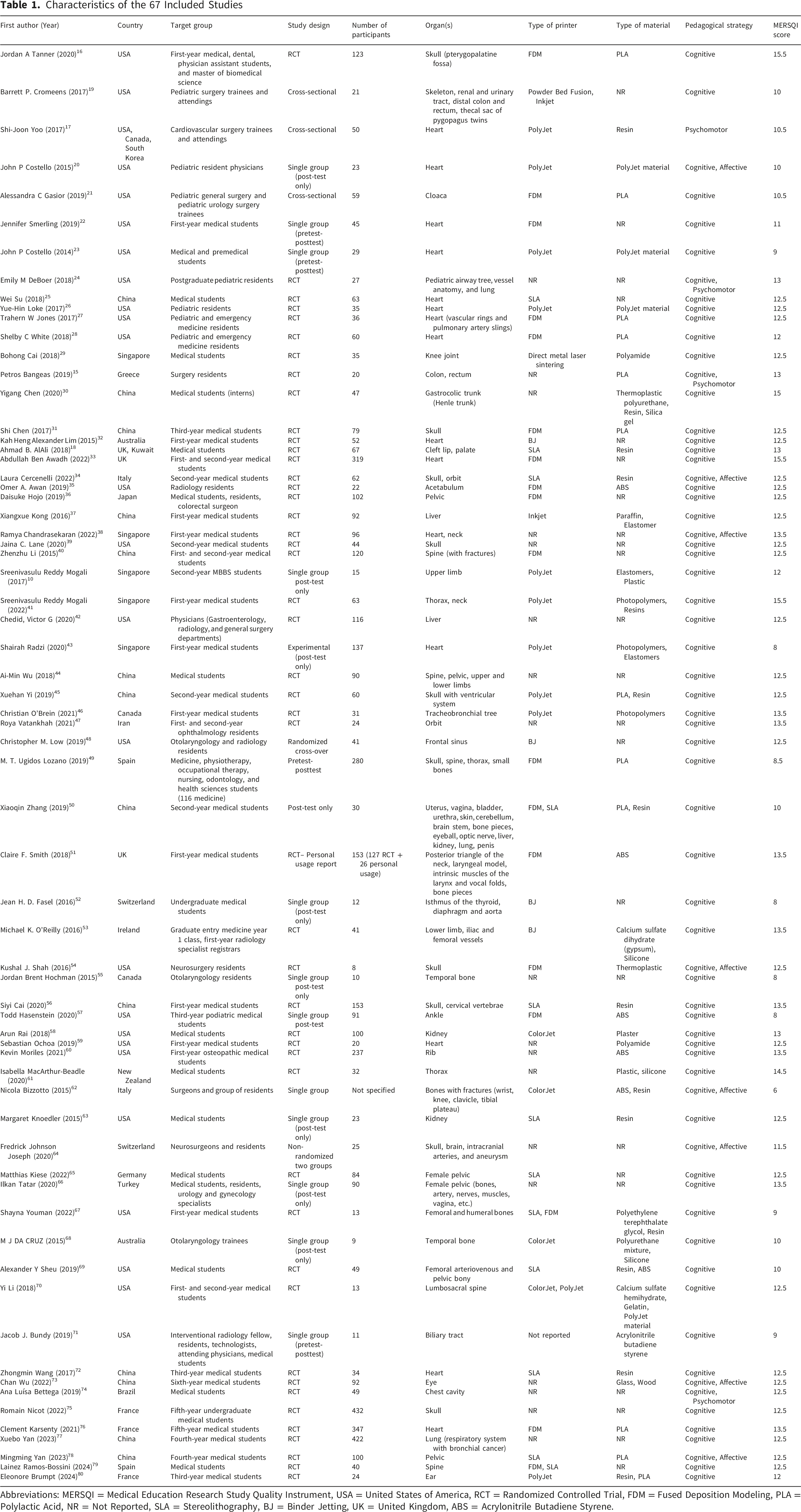
Abbreviations: MERSQI = Medical Education Research Study Quality Instrument, USA = United States of America, RCT = Randomized Controlled Trial, FDM = Fused Deposition Modeling, PLA = Polylactic Acid, NR = Not Reported, SLA = Stereolithography, BJ = Binder Jetting, UK = United Kingdom, ABS = Acrylonitrile Butadiene Styrene.
Printing Technologies and Materials
Five distinct 3D printing technologies were reported. Fused Deposition Modeling (FDM) was the most utilized (17 studies), followed by Stereolithography (SLA) (12 studies) and PolyJet (11 studies). Binder Jetting (BJ) (also termed ColorJet or InkJet) was used in 10 studies, while Selective Laser Melting (SLM) appeared in two forms: Powder Bed Fusion and Direct Metal Laser Sintering. Printer technology or brand was not specified in 17 studies.
Thermoplastics dominated the materials: PLA in 12 articles, acrylonitrile butadiene styrene (ABS) in 7, polyamides in 2, and thermoplastic polyurethane and polyethylene terephthalate glycol in one each. Photopolymers were listed in 14 articles as resins, 4 as PolyJet materials, and 3 without specific chemical names. Elastomers appeared in six studies (three as silicone). Calcium sulfate (gypsum or hemihydrate) was noted three times, and single uses of paraffin, glass, wood, and unspecified plastics were reported. Material composition was not described in 23 studies.
Pedagogical Strategies and Participant Groups
Almost all studies (n = 66) applied a cognitive learning strategy. Affective strategies were incorporated in 8 articles, psychomotor strategies in 3, and no study combined all three domains simultaneously. One study 17 relied exclusively on a psychomotor approach.
Methodological Quality
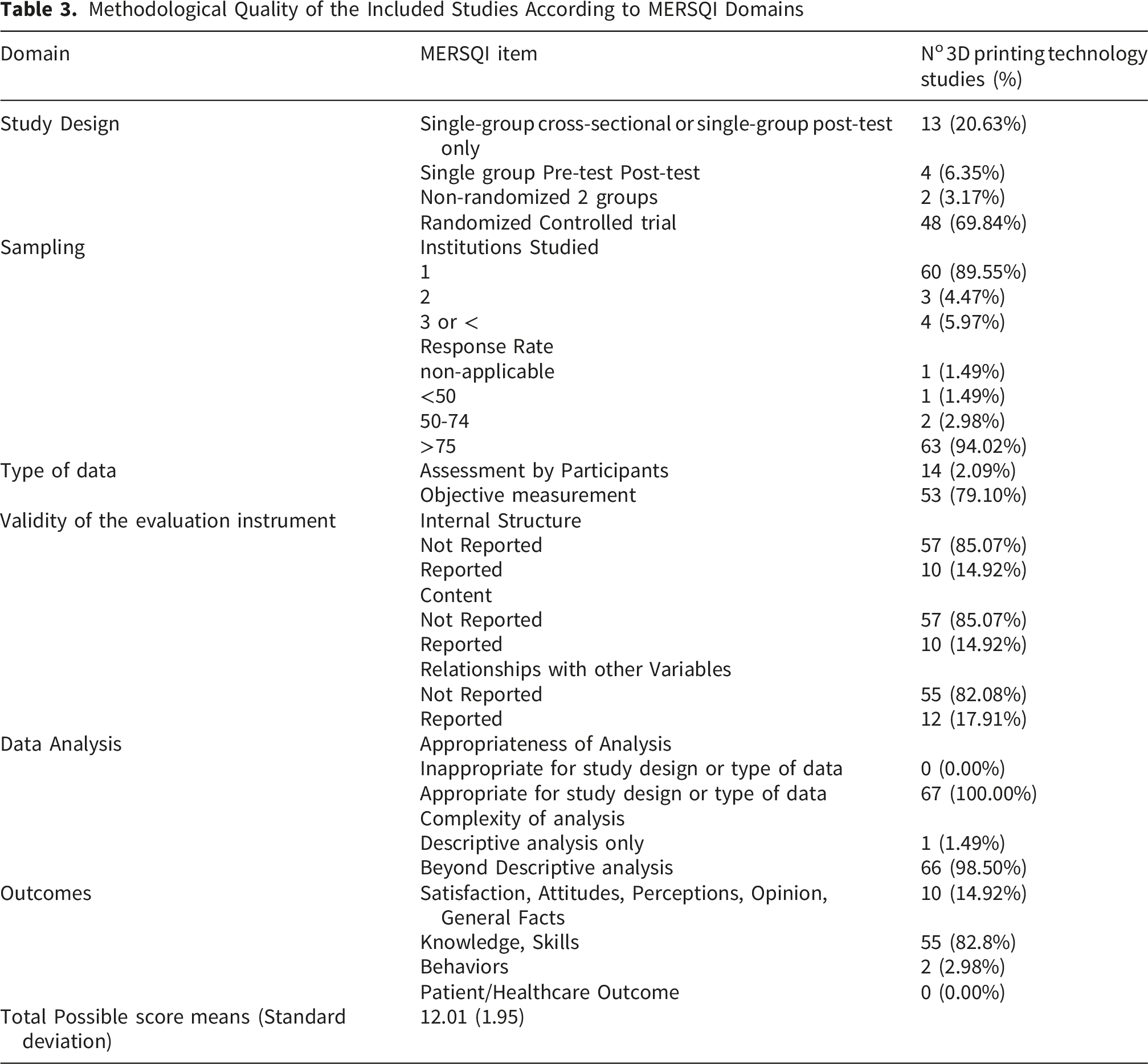
Based on the Medical Education Research Study Quality Instrument (MERSQI) scale (maximum score 18; low: 5–9, moderate: 10–14, high: ≥15), study quality was predominantly moderate. Three articles achieved the highest score of 15.5,16,33,41 and one additional study 30 scored 15, meeting the high-quality threshold. The lowest score was 6. 62 Overall, 9 studies were of low quality, 54 of moderate quality, and 4 of high quality. The mean MERSQI score was 12.01 ± 1.95.
Kirkpatrick-Level Outcomes and Summarized Main Findings

Abbreviations: 3DPM = Three-Dimensional Printed Model, 3D = Three-Dimensional, 2D = Two-Dimensional, TOF = Tetralogy of Fallot, MCQ = Multiple Choice Question, CT = Computed Tomography.
Methodological Quality of the Included Studies According to MERSQI Domains
Discussion
A skilled human force who can develop and expand the discipline of medicine needs certain competencies, including knowledge, skills, attitude, and abilities. Therefore, the best educational material should be used to engage them with problems and challenges and conceptualize these competencies in their minds Recently, 3D printing has become more popular in medical education, because it can make personal medical models with complex shapes. 81
The using of 3D printers in medical education has great potential to improve the teaching-learning process. The results of this systematic review showed that the use of 3D printers in most cases has improved the satisfaction, knowledge and attitude of medical students. Although this field is still relatively new, the results of this study showed that 3D printed products can be used as an alternative or complementary educational material in medical education. 82
The predominance of positive findings at Kirkpatrick Levels 1 and 2 in our review aligns closely with the existing evidence base, while extending it in important ways. The 2025 systematic review and meta-analysis by Guanli Xieet al., which included 33 randomized controlled trials with 2,716 medical undergraduates, reported that 3DPMs demonstrated significant advantages over control groups in theory tests of the skeletal system (Standardized mean difference (SMD) = 0.56, 95% CI 0.20–0.93) and in laboratory tests (SMD = 0.57, 95% CI 0.34–0.80), with an overall small effect size for combined outcomes (SMD = 0.26). 83 That review concluded that 3DPMs serve as a valuable adjunct to traditional teaching. However, it emphasizes that caution is warranted due to variations in model types, low study quality, and small sample sizes. 83 Our review, with twice the number of studies and a broader participant base that includes residents and attending physicians in addition to undergraduates, corroborates these effect estimates while extending their generalizability beyond undergraduate populations.
In their 2023 systematic scoping review, Carlos M. Ardila et al assessed the effectiveness of 3D models in medical education. 84 They found that medical students exhibited greater learning outcomes in terms of skills and knowledge when using 3D systems. 84 Our findings support this conclusion and extend it to a broader range of outcome areas and learner levels.
Yi et al conducted a systematic review on randomized controlled studies to examine the effectiveness of 3DPMs of the ventricular system for anatomy education. 45 They found that the group using 3DPMs showed the greatest improvement in knowledge and satisfaction, followed by the group using 3D images, and finally the group using 2D Computed topography (CT) images. 45 These findings, which are integrated into our analysis, reflect a consistent pattern: 3DPMs consistently outperformed 2D methods and were at least as effective as other 3D visualization approaches.
A key finding from our review is the almost complete lack of higher-level Kirkpatrick outcomes in the literature. Only two studies (3.0%) evaluated behavioral change (Level 3), and none assessed patient or healthcare outcomes (Level 4), which is a significant limitation. Although improvements in satisfaction and knowledge are important steps toward practice change and benefiting patients, the ultimate goal of medical education is to enhance clinical care. Similarly, the reviews by Li et al (2025) and Asif et al (2021) emphasized the need for studies with long-term follow-up and clinically assessed outcomes. Until such evidence is available, the argument for widely integrating 3D printing into medical curricula while educationally compelling remains based on an incomplete evidence base.83,85
Our finding that 66 of 67 studies employed a cognitive learning strategy, with only eight incorporating affective approaches and three using psychomotor strategies, is noteworthy. It suggests that the current application of 3D printing in medical education is heavily skewed toward knowledge transmission, with relatively underdeveloped applications in attitudinal and skills-based domains. Given that 3DPMs offer tangible, hands-on learning opportunities, the paucity of psychomotor applications is particularly surprising. The 2025 scoping review on 3D printing for simulation educators identified skill development as a key theme, yet also noted training gaps for educators as a barrier. 86 This may partly explain the underutilization of psychomotor and affective strategies: educators themselves may require additional training to design and implement pedagogically sophisticated 3D printed interventions. 86 Future work should explore how 3DPMs can be integrated into more comprehensive pedagogical frameworks that intentionally target all three learning domains.
Among 3D printing technologies, FDM was the most used method (17 studies), followed by SLA (12 studies) and PolyJet (11 studies). This distribution aligns with patterns reported in recent systematic reviews of 3D printing in healthcare education 86 The predominance of FDM is likely attributable to its lower cost (entry-level FDM printers range from $200–2,000 compared with $2,000–50,000 for SLA and $20,000–200,000 for PolyJet), 87 wider availability in academic institutions, and compatibility with inexpensive, biocompatible thermoplastics such as PLA. However, FDM produces models with visible layer lines and lower resolution than SLA or PolyJet, which may affect anatomical fidelity for fine structures. 88 Notably, 17 studies (25.4%) did not specify the printing technology used, and 23 (34.3%) omitted material composition.This underreporting constrains reproducibility and prevents meaningful comparison of cost-effectiveness across technologies.
Geographically, the evidence base was concentrated in high-income countries, with the USA (25 studies) and China (13 studies) together accounting for over half of the included studies. This concentration raises questions about the generalizability of findings to low-resource settings, where 3D printing might paradoxically offer the greatest benefit by circumventing the ethical, legal, and financial barriers to cadaveric dissection.
Strengths and Limitations
This review has several notable strengths. It is, to our knowledge, the largest systematic review of 3D printing in medical education conducted to date, encompassing 67 studies, 5,329 participants, and a comprehensive range of learner levels, anatomical topics, and printing technologies. The use of the MERSQI instrument allowed for standardized quality appraisal, and the application of the Kirkpatrick model provided a structured framework for categorizing educational outcomes. Our search strategy was comprehensive, spanning multiple databases through December 2024, and captured the rapidly expanding recent literature that earlier reviews could not include.
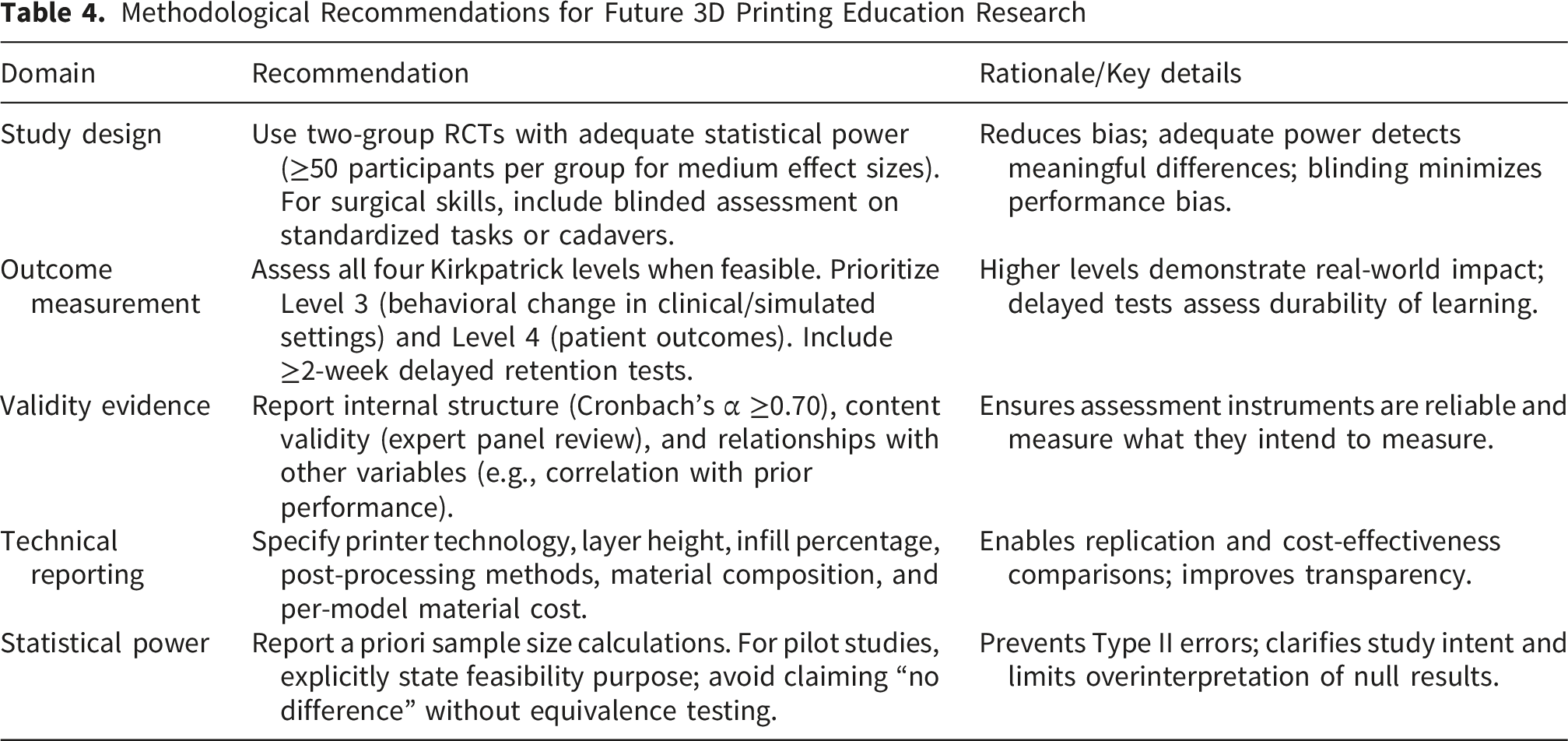
Several limitations must also be acknowledged. First, despite the large overall sample, the predominance of single-institution studies (89.6%) limits generalizability. Second, the heterogeneity of interventions, outcome measures, and learner populations precluded formal meta-analysis of pooled effect sizes. Third, the MERSQI instrument itself has limitations relevant to 3D printing research. It does not distinguish between knowledge and skill outcomes, grouping both under a single category. This is problematic because 3D printing may differentially affect these domains: our review found stronger effects for spatial anatomical understanding (a knowledge-adjacent skill) than for procedural skills. Additionally, MERSQI does not account for statistical power; an underpowered RCT (e.g., n=8 per group) receives the same study design score as a large, adequately powered trial. Among the 48 RCTs in our review, only 13 (27.1%) reported a priori sample size calculations. Furthermore, validity evidence for assessment instruments was rarely reported—only 10–12 studies (14.9–17.9%) provided any validity data, despite many using novel, ad hoc knowledge tests without psychometric validation. Fourth, the Kirkpatrick model assumes a linear, hierarchical progression from Reaction (Level 1) to Results (Level 4), implying that lower-level positive effects predict higher-level outcomes. However, our review found high satisfaction (71.6% at Level 1) and knowledge gains (85.1% at Level 2) but almost no behavioral outcomes (3.0% at Level 3), challenging this assumption. Moreover, the Kirkpatrick model does not capture unintended or negative outcomes; no study in our review systematically assessed potential harms such as cognitive overload, over-reliance on models, or opportunity costs. Fifth, publication bias cannot be excluded, as studies with null or negative results may be underrepresented in the published literature.
Methodological Guidance for Future Researchers
Methodological Recommendations for Future 3D Printing Education Research
Conclusion
This systematic review of 67 studies demonstrates that 3DPMs consistently enhance learner satisfaction and knowledge acquisition across undergraduate, postgraduate, and continuing medical education. With 85.1% of studies documenting significant improvements at Kirkpatrick Level 2 and 71.6% at Level 1, the evidence base supporting the educational value of 3DPMs is now substantial, corroborating and extending findings from recent systematic reviews. The technology is often superior to traditional 2D teaching methods and offers practical advantages like tactile learning, reusability, and the ability to represent complex or rare pathologies. However, the evidence remains constrained by moderate methodological quality, a near-total absence of behavioural and patient-level outcomes, and limited investigation in resource-varied settings. As 3D printing technology becomes more accessible and affordable, medical educators and researchers face the challenge of advancing beyond simply demonstrating that these models are well-received and effective for education. They need to establish that these models truly make a significant impact on clinical practice and patient care.
Supplemental Material
Supplemental Material - A Systematic Review of Three-Dimensional Printing in Medical Education: Educational Impact and Methodological Quality
Supplemental Material for A Systematic Review of Three-Dimensional Printing in Medical Education: Educational Impact and Methodological Quality by Amir Mohammad Salehi, Shayan Bahadivand Chegini, Fatemeh Esmaeili, Ensiyeh Jenabi, Mahnaz Khatiban, Mohammad Ahmadian, Mohamad Reza Bastan in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval for this study was obtained from the Ethics Committee of the Hamadan University of Medical Sciences, which approved the protocol of this study (IR.UMSHA.REC.1400.112).
Author Contributions
Conceptualization: EJ and AS.; methodology: SBC and AS.; data curation, SBC, FE and MA.; writing—original draft preparation, AS and MB.; writing—review and editing: All of the authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The protocol of this study was supported by Student research center of Hamadan University of Medical Sciences with code 140103242075.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.