
Abstract
The use of immune checkpoint inhibitors has been increasing rapidly. Numerous untoward immune-related adverse events due to immune checkpoint inhibitors have been reported. Acute interstitial nephritis due to immune checkpoint inhibitors is one of these immune-related adverse events. Although gold standard, it is not always straightforward to perform a kidney biopsy in oncological patients. Helpful diagnostic methods are lacking. In this case report, we discuss the potential role of positron emission tomography–computed tomography on supporting the diagnosis of acute interstitial nephritis or ruling it out in the setting of acute kidney injury following treatment with immune checkpoint inhibitors. Studies are needed to assess the possible role of positron emission tomography–computed tomography for the diagnosis of acute interstitial nephritis in these subjects.
Keywords
Introduction
Immune checkpoint inhibitors (ICIs) have dramatically improved outcomes of patients with several types of cancers. These drugs act by inhibiting regulatory proteins, which modulate the balance between activating T-cells to enhance immune system response against foreign antigens and suppressing T-cell activation against self-antigens in order to avoid autoimmune damage. Briefly, ICIs work against the cancer cell resistance by allowing immune cells to identify and eliminate malignant cells. In addition to its benefits from an oncological point of view, this immune enhancement may lead to extensive autoimmune effects in various organ systems commonly referred to as immune-related adverse events (iRAEs). ICI-associated acute interstitial nephritis (AIN) has been reported by many studies to date, and its recognition has increased. However, the development of renal injury in patients with cancer can occur due to numerous causes, which may not be related to the immunotherapy. Kidney biopsy is the gold standard, but in some cases, it may be contraindicated. Diagnostic imaging tools may be used to help lead to the diagnosis of AIN. Here, we present one case of acute kidney injury (AKI) in the setting of treatment with ICIs using an 18F-fluorodeoxyglucose positron emission tomography–computed tomography (FDG PET-CT) scan as an adjuvant diagnostic tool.
Report of the case
A 62-year-old male with a history of type 2 diabetes mellitus presented for an oncology outpatient visit as a routine follow-up for metastatic melanoma involving the lungs and brain. He was treated with nivolumab and ipilimumab in combination for four cycles, with the last dose given approximately 1 month prior to this visit when he was noted to have developed AKI. His serum creatinine was noted to be elevated from a baseline 0.6 up to 1.7 mg/dL. Immunotherapy was placed on hold and the patient was referred for a nephrology evaluation. At the same visit, the patient was also noted to have a further elevation of thyroid-stimulating hormone (TSH) to 72 mIU/L with free T4 undetectable, but no hypophyseal function was evaluated. He did have a history of biochemical thyroiditis (2 months prior to the AKI) with normal kidney function, and as the patient was essentially asymptomatic, no further therapy was recommended at that time. At 4 weeks prior to the AKI, patient was seen and TSH was increased to 10.2 mIU/L, free T4 of 0.6 ng/dL, and serum creatinine was still normal at 0.7 mg/dL; no thyroid hormone therapy was initiated. At the time of the diagnosis of AKI, the patient had decreased appetite, but he denied nausea, vomiting, or diarrhea. He also denied any difficulty in emptying his bladder, dysuria, increased urgency or frequency, foamy urine, or gross hematuria. There was no history of non-steroidal anti-inflammatory drug use. Serum creatine kinase was normal. Blood pressure was 124/75 mm Hg. Urinalysis revealed 1–5/ higher power field eosinophils (shown by Hansel’s stain) with occasional granular casts. Findings on renal ultrasound were unrevealing. Nivolumab and ipilimumab treatment was held, but no steroid treatment was given. The patient was started on thyroid hormone (Levothyroxine 100 mcg daily p.o.) for ICI-induced thyroiditis. With ICIs withheld, serum creatinine improved at follow-up to 1.0 mg/dL (Figure 1). FDG PET-CT scans of the patient before and after treatment with ICIs are shown in Figure 2. Coronal FDG PET/CT image demonstrated increased renal cortical activity (Figure 2(b)) following treatment with nivolumab and ipilimumab.
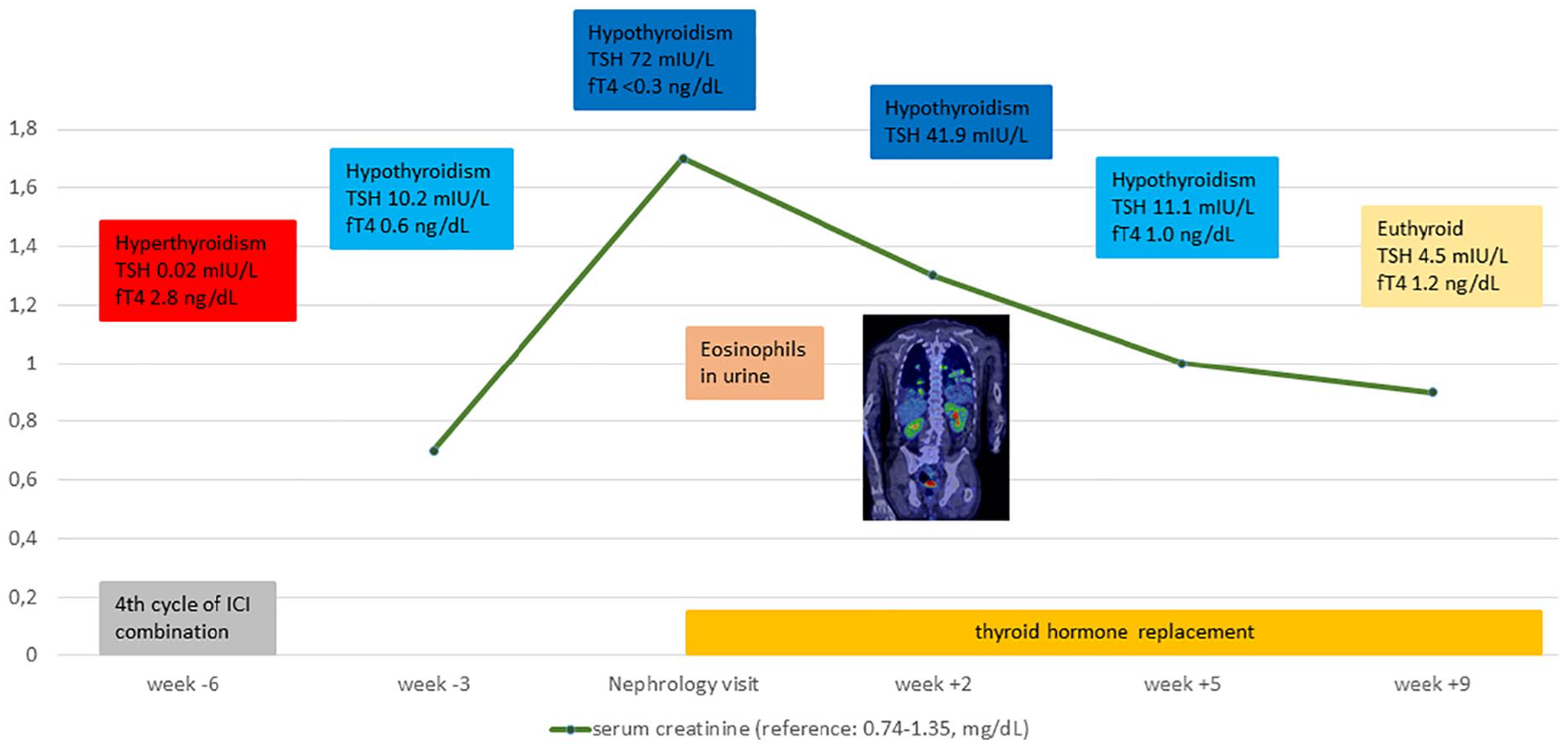
Clinical course of the patient. The development of severe hypothyroidism after treatment with immune checkpoint inhibitor and the temporal association between these events and the increase in serum creatinine are shown. Similarly, there is a temporal association between treatment of hypothyroidism and improvement in kidney function. Increase in renal cortical activity in positron emission tomography at the time of kidney injury supported a presumed diagnosis of acute interstitial nephritis.
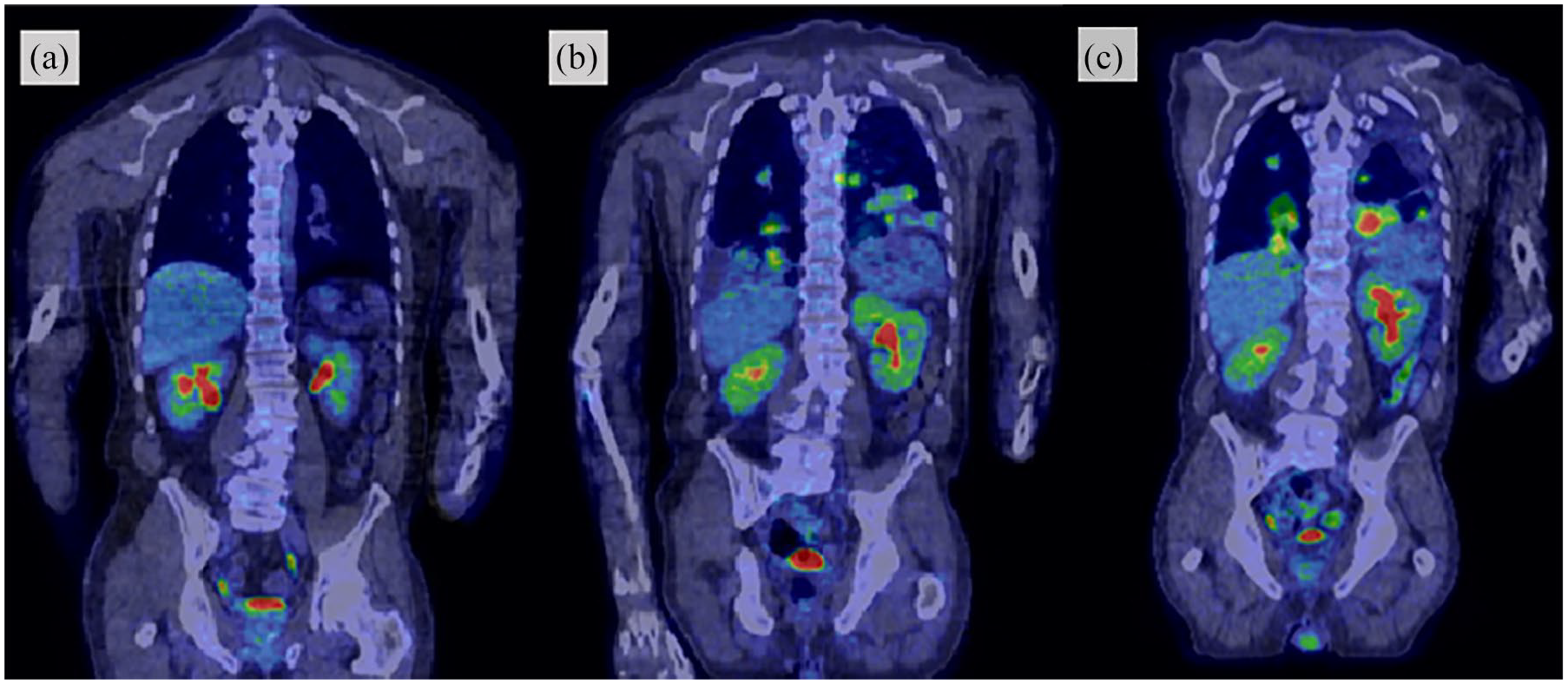
Positron emission tomography images of the patient. In comparison to baseline scan seen in (a), renal cortical activity slightly increased following treatment with nivolumab and ipilimumab as seen in (b). The decrease in renal cortical activity 4 weeks following discontinuation of ICIs was not significant as shown in (c).
Discussion
Although novel agents act in a more targeted manner, nephrotoxicity from cancer therapies is still common, contributing to the emergence of the “onco-nephrology” field. ICIs are such agents that have revolutionized the treatment of various malignant disorders. However, these agents act by inducing the immune response against tumor antigens, a response that may not be without cost. It is common for patients on ICIs to experience iRAEs, autoimmune disorders affecting many organ systems particularly the skin, gastrointestinal tract, endocrine system, as well as the liver during treatment with ICIs. Kidney involvement as a result of this autoimmune injury is not as common. However, in a meta-analysis of 48 clinical trials with a total of 11,482 patients, the relative risk of AKI following Programmed Death-1 (PD-1) inhibitors was found to be increased 4.19 times. 1 A recent retrospective observational study which included 1016 patients treated with ICIs 2 found that the rate of potential ICI-associated AKI was 3%. AIN was the most common disorder in the recent multicenter study by Cortazar and colleagues, which was shown in 93% of the 60 patients with a kidney biopsy. AIN was also the most frequent diagnosis reported by other papers.3,4
The pathophysiology of ICI-related AIN is not clear. In a typical drug-induced AIN, the hypothesized mechanism of kidney injury involves activation of circulating T-cells directly by a drug or its metabolites, which may acquire immunogenicity locally by tubular cell processing or systemically by binding to carrier proteins and forming a drug–carrier complex. In addition to similar clinical and histological characteristics with typical drug-induced acute tubulointerstitial nephritis, the longer latency period leads to the hypothesis that AKI secondary to ICIs may be due to reprogramming of the immune system subsequently leading to loss of tolerance. 3 Several studies suggested a role for a concomitant use of drugs which are well known to cause AIN, particularly proton-pump inhibitors.2,5 These observations lead to the speculation that ICIs may have broken the long-standing immune tolerance against concurrent drugs which are well-known causes of AIN. Our case was not exposed to concurrent drugs that typically cause AIN; however, he was treated with a combination of ICI therapy. It was previously shown that dual checkpoint blockade is associated not only with a stronger immune response and antitumor activity but also with a higher incidence of adverse events. Cortazar et al. also observed that the ICI drug combination therapy is an independent predictor of ICI-related AKI. 5
Temporal association with the ICI is less clear-cut in comparison to other agents causing AIN. Immune-related side effects of each organ system occur at different times following anti-PD-1 commencement. In the recent multicenter trial by Cortazar et al., median time from ICI treatment initiation to AKI was 14 (6–37) weeks. 5 The onset of kidney injury seen with PD-1 inhibitors is usually late (3–10 months) compared to cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) antagonist-related renal injury, which happens earlier (2–3 months). 4
Kidney biopsy was not available in this case, but absence of other causes (except severe hypothyroidism), presence of eosinophiluria, improvement in kidney function after holding the ICI therapy, and increased renal cortical FDG uptake on PET-CT suggested the diagnosis of AIN. FDG PET-CT scanning has been used for various indications in nephrology, including several case reports on the experience of FDG PET-CT for the diagnosis of AIN.6,7 However, the use of FDG PET-CT for the diagnosis of AIN should be studied in detail before a recommendation is made for the use of this imaging modality for AIN. Qualls and colleagues recently published a case of ICI-induced AIN. 8 In the report, it was stated that activity in the cortex of the kidney was not increased in three patients with AKI due to non-inflammatory conditions in the setting of ICI. In addition, their patient with AIN was non-oliguric, which leads to a more reliable assessment of the activity by PET-CT in the kidney. Our case was also non-oliguric with relatively milder stage of renal impairment according to serum creatinine measurements. The FDG PET-CT studies were performed for oncological follow-up purposes and not solely for the kidney. However, it is not studied whether PET-CT is reliable as a means to detect or rule out the inflammation in the kidney parenchyma in drug-induced AIN. In the report by Qualls et al., standardized uptake values maximum (SUVmax) values were reported in order to quantitatively follow the change during the time course. In fact, it may not be possible to quantify the SUVmax specific to parts of the kidney due to physiologic excreted urine activity in the adjacent renal collecting tubules and calyces. The accuracy of this measurement would be further complicated by the innumerable confounding factors, including imaging time after injection, burden of metastatic disease taking up the FDG (thus limiting amount available to the kidneys), fasting state, and injected FDG dose. In addition, even if it is possible to reliably quantify the standardized uptake values maximum (SUVmax) in the renal cortex, it still may not be specific for AIN.
Our case had marked hypothyroidism. This may be particularly relevant in subjects exposed to ICIs. Cortazar et al. reported that extrarenal adverse events occurred in 43% of the cases with ICI-induced AKI. 5 A slight increase in serum creatinine is expected in hypothyroidism. More typically, hypothyroidism may cause AKI because of rhabdomyolysis. Serum creatine kinase was not checked in our case. However, serum aspartate aminotransferase and lactate dehydrogenase were completely normal which would be quite unlikely for a patient with rhabdomyolisis. On the contrary, there have been case reports suggesting an association between hypothyroidism and acute renal failure in the absence of rhabdomyolisis. In this instance, renal failure was shown to be reversible following thyroid hormone replacement. Possible mechanisms of AKI during a hypothyroid state are not studied in detail, but experimental research showed a decreased activity of mitochondrial oxidative enzymes and change in membrane transporters in proximal tubule epithelium. 9 Since thyroid dysfunction is a common iRAE of ICI therapy, a possible association with renal impairment may be of considerable importance. In our case, beyond cessation of ICI therapy, treatment of hypothyroidism may have also contributed to improvement in serum creatinine. However, most of the cases with ICI-induced AIN require steroid therapy and frequently present with a severe increase in serum creatinine. The improvement may be partial even when glucocorticoid treatment is given and ICI therapy is held. 3 Low free T4 levels suggest a hypophyseal involvement; however, improvement with Levothyroxine replacement alone argues against involvement of the hypothalamic-pituitary-cortisol axis. In our case, in addition to increased activity on FDG PET-CT, laboratory and clinical findings such as eosinophiluria could be suggestive of the diagnosis of AIN. Potential role of eosinophiluria detected by Hansel’s stain in making the diagnosis of AIN has been proposed over three decades ago. 10 However, in a study from the Mayo Clinic, Muriithi et al. demonstrated that eosinophiluria was found in a variety of kidney diseases in addition to AIN. 11 We acknowledge that eosinophiluria is neither sensitive nor specific for the diagnosis of AIN. However, urine eosinophils may support the presumed diagnosis of AIN in conjunction with the PET scan, history of exposure to ICIs, and improvement in kidney function following discontinuation of ICIs. We cannot completely rule out that untreated hypothyroidism may have contributed for the AKI, which in some cases may occur in the absence of rhabdomyolisis. Our findings on these cases support the possibility that FDG PET-CT has potential as an adjuvant imaging tool for AIN, but until a more comprehensive study can evaluate the role of FDG PET-CT in AIN, this imaging cannot substitute for the histopathologic findings of biopsied renal tissue.
Conclusion
In conclusion, whether FDG PET-CT may help to provide imaging support for the diagnosis of AIN requires more robust comprehensive study. Severe hypothyroidism as an iRAE may contribute to renal impairment during treatment with ICI and should be considered in the differential diagnosis when encountering these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SMH is supported by National Institutes of Health K08 DK118120 from the National Institute of Diabetes and Digestive and Kidney Diseases and by a Mary Kathryn and Michael B. Panitch Career Development Award. All the other authors declared no competing interests.
Consent for publication
All patient information was de-identified and patient consent was not required.
Ethics approval and consent to participate
Need for approval was waived.