
Abstract
Background:
Systemic sclerosis is a fibrotic disease. Body image assessments could be key in optimizing care; however, data are scarce. The main objective was to assess the perception of aesthetic impairment using a visual aesthetic evaluation scale in patients with systemic sclerosis compared with healthy subjects. The secondary objectives were to assess associations between the perception of aesthetic impairment and scores on standardized questionnaires for aesthetic impairment as well as clinical, psychological/quality of life, and functional parameters of patients with systemic sclerosis.
Methods:
This study evaluated and compared the perception of aesthetic impairment in two populations: patients with systemic sclerosis from a referral center at Lille Hospital, France, and healthy controls.
Results:
This study included 88 patients (69 (78.4%) women) with a median age of 52 years and 88 controls (49 (55.7%) women) with a median age of 45 years. The perception of aesthetic impairment assessed using the aesthetic evaluation scale was poorer in systemic sclerosis patients than in controls (3.7 ± 0.3 vs 2.8 ± 0.3, p = 0.028) and was statistically correlated with assessments using the adapted satisfaction with appearance, a specific aesthetic impact assessment questionnaire for patients with systemic sclerosis. Patients with anxiety or depressive symptoms had significantly higher aesthetic evaluation scale scores. Systemic sclerosis patients with facial involvement and pitting scars had a worse perception of aesthetic impairment. Compared with healthy controls, systemic sclerosis patients had a worse perception of aesthetic impairment, especially systemic sclerosis patients with anxiety or depression and those with facial and hand involvement.
Conclusion:
The aesthetic evaluation scale appears to be an easy-to-use tool to evaluate body image. Correlations of the aesthetic evaluation scale score with psychological and quality of life parameters reflect the importance of these parameters for body image evaluation and its complex assessment.
Trial registration:
Clinical Trial NCT03271320 (Registered 9 January 2017, https://www.clinicaltrials.gov/ct2/show/NCT03271320?term=NCT03271320&cntry=FR&draw=2&rank=1).
Introduction
Systemic sclerosis (SSc) is a fibrotic autoimmune disease that mainly affects women between the ages of 40 and 60 years, with a prevalence estimated between 50 and 200 cases per million persons. 1 Fibrosis involvement of the skin is more or less extensive, characterizing “diffuse” or “limited” SSc, respectively. SSc patients can present with internal organ involvement. 2 Skin involvement is assessed by the modified Rodnan skin score (mRSS), which reflects the severity of the disease. 3 Skin involvement is also represented by Raynaud’s phenomenon, 2 sclerodactyly, telangiectasia, 4 calcinosis, 5 or pigmentation disorders. 6 Facial involvement is characterized by a possible loss of expression lines, the loss of the nasolabial fold, and the accentuation of perioral wrinkles, as well as wasting of the temporal and neck muscles. Management of these facial modifications includes CO2 laser techniques with a grade 4 level of evidence 7 or plastic surgery. 8 Obviously, skin involvement and especially facial localization of the disease can affect body image, with various consequences.
The concept of body image is defined as a mental image, describing both the physical and psychological personality that a person develops both by himself or herself and through others. To assess body image, the purpose is to objectively “measure” it not only through physical parameters but also through psychological parameters. 9 These interactions become more complex when a pathology modifies a person’s physical appearance with more frequently negative emotions (such as anxiety), negative thought mechanisms (such as excessive fear of pejorative evaluation), negative self-concept (NSC) (associating low self-esteem and negative self-image), and negative behaviors (such as social avoidance). 10
Benrud-Larson et al. 11 found a positive correlation between depressive symptoms and aesthetic impairment for patients with SSc assessed by the Satisfaction With Appearance (SWAP) scale, 12 a questionnaire validated for burn-injured populations. Correlations among age, dissatisfaction with self-image, and depressive symptoms were significant. Kwakkenbos et al. 13 reported that fear of disease progression and low appearance self-esteem were correlated with depression and affecting anxiety in patients with SSc. The prevalence of anxiety among SSc patients is correlated with digital ulcers. 14 In the study by Amin et al., 15 changes in facial appearance were found to be correlated with both the Derriford Appearance Scale-24 (DAS-24) score and the Hospital Anxiety and Depression Scale (HADS) score. Out of 303 patients with SSc, 76% considered telangiectasia and 73% considered thin lips to be anxiety-inducing. 16
A meta-analysis by Thombs et al. 17 summarized the prevalence of depression in patients with SSc, as assessed in eight studies in various countries using different scales, all converging toward a high prevalence of depressive symptoms in SSc patients; 46% to 65% of SSc patients were determined to have depression according to the Beck Depression Inventory (BDI) questionnaire, higher than in a population with severe burns, 18 and 38% were determined to have depression according to the HADS, higher than in patients with other chronic inflammatory rheumatisms (11%–17%).19,20
Assessments of body image are crucially important to optimize care21,22 for patients with SSc. Nguyen et al. 23 investigated anxiety/depressive symptoms as the primary objective and quality of life and aesthetic impairment as secondary objectives in SSc patients. The aesthetic evaluation scale (AES), a rapid tool, is rated on a scale ranging from 0 (no aesthetic impact) to 10 (maximum perception of aesthetic impairment). Heinberg et al. 24 validated an aesthetic impact assessment questionnaire for patients with SSc, the adapted satisfaction with appearance (ASWAP) scale. To our knowledge, no study has evaluated the perception of aesthetic impairment as a primary endpoint for patients with SSc.
The main objective of our study was to assess the perception of aesthetic impairment in patients with SSc compared with a control group of healthy subjects using the AES developed by Nguyen et al. 23 The secondary objectives were to assess associations between the perception of aesthetic impairment, evaluated using the AES, and scores on standardized questionnaires for the assessment of aesthetic impact (including the ASWAP scale (24)) and to evaluate associations of the perception of aesthetic impairment with clinical, biological, psychological, and functional parameters of patients with SSc to evaluate both body image and aesthetic impairment.
Methods
Patients and procedures
The “Sclero-esthet” study was a descriptive single-center epidemiological study that was performed in the Department of Internal Medicine, National Referral Center for systemic diseases and rare autoimmune diseases at Lille University Hospital, France, in 2017. Cases were consecutive patients with SSc seen during consultations or scheduled hospitalizations. Controls were healthy persons accompanying nonscleroderma patients. All consecutive participants were included, after receiving oral and written information, according to their eligibility and after signing an informed consent form. The promoter submitted an authorization request to the French National Agency for Medicines and Health Products Safety and obtained the favorable opinion of the ethics committee (Personal Protection Committee (CPP)) before the start of the research, in accordance with article L1121-4 of the French Public Health Code (registration number 2016 A0073546). The study is registered in Clinical Trials (ClinicalTrials.gov) (grant no. NCT03271320).
All participants had to be aged between 18 and 65 years. To be eligible for the study, patients had to have SSc meeting the American College of Rheumatology (ACR)-European League Against Rheumatism (EULAR) 2013 criteria, regardless of severity. Patients with any of the following connective tissue diseases were not included: rheumatoid arthritis, 25 Sjögren syndrome, 26 systemic lupus erythematosus, 27 and mixed connective tissue disease syndrome. 28 Controls with any connective tissue disease were not included. For all participants, any history of a serious psychiatric pathology leading to hospitalization in a psychiatric ward was considered an exclusion criterion, as was any reported acquired (e.g. burn) or congenital aesthetic malformation.
For all patients and controls included in the study, the following data were collected: demographic information (age, sex, number of children, tobacco use, and level of education), current treatments, family history, and lifestyle factors (marital status and occupation). For patients, an overall assessment of SSc was performed, which included the following: year of onset of Raynaud’s phenomenon; year of the first manifestation of SSc other than Raynaud’s phenomenon; treatment for SSc; skin involvement: the mRss, calcinosis, telangiectasia, and skin ulcers; the Medsger score; the European Scleroderma Activity (EUSTAR) score; and cardiopulmonary and digestive involvement.
Measures
All volunteer participants completed the following self-administered questionnaires once via a paper form, which took approximately 30 min to complete.
1. Evaluation of aesthetic impairment:
● The overall assessment of the perception of aesthetic impairment was, for both cases and controls, quantified by the AES, a semi-quantitative scale with scores ranging from 0 to 10 (a value of 10 corresponded to a maximum alteration in a patient’s perception of aesthetic impairment). 23 Patients were asked to answer the following question: “Please rate what you consider to be the alteration in your aesthetic appearance by drawing a vertical line on the following scale.”
● The ASWAP scale questionnaire 24 is divided into two parts: an individual’s perception of each area of their body (eight items) and the social impact caused by their self-image (seven items). Scores range between 0 and 90, with the highest values indicating maximum dissatisfaction. For the purposes of this study, the questionnaire was translated into French and then validated using a process of back-translation into English until the two versions matched.
● The Derriford Appearance Scale-59 (DAS-59) questionnaire, 29 comprising an overall assessment of appearance and an assessment focusing on physical discomfort reported by a patient. The questionnaire explores the following dimensions: general self-consciousness of appearance (GSC), social self-consciousness of appearance (SCL), sexual and bodily self-consciousness of appearance (SBSC), NSC, facial self-consciousness of appearance (FSC), and full-scale (FS). Scores for each category range from 0 to 5, with higher values reflecting maximum discomfort.
● The Multidimensional Body-Self Relations Questionnaire (MBSRQ) 30 comprises 34 items divided into the following subcategories: satisfaction with appearance, importance given to appearance, satisfaction with areas of the body, concerns about being overweight, and self-classification of one’s weight. This questionnaire 31 is an indicator of a subject’s investment in their appearance, with high values reflecting an individual’s satisfaction with their self-image.
2. Anxiodepressive symptoms were assessed using the HADS, 32 comprising 14 items rated from 0 to 3. These items are equally divided into two categories: anxiety symptoms and depressive symptoms. For each category, a total score more than 7 33 indicates the presence of that category of symptoms.
3. Self-esteem was assessed using the Rosenberg Self-Esteem questionnaire, comprising 10 items indicating either a negative or a positive view of oneself. Scores range between 10 and 40; values below 30 indicate low self-esteem. 34
4. Measure of function was assessed using the following:
The health assessment questionnaire (HAQ) 35 was used to assess overall functional capacities across eight domains (clothing, body care, getting up, feeding, walking, hygiene, catching, grasping, and other activities). The rating for each of the eight categories corresponds to the highest score for the questions in that category. The total score obtained is between 0 and 3. The functional index is the sum of the ratings of the various categories divided by the number of categories assessed; the highest scores indicate maximum disability. The scleroderma health assessment questionnaire (sHAQ) has specific questions to evaluate the functional impact linked to SSc symptoms. 36
5. Quality of life was assessed using the following:
The 36-item short-form health survey (SF-36) 37 evaluates eight dimensions: physical functioning, physical limitation, physical pain, general health, vitality, social functioning, emotional limitation, and mental health. Each dimension is rated from 0 to 100, with high values indicating a better health status.
All questionnaires have been validated in the literature, and the ASWAP and AES are specific to SSc.
Statistical analysis
The results are expressed as the mean (standard deviation (SD)) or as the median (interquartile range (IQR)) for quantitative variables and as the number (percentage) for categorical variables. The normality of distribution was assessed graphically using the Shapiro‒Wilk test.
Comparisons between cases and controls were performed using the Mann‒Whitney U test for quantitative or ordinal variables and the chi-square test (or Fisher’s exact test for cell frequencies <5) for categorical variables. Comparisons were further adjusted for age and sex using analysis covariance (on rank-transformed data with a non-Gaussian distribution) for quantitative variables and multiple logistic regression analysis for binary variables.
Statistical associations were performed using Pearson’s correlation test or Spearman’s rank correlation test (in cases of a non-Gaussian distribution) for quantitative or ordinal variables and with the Mann‒Whitney U test for categorical variables.
The associations and comparisons made are summarized in Figure 1.
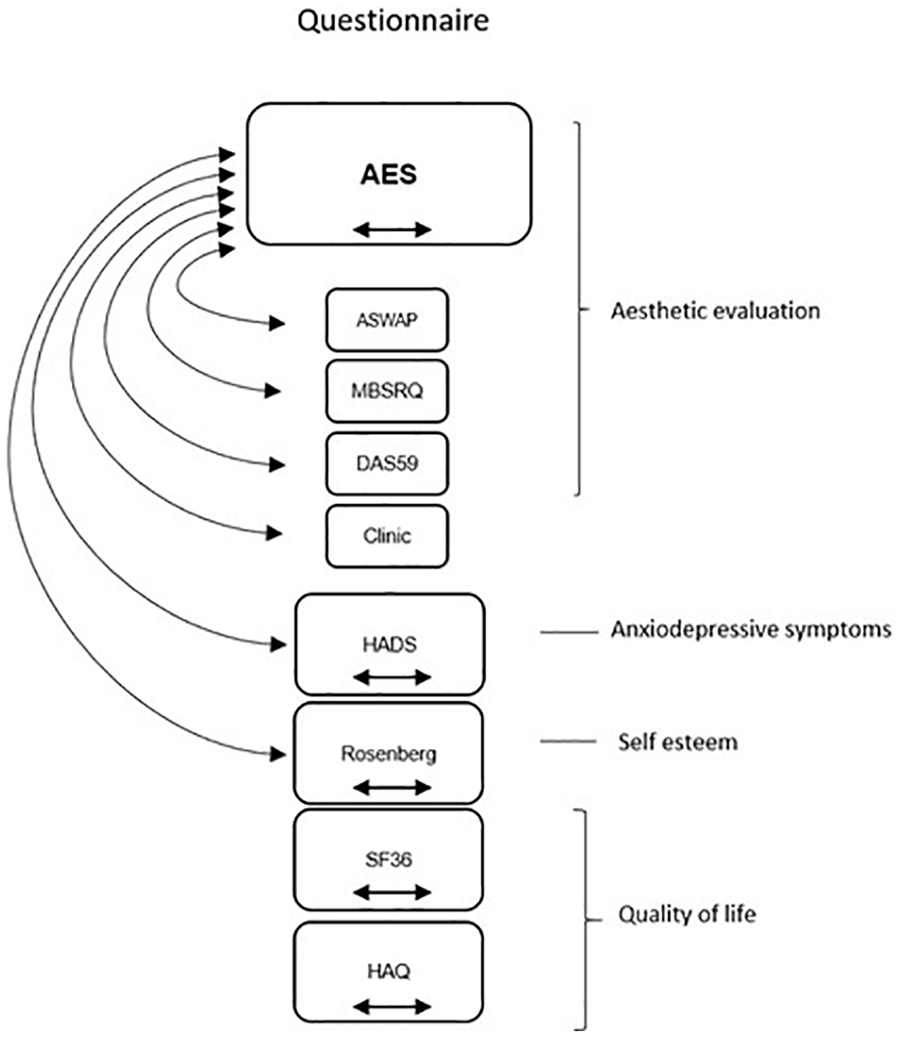
Representation of intragroup correlations and intergroup analysis. Side arrows indicate statistical correlations made. Horizontal arrows indicate comparisons made between cases and controls.
Statistical testing was performed at the two-tailed α level of 0.05. Data were analyzed using SAS software, version 9.4 (SAS Institute, Cary, NC). We estimated the common SD to a score of 3 on the AES between cases and controls. Under these conditions, with a power of 90% and an alpha risk of 5%, we recruited 88 patients and 88 controls.
Results
Between January and October 2017, 180 individuals were assessed for eligibility (four were excluded because of overlap with other autoimmune diseases) (Figure 1(b)). Eighty-eight patients (69 (78.4%) women) with a median age of 52 years (43–59) were included, along with 88 controls (49 (55.7%) women) with a median age of 45 years (32–55). Among the controls, seven (8%) were followed up in the hospital’s psychiatry department (but without hospitalization) (4 (4.5%) for depression, 1 (1.1%) for bipolar disorder, and 2 (2.3%) for burnout); two (2.3%) had psoriasis; one (1.1%) had undergone surgery for breast cancer; one (1.1%) had undergone bariatric surgery; and one (1.1%) had undergone plastic surgery of the abdomen. The main characteristics of the cases and controls are shown in Table 1. Compared with controls, cases were older, more often women, and less often involved in professional activities. A significant difference in smoking status was also found, with cases being less often current smokers and more often former smokers than controls. The clinical characteristics of the cases are summarized in Table 2.
Main characteristics of cases (SSc patients) and controls.
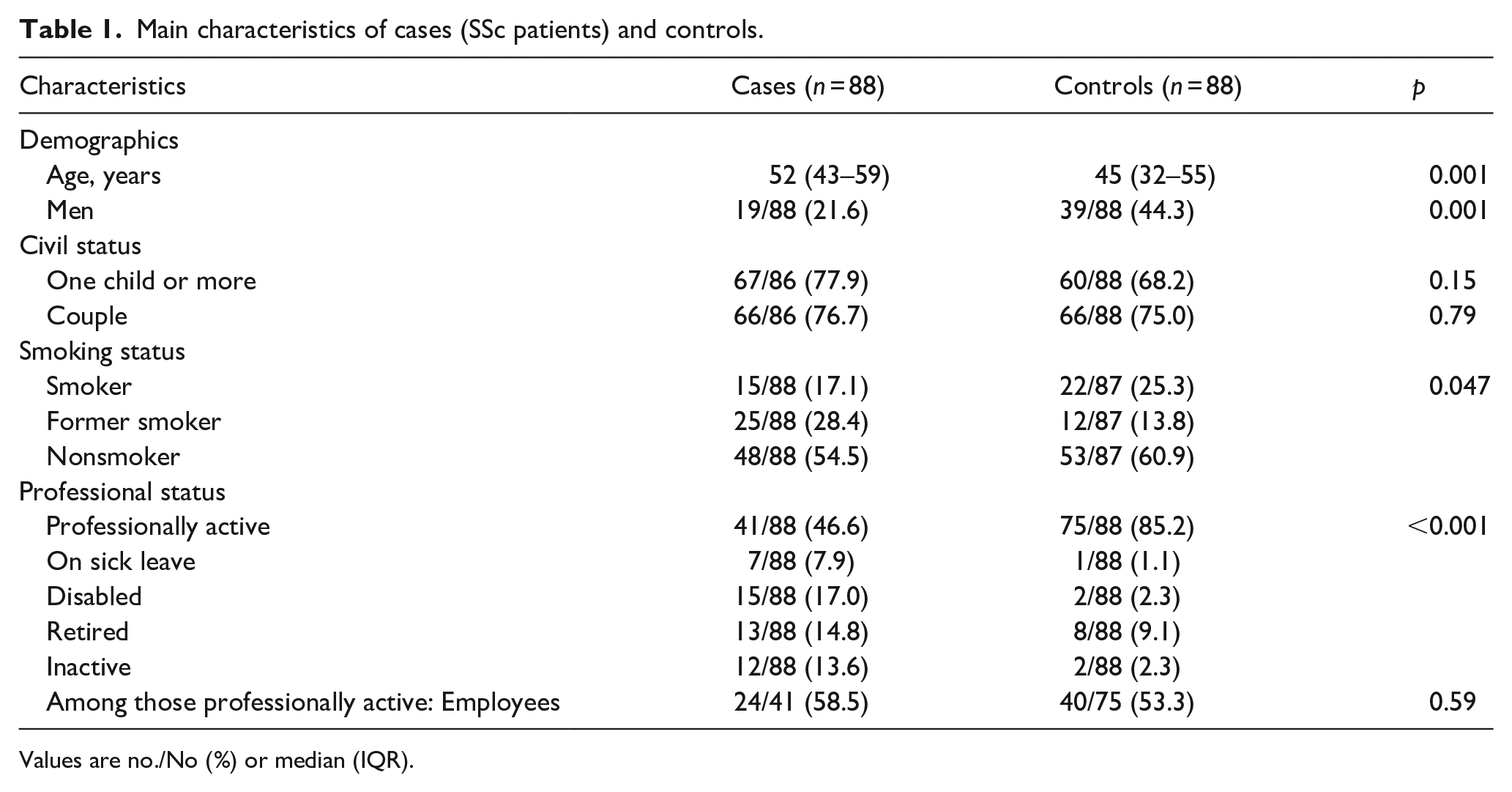
Values are no./No (%) or median (IQR).
Clinical characteristics of cases.
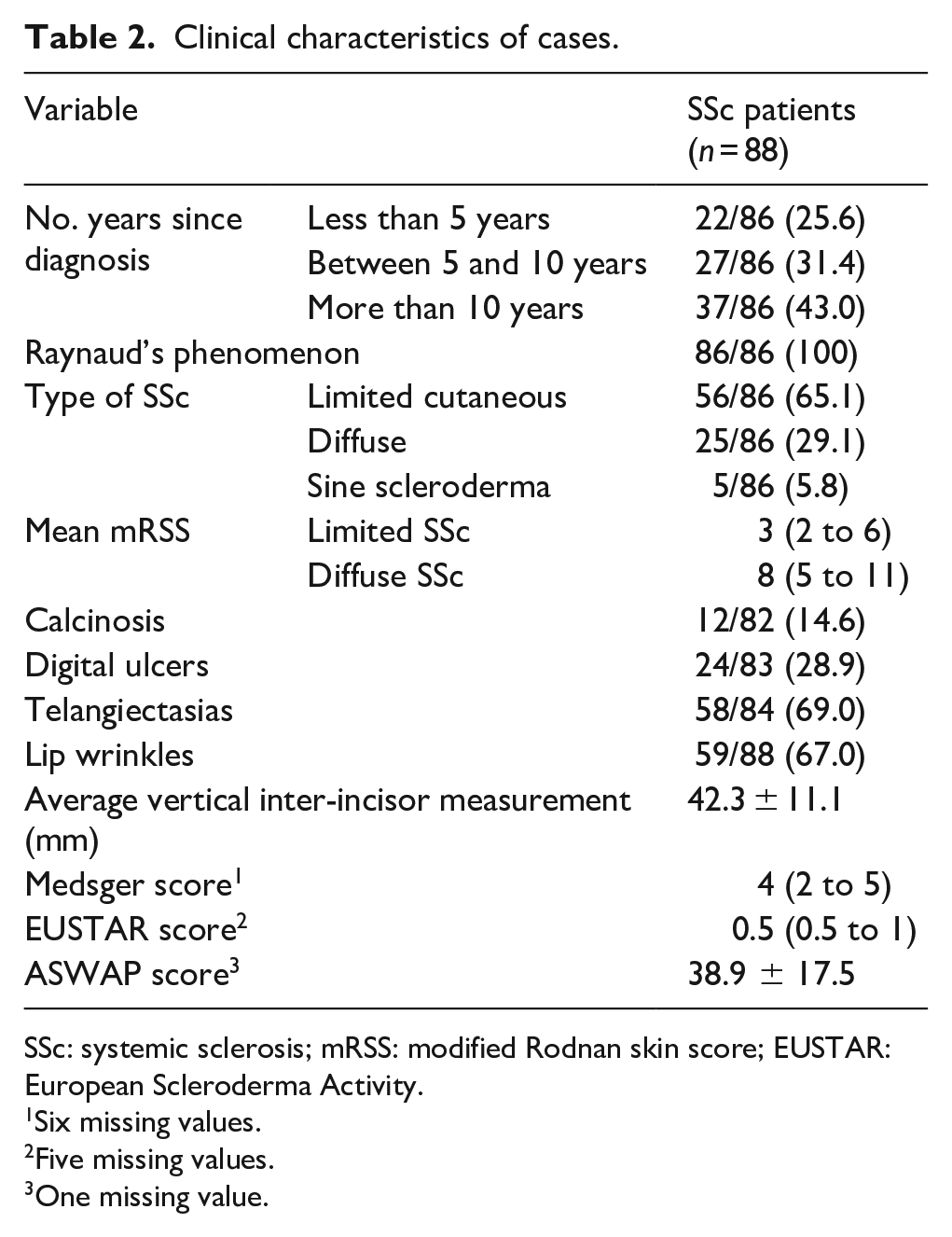
SSc: systemic sclerosis; mRSS: modified Rodnan skin score; EUSTAR: European Scleroderma Activity.
Six missing values.
Five missing values.
One missing value.
Comparisons between cases and controls
All participants completed the entire questionnaire without missing data. As shown in Table 3, concerning the main objective of the study, SSc patients had a higher AES score than controls (3.7 ± 0.3 vs 2.8 ± 0.3, p = 0.028 after adjustment for age and sex). Quality of life, measures of function, anxiety/depressive symptoms, and self-esteem also differed between cases and controls. Sixty-two (70.5%) cases experienced physical discomfort, of whom 31 (50%) were concerned with the face, 17 (27.4%) were concerned about the hands, and 14 (22.6%) were concerned about areas potentially not visible to others. Regarding quality of life, cases presented poorer quality of life than controls, with all dimensions except social functioning and emotional well-being differing significantly between the two groups. Self-esteem was considered pathological in 44.2% of cases, compared with 23.9% of controls (p = 0.027 after adjustment for age and sex).
Comparison of aesthetic assessment, measure of function, quality of life, anxiety/depressive symptoms, and self-esteem analysis between cases and controls.
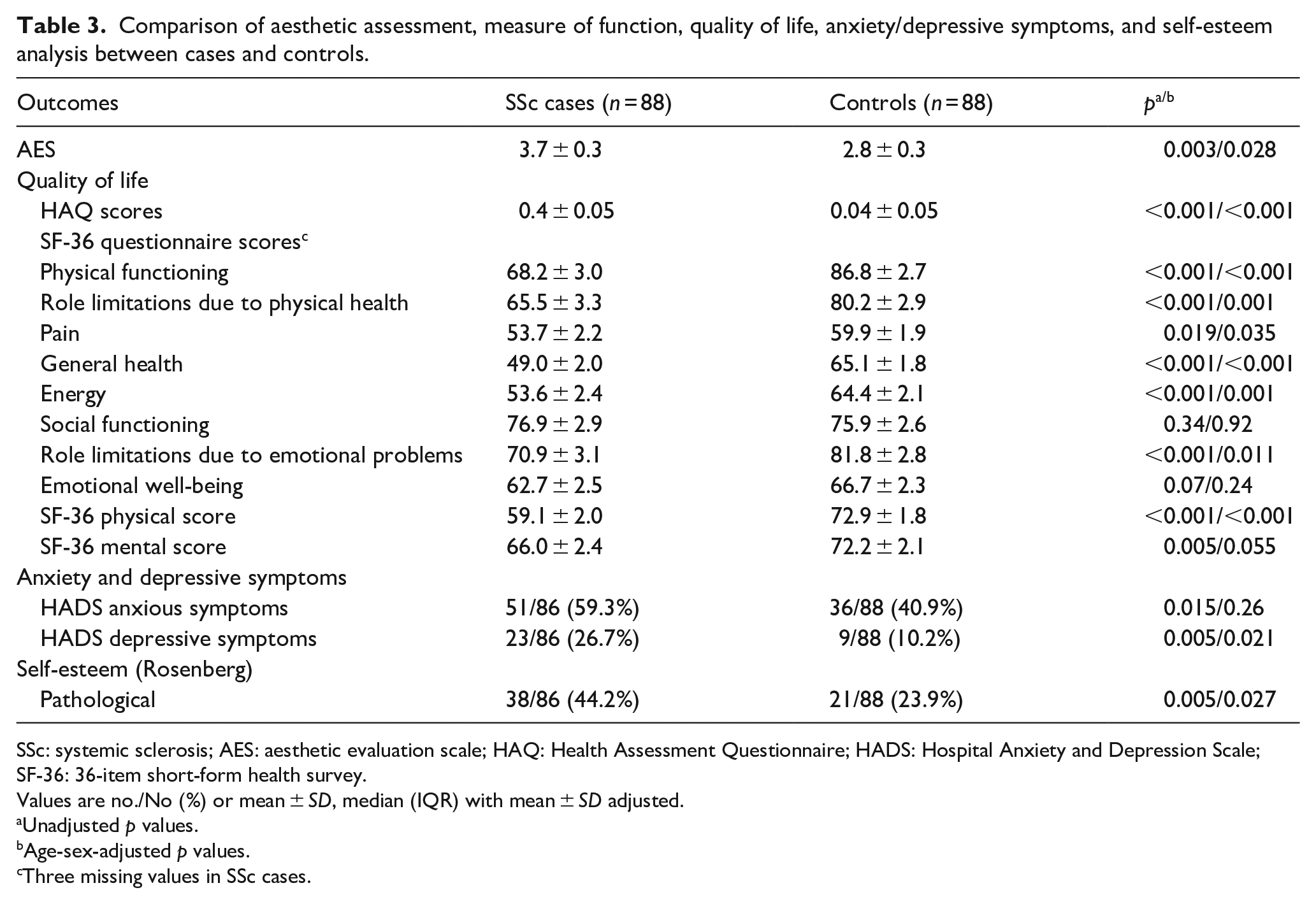
SSc: systemic sclerosis; AES: aesthetic evaluation scale; HAQ: Health Assessment Questionnaire; HADS: Hospital Anxiety and Depression Scale; SF-36: 36-item short-form health survey.
Values are no./No (%) or mean ± SD, median (IQR) with mean ± SD adjusted.
Unadjusted p values.
Age-sex-adjusted p values.
Three missing values in SSc cases.
Association of the AES and other scoring evaluations in cases
We found a significant positive correlation between AES and ASWAP scores (r = 0.55), as well as with the DAS-59 score (r = 0.30). Regarding the dimensions evaluated by the DAS-59, the strongest correlation was found for GSC (r = 0.37). However, no correlation was found between AES and MBSRQ scores; only a weak negative correlation was found with satisfaction with areas of the body (r = −0.26). The AES score was also positively associated with both the presence of anxiety symptoms and the presence of depressive symptoms (Table 4).
Association of AES with other evaluations (aesthetic evaluation, anxiety/depressive symptoms, and self-esteem) in SSc cases.
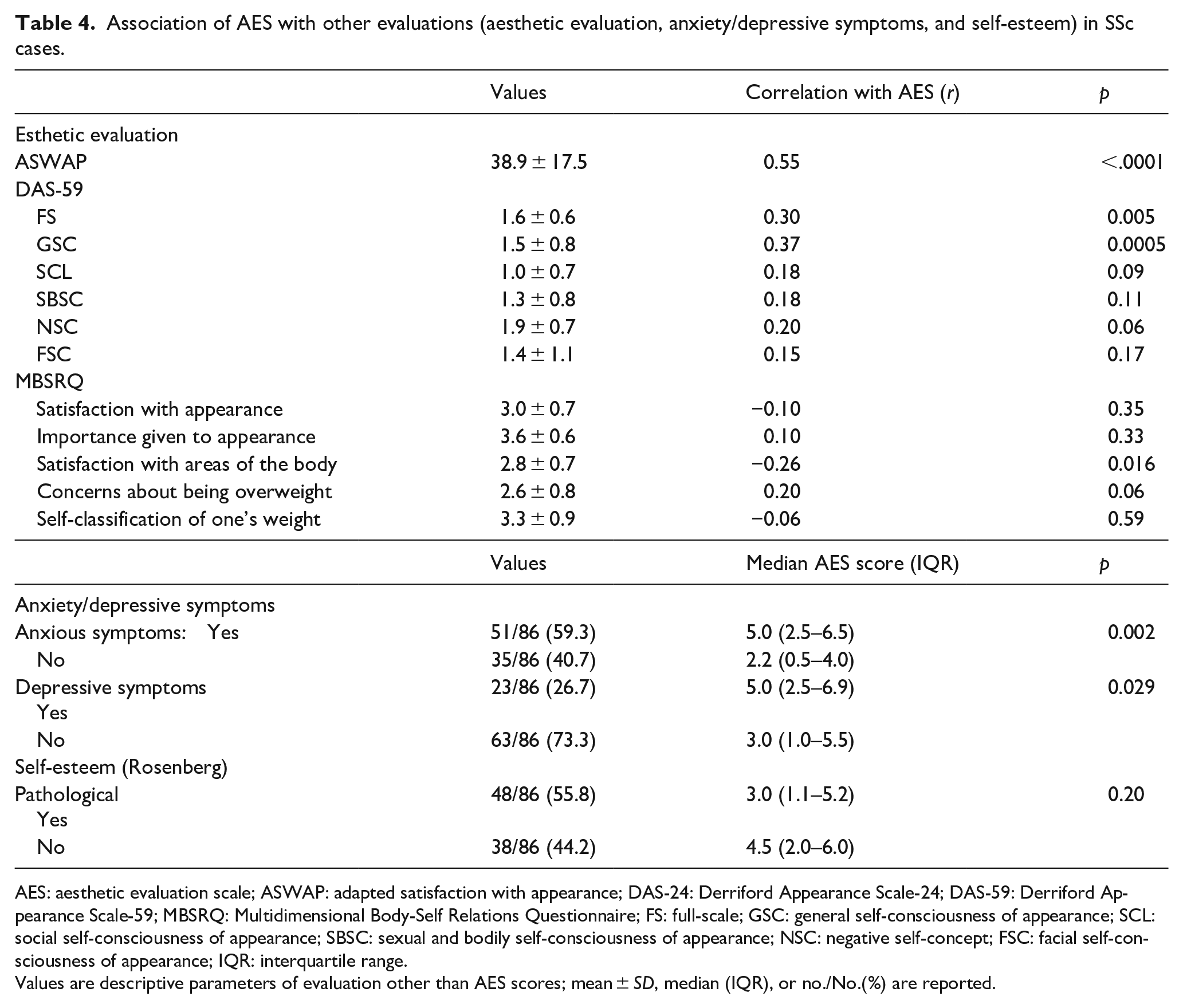
AES: aesthetic evaluation scale; ASWAP: adapted satisfaction with appearance; DAS-24: Derriford Appearance Scale-24; DAS-59: Derriford Appearance Scale-59; MBSRQ: Multidimensional Body-Self Relations Questionnaire; FS: full-scale; GSC: general self-consciousness of appearance; SCL: social self-consciousness of appearance; SBSC: sexual and bodily self-consciousness of appearance; NSC: negative self-concept; FSC: facial self-consciousness of appearance; IQR: interquartile range.
Values are descriptive parameters of evaluation other than AES scores; mean ± SD, median (IQR), or no./No.(%) are reported.
Association of AES scores and the clinical characteristics of SSc
A statistically significant difference was found between the AES scores of patients with and without perioral radiated wrinkles (median (IQR) = 4.5 (2.5–6) and 2.2 (1–5), p = 0.045), as well as between patients with and without pitting scars (median (IQR) = 5 (3.5–7) and 3 (1–5.85), p = 0.027) (data not shown). There was a statistical difference between the AES scores of patients with and without telangiectasias (p = 0.053). There was no difference in the distribution of AES scores between patients with the limited cutaneous form and those with the diffuse form of SSc, nor was there an association with the mRSS. We did not find a significant association between AES scores and the following: other clinical characteristics of SSc, including calcinosis, ulcers, and vertical interincisor measurements; the Medsger score; the EUSTAR score; and visceral lesions related to SSc (cardiopulmonary and digestive impairment).
Discussion
SSc is a chronic autoimmune disease resulting in fibrosis of the dermis, which induces visible and palpable modifications of the skin. We assessed patients’ perceptions of these physical changes using the AES score, which was the primary endpoint of the study. Using this scale, we showed that SSc patients presented a greater perception of aesthetic impairment than controls. The results of the AES were correlated with results of the ASWAP, a specific questionnaire not yet used in the literature for the evaluation of aesthetic impairment in SSc patients. The AES results were correlated with symptoms of anxiety and depression. SSc patients reported poorer quality of life than controls. The AES appears to be an easy tool to evaluate body image and the perception of aesthetic impairment in patients with SSc.
Body image is not limited to a mental body image and must also take into account cognitive and behavioral dimensions. 38 This is how Thompson 39 defined methodological strategies in body image studies, insisting on the choice of general versus specific questionnaires and on the components that should be evaluated. We chose the three questionnaires based on the following: the DAS-59 due to its mixed assessment, including both a global assessment and an assessment focused on a physical complex; the ASWAP due to its specificity for SSc; and the MBSRQ due to the assessment of an individual’s investment in their appearance.
The AES is a rapid and easy-to-use assessment tool for measuring aesthetic impairment associated with SSc
The results of the ASWAP questionnaire, the only aesthetic evaluation questionnaire specific to SSc, were correlated with those of the AES. Although this questionnaire has already been validated in the literature, 24 it has, as far as we are aware, never been used. The AES was correlated with the overall “FS” score of the DAS-59, a benchmark test for evaluating aesthetic impairment. Evaluation of the discomfort felt by patients essentially revealed discomfort of the face and hands, with a description compatible with dermatological lesions of SSc (“red spots on the face, swollen hands, and wrinkles around the lips”). However, the DAS-59 questions on the Assessment of Investment in Facial Aesthetics (FSC) were not significantly correlated with the AES. This could be explained by the fact that questions in this category relate to elements not adapted to the patient experience in the case of SSc, 29 with questions like “you are unable to change your hairstyle or you avoid having wet hair.”
The AES score correlates with visible signs of SSc
The presence of radiated folds was correlated with the AES results. This suggests that visible damage could be the most disturbing for patients, tying in with the body image concept as defined in the literature with others’ approval predicting body concerns. 40 Although not quantifiable, physical complexes reported in the DAS-59 were also visible signs, namely damage to the face and hands. The AES was used in a study to evaluate the aesthetic impact of digital ulcers; patients with digital ulcers had higher scores than patients without digital ulcers. 41 We did not find a correlation between clinical signs of the disease (calcinosis, telangiectasias, and mRSS score) and the AES score. However, the prevalence of these complications was quite low, and our study may have lacked the power to find a significant correlation. Likewise, disease activity scores or internal organ involvement did not correlate with the AES score, suggesting that visceral involvement does not deeply impact body image.
Correlations with psychological parameters make the AES an easy tool to use to evaluate body image
In 2014, Nguyen et al. 23 evaluated the aesthetic impact of SSc in patients using the same scale but without a control group. The median score in their study was 5 (3–7), a value close to that in our study, namely 3.9 (1.55–6). Their study focused on the evaluation of anxiety/depressive symptoms in patients with SSc; aesthetic evaluation was, therefore, a secondary objective but still allowed them to reveal a previously unknown aspect of the management of the disease. The perception of aesthetic alterations appears not only to be linked to visible aspects of the disease but also underpinned by notions including a psychological aspect relating to the image perceived by society. Thus, it was important to assess anxiety/depressive symptoms and self-esteem. The prevalence of depressive symptoms, as assessed by the HADS, was significantly higher in cases than in controls, with values comparable to those in the literature. 42 We did not find differences in anxiety symptoms between the two groups. The prevalence of anxiety symptoms found among controls in our study was higher than that reported in the general population, 43 possibly explained by hospital recruitment. 44 Psychological impairment in SSc patients, therefore, does not seem marginal in self-image assessments. Thombs et al. 18 showed that self-image contributed to depressive symptoms in a severe burn population years after the trauma caused by the accident and despite surgical management. As SSc is a chronic disease, the influence of depression on body image and its reciprocity is more complex to define due to the slow progression of the disease. A follow-up of anxiety and depression in patients with SSc over time could provide some answers.
The image of oneself, when it is related to physical identity, is, therefore, assimilated to the image of our body that we perceive and to our interpretation of it. Psychologically, it is related to self-esteem, which depends on the degree of cohesion between aspirations and reality at a given time. In our study, SSc cases had lower self-esteem than controls. It has already been shown that there is a strong link among self-esteem, acceptance of the disease, and coping in people with SSc.45,46 van Lankveld et al. 45 also found that “active” coping styles, that is, problem-oriented coping methods, were associated with improved self-esteem in patients with SSc. 46 It would be interesting to evaluate the strategies developed by patients in our study to adapt to aesthetic changes induced by the disease. van Lankveld et al. 45 also looked at the cognitive capacities of patients with SSc, particularly the processes by which an individual acquires awareness of a disease; they found that better acceptance of the disease was related to better self-esteem. This finding could explain the lack of correlation between the scores on the Rosenberg Self-Esteem questionnaire and the results on the AES in our study. In contrast, resignation, a form of giving up, was associated with low self-esteem. This finding may help to explain the lack of correlation between the MBSRQ and visual AES scores; the MBSRQ assesses an individual’s investment in their appearance, that is, the strategies developed to deal with dissatisfaction with appearance. We, therefore, see the importance of connecting cognitive processes and strategies developed by an individual who is faced with changes in their appearance.
As these processes are also influenced by the environment, patients had higher scores than healthy subjects on the HAQ. This reflects the physical limitations induced by the disease, as shown in the study of Poole et al. 47 In our study, the physical limitations of SSc cases, as measured by the HAQ, were statistically significant compared with those of controls. These limitations, impacting quality of life, introduce the notion of a “disabling disease,” which can give rise to a situation of disability (French law n° 2005-102,2005.)48. However, aesthetic impairment in connection with a chronic pathology like SSc is not yet recognized as an aesthetic disability, although it meets the definition.
Our study has limitations. It was a single-center study based on voluntary participation, thus introducing a potential bias in the self-selection of cases or controls. This risk was partly controlled for by excluding participants with acquired or congenital aesthetic defects or a history of serious psychiatric disorders leading to hospitalization. In addition, hospital recruitment of patients and controls created a possible admission bias. This can lead to an overestimation of parameters, in particular anxiety/depressive symptoms. The number of subjects included (176 in total) is a sufficiently representative sample of the two populations. The systematic comparison with the control group is the main strength of this study, allowing us to analyze correlations between the parameters evaluated. Older age and a higher proportion of males among the controls may introduce a bias in body image evaluation, which was partially addressed with statistical adjustment. In our study, we evaluated all parameters at a given time, which did not allow us to analyze the questionnaires’ sensitivity to change. Prospective longitudinal studies are needed to assess causal links between aesthetic impact in SSc patients and psychological aspects, especially since body image is generally not very resistant to change. 49 The choice of questionnaires can also be discussed. Indeed, the HADS and the Rosenberg Self-Esteem Questionnaire are aimed at screening for psychological disorders. They cannot replace structured interviews by a specialist in the analysis of a disorder. However, our data on anxiety and depressive symptoms in patients with SSc remain superimposable on the prevalence reported in the literature. Our results could usefully be enriched by additional tests to evaluate patient coping strategies and personality traits. 45
Conclusion
The perception of aesthetic impairment assessed using the AES was poorer in SSc patients than in healthy individuals. The AES appeared to be a good evaluator of body image in patients with SSc, reflecting dissatisfaction linked to psychological, social, and functional dimensions. The AES could thus become a tool for use during clinical assessments to better meet the needs of patients, both physically and through individualized psychological care. In addition to symptomatic treatment, consideration of aesthetic damage associated with SSc should focus on the following two areas: the physical and psychological dimensions. Depending on the predominant parameter, patients would be referred to a specialist, including psychologists, psychiatrists, dermatologists, or plastic surgeons, for physical, psychological, or even combined treatment. This could make the care pathway more efficient and provide solutions for patients’ unmet needs.
Footnotes
Author contributions
M.-M.F. collected the data and wrote the paper. P.G. and S.M.-D. conceived the analysis. V.D. and J.L. performed the analysis. S.S., V.S., E.H., and O.C. conceived the analysis. D.L. collected the data and wrote the paper.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate: Trials registration
The promoter submitted an authorization request to the French National Agency for Medicines and Health Products Safety and obtained the favorable opinion of the ethics committee (Personal Protection Committee (CPP)) before the start of the research, in accordance with article L1121-4 of the French Public Health Code (registration no. 2016 A0073546). The study is registered in Clinical Trials (ClinicalTrials.gov) (grant no. NCT03271320).