
Abstract
Crystalcryoglobulinemia refers to the extracellular deposition of crystals in the systemic vasculature, leading to vascular injury, thrombosis, and occlusion. This entity is usually described as a complication of multiple myeloma, although it can also occur in the setting of a monoclonal gammopathy of renal significance. Synchronous presentation of a monoclonal gammopathy and renal cell carcinoma is rare. Hypothetically, as both neoplasms’ growth depends on certain cytokines such as interleukin-6, it is possible that cytokine production from one neoplasm may stimulate the growth of the other. In this report, we describe a case of crystalcryoglobulinemia in a patient with a monoclonal gammopathy of renal significance and concomitant renal cell carcinoma. Additionally, we performed a systematic review of the literature and analyzed data of 61 reported cases of crystalcryoglobulinemia and of 40 reported cases describing the association between multiple myeloma and renal cell carcinoma.
Keywords
Introduction
Cryoglobulinemia is a condition characterized by the persistent presence of abnormal immunoglobulins in the serum that condensate and precipitate at temperatures lower than 37°C. These immunoglobulins (cryoglobulins) lose solubility when present at sufficiently high concentrations, resulting in condensation into aggregates, concentrated liquid phases, and rarely, into crystals. 1 The latter may be found in the bloodstream (crystalcryoglobulinemia), and deposit in several organs and tissues, most frequently in the skin and the kidneys. 2
The cryoglobulins can be monoclonal (type 1), can be a mixture of monoclonal IgM with polyclonal IgG (class 2 or mixed), or can be polyclonal IgG and IgM (class 3). Mixed or class 2 cryoglobulinemia is most commonly associated with infections (e.g. hepatitis C virus [HCV] infection) and autoimmune disorders (e.g. Sjögren syndrome). In contrast, class 1 cryoglobulinemia is usually caused by hematologic malignancies, such as multiple myeloma and lymphoproliferative disorders. 3 Less commonly, the abnormal proteins are associated with a monoclonal gammopathy of undetermined significance. 4
Here, we report a case of crystalcryoglobulinemia manifesting with skin purpura, peripheral neuropathy, and acute kidney injury, in a patient with concomitant clear cell renal cell carcinoma (RCC). Treatment and outcomes after 32 months of follow-up are also described, and we discuss the possible bidirectional association between plasma cell dyscrasias and renal cell carcinoma. 5
Case description
A 45-year-old Mexican female presented to her local hospital in August 2017 with malaise, lower limb paresthesias, Raynaud’s phenomenon, and 8 kg weight loss. She was treated with symptomatic measures without improvement. By January 2018, she developed progressive weakness and a dermatosis in her lower limbs characterized by erythematous macules progressing to a confluent purpuric rash which extended to her upper extremities. She was evaluated in the emergency department of our Institution in June 2018 for purpuric rash, weakness, and acute kidney injury. Her physical exam revealed the previously described dermatosis (Figure 1(a)) along with a distal sensory and motor polyneuropathy involving all four extremities. Her serum creatinine was 9.7 mg/dL, BUN 168 mg/dL, C-reactive protein 2.8 mg/dL, erythrocyte sedimentation rate 65 mm/H, hypocomplementemia with C3 68 mg/dL, undetectable C4, and cryoglobulins involving 14% of the sample, with negative rheumatoid factor activity. On urine sediment she had dysmorphic hematuria, and proteinuria was quantified at 1.5 g per gram of creatinine. Serologies for HIV, HBV, and HCV were negative, as well as HCV PCR. There was no evidence of hemolysis. ANA was positive at 1:80, with negative anti-dsDNA, anti-SSA, and anti-SSB antibodies.
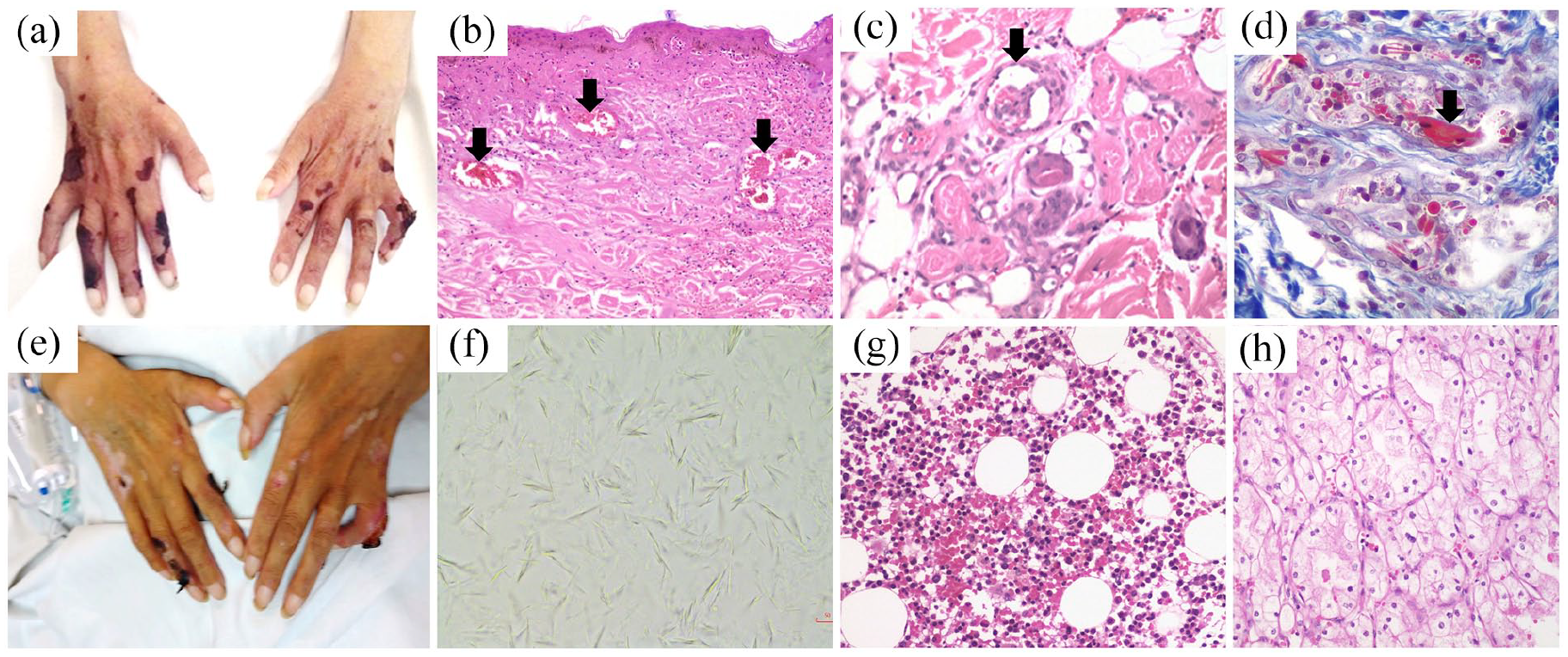
Clinical manifestations and histopathological findings. (a) Confluent necrotic lesions in both hands at admission to our Institution. (b) Skin biopsy from the lesions showing an occlusive vasculopathy with intravascular crystals, with a rectangular shape after magnification (c and d) (hematoxylin and eosin stain (b) and (c), trichrome stain (d)). (e) Skin lesion improvement after treatment with nephrectomy, plasmapheresis, and methylprednisolone pulses. (f) Unstained microscopy of a droplet of the cryoprecipitate shows needle-shaped crystals. (g) Bone marrow biopsy with normal maturation without plasma cell infiltration (hematoxylin and eosin stain). (h) Histopathological analysis of the kidney tumor shows a clear cell renal cell carcinoma (hematoxylin and eosin stain).
The patient was admitted and started on renal replacement therapy. Further testing showed a monoclonal serum spike in the gamma region of 2.2 g/dL, free serum kappa light chain 26.6 mg/L, free serum lambda light chain 248.3 mg/L (kappa/lambda ratio 0.11), and immunofixation revealed a monoclonal IgG lambda. The cryoprecipitate immunofixation also revealed a monoclonal IgG lambda, and spindled crystals were seen when a drop of the cryoprecipitate was mounted on a slide (Figure 1(f)). Skin biopsy revealed an occlusive vasculopathy with intravascular rectangular crystals (Figure 1(b)–(d)). Bone marrow showed a normocellular marrow with 1% plasma cells and no light chain restriction (Figure 1(g)). Kidney ultrasound revealed a hypervascular right kidney tumor of 31 mm × 30 mm × 31 mm. Treatment with methylprednisolone pulses and plasma exchange was started and the patient underwent a surgical nephrectomy.
Kidney histopathology
The histopathological analysis of the right kidney revealed a Fuhrman grade I clear cell renal cell carcinoma (RCC) (Figure 1(h)). The kidney tissue not involved by carcinoma had thrombi in the interlobar vessels, signs of hypo-perfused glomeruli (Figure 2(a)), crystal deposits in the glomerular and interstitial vessels (Figure 2(b) and (c)), along with findings suggestive of active and chronic thrombotic microangiopathy (Figure 2(d)). The tubules had features of acute tubular necrosis (Figure 2(e)). Interstitial fibrosis of 20% was estimated. Fresh tissue immunoglobulin and light chain immunofluorescence were negative for all reactants, however, after proteinase K digestion, immunohistochemistry revealed that the crystalline deposits corresponded to IgG lambda light chains (Figure 2(f)).
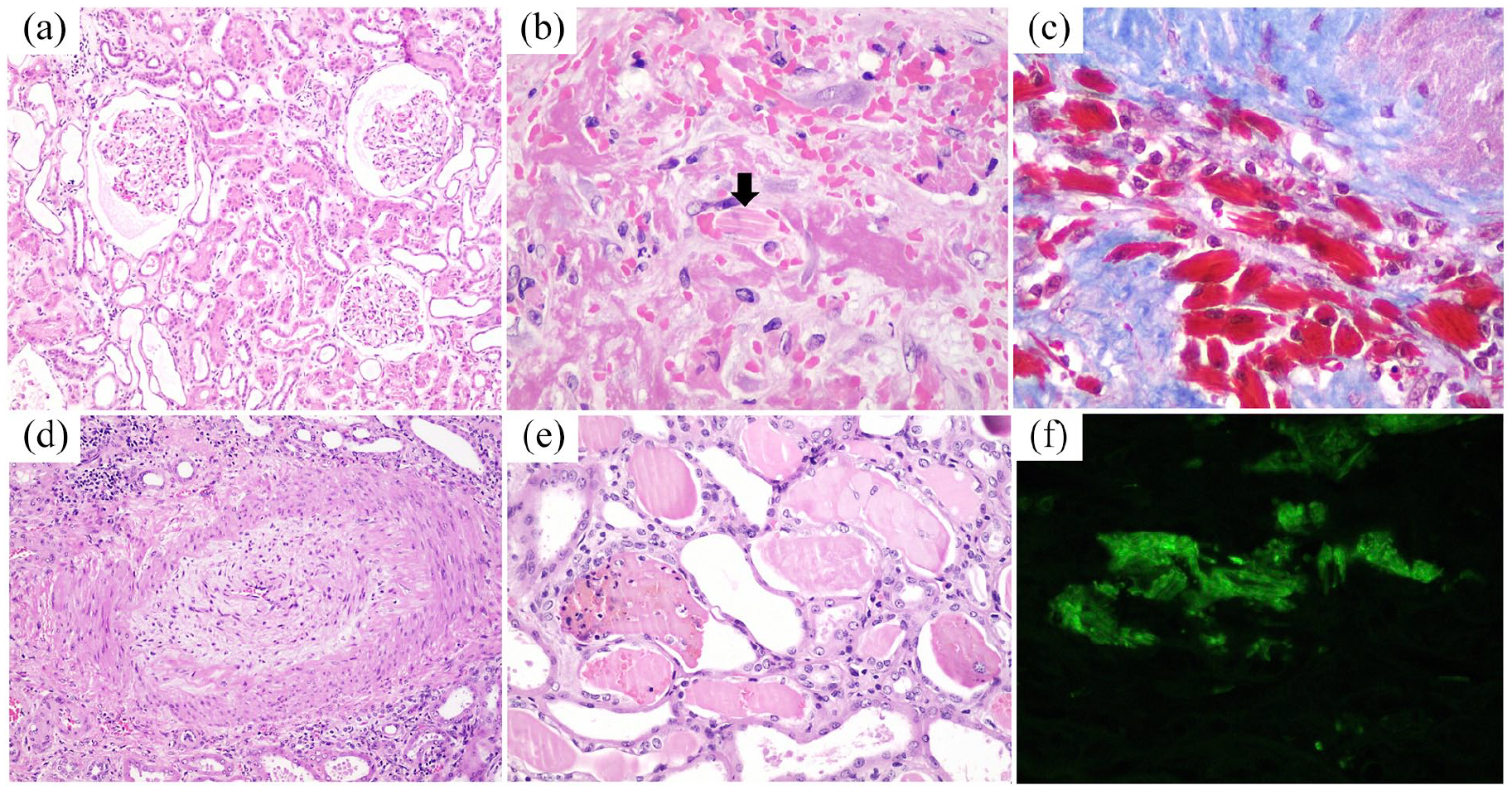
Histopathologic analysis of the kidney biopsy. The kidney biopsy shows hypo-perfused glomeruli (a), with intravascular crystal deposition (arrows in b, c). There were signs of thrombotic microangiopathy in the medium-sized vessels (d) and intratubular crystal deposition (e). Immunofluorescence from the paraffin block after proteinase K digestion shows that crystals correspond to a monoclonal IgG lambda (f). (H&E (a, b, d, e) and trichrome stains (c), immunofluorescence with antibodies against lambda light chain).
The final diagnosis was clear cell RCC, monoclonal gammopathy of renal significance manifesting as crystalcryoglobulinemia, and thrombotic microangiopathy. After the RCC excision and treatment with glucocorticoids and five sessions of plasma exchange, cryoglobulinemia rapidly diminished to 0%, the skin lesions resolved (Figure 1(e)), and the peripheral neuropathy significantly improved. The initial plan was to treat the patient with proteasome inhibitors, however, due to financial reasons, she was managed with cyclophosphamide and glucocorticoids for a total of twelve cycles. By 2 months of treatment, her kidney function improved and renal replacement therapy was suspended. During her last follow up visit in February 2021 she had negative cryoglobulins, an estimated glomerular filtration rate of 22 mL/min/1.73 m2, no monoclonal serum spike, and minimally increased free lambda light chain (46.1 mg/L, reference 5.7–26.3) with a normal kappa/lambda ratio (0.40, reference 0.26–1.65). None of her presenting symptoms have recurred to date.
Discussion
Crystals in crystalcryoglobulinemia are deposited in the extracellular space within the lumen of arteries, arterioles or capillaries with or without secondary vascular thrombosis. This extravascular deposition differentiates crystalcryoglobulinemia from the crystalline variant of cast nephropathy, in which the crystals deposit in distal tubular lumen; and from entities in which the crystals deposit in the intracellular space (e.g. crystal-storing histiocytosis, light chain proximal tubulopathy with crystals). 2
The diagnosis of crystalcryoglobulinemia is established by demonstrating the crystal deposition in the vasculature of the affected organs. The immunofluorescence can be negative for light chains due to changes in the binding site conformation or due to hidden antigen sites because of abnormal folding. Pre-treatment of the sample with protease digestion allows these binding sites to be exposed. To prove the crystallization potential of the cryoglobulins, a droplet of the cryoprecipitate can be placed on a slide and covered with a cover slip before analyzing by simple microscopy for spindled crystals.
The biochemical basis for immunoglobulin crystallization is unknown. Scarce evidence suggests that crystals may form from interactions between the Fc-Fc fractions of the monoclonal immunoglobulins, 6 interactions between the monoclonal protein and proteins such as albumin or fibrinogen,4,7 or due to abnormal glycosylation of the monoclonal immunoglobulin. 8
We performed a systematic review of the literature and found 92 reports of crystalcryoglobulinemia. We excluded 36 reports from our analysis due to incomplete clinical information. In total we included 61 patients from 55 reports (Table 1) (references provided in Supplemental Table 1). Skin, joints, kidneys, peripheral nervous system, and cornea are the most commonly affected organs, but other organ involvement has been described in autopsy series. Acute kidney injury, glomerular hematuria, and non-nephrotic proteinuria were the most common renal manifestations. Complement proteins C3 and C4 were low in 50% and 58% of cases with kidney involvement, respectively. Crystallization of cryoglobulins was mostly reported in association with multiple myeloma. However, 15%–20% of cases occurred in the setting of a monoclonal gammopathy of undetermined significance. The majority of cases corresponded to type I (or monoclonal) cryoglobulins, most commonly IgG kappa (Table 1), but a third of patients had IgG lambda.
Systematic review of 61 patients with cryocrystalglobulinemia described in 55 published reports*.
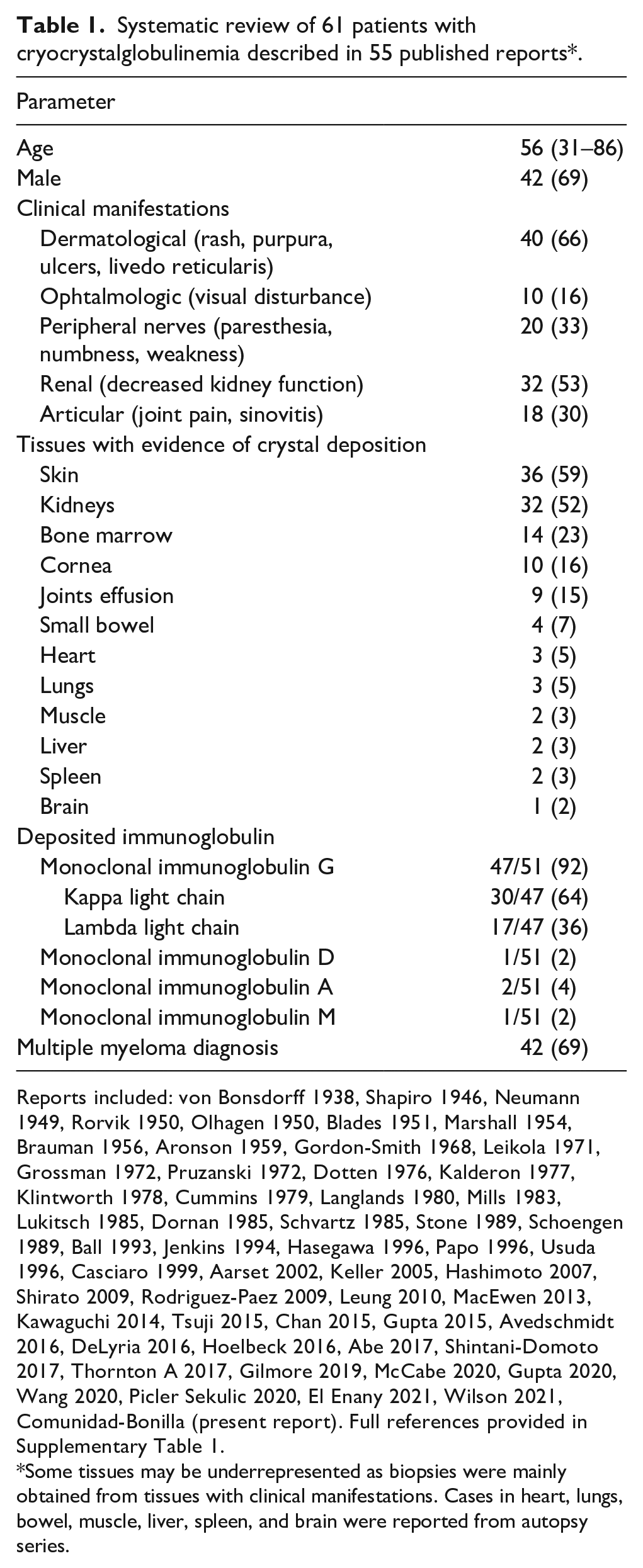
Reports included: von Bonsdorff 1938, Shapiro 1946, Neumann 1949, Rorvik 1950, Olhagen 1950, Blades 1951, Marshall 1954, Brauman 1956, Aronson 1959, Gordon-Smith 1968, Leikola 1971, Grossman 1972, Pruzanski 1972, Dotten 1976, Kalderon 1977, Klintworth 1978, Cummins 1979, Langlands 1980, Mills 1983, Lukitsch 1985, Dornan 1985, Schvartz 1985, Stone 1989, Schoengen 1989, Ball 1993, Jenkins 1994, Hasegawa 1996, Papo 1996, Usuda 1996, Casciaro 1999, Aarset 2002, Keller 2005, Hashimoto 2007, Shirato 2009, Rodriguez-Paez 2009, Leung 2010, MacEwen 2013, Kawaguchi 2014, Tsuji 2015, Chan 2015, Gupta 2015, Avedschmidt 2016, DeLyria 2016, Hoelbeck 2016, Abe 2017, Shintani-Domoto 2017, Thornton A 2017, Gilmore 2019, McCabe 2020, Gupta 2020, Wang 2020, Picler Sekulic 2020, El Enany 2021, Wilson 2021, Comunidad-Bonilla (present report). Full references provided in Supplementary Table 1.
Some tissues may be underrepresented as biopsies were mainly obtained from tissues with clinical manifestations. Cases in heart, lungs, bowel, muscle, liver, spleen, and brain were reported from autopsy series.
Treatment of crystalcryoglobulinemia involves rapid initiation of glucocorticoids to decrease the inflammation, and plasma exchange to remove the monoclonal cryoglobulins. 2 In the systematic review we found these two interventions commonly used in most patients, followed by plasma cell-directed therapies appropriate to the period of the report. These therapies include melphalan, cyclophosphamide, thalidomide, and most recently lenalidomide and proteasome inhibitors, alone or in combinations. Caution is advised when using lenalidomide and thalidomide due to their pro-thrombotic effects. Response rates are difficult to estimate for crystalcryoglobulinemia due to the selective and heterogeneous reporting of these data in the literature. If extrapolated from type I cryoglobulinemia, the response rate to treatment is approximately 70%, but 40% to 50% of patients relapse at a median of 12 months of follow-up. 9 Adverse prognostic factors for survival include age, the severity of organ damage (especially kidney injury), and infections occurring during treatment. 9
The association between RCC and MM was reported in a large epidemiologic study. 5 This study found 88 MM cases that occurred in 57,190 patients with RCC, and 69 RCC cases that occurred in 34,156 patients with MM. It was estimated that the risk of MM in subjects with RCC is 51% higher than in the general population (standardized incidence ratio [SIR] = 1.51, 95%CI 1.21–1.85), with the highest risk observed within the first year after RCC diagnosis (SIR = 3.82, 95%CI 2.59–5.42). Conversely, the risk of RCC in MM subjects is 89% higher than in the general population (SIR = 1.89, 95%CI 1.47–2.40), and is also higher within the first year after MM diagnosis (SIR = 4.14, 95%CI 2.93–5.69).
We reviewed 40 cases of MM and RCC reported to date (references provided in Supplemental Table 2). Among them, 16 (40%) had a synchronous presentation of both neoplasms, in 14 (35%) cases the RCC preceded the MM diagnosis, and the opposite was true for 10 (25%) cases. Three cases with a synchronous presentation evidenced the presence of monoclonal plasma cells infiltrating the RCC or the surrounding tissue,10–12 and one case report described the finding of a para-aortic plasmacytoma adjacent to the RCC. 12
Plasma cell and RCC growth depend on cytokines, including interleukin-6 (IL-6). Serum IL-6 levels were reported elevated in a few cases with synchronous MM and RCC.13–15 Furthermore, immunohistochemistry for IL-6 was positive within the RCC. 16 Interestingly, in one case serum IL-6 decreased after the RCC excision. 13 Some RCCs have mutations in c-Met, a tyrosine kinase that binds the hepatocyte growth factor (HGF). It has been reported that HGF potentiates the IL-6-induced growth of myeloma cells. 17
Our case corresponds to a monoclonal gammopathy with renal significance with a synchronous presentation with a RCC. It is possible that in this case, cytokine production by the RCC may have stimulated a plasma cell clone to proliferate and produce monoclonal immunoglobulins that crystalized in several organs. The rapid RCC excision may have aided in achieving a quick response to therapy.
In summary, to our knowledge, this is the first case reported in the literature of concomitant RCC and crystalcryoglobulinemia as a manifestation of MGRS. We successfully achieved remission by treating our patient with removal of the RCC, plasma exchange, steroids, and cyclophosphamide. After 32 months of follow-up, the patient remains in remission with no evidence of monoclonal gammopathy or active disease. She was able to come off renal replacement therapy, but remains with stage IV chronic kidney disease.
Supplemental Material
sj-docx-1-jnp-10.1177_23993693211027876 – Supplemental material for Crystalcryoglobulinemia as a manifestation of monoclonal gammopathy of renal significance in a patient with renal cell carcinoma
Supplemental material, sj-docx-1-jnp-10.1177_23993693211027876 for Crystalcryoglobulinemia as a manifestation of monoclonal gammopathy of renal significance in a patient with renal cell carcinoma by Roque A Comunidad-Bonilla, Megan A Navarro-Gerrard, Norma Uribe-Uribe, Silvia E Ramírez-Andrade, Abraham Cohen-Bucay and Juan M Mejia-Vilet in Journal of Onco-Nephrology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.