
Abstract
The interface between systemic sclerosis and cancer has offered valuable insights into our understanding of systemic sclerosis disease pathogenesis. Defining systemic sclerosis subgroups both temporally and serologically has been instrumental in stratifying cancer risk, with autoantibodies to RNA polymerase 3, RNA polymerase 1 large subunit, RNA binding region containing 3, and centromere identifying subgroups at increased or decreased risk of cancer. Clinically, improved subgrouping of systemic sclerosis patients provides the opportunity to detect cancer at earlier stages of disease while increasing our efficiency of cancer assessment. Additional studies are needed to define the optimal approach to cancer screening in systemic sclerosis, and validation studies in different cohorts will be needed to confirm all findings.
Keywords
Epidemiology of cancer risk in systemic sclerosis
An association between cancer and systemic sclerosis (SSc) has been recognized since the 1980s. The increased risk of cancer in SSc patients adjusted for age and sex (e.g. standardized incidence ratios, SIRs), has been reported to range from 1.24 to 4.20,1–14 with only a single study reporting a SIR < 1 15 (Table 1).
Risk of cancer in scleroderma from cohort studies, national registries, and systematic reviews and meta-analyses. Adapted, with permission. 16
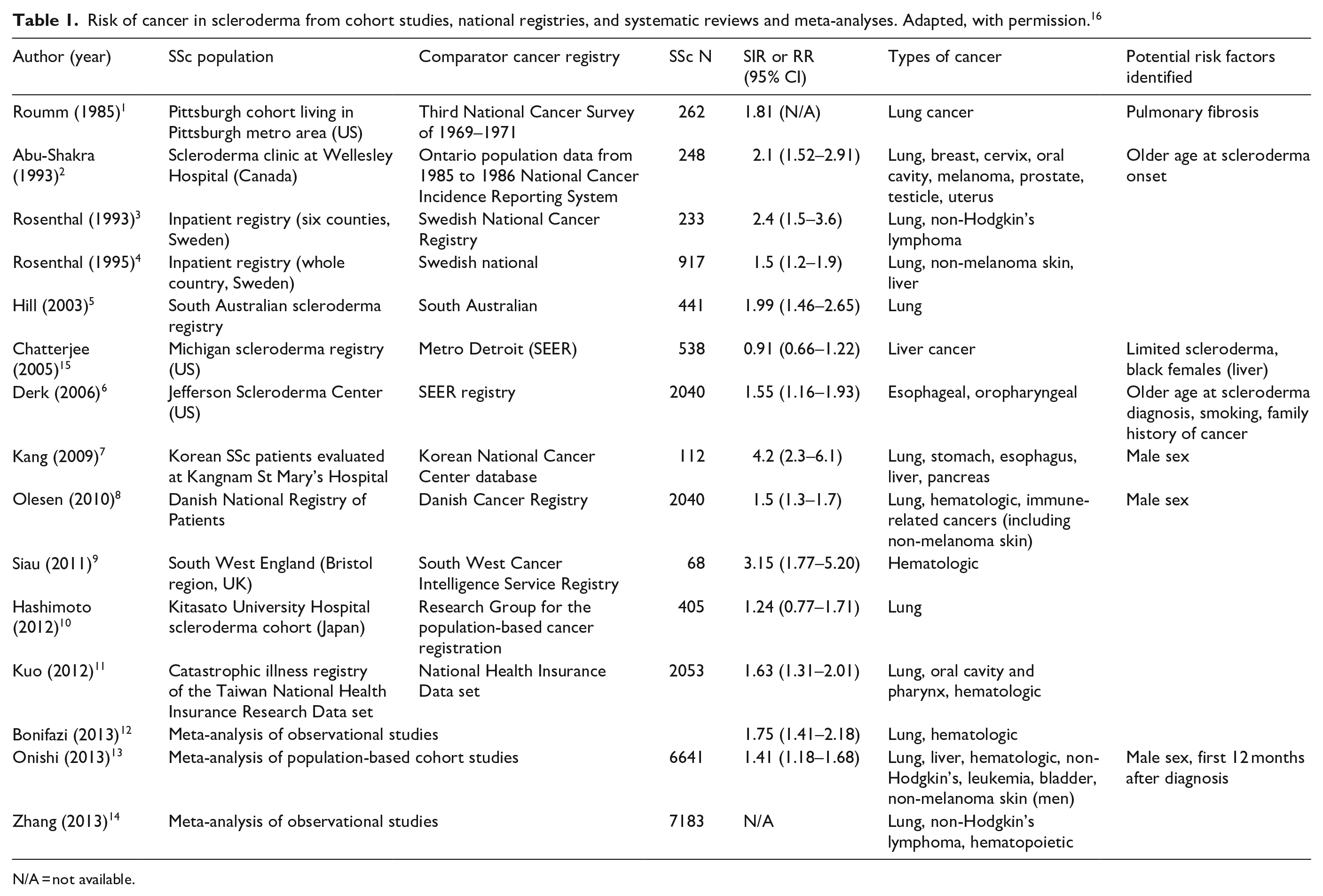
N/A = not available.
A large number of tumor types have been observed to occur more frequently in SSc patients, including lung, liver, esophageal and oral cavity, thyroid, melanoma, non-melanoma skin, and hematologic among others. Historically, some cancer types have been a consistent finding, such as lung cancer (attributed at least in part to interstitial lung disease). Others, however, have been less consistently found, including breast and thyroid cancers.12–14
In 2013, three meta-analyses were published to synthesize findings from the multitude of observational cohort studies. Bonifazi et al. 12 pooled 16 studies totaling over 7000 SSc patients and calculated a relative risk of 1.75 (95% CI = 1.41–2.18) for cancer compared to the general population. The two cancer types with the strongest associations were lung (RR = 4.4, 95% CI = 2.1–9.1) and hematologic (RR = 2.2, 95% CI = 1.5–3.3). The second meta-analysis pooled six articles totaling over 6000 patients. 13 The SIR for cancer incidence was 1.41 (95% CI = 1.2–1.7). Again, increases in lung (SIR = 3.2, 95% CI = 2.1–4.9) and hematologic cancers (SIR = 2.6, 95% CI = 1.1–3.8) were observed, as well as for liver and bladder cancer. In a third report, Zhang et al. 14 analyzed seven studies totaling over 7000 patients (many of whom were the same as Bonifazi and Onishi) and reported similar SIRs for cancers of the lung, non-Hodgkin’s lymphoma, and hematopoetic cancer of 3.14 (95% CI = 2.02–4.89), 2.68 (95% CI = 1.58–4.56), and 2.57 (95% CI = 1.79–3.68), respectively.
Similar to the heterogeneity and breadth of cancer types, a number of clinical and SSc-specific risk factors for cancer have been identified: cutaneous skin type (both diffuse and limited)5,9, older age at scleroderma onset,9,18,19 male sex,8,13 PM-Scl autoantibodies, 17 tumor-associated antigens (e.g. CA–125, CEA) 20 and smoking. 21 In contrast, negative associations with cancer have been reported for patients on aspirin 17 and those with anti-centromere antibodies. 22 However, not all of these findings have been reproduced,23–25 limiting the ability to use these factors for risk stratification.
Although the cancer–SSc association has been recognized for decades, high-risk SSc subgroups have only recently been defined. 26 Careful analysis of these subgroups has provided a better understanding of the cancer-autoimmunity interface, and has afforded new insights into the pathogenesis of SSc itself. 27 This knowledge likely will enable the development of clinically-relevant targeted cancer-screening strategies.
Cancer subgrouping: the importance of temporality and autoantibodies
Almost 10 years ago, our group published the important observation that anti-RNA-polymerase 3 (RNApol3)-positive SSc patients had a close temporal relationship between cancer and the clinical onset of SSc. 26 This finding has since been replicated in several other international SSc cohorts.19,22,28–32 Compared to SSc patients with anti-centromere and anti-Scl70 antibodies, patients with anti-RNApol3 have a significantly shorter interval between the onset of SSc symptoms and diagnosis of malignancy (Table 2). In addition, the odds of coincident cancer in RNApol3-positive SSc patients is significantly higher compared to RNApol3-negative patients (OR = 4.2–7.4). The studies in Table 2 largely focused on the comparison of SSc patients with anti-RNApol3 to SSc patients in other autoantibody subgroups; however, the excess risk relative to the general population and whether any specific cancer types were enriched in these high-risk subgroups was unknown.
Various cohorts of cancer prevalence and risk by autoantibody status.
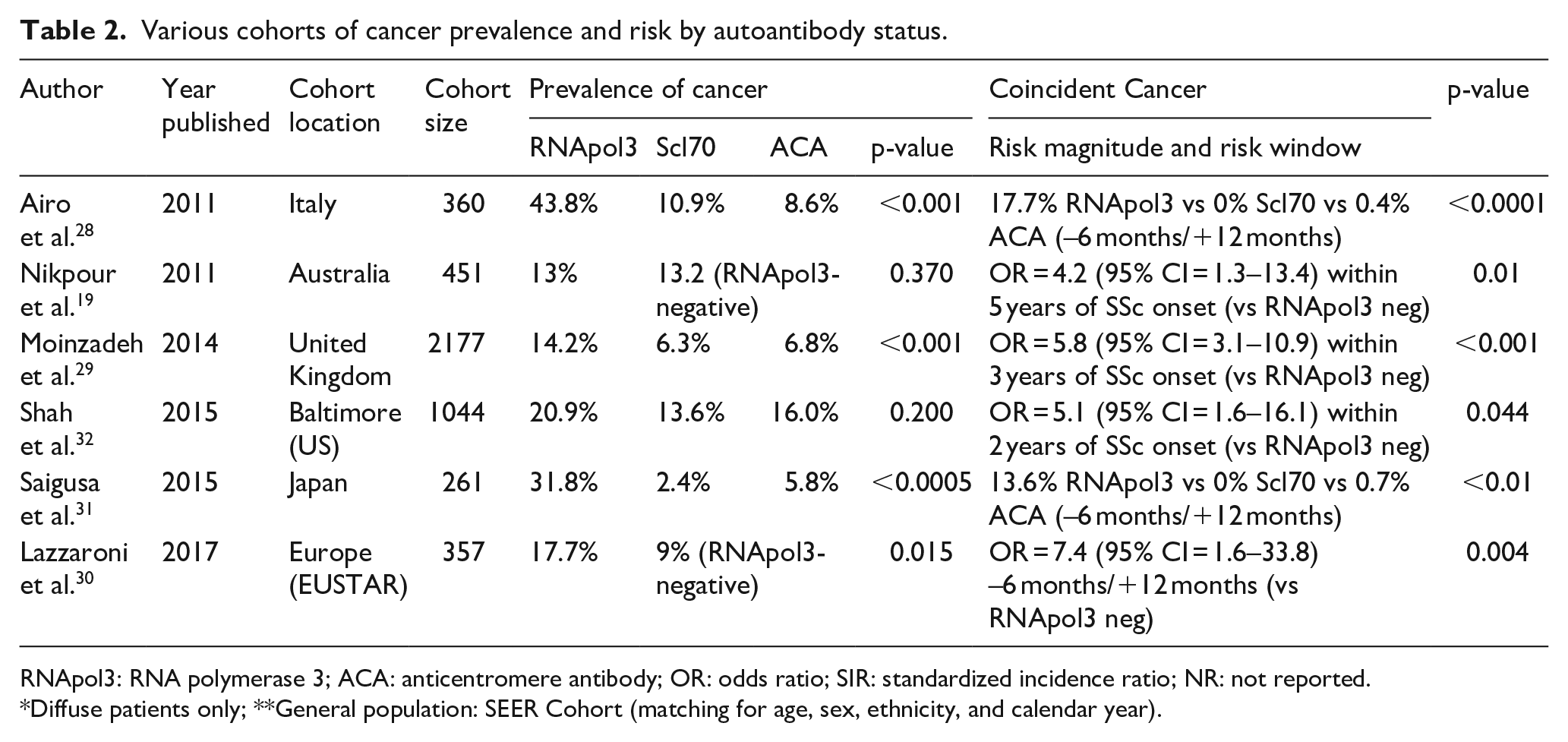
RNApol3: RNA polymerase 3; ACA: anticentromere antibody; OR: odds ratio; SIR: standardized incidence ratio; NR: not reported.
Diffuse patients only; **General population: SEER Cohort (matching for age, sex, ethnicity, and calendar year).
To address these questions, we performed an observational cohort study of 2383 SSc patients followed in the Johns Hopkins Scleroderma Center. 22 Cancer risk was determined by comparing the incidence in this cohort to the Surveillance, Epidemiology, and End Results (SEER) registry, a nationally representative sample of the US population. Overall, patients with RNApol3 autoantibodies had a 2.8-fold increased risk of cancer (SIR = 2.84, 95% CI = 1.89–4.10) within 3 years of SSc-symptom onset compared to the general population (Figure 1). Among anti-RNApol3-positive patients, the risk of different cancer types within 3 years of SSc onset differed based on skin subtype. Those with diffuse SSc had an increased breast cancer risk (SIR = 5.14, 95% CI = 2.66–8.98), whereas those with limited SSc had a high lung cancer risk (SIR = 10.4, 95% CI = 1.26–37.7). In addition to breast and lung, several other cancers were enriched in RNApol3-positive patients including prostate (SIR = 7.2, 95% CI = 1.95–18.4) and tongue cancer (SIR = 43.9, 95% CI = 5.31–158.5). 22 The proportion of each cancer site in the overall SSc cohort and within each autoantibody subset is depicted in Figure 2.
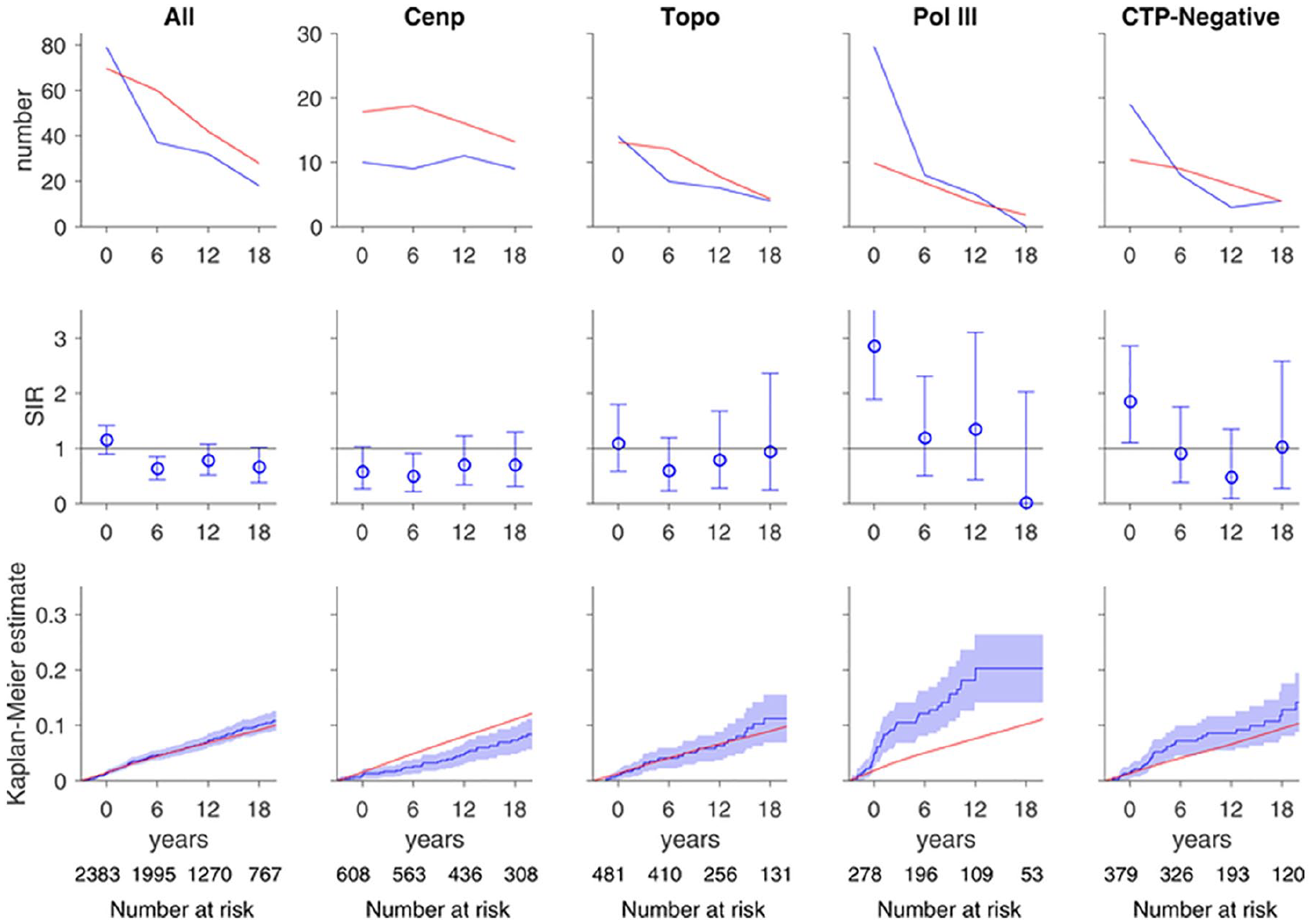
Risk of all cancers over time. In each graph, the x-axis reflects time from scleroderma onset (defined as time zero). Top and middle rows, each time window represents a 6-year period (±3 years); for example, data plotted at time zero reflects cancer risk within ±3 years of scleroderma onset. The number at risk for each time window is denoted at the bottom of the graph. Top row, the observed number of cancer cases (blue) is presented in comparison with the number of cancer cases that are expected based on SEER data (red). Middle row, the ratio between the observed and expected cancer cases is presented as a standardized incidence ratio (SIR) along with its 95% confidence interval. Values of 1 denote a cancer risk equivalent to that of the background population. Bottom row, the cumulative incidence of cancer among scleroderma patients (solid blue line) starting at 3 years before scleroderma onset is presented with 95% confidence intervals (shaded blue region). Red lines represent the expected cumulative incidence of cancer based on SEER data for the general population. Scleroderma patients with anti-centromere antibodies appear to have a decreased risk of cancer over time. Scleroderma patients with pol3 antibodies and the CTP-negative group have an increased risk of cancer that is prominent at scleroderma onset. The cumulative incidence of cancer is significantly higher than that observed in the general population among patients with pol3 autoantibodies. Adapted with permission. 22

Proportions of each cancer site in the overall scleroderma cohort and within each autoantibody subset. The “Other” cancer category includes testicle, vagina/vulva, esophagus, gall bladder/biliary tree, stomach, bladder, cervix, uterus, appendix, small bowel, anal, muscle, and carcinoma with unknown primary. Adapted with permission. 22
In patients with SSc who were negative for centromere, topoisomerase 1, and RNApol3 autoantibodies (“CTP-negative” SSc patients) there was an elevated risk of cancer (SIR = 1.83, 95% CI = 1.10–2.86) within 3 years of symptom onset. Among CTP-negative patients with limited SSc, there was an increased risk of breast cancer (SIR = 4.44, 95% CI = 1.92–8.74) and melanoma (SIR = 7.10, 95% CI = 1.46–20.8), whereas CTP-negative patients with diffuse SSc had an increased risk of tongue cancer (SIR = 40.5, 95% CI = 1.02–225.5).
Perhaps of equal interest was a significantly decreased risk of cancer in SSc patients with anti-centromere antibodies (SIR = 0.59, 95% CI = 0.44–0.76). It is noteworthy that in small cohorts of breast cancer patients without rheumatic disease, anti-centromere antibodies have been identified that associate with improved breast cancer-free and overall survival.33–35 These data raise the intriguing hypothesis that anti-centromere immune responses may be cancer protective, as has been postulated for anti-DNA antibodies. 36 In addition, these findings may explain the varying cancer risk in different SSc cohorts internationally, as the overall risk appears to be driven at least in part by the prevalence of specific autoantibodies such as centromere and RNApol3. These data, if validated in other cohorts, can help risk-stratify SSc patients for cancer, and can inform future prospective studies evaluating different cancer assessment strategies.
Insights into SSc pathogenesis
The discovery of contemporaneous cancer and SSc in patients with RNApol3 antibodies was followed by investigations into whether mutations in the POLR3A locus were present in the tumors of anti-RNApol3-positive SSc patients. These studies culminated in a groundbreaking publication showing that in some cases, autoantigen (POLR3A) mutation within the patient’s cancer may trigger the development of mutation-specific cellular immunity and cross-reactive humoral immune responses. 27 These data strongly suggest a model of cancer-induced autoimmunity, in which autoantigen mutation may trigger an anti-tumor immune response. 18 If this immune response spreads to the wild-type autoantigen, it may cross react with self tissues and in the susceptible host, result in autoimmunity.
An new cancer-associated antibody: RNPC3
At the time the initial observation was made that anti-RNApol3-positive SSc patients are at increased risk for contemporaneous cancer around the time of SSc onset, it was noted that this is also a feature of CTP-negative SSc patients (SIR = 1.83, 95% CI = 1.10–2.86).18,22 Based on the hypothesis that this group likely represents multiple distinct immune responses, some of which associate with an increased risk of cancer, the Hopkins researchers teamed up with investigators at Harvard to use innovative approaches to test for new antibody specificities in this patient subset. Using phage-immunoprecipitation sequencing (PhiPSeq), this team of investigators identified autoantibodies to RNA binding Region Containing 3 (RNPC3) in a small, meticulously phenotyped cohort of CTP-negative SSc patients with short-interval malignancy. 37 A subsequent validation study performed on a cohort consisting of 318 SSc patients with cancer confirmed that patients with anti-RNPC3 antibodies have an increased risk of cancer close to SSc onset, similar to the anti-RNApol3 subset. 38 Relative to SSc patients with anti-centromere antibodies, those with anti-RNPC3 antibodies had a >four-fold increased risk of cancer within 2 years of SSc onset (OR = 4.3, 95% CI = 1.1–16.9). These findings suggest that development of a clinical assay for anti-RNPC3 antibodies may have important clinical utility in identifying those SSc patients at heightened risk for malignancy.
Modulating cancer risk in SSc: RPA194
Despite the increased cancer risk in recent-onset SSc among patients with RNApol3 autoantibodies, ~80%–85% of anti-RNApol3-positive patients do not develop a clinically detectable cancer. 22 We hypothesized that cancer may drive the development of SSc in patients with RNApol3 autoantibodies but that the immune response may be variably successful in either eliminating an underlying cancer or maintaining the cancer in equilibrium such that further growth is prevented. These considerations raise the important question of whether multiple orthogonal immune responses may have a more potent anti-cancer effect than immune responses with a narrower set of targets.
To investigate this, our group recently explored whether SSc patients with anti-RNApol3 antibodies who did not develop cancer differed serologically from those in whom cancer was detected. In a cohort of 168 SSc patients with anti-RNApol3 antibodies (80 with a history of cancer, 88 without cancer after 5 years of follow-up), it was found that antibodies against the large subunit of RNA polymerase 1 (RPA194) were enriched in the group without cancer (16/88 (18%) versus 3/80 (3.8%), p = 0.003). 39 Interestingly, although antibodies to RNA polymerase 1 were first reported in SSc patients in the 1980s,40,41 their association with cancer (or lack of it) was never investigated. Recent elegant studies have demonstrated that BMH21, a small molecule inhibitor of RNA polymerase 1, has anti-tumor activity against multiple cancer cell lines in vitro as well as in animal models. 42 These findings are especially interesting in the context of the RPA194 antibody observations discussed above. Whether anti-RPA194 immune responses in SSc patients have similar anti-cancer properties is an important question that warrants further study.
Together, these data suggest that SSc patients who produce autoantibodies to both RPA194 and RNApol3 are at decreased risk for cancer. If validated in other cohorts, this association may help inform clinicians which RNApol3-positive patients warrant increased intensity of cancer assessment.
Implications for cancer screening
The identification of SSc patient subgroups who are at high risk for cancer naturally leads to a discussion on optimal strategies to assess for malignancy at SSc onset. We recommend age- and sex-appropriate screening in all SSc patients, such as mammography and colonoscopy, as well as increased screening as symptoms and signs warrant (detailed in Table 3). These recommendations are largely based on the United States Preventive Services Task Force (USPSTF) and American Cancer Society cancer-screening recommendations.43,44 However, for SSc patients at higher risk (e.g. anti-RNApol3 or RNPC3-positive within 5 years of symptom onset), the optimal cancer assessment strategy has yet to be determined. Given the potential signal of breast and lung cancers in this patient population, intensive cancer detection strategies, such as CT of the chest, abdomen, and pelvis, whole body positron emission tomography/computed tomography (PET/CT), and breast magnetic resonance imaging (MRI), may be warranted only after careful study determines their value. In certain subgroups (e.g. anti-centromere or anti-RNApol3 + anti-RPA194), the lower cancer risk noted may, if validated, obviate the need for aggressive cancer testing.
Recommendations for all SSc patients upon diagnosis.
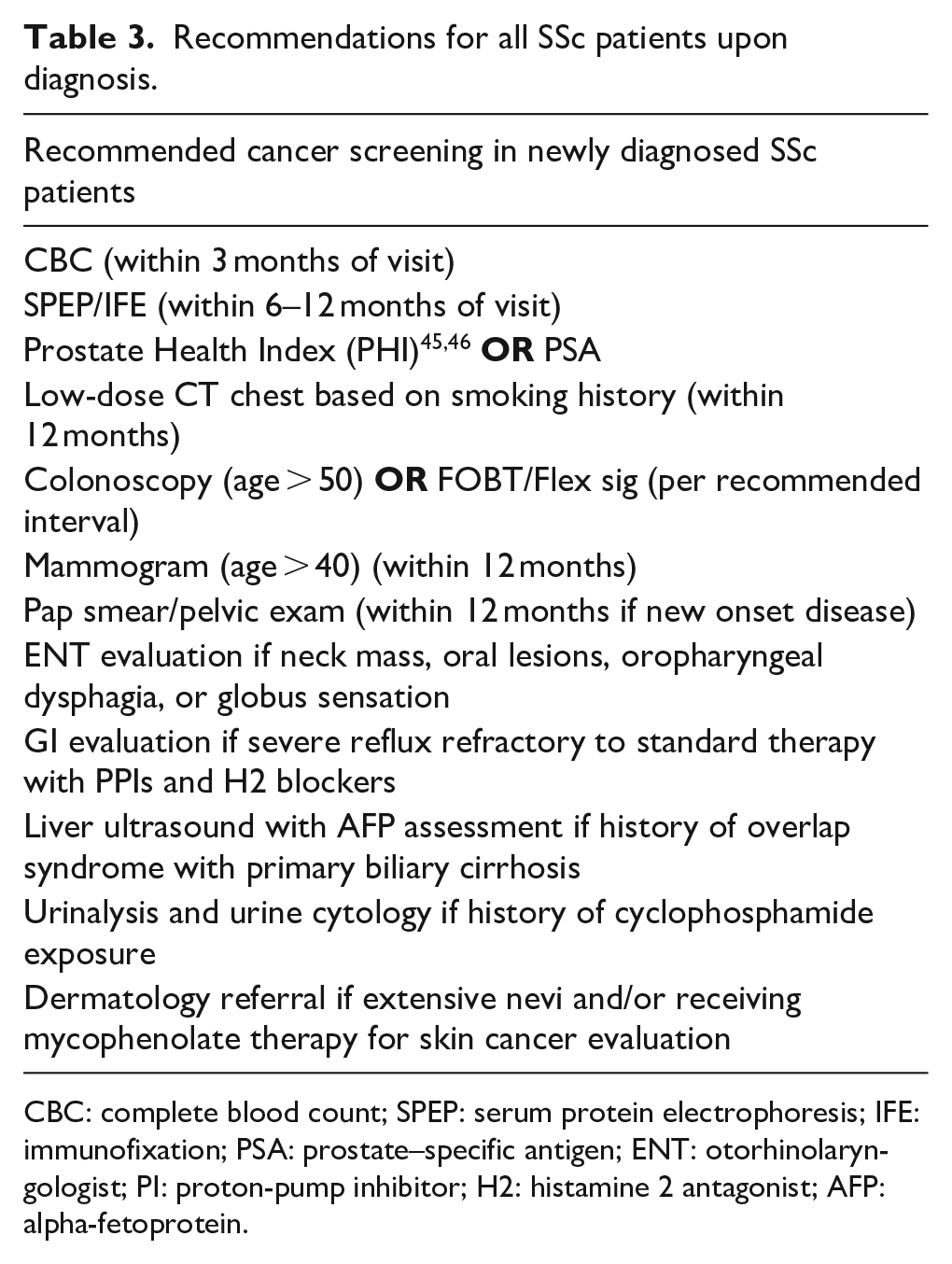
CBC: complete blood count; SPEP: serum protein electrophoresis; IFE: immunofixation; PSA: prostate–specific antigen; ENT: otorhinolaryngologist; PI: proton-pump inhibitor; H2: histamine 2 antagonist; AFP: alpha-fetoprotein.
The EUSTAR group has generated cancer-screening recommendations for anti-RNApol3-positive patients based on a Delphi exercise of 82 SSc experts. Their recommendations included a specific focus on breast cancer and heightened vigilance in the 2–5 years following SSc-symptom onset. This includes ultrasound or MRI “when needed.” The Delphi further yielded consensus that serum tumor markers are not useful for screening every patient, and that PET/CT may be considered when “unspecific systemic signs suggest the possible presence of neoplasms.” 30
A word of caution should be mentioned on adopting any of the above recommendations, as all of them are eminence-based rather than based on systematic, prospective studies. Until data-driven guidelines are developed, clinicians will need to be cognizant of the risks of both false-positive and false-negative findings on cancer-screening tests.
Summary
Recent studies have focused on SSc patient subgrouping based on the application of relevant filters (such as autoantibody status) to meticulously phenotyped patient cohorts. This has led to important new understanding of SSc disease pathogenesis and the malignancy relationship. Ultimately, it is hoped that these insights will enable improved cancer-screening strategies to be rationally designed and implemented in SSc patients. Further validation studies in different cohorts are required to properly risk-stratify patients, and prospective studies of various cancer assessment strategies are warranted. Finally, carefully conducted studies at the cancer–scleroderma interface may provide valuable insight into mechanisms of natural anti-tumor immunity and cancer-induced autoimmunity in the rheumatic diseases.
Footnotes
Acknowledgements
The Editor/Editorial Board Member of JSRD is an author of this paper, therefore, the peer review process was managed by alternative members of the Board and the submitting Editor/Board member had no involvement in the decision-making process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Scleroderma Research Foundation and NIH/NIAMS R01 AR073208, P30-AR070254, and K23 AR075898. C.M. receives support from the Jerome L Greene Foundation and is a Clinician Scientist Award recipient from Johns Hopkins University.