
Abstract
Background and Aims
When it is positive, humor can improve psychological well-being and social interactions, but when it is negative, it can also be harmful. As such, it is important to better understand what type of humor individuals with different neurodevelopmental conditions tend to use. This study investigated the use of four different humor styles, that is, affiliative, self-enhancing (both positive), aggressive, and self-defeating (both negative) humor, in individuals with Autism Spectrum Condition (ASC), Down syndrome (DS), and Williams syndrome (WS). Moreover, it investigates the relation of potential differences in humor styles with social, emotional, and behavioral difficulties and strengths.
Methods
Parent-reported questionnaires were used to assess humor styles, social difficulties, and mental health in young individuals (5–25 years old) with ASC (N = 31), DS (N = 82), or WS (N = 34).
Results
The results revealed that autistic individuals are reported to use more self-defeating humor than both individuals with DS and WS, which seems to be related to increased externalizing conduct problems, as well as less affiliative humor which was associated with fewer emotional difficulties, better social cognition, and greater prosocial behavior.
Conclusions and implications
These results are discussed in relation to how humor styles use enhances our understanding of humor in neurodevelopmental conditions.
Keywords
Introduction
Humor plays an important role in humans’ everyday communication and serves a variety of social, cognitive, and emotional functions. Indeed, research has shown that humor development improves socio-cognitive skills (Soy Telli & Hoicka, 2022), fosters social interactions by improving self-confidence (Nezlek & Derks, 2001), and promotes reciprocal liking (people typically like those who make them laugh) (Treger et al., 2013), and contributes to group cohesiveness (Martin et al., 2003). More importantly, humor contributes to life satisfaction (Peterson et al., 2007) and can have a positive impact on psychological well-being (Curran et al., 2021; Kuiper, 2012; Papousek, 2018). Indeed, the production of humor is a powerful means of down-regulating negative emotions in oneself (Kugler & Kuhbandner, 2015; Samson & Gross, 2012; Samson et al., 2014) and in others (Horn et al., 2018; Papousek, 2018). Moreover, it can also be used to up-regulate positive emotions (Geisler & Weber, 2010; Samson & Gross, 2012; Samson et al., 2014), which are widely known as having a strong, positive impact on well-being (Fredrickson, 2004).
However, all of these positive effects of humor on well-being seem to occur under one condition: humor has to be benevolent, harmless, and benign. But humor also has a dark side, when it is depreciating, hostile, and harmful, and can negatively impact psychological well-being (Samson & Gross, 2014). Depreciating mockery can affect negatively the targeted person, and this can have strong consequences such as the development of gelotophobia, which is the fear of being laughed at (Ruch & Proyer, 2008), leading individuals to experience high fear and anger when exposed to ridicule (Platt, 2008) or to difficulties developing close relationships (Brauer et al., 2020). Whether humor plays a positive or negative role in psychological well-being depends notably on the nature of the specific type of humor involved, and more specifically on whether it is good- or ill-intentioned and whether it is well or badly perceived.
Martin et al. (2003) defined four humor styles, on the basis of a 2 × 2 categorization. The styles are thus defined according to whether the type of humor is interpersonal (i.e., directed toward others and with the purpose of increasing or decreasing others’ psychological state and one's relation with others) or intrapersonal (directed toward oneself and with the purpose of increasing one's own well-being). The second dimension is linked to whether individuals use humor that is rather positive (benevolent, harmless, and benign), or negative (detrimental, hostile, and harmful). The four resulting humor styles are as follows (Martin et al., 2003): Affiliative humor (interpersonal and positive) represents the tendency to say funny things, amuse others, engage in humorous interactions with others to enhance the relationship and reduce potential tensions. It is intended to make others laugh in a benevolent and benign manner. This style of humor correlates positively with cheerfulness, extraversion, openness to experience, self-esteem, social intimacy, and psychological well-being, and correlates negatively with seriousness, bad mood, anxiety, and depression. Aggressive humor (interpersonal and negative) represents a form of humor produced to the detriment of others. It can be hurtful, as the one engaging in such humor will produce hostile mockery, ridicule, or derision. It can also be used as a manipulative tool, by threatening the other to get ridiculed. Such humor correlates positively with neuroticism, hostility, and aggression, and negatively with agreeableness, conscientiousness, and seriousness. Self-enhancing humor (intrapersonal and positive) is produced to enhance one's own well-being, by using humor to cope with stress, and regulate one's own emotions. Individuals who are high on this dimension tend to generally look at life, its incongruities and adversities, with an amused and humorous eye. It correlates positively with cheerfulness, optimism, self-esteem, well-being, openness, and extraversion, and negatively with bad mood, depression, anxiety, and neuroticism. Self-defeating humor (intrapersonal and negative) involves self-disparaging humor, that is, trying to integrate or gain approval by letting others mock and ridicule oneself. It also includes a tendency to avoid and deny the problems by engaging in humorous behavior to hide negative feelings (which is different from positive humorous coping behavior, since here it is a matter of denial and not reappraisal). It correlates positively with bad mood, depression, anxiety, neuroticism, hostility, and aggression, as well as with shyness (Hampes, 2006), and negatively with psychological well-being, self-esteem, agreeableness, and conscientiousness.
In terms of the relation between humor and psychological well-being, it appears that it is positive humor, that is, affiliative and self-enhancing humor, that has a positive impact. Samson and Gross (2012) have shown that positive (i.e., benevolent) humor was substantially more efficacious than negative humor in down-regulating negative emotions. Cann and Collette (2014) showed that only self-enhancing humor was related to positive stable affect and thus to psychological well-being (Fredrickson, 2004), while Kuiper (2012) highlighted that only positive humor contributes to resilience. Overall, research has widely confirmed that affiliative and self-enhancing humor have a positive impact on well-being, whereas self-defeating humor has a negative impact on well-being (Martin et al., 2003; Schneider et al., 2018), and this appears to be true independently of culture and age (Jiang et al., 2020). Moreover, a higher use of self-defeating humor and lower use of self-enhancing and affiliative humor correlate positively with increased depressive symptoms (Frewen et al., 2008).
Although research has mainly investigated the influence of humor styles on individuals’ well-being, it is also likely that well-being influences individuals’ relation toward humor. Indeed, in the broaden-and-build model, Fredrickson (2004) suggests that positive emotions and psychological well-being influence each other in a loop. Indeed, according to the model, positive emotions broaden the mind to new experiences, which contributes to building personal resources that will in turn enhance mental health and well-being. This state of enhanced health and well-being brings individuals to be more open to experiencing positive emotions, which creates a virtuous spiral. Therefore, it seems highly likely, not only that positive humor influences well-being and mental health, but also that well-being and mental health influence one's relation toward more positive and negative humor.
Humor is intrinsically social by nature. Indeed, it usually occurs in social interactions (Ruch, 2008), which might imply that individuals with higher social motivation and abilities will have a greater relationship toward humor. Additionally, humor processing requires quite high socio-cognitive skills, since the understanding of humor often relies on inferring the joker's intentions (i.e., that they have the intention to produce humor and not an unintentional mistake or a lie) (Hoicka & Gattis, 2008; Ruch, 2008). Therefore, individuals who show lower social motivation or difficulties with social cognition, such as autistic individuals might have a more conflictual or less evident relation toward humor.
Autism spectrum condition (ASC) has a median prevalence of 100 in 10,000 individuals worldwide and in Europe (Zeidan et al., 2022). The spectrum is characterized by two main criteria: difficulties in social communication and social interaction, and restrictive interests and repetitive behaviors (DSM-5-TR, American Psychiatric Association, 2022). Various theoretical accounts have been proposed to explain social communication differences in autism, including Theory of Mind or perspective-taking frameworks, which propose that differences in understanding others’ mental states may contribute to some social communication differences (e.g., Senju, 2012), as well as social motivation accounts, which propose that differences in the tendency to seek or initiate social interactions may contribute to social communication differences (Chevallier et al., 2012). However, both frameworks have been the subject of substantial debate, theoretical refinement, and empirical challenge, including questions regarding the interpretation and replicability of some influential findings (e.g., Jaswal & Akhtar, 2019; Kampis et al., 2021). In addition, studies have reported differences in emotional experiences in autism, including a greater tendency to experience negative emotions (Cai & Samson, 2025), and autistic individuals have been perceived as more serious and less cheerful than non-autistic individuals (Samson et al., 2013; Treichel et al., 2023). Importantly, these social and emotional characteristics vary considerably across individuals and are not unique to autism, making a transdiagnostic perspective particularly relevant. Such characteristics may be important for understanding individual differences in humor-related experiences, and notably, the humor styles they tend to produce (Treichel et al., 2022).
Samson et al. (2013) showed that autistic adults without intellectual disabilities scored lower than neurotypical adults in both positive types of humor (i.e., affiliative and self-enhancing humor), but no difference appeared in aggressive and self-defeating humor. They argued that the reported lower scores of autistic individuals in affiliative humor might be related to their difficulties in the social domain. Moreover, the authors pointed out that autistic individuals’ lower scores in self-enhancing humor could be related to their difficulties in regulating their emotions (Cai & Samson, 2025). It could also be argued that these results are coherent with autistic individuals’ negativity bias (Joseph & Tager-Flusberg, 1997), which may impact their general humor temperament (Samson et al., 2013; Treichel et al., 2022).
Autistic people seem to be at the opposite pole of a social motivation spectrum compared to individuals with Williams syndrome (WS) and Down syndrome (DS) (Treichel et al., 2022) who have been described as having high social motivation, which is a pronounced tendency to seek out social interactions. WS is a rare genetic disorder that concerns approximatively 1 in 10,000 births (Morris & Mervis, 2021), involving mild to moderate intellectual disabilities (Korenberg et al., 2000), that is notably characterized by a particularly high social approach tendency and an overly friendly and disinhibited personality (Järvinen et al., 2013; Jones et al., 2000). People with WS are also described as highly cheerful (Tager-Flusberg & Sullivan, 2000), and particularly expressive when it comes to positive emotions (Treichel et al., 2024). DS is a genetic disorder affecting roughly 1 in 800 births (Lanphear & Castillo, 2007) that notably involves intellectual disabilities (Antonarakis et al., 2020; Määttä et al., 2006). Individuals with DS have been described as very sociable (Porter et al., 2007) and cheerful (Grieco et al., 2015; Treichel et al., 2023). Although they differ greatly from autism on the social motivation level, WS and DS share some important similarities with autism (Klein-Tasman et al., 2009; Niego & Benítez-Burraco, 2022; Reilly, 2009). For example, individuals with WS and DS present with difficulties in social cognition and communication including Theory of Mind (Channell, 2020; Fisher & Morin, 2017; Neitzel & Penke, 2021; Tager-Flusberg & Sullivan, 2000), and in sustaining friendships (Iarocci et al., 2008; Järvinen et al., 2013). Moreover, individuals with ASC, WS, and DS all show a tendency to develop mental health problems such as anxieties, specific phobias, hyperactivity, and depression (Lai et al., 2019; Määttä et al., 2006; Stinton et al., 2010).
So far, little research has been conducted on humor in WS and DS (for reviews, see Chadwick & Platt, 2018 and Treichel et al., 2022), and to our knowledge, no studies have investigated humor styles in either of these neurodevelopmental conditions. Moreover, studies on humor in autism have mainly focused on adults without intellectual disabilities, which is not entirely representative of the spectrum. As a result, comparisons of humor styles across ASC, DS, and WS are currently lacking. Doing so could be helpful to highlight potential syndrome-specific patterns in humor use while also allowing a transdiagnostic perspective. In this context, a transdiagnostic approach refers to examining whether differences in humor are better explained by underlying characteristics, such as social abilities or mental health, rather than by diagnostic categories alone. This approach is important because individuals with different neurodevelopmental conditions may share similar social or emotional difficulties, which could influence how they use humor in everyday interactions.
In the present study, questionnaires were distributed to parents of autistic individuals (with and without intellectual disabilities) and of individuals with WS or DS, to assess which humor styles they tend to employ, as well as to assess individual differences in social difficulties (including social awareness, cognition, communication, and motivation) and mental health problems (social, emotional, or behavioral). First, we examine whether humor styles differ across these three neurodevelopmental conditions. Based on previous research suggesting reduced engagement in positive humor among autistic individuals, we hypothesize that individuals with ASC would show a lower tendency to engage in positive forms of humor. By targeting younger participants and individuals both with and without intellectual disabilities, this study also extends previous findings on humor in autism to a broader and more representative sample. Second, given the lack of previous research on humor in WS and DS, we explore which humor styles are most commonly used by individuals with these conditions and how they compare with those observed in ASC. As there is limited empirical evidence to guide predictions, this part of the analysis is considered exploratory. Third, we investigate whether individual differences in social difficulties and mental health predict the use of humor styles beyond diagnostic group membership and demographic factors. We expected social difficulties related to social motivation and social cognition to be negatively correlated with positive forms of humor and positively correlated with negative forms of humor. We also hypothesized that higher levels of emotional, behavioral, and social problems related to mental health would be related to lower levels of positive humor styles and higher levels of negative humor styles. Considering the important role that positive humor can play in regulating emotions and enhancing well-being, it is crucial to better understand the extent to which individuals with different neurodevelopmental conditions engage in different types of humor.
Methods
Participants
After a data cleaning procedure explained in the following section, 230 parents took part in the study. Parents were asked to report whether their child used verbal speech. Participants whose children were reported as not using verbal speech were categorized as non-speaking. Because the Humor Styles Questionnaire used in this study primarily assesses humor expressed through verbally mediated behaviors (e.g., joking or teasing), analyses were restricted to participants whose parents reported that their child used verbal speech, as the instrument may not validly capture humor expressed primarily through non-spoken forms of communication or AAC devices. As such, the final cohort consisted of 147 parents of young individuals with ASC (N = 31), DS (N = 82), or WS (N = 34). Most participants (93.2%) described their child as being Caucasian, with a few (6.1%) describing them as having mixed ethnical origins, and one (0.7%) as being Asian. 83.9% of participants lived in England, 7.4% in Scotland, 2.7% in Wales, 2% in Ireland, 1.4% in Northern Ireland, and the remaining 2.8% were spread between Japan, USA, Canada, and Portugal.
Table 1 presents the children's characteristics. A one-way ANOVA revealed there was no significant difference in mean age between the three groups, F(2, 144) = .508, p = .603. A Pearson chi-square test revealed a significant difference in the sex distribution between the groups, X2(2, 146) = 10.56, p = .005. This difference is explained by the higher prevalence of an autism diagnosis in males than females, which is representative of the general tendency and not just a peculiarity of the current cohort: Zeidan et al. (2022) estimate a median male-to-female ratio of 4.2 across several international studies. In this study the male-to-female ratio is 5.0.
Participants’ Characteristics.

Note: ASC = Autism Spectrum Condition; DS = Down syndrome; WS = Williams syndrome. One parent in the ASC group did not indicate their child's sex.
There was also a significant group difference in the presence or not of an intellectual disability, X2(2, 147) = 53.36, p < .001. This is due to the heterogeneity of cognitive abilities in the ASC group (Charman et al., 2011). Indeed, individuals with DS and WS are typically characterized by having intellectual disabilities (Chapman & Hesketh, 2000; Korenberg et al., 2000), which is not necessarily the case with autistic individuals. However, differences in humor styles between individuals with and without intellectual disabilities in the ASC group should and will be controlled for.
Procedure
Participants were recruited in the UK: an advertisement was distributed to specific groups on social media, sent to schools, associations, and parents who had previously participated in other studies. The current study is part of a larger survey-based project on different socio-emotional processes in individuals with neurodevelopmental conditions. In this context, parents received a total of £50 in exchange for completing a series of 23 questionnaires administered across three assessment sessions. The questionnaires in the current study included the ones used in the first part of the project. The inclusion criteria were that participants needed to be parents of a child with autism, DS, or WS, aged between 5 and 25 years old. To avoid as much as possible “scammer” participants (Pellicano et al., 2023), we established a few strategies, during and after recruitment: (a) we checked the IP addresses and excluded participants who's IP addresses appeared several times (with the exception of one family with twins that the researchers were aware about); (b) participants were asked to send an email to us indicating their child's age and diagnosis and the link to the study was sent only to those who wrote to us (the email addresses and names were not kept in the data set of the analysis in order to keep the study anonymous); (c) the questionnaire included a few redundant questions, e.g., asking for the date of birth as well as the age, and only the participants for which the calculated and reported ages matched were kept; (d) respondents who answered the same response to all questions (e.g., always checking “1” on the likert scales) were excluded; and (e) respondents who responded in less than 10 minutes (the whole study included 10 questionnaires, with a total of 260 items) were excluded. The first round of recruitment led to a lot of fraudulent attempts to participate so some of these measures were implemented subsequently. Indeed, there were initially 1,070 answers on the Qualtrics platform online, but only 230 remained after checking and cleaning the data according to the criteria mentioned above. Given the initial and subsequent measures taken, we are confident that only data given by genuine participants has been analyzed.
Instruments
For this study, data from 4 questionnaires was analyzed to assess social impairment, affective predispositions and humor styles.
Socio-Demographic Information and Diagnosis
Before answering the specific questionnaires, parents were asked a series of socio-demographic questions, such as the age, sex and ethnic origins of their child. They were also asked which diagnosis their child had (with a selective list which included ASC, DS, and WS), as well as whether their child used verbal speech or was non-speaking, and whether they had an intellectual disability or not.
Humor Style
To assess different humor styles, we used the Humor Style Questionnaire for children (HSQ-c; Fox et al., 2013), which is a simplified version of the Humor Style Questionnaire (HSQ; Martin et al., 2003). Compared to the original HSQ, the HSQ-c is shorter (24 items instead of 32), the scale is of 4-point instead of 7-point, and it uses simpler formulations. As in the HSQ, the HSQ-c assesses children's use of four different humor styles, corresponding to four different subscales: affiliative, aggressive, self-enhancing, and self-defeating. The child version was preferred for reasons related to the larger project of which this study is only a part. For the present study, items were adapted for parent-report because the target population consisted of neurodivergent children, for whom reliable self-report data may be difficult to obtain due to developmental, communication, or meta-cognitive differences. A 4-point scale was used: (1) strongly disagree, (2) disagree, (3) agree, (4) strongly agree. A score for each subscale can be calculated, ranging from 6 to 24.
Social Difficulties
The Social Responsiveness Scale 1 (SRS-2, Constantino & Gruber, 2012) is built to assess the severity of autism symptoms and general social impairments. It is rated on a 4-point scale, ranging from (1) not true to (4) almost always true. The scale contains 65 items and 5 subscales: social awareness (the ability to detect social cues, e.g., noticing when others are uncomfortable), social cognition (the ability to interpret social information and others’ intentions), social communication (the use of verbal and non-verbal behaviors during social interactions), social motivation (the tendency to seek or enjoy social interactions), and restricted interests and repetitive behaviors (rigid or repetitive patterns of behavior or interests). The questionnaire is parent-reported and exists in different versions according to the child's age (specifically, one version for children under 18, and one for adults aged 18 years or older).
A raw score of each subscale can be separately calculated, the range depending on the number of items in each subscale (social awareness: 8–32; social cognition: 12–48; restrictive repetitive behavior: 12–48, social communication: 22–88; social motivation: 11–44). A total raw score can also be calculated for each participant, including all the items and based on which cut-offs have been defined to evaluate the severity of autistic symptoms and social impairments. Only raw scores were used in the present study.
Mental Health
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) is a widely used questionnaire in research and in practice to assess children and young individuals’ mental health. It is notably used to assess the severity of symptoms (emotional, behavioral, and social) and to evaluate the impact of different conditions on the individuals’ emotional, behavioral, and social lives. It has been shown as being a consistent tool to measure socio-emotional difficulties as co-occurring conditions in ASC (e.g., Salayev & Sanne, 2017). In the current study, different parent-report versions were used, according to the age of the participant's child (younger than 4 years old, between 4 and 17 years old, and 18 years old and more). Each version contains the same number of items but the formulation changes to correspond to the environment and behaviors of individuals of different ages. Parents are asked “For each item, please select the answer that best describes your child's behavior,” and their rating is done with a 3-points scale: (0) not true, (1) somewhat true, (2) certainly true. The questionnaire contains 25 items divided between 5 subscales (5 items each): emotional problems (e.g., worries, fears), conduct problems (e.g., rule-breaking or aggressive behavior), hyperactivity/inattention (e.g., restlessness or difficulty concentrating), peer relationship problems (e.g., difficulties interacting with peers), and prosocial behavior (e.g., helping, sharing, or showing concern for others). For each subscale, a score can be calculated, ranging from 0 to 10. Cut-offs have been defined to assess the severity of symptoms, but only raw scores were used in the present study.
Analysis
The analysis was conducted with the software IBM SPSS Statistics version 29. First, we evaluated the reliability of each scale and subscale, for all groups together and each group separately, by calculating the Cronbach's alpha. Scales were considered as reliable, with αC ≥0.7. The data is available here: (OSF link: https://osf.io/dhqrw).
Second, we calculated descriptive statistics (i.e., means and standard errors) for each subscale and each group separately. For each subscale from the HSQ-c, SRS and SDQ, we looked at group differences by running one-way analyses of variance (ANOVAs). Prior to analysis, assumptions were examined. Homogeneity of variances was assessed using Levene's tests. When this assumption was violated, Games–Howell post hoc comparisons were used to examine pairwise group differences. Statistical significance was set at p < .05. Effect sizes (η2) were calculated to estimate the magnitude of group differences. We ran Pearson correlations to examine the associations between humor styles and behavioral and social functioning measures, including the subscales of the SRS and SDQ, as well as age. For humor styles, we also ran independent-samples t-tests to determine whether there were differences in the scores between individuals with and without intellectual disabilities in the ASC group.
Finally, for humor styles for which group differences were observed, separate hierarchical multiple regression analyses were conducted to examine whether these differences were primarily explained by diagnostic group membership or by individual behavioral characteristics measured by SRS and SDQ. In the first model, the diagnostic groups (ASC, DS, and WS) were used as independent variables. Since dummy variables were used, ASC served as the reference category, with DS and WS entered as predictors. In the second model, the groups remained, and demographic information (i.e., sex and age) and individual traits (scores in the respective subscales of the SRS and SDQ) were entered as additional independent variables. This approach allowed us to examine whether individual traits predicted humor styles beyond the effect of diagnostic group. The significance level for all statistical tests was set at α = .05. Assumptions of multiple regression were examined prior to analysis. Multicollinearity was assessed using variance inflation factors (VIFs) and tolerance statistics. Influential observations were evaluated using Cook's distance. Normality of residuals was inspected using normal P–P plots and histograms, and homoscedasticity was examined by inspecting a scatterplot of standardized predicted values against standardized residuals.
Results
Reliability Analysis
As revealed in Table 2, reliability analysis showed that, when all groups were considered together, all scales reached acceptable reliability (αC ≥0.7). However, the SDQ did not reach an acceptable score for the ASC group (αC = .56). HSQ—Aggressive and SRS—Awareness subscales showed poor reliability across all groups. The SDQ—Emotional problems and SDQ—Peer problems subscales were below 0.7 for the ASC and WS groups and the SDQ—Conduct problems subscale was below the acceptable threshold for the ASC and DS group. Thus, the following results should be interpreted cautiously.
Reliability Analysis—Cronbach's Alphas.
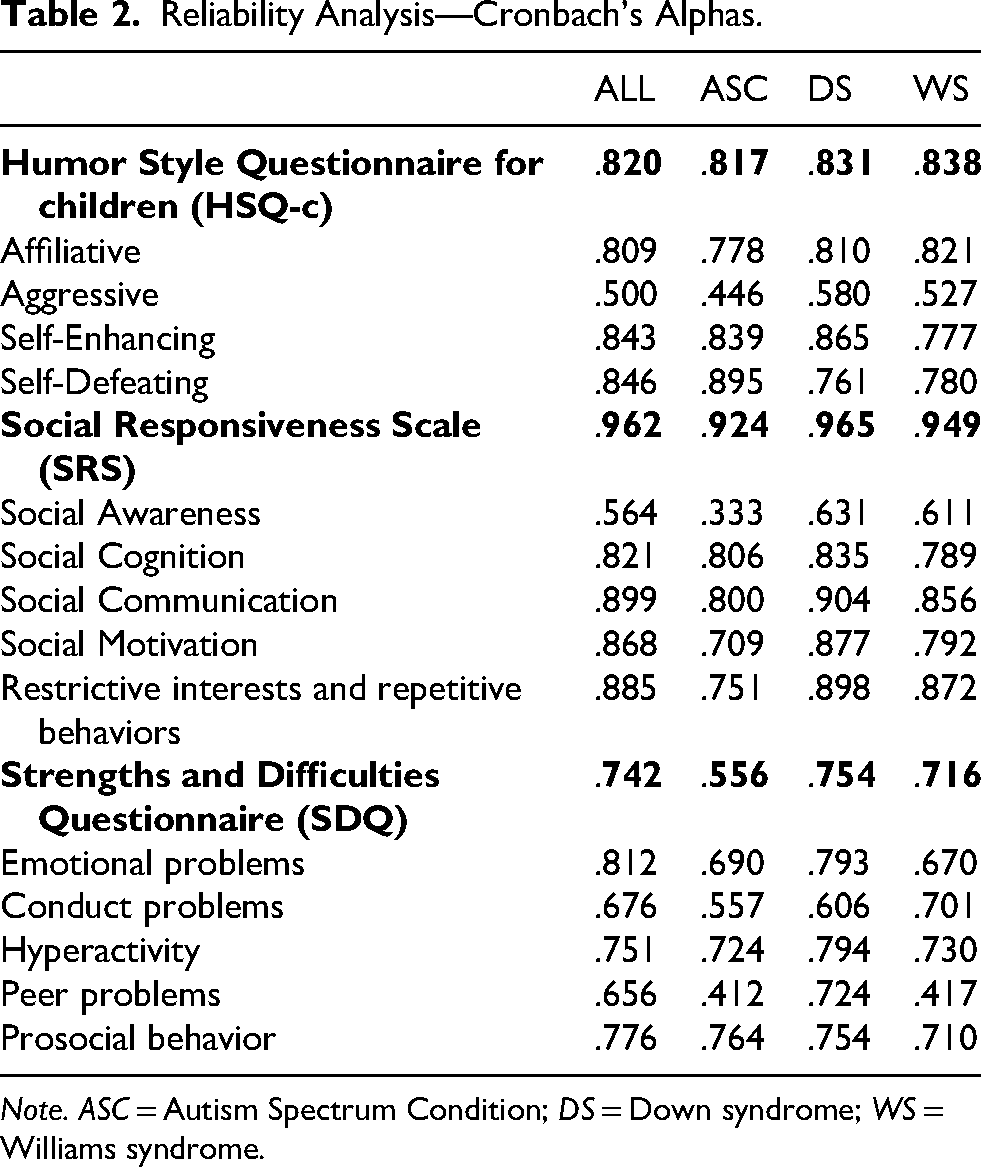
Note. ASC = Autism Spectrum Condition; DS = Down syndrome; WS = Williams syndrome.
Group Differences
As shown in Table 3, there was a significant group difference between ASC, DS, and WS in the use of two humor styles: self-defeating humor and affiliative humor. Self-defeating humor differed significantly across groups, F(2, 142) = 17.41, p < .001, η2 = .197. Games–Howell post hoc comparisons indicated that the ASC group showed significantly higher levels of self-defeating humor (M = 13.70, SE = .91) than both the DS group (M = 9.02, SE = .35, p< .001) and the WS group (M = 10.00, SE = .63, p = .004) whereas the DS and WS groups did not differ significantly (p = .368). In addition, affiliative humor also differed across groups, F(2, 142) = 4.87, p = .009, η2 = .064, indicating a moderate effect size. Games–Howell post hoc comparisons indicated that the DS group (M = 18.65, SE = .41) showed significantly higher affiliative humor than the ASC group (M = 16.23, SE = .69, p = .011) while other pairwise comparisons were not significant.
Descriptive Statistics and Group Differences.
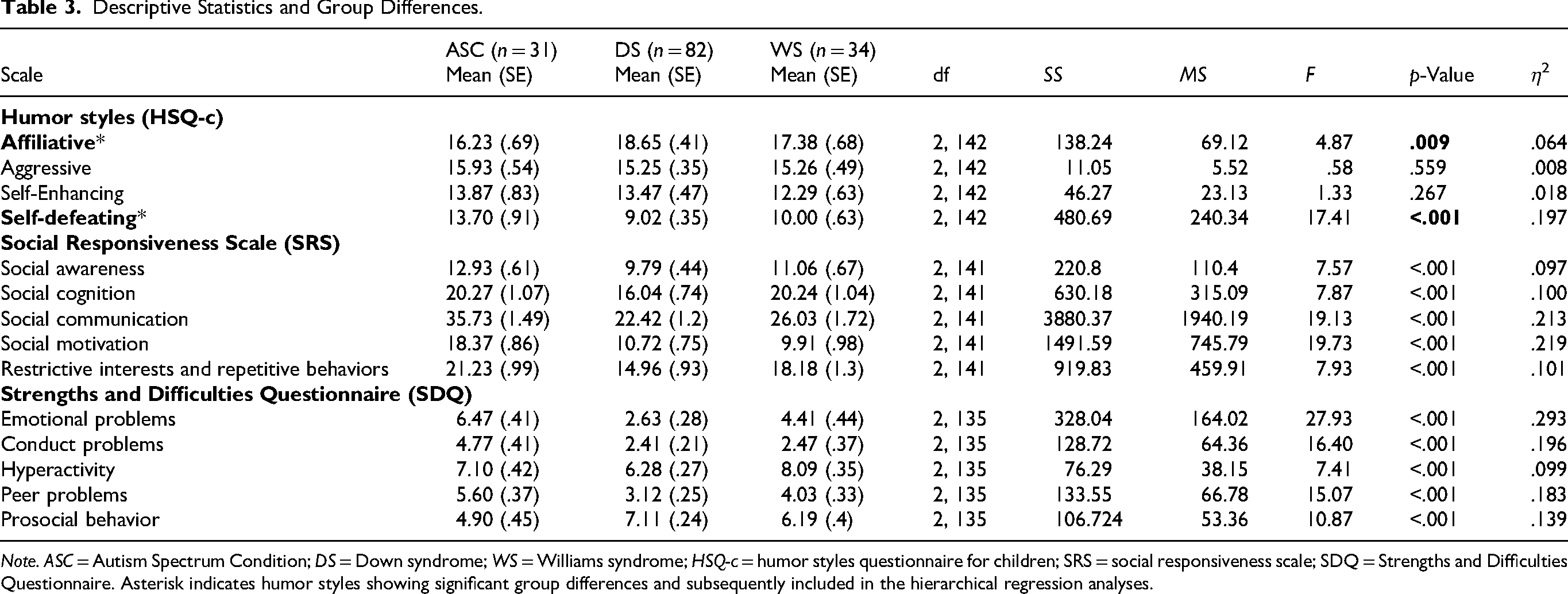
Note. ASC = Autism Spectrum Condition; DS = Down syndrome; WS = Williams syndrome; HSQ-c = humor styles questionnaire for children; SRS = social responsiveness scale; SDQ = Strengths and Difficulties Questionnaire. Asterisk indicates humor styles showing significant group differences and subsequently included in the hierarchical regression analyses.
We have also conducted additional ANCOVAs including age as a covariate and sex as a factor to examine whether demographic factors could account for the observed effects. They showed that neither age nor sex significantly predicted self-defeating or affiliative humor, and the group × sex interactions were also not significant (all ps > .05). Importantly, the group effects remained significant for both self-defeating humor, F(2,137) = 6.28, p = .002, and affiliative humor, F(2,137) = 4.31, p = .015, indicating that the observed group differences are unlikely to be explained by age or sex differences across the sample.
Table 3 reveals significant group differences across all SRS and SDQ subscales. The raw means indicate that, overall, ASC individuals show greater social difficulties than individuals with DS and WS. This pattern is reflected in higher scores across SRS domains—including social awareness, social cognition, social communication, social motivation, and restrictive interests and repetitive behaviors—as well as higher scores on SDQ peer problems and lower scores on SDQ prosocial behavior. Notably, a large group effect was observed for the SRS Social Motivation subscale (F(2,141) = 19.73, p < .001), indicating lower social motivation in the ASC group compared with the DS and WS groups. However, individuals with WS showed levels of social cognition difficulties comparable to those of the ASC group, while exhibiting higher levels of hyperactivity than both other groups. Detailed statistical results are presented in Table 3. Cut-off percentages describing the distribution of symptom severity for each subscale across groups are provided in the Supplementary Material. 1
Within the ASC group, independent-samples t-tests indicated no significant differences between autistic participants with and without intellectual disability for affiliative humor, t(28) = 1.49, p = .147, aggressive humor, t(28) = −0.47, p = .639, or self-defeating humor, t(28) = 1.47, p = .152. Autistic participants with intellectual disability showed higher levels of self-enhancing humor than those without intellectual disability, t(28) = 2.24, p = .034, however, this difference did not remain significant after Bonferroni correction for multiple comparisons (α = .0125).
Correlations
Table 4 presents Pearson correlations for humor styles with social responsiveness (SRS), behavioral difficulties (SDQ), and age. Affiliative humor was negatively associated with several indicators of social and behavioral difficulties, including emotional problems (r = −.45, p < .001) and peer problems (r = −.41, p < .001), and positively associated with prosocial behavior (r = .42, p < .001). Self-enhancing humor was negatively associated with several indicators of social difficulties, particularly social cognition (r = −.32, p < .001) and with repetitive behaviors (r = −.22, p = .009). In contrast, self-defeating humor was positively correlated with emotional problems (r = .41, p < .001), conduct problems (r = .49, p < .001), and peer problems (r = .33, p < .001). Aggressive humor showed few associations with behavioral or social functioning measures, although it was weakly negatively correlated with prosocial behavior (r = −.18, p < .05).
Pearson Correlations for Humor Styles With Social Responsiveness, Behavioral Characteristics and Age.
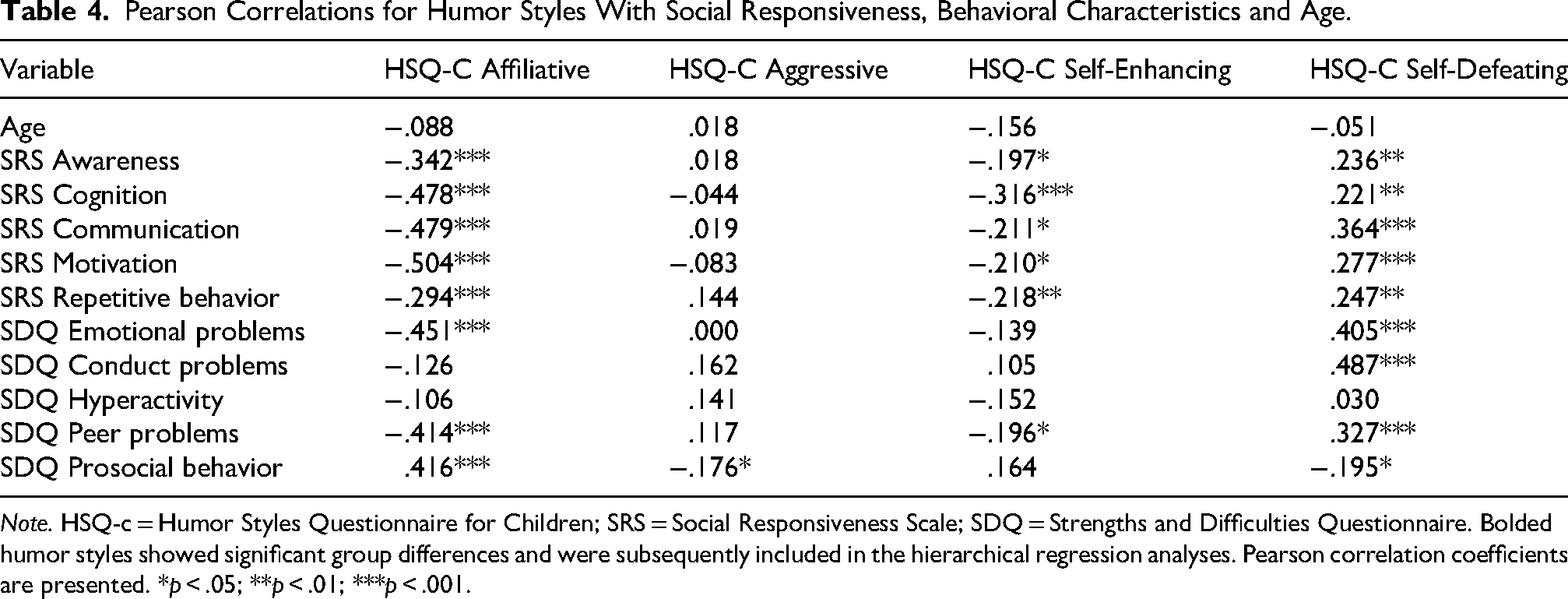
Note. HSQ-c = Humor Styles Questionnaire for Children; SRS = Social Responsiveness Scale; SDQ = Strengths and Difficulties Questionnaire. Bolded humor styles showed significant group differences and were subsequently included in the hierarchical regression analyses. Pearson correlation coefficients are presented. *p < .05; **p < .01; ***p < .001.
Regression Analysis
Considering that the groups differed in the use of self-defeating and affiliative humor, separate regression analyses were run with HSQ-c—Self-defeating and for affiliative humor as dependent variables.
Table 5 reports the scores on the two models of the regression analyses for HSQ-c—Self-defeating humor as dependent variable, as well as affiliative humor as dependent variable. In Model 1, diagnostic group was entered as the predictor and the model was significant, R2 = .197, F(2,142) = 17.41, p < .001. Both the DS (β = −.59, p < .001) and WS groups (β = −.41, p < .001) reported lower self-defeating humor than the ASC group. In Model 2, the SRS and SDQ subscales were added as predictors. This model was also significant, R2 = .390, F(14,121) = 5.53, p < .001, explaining more variance than Model 1. After including behavioral characteristics, diagnostic group was no longer significant, and conduct problems (β = .32, p = .001) and hyperactivity (β = −.23, p = .023) emerged as significant predictors of self-defeating humor.
Regression Analyses With HSQ-c—Self-Defeating and Affiliative Humor as Dependent Variables.
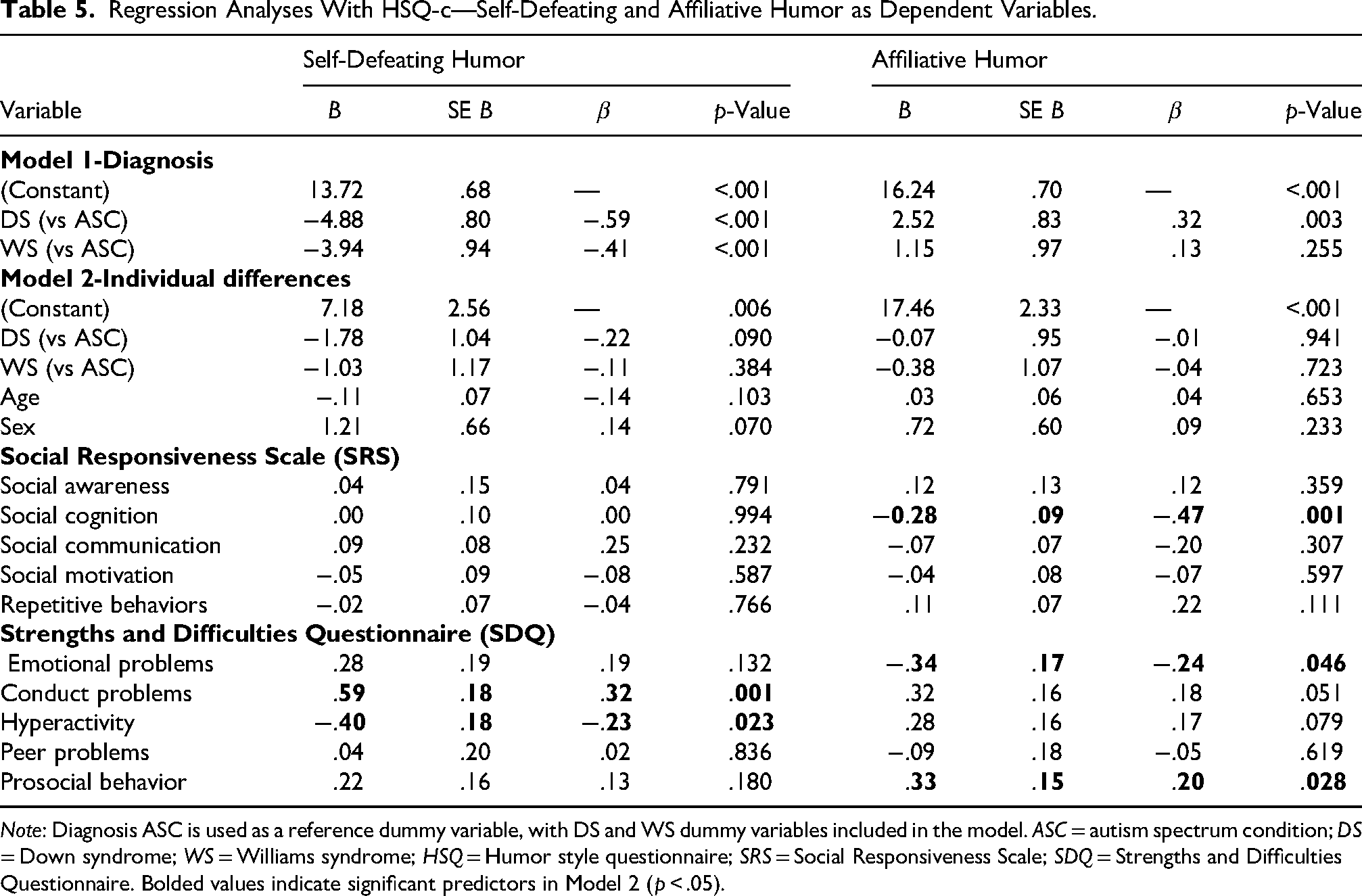
Note: Diagnosis ASC is used as a reference dummy variable, with DS and WS dummy variables included in the model. ASC = autism spectrum condition; DS = Down syndrome; WS = Williams syndrome; HSQ = Humor style questionnaire; SRS = Social Responsiveness Scale; SDQ = Strengths and Difficulties Questionnaire. Bolded values indicate significant predictors in Model 2 (p < .05).
A hierarchical multiple regression analysis was also conducted for affiliative humor. In Model 1, diagnostic group significantly predicted affiliative humor, F(2,133) = 5.30, p = .006, explaining 7.4% of the variance. DS participants reported higher affiliative humor than those with ASC (β = .32, p = .003), whereas the WS group did not differ from ASC. In Model 2, demographic and behavioral variables were added. The model was significant, F(14,121) = 6.74, p < .001, explaining 43.8% of the variance in affiliative humor. The diagnostic groups had no longer an effect, but social cognition difficulties (β = −.47, p = .001) and emotional problems (β = −.24, p = .046) were significant negative predictors, whereas prosocial behavior (β = .20, p = .028) was a positive predictor. Diagnostic checks indicated no problematic multicollinearity (all VIFs < 10; largest VIF = 8.24) and no influential observations (maximum Cook's distance = 0.069).
Discussion
Humor can be a strong tool to regulate emotions and enhance well-being. The main goals of the current paper were to examine the use of humor styles in individuals with autism, WS, and DS, as well as to examine the impact of individual differences in social, psychological, and behavioral characteristics on the use of humor styles from a transdiagnostic perspective. While previous studies have examined autistic adults compared to a neurotypical population (Samson et al., 2013), we focused on a younger and more cognitively diversified autistic sample, and, for the first time, on individuals with WS and DS. Our main results revealed that autistic individuals were reported to use significantly more self-defeating humor than both individuals with WS and with DS, and less affiliative humor compared to individuals with DS. Moreover, several variables seemed to explain the use of these two humor styles better than group membership alone.
For affiliative humor, autistic individuals seem to have lower scores than individuals with DS. This finding may be partly consistent with the positivity bias found in individuals with DS, reflected in a tendency to interpret negative emotional expressions more positively (Porter et al., 2007). However, because a similar positivity bias has also been described in individuals with WS, and affiliative humor did not differ significantly between the WS and ASC groups, positivity bias alone is unlikely to account for the observed pattern. Notably, our regression analyses indicated that individual differences in social cognition, emotional problems, and prosocial behavior were more strongly associated with affiliative humor than diagnostic group membership, suggesting that these characteristics may provide a more informative explanation of variation in affiliative humor than diagnosis alone. Nevertheless, the lower use of affiliative humor among autistic individuals seems to be in line with previous studies showing reduced use of positive humor styles in autistic individuals (Samson et al., 2013). In turn, the lower use of positive humor may impact their well-being. Indeed, it has notably been shown that autistic individuals are more prone to develop a fear of being laughed at (Samson et al., 2011; Treichel et al., 2023). Interestingly, across syndromes, affiliative humor is associated with fewer social cognition difficulties, fewer emotional problems, and more prosocial behavior, which seems to be consistent with the expectations of what a warm, social, and benevolent humor style is associated with. In this line, affiliative humor may be particularly interesting to up-regulate positive emotions. Recently, Samson et al. (2022) showed that only young autistic individuals without intellectual disabilities used humor to regulate emotions that were linked to lower levels of anxiety, compared to other neurodevelopmental conditions. In line with this and to expand the current findings, it would be interesting to study different humor styles and their relation to lower anxiety levels in different neurodevelopmental conditions.
While Samson et al. (2013) identified no differences in negative humor styles between autistic and TD individuals, the present study found a more frequent use of self-defeating humor in autistic individuals compared to individuals with DS and WS. Regression analysis showed that the stronger predictor for differences in self-defeating humor were conduct problems, which belongs to the general category of “externalizing problems” of the SDQ 2 (Goodman et al., 2010). Conduct problems correlate positively with self-defeating humor and are much less concerning for individuals with WS and DS than for autistic individuals. Conduct problems include maladaptive behaviors such as having temper tantrums, fighting, lying, stealing, or disobeying. One possible explanation for the relation between conduct problems and self-defeating humor could be that maladaptive behaviors might lead individuals to have a poorer opinion of themselves. Indeed, the conduct problems defined in the SDQ are generally behaviors that do not respond to norms, social rules, and rules of conduct. As such, these behaviors can lead to negative responses coming from others, who witness them or are targets of them, and these negative responses might lead individuals who engage in such behaviors to have a poorer opinion about themselves and thus easily self-depreciate themselves. On the other hand, individuals who engage less in maladaptive behaviors will have less reason to self-depreciate themselves in the eyes of others. This would be consistent with previous research which has shown a negative correlation between self-defeating humor and self-esteem (Martin et al., 2003) and a positive correlation between self-esteem and conduct problems (Ha et al., 2008). Future research should investigate more thoroughly the link between self-esteem, externalizing mental health problems, and self-defeating humor in neurodevelopmental conditions.
Our results are partly overlapping with previous research on humor styles in autism and humor as an emotion regulation strategy (Samson et al., 2013, 2022, see also Manfredi et al., 2026). Differences could be partly explained by differences in age, intellectual skills, and self- versus parent-report. However, differences in intellectual disability cannot be the main driver for differences between the studies, since in the current study, affiliative and self-defeating humor did not differ according to intellectual disability status in the ASC group. In a study comparing autistic and TD adults, Samson et al. (2013) observed a less frequent use of both positive humor styles in individuals with ASC. However, it may be difficult to compare our results with the findings by Samson et al. (2013), since their participants were adults—whereas the present study included children, adolescents and young adults—and they had no participants with intellectual disabilities—whereas the current study's sample is more cognitively diverse. In addition, the comparison groups are not the same: while Samson et al. (2013) included a group of TD individuals, the present study compared different neurodevelopmental conditions. Finally, Samson et al. (2013) used self-reports, whereas the present study used parent-reports. Any of these differences or a combination of them might explain why the current study differs slightly from the study by Samson et al. (2013). It may also be hypothesized that it may be at times difficult for parents to report on specific humor styles, since they relate at times to intrapersonal mechanisms that are not necessarily perceptible from a third person's perspective. Indeed, parents might detect that their child uses humor, but the intention behind it (i.e., whether it is to cheer oneself up, or for any other reason) might be more difficult to detect.
The results of these regressions suggest that differences in humor processing should be understood from a transdiagnostic perspective, perhaps surpassing the strict definition of specific diagnoses in favor of focusing on psychological and neurological processes that can be common to different diagnoses and better highlight the origins of specific difficulties (Astle et al., 2022; Insel et al., 2010; Monestès & Baeyens, 2016). In our study, group differences have been observed in the use of self-defeating humor as well as affiliative humor, but when individual differences were included in the analyses, the diagnoses did not appear as significant predictors anymore. These results suggest that a strictly observed difference between the conditions is limited in terms of our understanding of the origins of these specific behaviors. This is in line with a previous study led by the same author which showed that differences between ASC, DS, and WS in the tendency to develop a fear of being laughed at (gelotophobia) were superseded by individual differences in humor temperament, namely bad mood and seriousness (Treichel et al., 2023).
Limitations
While a particular strength of our study is that it is the first one to address humor styles in WS and DS and that it brings a transdiagnostic explanation to differences in humor styles in various developmental conditions, several limitations have to be addressed. One limitation of the present study is that it did not include a neurotypical group. Future studies should include mental age-matched and chronological age-matched typically developing participants, to allow for a more precise interpretation of the specificities of autism, DS, and WS in relation to humor styles. It would be interesting, for example, to test how individuals with WS and DS appear to engage in different humor styles comparatively to neurotypical individuals, and whether young and more cognitively diverse autistic individuals also differ from neurotypical individuals in their use of positive humor styles. Another limitation of the current sample is the limited number of participants with ASC, when considering the higher prevalence of this condition in comparison with DS or WS (Sherman et al., 2007; Strømme et al., 2002; Zeidan et al., 2022). As such, future studies should include a larger group of participants with autism. As in the current study, the humor styles questionnaire primarily assessed humor expressed through spoken language, it may not adequately capture humor communicated through non-spoken forms of communication, or AAC devices. Future research should use measures that better account for humor expressed through non-spoken forms of communication. Further limitation concerns the use of a parent-report adaptation of the HSQ, for which formal validation evidence is currently lacking. Although parent reports are commonly used in developmental and clinical research, some humor styles, such as self-enhancing humor, reflect internal emotion-regulation processes that may not be directly observable. As a result, parents may not always be able to accurately infer the motivations underlying their child's use of humor. Consequently, findings based on these measures should be interpreted with caution, and future research should aim to validate parent-report adaptations of the HSQ. Another limitation concerns the relatively low internal consistency observed for several subscales, particularly the SRS Social Awareness subscale and some SDQ subscales. Notably, the SDQ Conduct Problems subscale showed low reliability in the ASC group while also emerging as a predictor of self-defeating humor. Although the SDQ subscales consist of only five items and modest Cronbach's alpha values have frequently been reported in previous studies across a range of populations (e.g., Goodman, 2001; Stone et al., 2010), lower reliability may increase measurement error and reduce the strength of conclusions that can be drawn from these associations. Therefore, findings involving these subscales should be interpreted with caution and future research should seek to replicate them using measures with stronger internal consistency. Finally, because the study relied exclusively on parent-report questionnaires administered online, it was not possible to collect standardized cognitive assessments within the scope of the current methodology. Future studies should thus add a more accurate evaluation of intellectual disabilities to get a better picture of the influence of cognitive abilities on humor processing in ASC, DS, and WS participants, compared to mental age-matched TD participants.
Conclusions
Humor can be highly beneficial for well-being, but research has shown the differing influences of positive humor styles and negative humor styles. Thus, to bring new knowledge for future interventions aiming at improving the use of humor to enhance social interaction, psychological well-being, and emotion regulation, it is important to better understand how individuals with different neurodevelopmental conditions engage in positive and negative humor styles, which would also allow them to better understand the conditions themselves. The results of the present study revealed that individuals with WS and individuals with DS seem to be less inclined than autistic individuals to engage in self-defeating humor, whereas individuals with DS reported higher levels of affiliative humor than autistic individuals. The findings further suggest that self-defeating humor is associated with greater emotional and behavioral difficulties, whereas affiliative humor is associated with more adaptive social and emotional functioning, including better social cognition, fewer emotional problems, and greater prosocial behavior. Although the higher use of affiliative humor in DS may be consistent with the positive social orientation often described in this population, individual social, emotional, and behavioral characteristics seem to explain humor styles more strongly than diagnostic group membership itself. Importantly, these findings support the use of a transdiagnostic perspective and suggest that humor styles may provide a useful lens through which to understand social and emotional functioning across neurodevelopmental conditions.
Supplemental Material
sj-docx-1-dli-10.1177_23969415261464457 - Supplemental material for Humor Styles in Neurodevelopmental Conditions and Their Links to Social, Emotional, and Behavioral Strengths and Difficulties
Supplemental material, sj-docx-1-dli-10.1177_23969415261464457 for Humor Styles in Neurodevelopmental Conditions and Their Links to Social, Emotional, and Behavioral Strengths and Difficulties by Noémie Treichel, Ana Milosavljevic, Verena Hofmann, Jo Van Herwegen and Andrea C. Samson in Autism & Developmental Language Impairments
Footnotes
Acknowledgements
The authors thank all the parents who took part in this study. Thanks also to Daniel Dukes, for proofreading an earlier version of the manuscript.
Ethical Approval
The ethics committee of Unidistance Suisse approved the study protocol.
Informed Consent
Informed consent was provided in written format.
Funding
This research was funded by the Swiss National Science Foundation (Andrea Samson's SNSF Professorship PP00P1_176722) and Research Funds of Unidistance Suisse.
Research Funds of Unidistance Suisse, Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung, (grant number PP00P1_176722).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.