
Abstract
Background:
Peptide receptor radionuclide therapy with 177Lu-dotatate is a novel therapy for metastatic neuroendocrine cancers. It undergoes reabsorption at the proximal tubule; after the breakdown of the peptide fragment, 177Lu is retained and continues its decay process exposing the nephron to continuous low dose radiation. Pivotal NETTER-1 trial did not include patients with eGFR <50 and so its effects in CKD patients is not known.
Methods:
We performed a retrospective chart review of all consecutive adult patients that received 177Lu-dotatate over 1 year at Mayo Clinic, Rochester. We analyzed renal and hematological laboratory data obtained prior to each of four treatment cycles and at 3- and 6-month post completion of all treatment. We defined CKD as eGFR <60 ml/min and AKI as creatinine increase of ⩾0.3 from baseline by AKIN criteria.
Results:
Overall 86 patients were included in the study with 39 (45%) with known CKD. About three patients had CKD, four with eGFR of 20–30 ml/min. About 4 (4.6%) patients had AKI and the predominant cause being hypotension. Among the CKD patients the average eGFR improved after the first cycle of PRRT therapy from baseline of 49 (13) to 53.5 (17) ml/min (p = 0.01) with no significant decline of renal function noted at 3- and 6-months post treatment follow up. Rate of thrombocytopenia and leukopenia were significantly more in the CKD patients starting even after single treatment. No drug dose correlation was noted.
Conclusion:
Patients with CKD are at a higher risk of hematological toxicity especially with thrombocytopenia and require close monitoring and ongoing dose adjustment. Ongoing safety studies to assess the long-term impact of 177Lu-dotatate on the kidney are needed.
Introduction
Peptide receptor radionuclide therapy (PRRT) was introduced in the mid-1900s for patients with inoperable or metastatic neuroendocrine tumors (NET). These are therapeutic radionuclides-tagged with octreotide analog protein for targeted therapy in these complex patients. The initial radionuclide yttrium-90 (90Y) had a high toxicity profile including development of end stage renal disease. 1 Since then many other radionuclides were studied and most recently Lutetium radionuclide—177Lu dotatate (Lutathera®) has been approved by Food and Drug administration (FDA) for metastatic neuroendocrine tumor. With the success of 177Lu dotatate, other radiolabeled peptides like 177Lu labeled prostate specific membrane antigen (PSMA) for metastatic prostate cancer are now being investigated.
This exciting growth in the field of Nuclear Theranostics unfortunately brings the radiation dose-limiting organs, the kidneys, back in the firing range as these drugs are still excreted via the urine. The Onco-nephrology community must pause and consider the risk of radiation nephropathy in these patients receiving targeted radionuclide therapy. In addition, the pivotal NETTER-1 trial excluded patients with chronic kidney disease (defined as serum creatinine >1.7 mg/dl or creatinine clearance <50 ml/min). 2 Hematological toxicity in CKD patients was a major concern. Four patients of 112 (4.4%) had an acute kidney injury (AKI) reported on their trial with none having CTCAE Grade 3 or 4 AKI. 2
The objective of this study was to (1) determine the incidence of acute kidney injury in the patients receiving this therapy at our institution and (2) determine the incidence of hematological toxicities in CKD patients.
Methods
Study design
This is a single center retrospective cohort study. We identified all consecutive adult patients that received peptide receptor radionuclide therapy with 177Lu dotatate at the Mayo Clinic Rochester from April 1, 2018 to April 30, 2019. Patients that did not provide research authorizations were excluded from this study. This retrospective review of patient records was approved by the Mayo Clinic Institutional Review Board. All patients receive a standard 4 h infusion of lysine + arginine (2.5%) prepared by our pharmacy during each of their 177Lu dotatate treatments. The amino acid infusion is started 1 h prior to the 177Lu dotatate infusion and continued for 3 h after the drug is infused.
Data collection
We collected study data by reviewing the electronic medical records of all included patients. Demographic variables included date of birth, gender, race, body mass index (BMI), baseline ECOG (eastern cooperative oncology group) score for performance status and specific comorbidities (including prior chronic kidney disease, diabetes mellitus, and hypertension). We also collected disease specific data including date of diagnosis of the underlying disease, underlying disease being treated with drug, primary site of cancer, baseline proliferation index Ki67, ENETS/WHO 2010 (European Neuroendocrine Tumor Society) grade available at the time of therapy, sites of metastasis known at the time of therapy, and prior therapies (including surgery, embolization procedures, chemotherapy, everolimus, and somatostatin) received.
We collected study data of hematological (hemoglobin, leukocyte count, and platelet count) and renal (serum creatinine, eGFR, and blood pressure) parameters at baseline and prior to every cycle. We also collected information on dose of 177Lu dotatate given and reasons for delay in therapy. We collected outcome variables including episodes of acute kidney injury, date of death, and date of last follow up.
Definitions
We defined acute kidney injury based on KDIGO criteria 3 as an increase in creatinine ⩾0.3 mg/dl within 48 h or ⩾50% within 7 days. We used the Common Terminology Criteria for Adverse Events (CTCAE) grading system to define the grade of injury, anemia, leukopenia, and thrombocytopenia. This is provided in Supplemental Table S1. We calculated eGFR based on the CKD-EPI equation. We defined CKD as per KDIGO guidelines as the presence of kidney damage or decreased kidney function for at least 3 months. In those patients that did not have past measurements available for review a chart review was done by the nephrologist (SM) for clinical decision on whether a patient could be deemed to have CKD based on history, imaging, and laboratories. All patients with eGFR <60 ml/min, or eGFR >60 ml/min with proteinuria was categorized to the CKD group.
We defined Standard dose of 177Lu-dotatate as dose of 190–210 mCi and all patients that received 90–110 mCi per dose were considered to have received the Adjusted Low dose. If patients received a cumulative dose of at least 580 mCi or if they had received at least two standard doses during their treatment, then they were categorized to have been overall in the Standard Drug Dose group. Patients were classified as having complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD) based on the imaging at the 3 and 6 months follow ups.
Statistical analysis
Summary statistics are presented as mean (SD) for continuous variables with normal distribution, median (IQR) for continuous variables with skewed distribution, and as n (%) for categorical variables. Comparisons between the two groups were made with t-test for continuous variables with normal distribution, the non-parametric Wilcoxon rank sum test for continuous variables with skewed distributions, the Chi-square test for categorical variables where the expected cell counts were greater than 5, and the Fisher’s exact test for categorical variables where the expected cell counts were less than 5.
Results
Patient population and characteristics
We had a total of 91 consecutive patients that started PRRT therapy with 177 Lu-dotatate between April 2018 and April 2019. Of these five patients were excluded as they did not provide any research authorization. The remaining 86 patients were included in our study. About 39 of the 86 (45%) patients had clinically defined CKD and the remaining 47 patients were deemed to have no CKD (Figure 1). CKD Stage 2, 3, and 4 were seen in 9, 27, and 3 patients respectively.
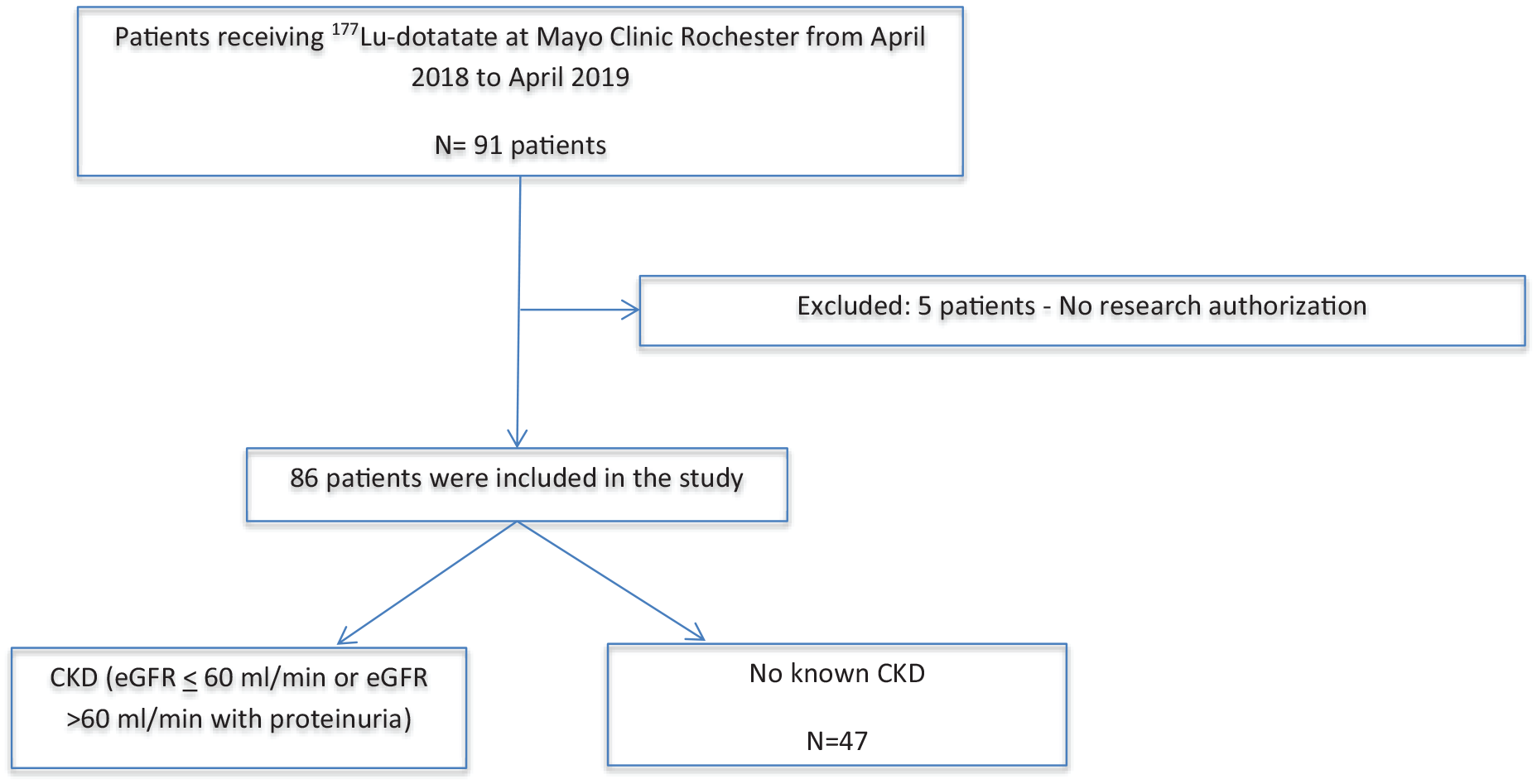
Flow chart of patient inclusion into the study.
They were overall an average age of 63 years (SD 10.3) with predominant male (56%) gender and white race (93%). These were patients with overall favorable baseline ECOG performance status with ECOG 0, 1, 2, and 3 in 31 (36.5%), 45 (53.57%), 6 (7.1%), and 2 (0.2%) respectively. The most treated underlying disease was neuroendocrine tumor (NET) with 83 (96.5%) patients. There were two patients with meningioma and one with a paraganglioma as well. In those with NET, the predominant site of tumor was the bowel with 46 (54.7%) patients; the pancreas being the second most common 28 (33.3%) followed by site unknown, bronchial, thymus, and brain in 8 (9.2%), 2 (2.3%),1 (0.1%), and 1 (0.1%) respectively. About 98.8% of the patients had been on a somatostatin analog prior to therapy. Patients had received various prior therapies including surgical resections, embolization procedures, everolimus, and systemic chemotherapy that included many nephrotoxic regimens like carboplatin, cisplatin, bevacizumab, and immune checkpoint inhibitors (Table 1).
Baseline characteristics of patients receiving 177Lu-dotatate therapy between April 2018 and April 2019.
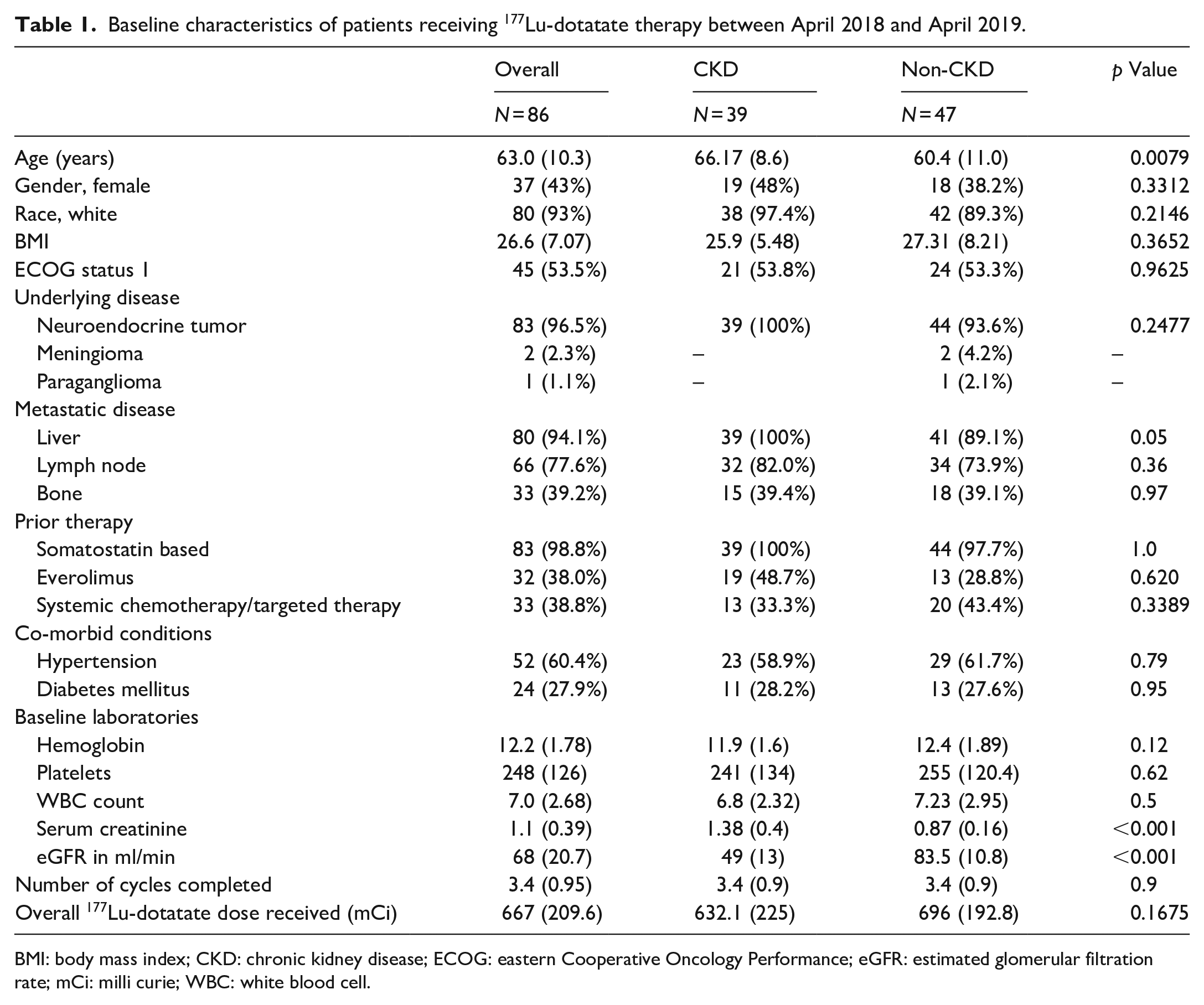
BMI: body mass index; CKD: chronic kidney disease; ECOG: eastern Cooperative Oncology Performance; eGFR: estimated glomerular filtration rate; mCi: milli curie; WBC: white blood cell.
Clinical characteristics of CKD and non-CKD patient groups
Patients that had CKD were significantly older compared to the non-CKD group with 66.17 (8.6) years versus 60.4 (11) years respectively. The average serum creatinine of the CKD group was 1.38 (0.4) mg/dl with eGFR of 49 ml/min as compared to the non-CKD group that had an average of 0.87 (0.16) mg/dl and 83.5 (10.8) ml/min (Figure 2). The rest of baseline hematological laboratories including hemoglobin, platelets, and WBC count were comparable between the two groups. There was no significant difference in prior use of systemic chemotherapy or targeted therapy these patients received in either of the groups especially for nephrotoxic drugs. About 59 of the 86 patients (68%) completed all four cycles. Only six patients (6.9%) had to stop after the first cycle. Overall, there was no difference in the cumulative dose of 177Lu-dotatate received between the two groups (632.1 mCi vs 696 mCi, p = 0.1675; Table 1).
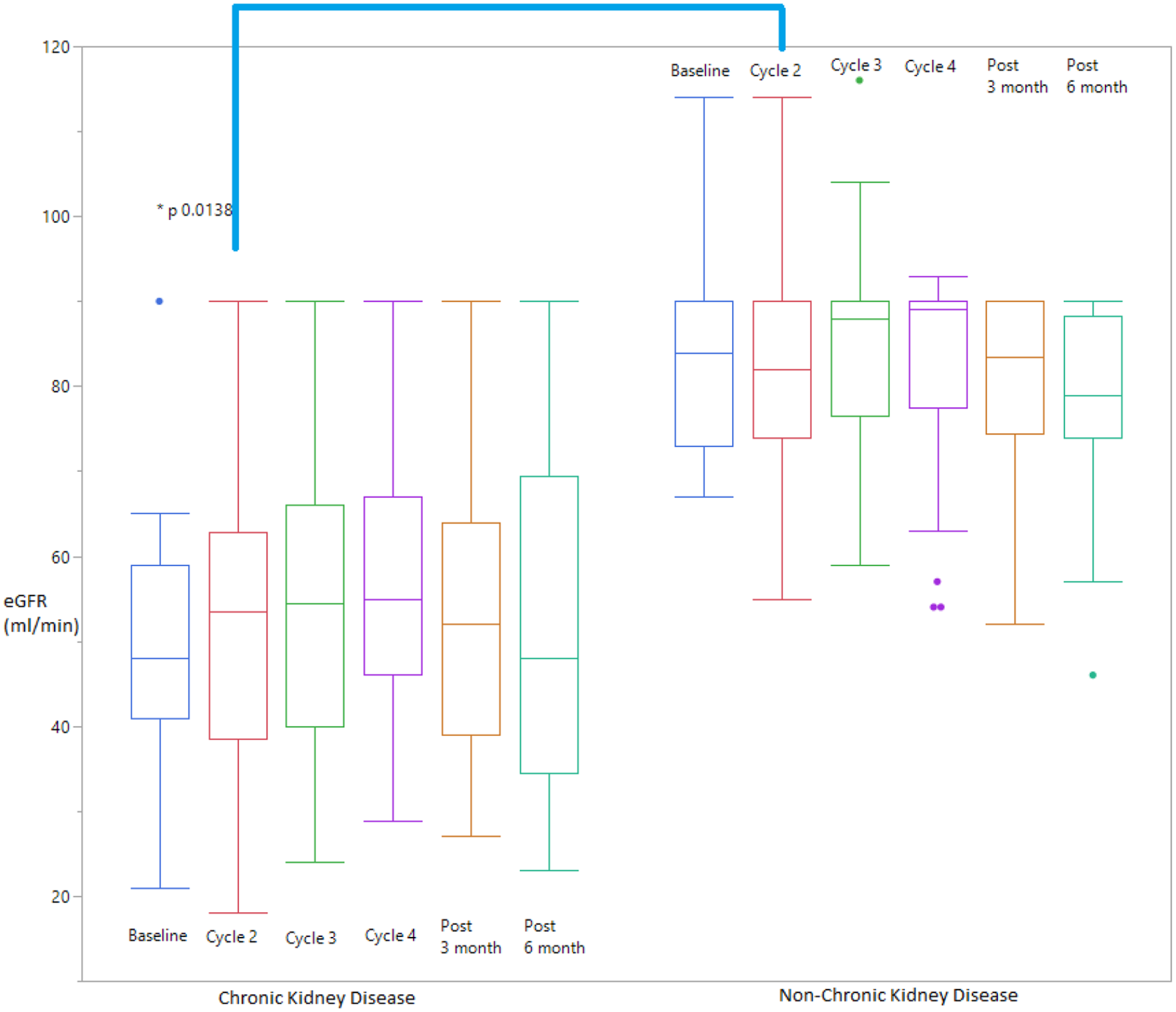
Trend of eGFR at baseline, prior to Cycle 2, 3, and 4 and post PRRT therapy at 3 and 6 month follow up as noted in the patients with Chronic Kidney Disease (CKD) and non-CKD group.
We reviewed the change in renal parameters (serum creatinine, eGFR) and hematological parameters (hemoglobin, platelet count, and WBC count) between the pre-defined CKD and non-CKD groups as compared to baseline. Interestingly, Among the CKD patients the average creatinine and eGFR improved after the first cycle of PRRT therapy from baseline of 1.38 (0.4) and 49 (13) to 1.3 (0.4) mg/dl and 53.5 (17) ml/min (p-value of 0.02 and 0.01 respectively). This is though statistically significant its clinical relevance is questionable. But there was no further creatinine improvement or worsening noted in the future cycles (Supplemental Table S2). These renal parameters were not statistically different from baseline at the end of 6 month follow up as noted in Table 2.
Mean (SD) pretreatment values for renal and hematological laboratories and blood pressure while on 177Lu-dotatate and at 3 and 6 month follow up.
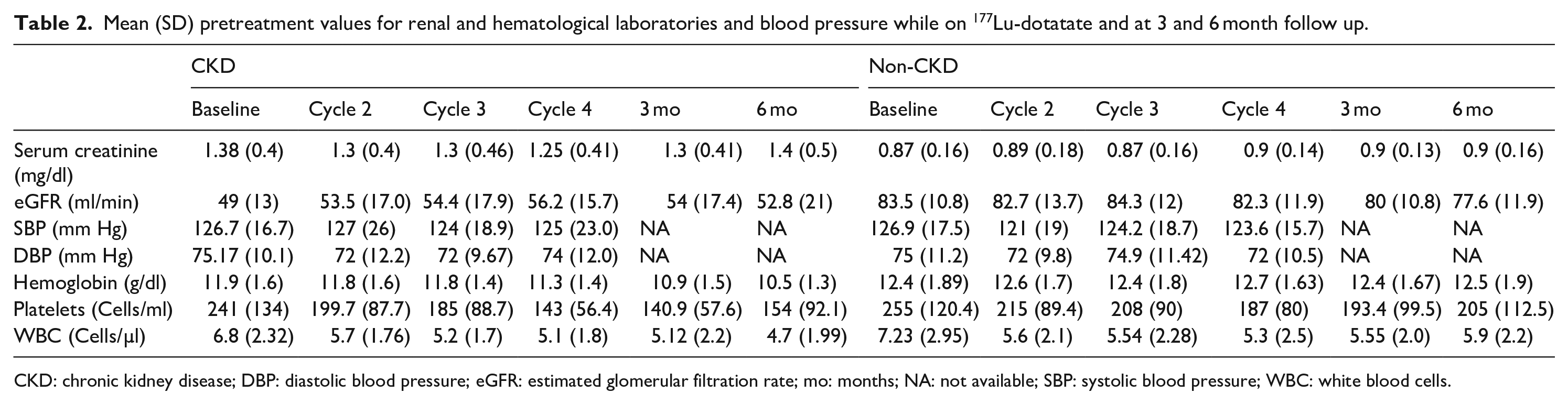
CKD: chronic kidney disease; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; mo: months; NA: not available; SBP: systolic blood pressure; WBC: white blood cells.
Incidence of acute kidney injury and their clinical characteristics
Overall, we had 4 of 86 (4.6%) patients that met criteria for our definition of AKI. All four events were mild and classified as AKIN Stage 1. None required dialysis. The predominant cause of AKI was hypotension based on documentation by the treating physician or by manual chart review by author (SM; Table 3).
Patients with acute kidney injury events while on therapy with 177Lu-dotatate.
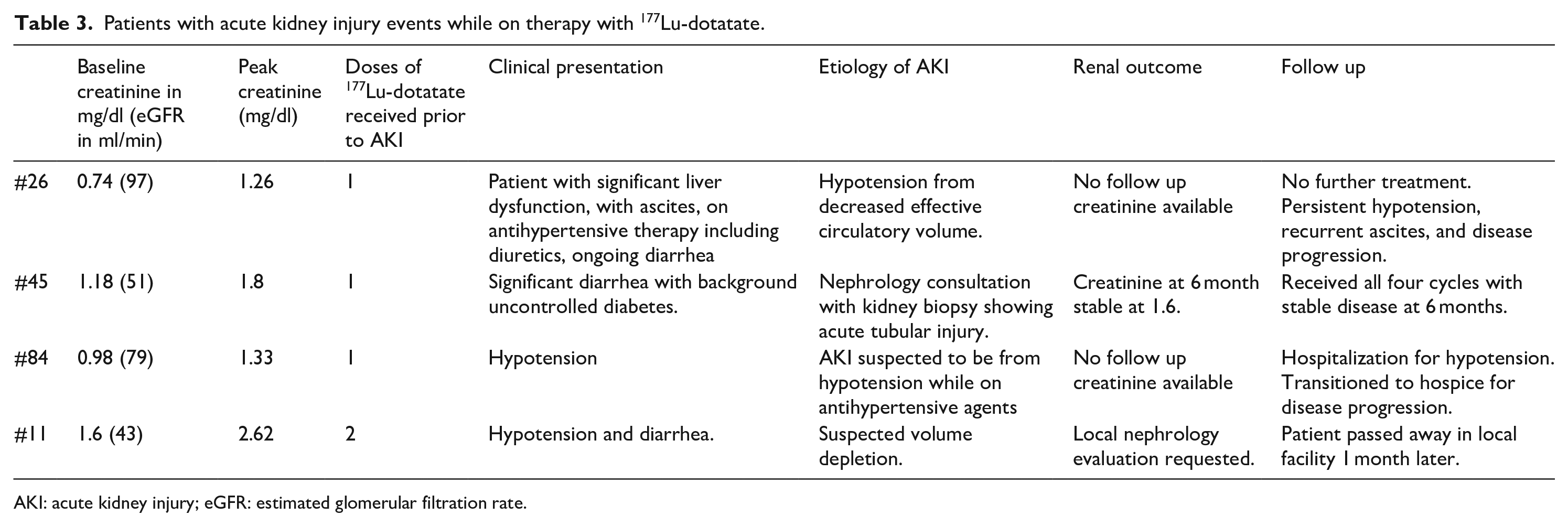
AKI: acute kidney injury; eGFR: estimated glomerular filtration rate.
Two (#26 and #84) of the four patients had normal renal function at baseline with serum creatinine (eGFR) of 0.74 mg/dl (97 ml/min) and 0.98 mg/dl (79 ml/min) respectively. The AKI was in the setting of hypotension while on antihypertensive agents. #26 unfortunately had significant liver dysfunction with clinical deterioration requiring TIPS procedure and did not receive any further treatment with PRRT. #84 had progressive disease requiring multiple hospitalizations locally and eventually transitioned to hospice 3 months later.
Two of the patients had baseline CKD Stage 3. #45 had a longstanding history of diabetes with possible diabetic nephropathy. The creatinine peaked at 1.86 mg/dl from a baseline of 1.1 mg/dl. Despite correction for volume depletion and withholding of the 177Lu-dotatate the serum creatinine had continued to rise and a kidney biopsy was performed. This showed evidence of mild background diabetes mellitus with diffuse acute tubular injury which was of unclear etiology. No evidence of thrombotic microangiopathy or glomerular injury. There was no evidence of enteric hyperoxaluria by labs or of oxalate crystals on the kidney biopsy. Patient eventually received all four cycles with a stable disease on imaging at 6 months and creatinine remained stable at 1.6 mg/dl as well. Unfortunately, the patient passed away from complications after small bowel obstruction a few months later. The #11 also had CKD Stage 3 in the setting of recurrent acute kidney injury. Creatinine increased from a baseline of 1.6–2.62 mg/dl when presented for cycle 3 and was volume depleted on exam from increasing diarrhea. Patient received intravenous fluids and was recommended local nephrology evaluation. The details of which was not available for us to review. This patient passed away a month later at a local hospital.
Hematological outcomes between CKD and non-CKD patients
There was evidence of hematological toxicity with thrombocytopenia, leukopenia, and anemia noted in both groups. Overall laboratory abnormality of thrombocytopenia and leukopenia was noted early, and for many even after a single dose of the 177 Lu-dotatate and this persisted even at the 6 months follow up. Anemia was late to develop starting to show significant difference from baseline at the 3 months follow up check. The trend of the mean values prior to each cycle and at post 3 and 6 months follow up are presented in Table 2.
When the two groups of CKD and non-CKD were compared for the same hematological parameters as a change from baseline values, we noted a skewed distribution. There was an overall trend of larger drop in platelets from baseline in the ckd group at all stages but reached statistical significance in labs prior to cycle 4. The median drop in platelets from baseline and prior to cycle 4 was [−78 (−45 to −130) cells/ml vs −37 (−10.25 to −96.75) cells/ml, p = 0.0371] (Figure 3).
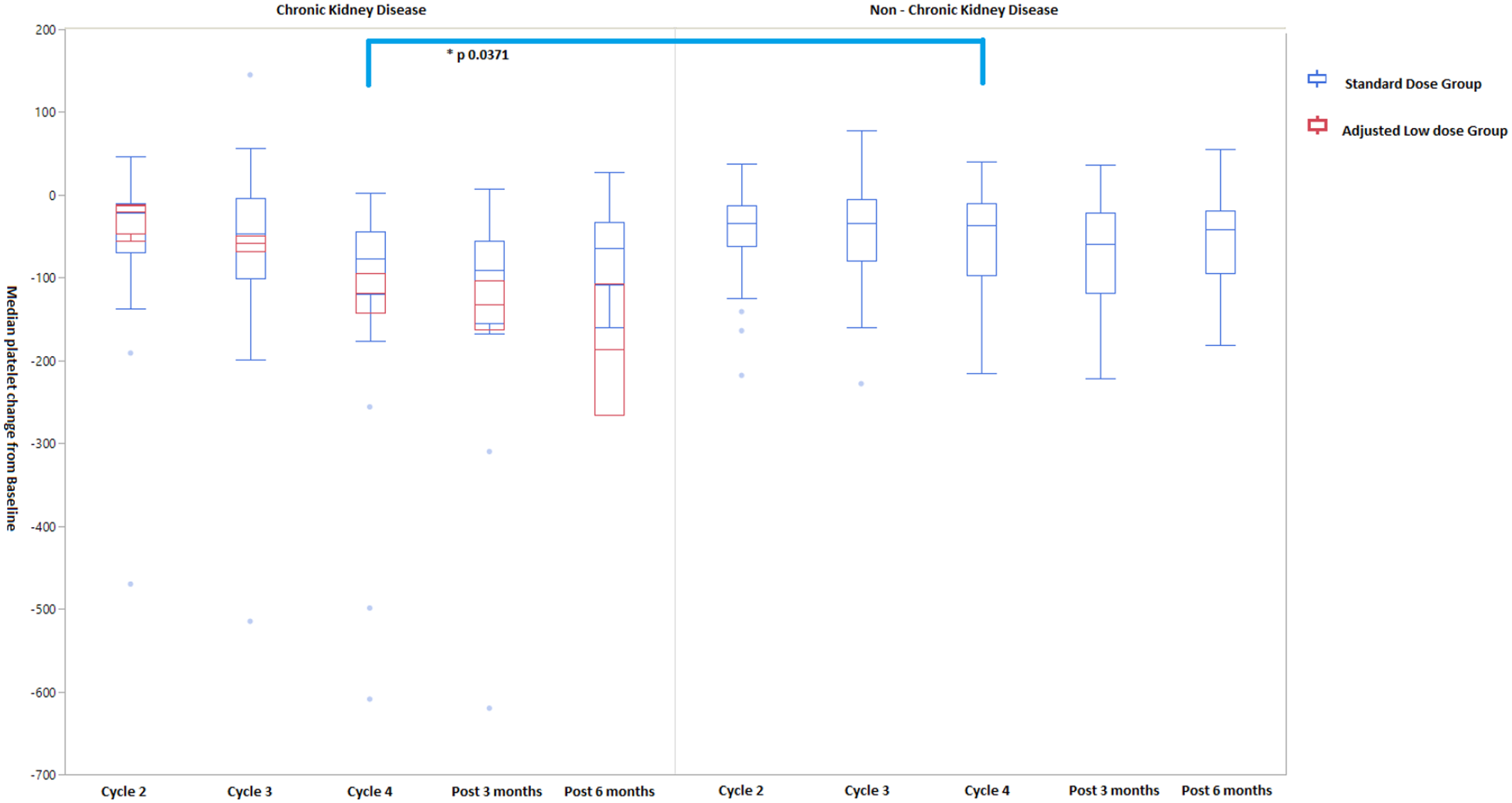
Change in median (IQR) platelets from baseline after receiving 177Lu-dotatate prior to Cycle 2, 3, 4, and 3- and 6-months post treatment among patients with and without chronic kidney disease. Overlay added of overall 177Lu-dotatate dose received into standard versus adjusted low dose within the CKD cohort.
We further analyzed the CKD group cohort of patients and within this compared them based on the cumulative dose received into adjusted low dose and standard dose to assess the change in platelets (Figure 3). These CKD patients who received our definition of standard dose still fared with better platelets than those that received an adjusted low dose regimen (Figure 3).
There was no significant difference in the leukopenia between the two groups. There was a greater drop in hemoglobin among the CKD group patients which reached statistical significance at the 6-month mark [−1.7 (−0.85 to −2.55) in CKD vs −0.4 (0.525 to −1.1), p = 0.0071] (Supplemental Table S3).
Disease and patient outcomes
With regards to cancer outcome at 3 months follow up, the patients with complete response, partial response, stable disease and progressive disease were 1(1.1%), 20 (22%), 19 (22%), and 10 (11.6%) respectively. No records were available for 36 (41%) of the patients. At the 6 months follow up, patients with partial response, stable disease, and progressive disease were 6 (6.9%), 22 (25.5%) 4 (4.6%) respectively. No patient had complete response and we had unavailable records for 54 (62%) of the patients. No statistically significant difference was noted when the disease outcome of PR, PD, and SD were compared between the CKD and non-CKD cohorts.
At the time of last follow up overall 18 (20%) of the 86 patients were dead with 7 (17.9%) from the CKD cohort and 11 (23.4%) of the non-CKD cohort of patients and this was not statistically significant.
PRRT therapy in advanced CKD
There were three patients (#6, #67, and #96) that had CKD 4 at the time of starting PRRT therapy with eGFR of 25, 29, and 21 ml/min (Supplemental Table S3). The #96 patient had received the treatment at low doses on compassionate basis due to lack of other treatment options but after two cycles had to be stopped due to significant thrombocytopenia. Follow up imaging had shown stable renal function but had progressive disease and died while on hospice. #6 had an excellent outcome with SD at 6 months and cumulatively received 403.8 mCi. The lowest platelet count was 111 cells/ml at the end of 6 months. A total of #67 received three cycles with a cumulative dose of 516.8 mCi by the end of three cycles with lowest platelet count of 62 cells/ml. No change in renal function was noted during this time but the patient did not receive any further PRRT therapy due to persistent thrombocytopenia. Unfortunately, no follow up renal parameters are available for review.
Discussion
In our study, we performed a retrospective review of 86 consecutive patients that received PRRT therapy with 177Lu-dotatate over a span of 1 year, and we found that 4 of 86 (4.6%) patients had an episode of mild AKI with the predominant cause of AKI being hypotension. This is consistent with the NETTER-1trial data. About 45% of our patients had known CKD with three patients having advanced CKD Stage 4. Interestingly, we found that among the CKD patients the average creatinine and eGFR improved after the first cycle of PRRT therapy from baseline of 1.38 (0.4) and 49 (13) to 1.3 (0.4) mg/dl and 53.5 (17) ml/min (p-value of 0.02, 0.01 respectively). At the end of 6 month follow up, there was no worsening of renal function noted. With regards to hematological toxicity, there was more profound thrombocytopenia in the CKD group which reached statistically significance prior to cycle 4 but we were unable to demonstrate any obvious correlation with the cumulative drug dose received by these patients.
The lessons we have learnt from external beam radiation therapy (EBRT) are important here to understand the safety concerns with PRRT and the kidney. Kunkler et al. 4 were the first to describe a series of radiation related kidney disease and hypertension and in their seminal paper their AKI rate was high at 20%. Fortunately, it is a rare occurrence in clinical practice. Mechanistically radiation related kidney damage was “simple” in EBRT, for if the kidneys are in the way then they are exposed to the damage but in PRRT the mechanism of damage would be much more complicated. In EBRT, this acute radiation nephropathy (previously erroneously termed acute radiation nephritis) was possibly from oxidative stress, activated renin angiotensin system (RAS), hypoxia, vascular endothelial damage, and inflammation. In PRRT, radiation related damage is different in that we would need to account for the nature of the radioactive substance, its mode of decay, the peptide fragment, characteristics of the linker molecule, size of the protein, hydration status of the patient, urine flow rate, concurrent nephrotoxic medications and prior renal disease. In PRRT, the additional concern in CKD patients is that the delay in clearance may cause a more profound bone marrow suppression. Clinically, our experience has been that patients with CKD or those with prior chemotherapy exposure have a more profound thrombocytopenia with resulting delay in their next treatment as we wait for marrow recovery between doses. 5 This was apparent in the platelet trend but did not reach statistical significance until their pre-cycle 4 labs. We also did not see any statistical correlation with prior chemotherapy use or cumulative dose received which was unexpected. It is likely our patient population was not large enough to find such a change and we still recommend cautious use in CKD patients with close monitoring of their platelets. Dosimetry studies in these select patients will be important to individualize the treatment regimen. 5
Cybulla et al. 1 in their paper described a patient who had received PRRT therapy with 90Y-DOTATOC and developed kidney function deterioration 15 months after the treatment had been stopped. Eventually this patient required dialysis. Bodei et al. 6 in their long term follow up study showed that the patients receiving 90Y-DOTATOC developed a slow decline in renal function. In a span of 8 years there was about 25% decline in kidney function especially in the high-risk patients who had diabetes, hypertension, history of prior chemotherapy, and embolization procedures. 6 They had shorter follow up data, of up to 2 years, for patients who had received 177Lu-dotatate and showed a trend to decline in renal function. 6 Our study is the largest cohort of patients, that we are aware of, have received 177Lu-dotatate specifically looking at the renal profile.
A healthy glomerular filtration barrier will not permit any molecule larger than about 5000 Da to pass through. 7 177 Lu-dotatate is 1609.6 Da and hence freely permeable. It has a protein fragment that binds to somatostatin 2 (sst2) receptor. In the kidney, sst2 is expressed in the glomeruli, proximal tubular cells, loop of Henle, and distal tubule.8–13 Interestingly, animal model studies have shown us that the renal retention of the radiolabeled peptides is independent of the somatostatin receptors. 14 A factor to consider for renal damage is the type of decay radiation and its penetration depth. One of the first radiolabeled somatostatin analog used was 111In-DTPA-octreotide and it showed rapid clearance from the blood with accumulation in tumor, pancreas, liver, and kidney and at 1 and 20 h mark; the kidneys had the highest biodistribution of percent dose/organ. 14 The majority of this was in the cortical areas and on subcellular fractionation was localized to the lysosomes. 14 But a study of 21 patients that received this did not report any kidney toxicity even after 3 year follow up 15 despite receiving up to 45 Gy to the kidneys. It is possible this is related to the decay pattern of the radionuclide as 111In emits gamma radiation and auger electrons with a very small penetration depth of 0.02–10 µm. 90Y-DOTATOC, a beta particle emitting drug, has significant kidney toxicity; including one case report of a patient needing dialysis, has a much higher penetration depth of about 12 mm which may explain the higher toxicity to the kidneys.1,16 177Lu-dotatae is a beta particle emitter but has a low penetration depth like 111In making this a more favorable radionuclide to use to prevent kidney toxicity.
Kidney biopsy in EBRT related AKI typically showed involvement of all compartments—glomerular, tubular, and the vascular beds. There was prominent capillary loop thickening, basement membrane duplication, mesangiolysis, interstitial fibrosis, and tubular atrophy in most patients while in severe cases there was also evidence of thrombotic microangiopathy. 17 Serial animal model studies by Cohen and Robbins 17 indicate that the insult is initially glomerular in a dose dependent manner, with eventual involvement of the tubular and interstitial compartment. Kidney biopsies in patients receiving 90Y have reported glomerular damage with thrombotic microangiopathy.18–21 One of our patients did undergo a kidney biopsy but the predominant finding was of acute tubular injury with no vascular lesions and is possibly reflective of its nature as a tubular toxin.
To reduce the endocytosis of the radiolabeled peptides, it is recommended to keep the urine flow rate high by having patients stay well hydrated, empty their bladder often and the use of positively charged basic amino acids. In a seminal paper Mogensen and Sølling 22 had shown that by use of positively charged basic amino acids one could reduce the absorption of proteins in the proximal tubule. Hammond et al. 23 studied 111In-DTPA-octreotide with an amino acid infusion and found there was a increase in urine clearance of isotope suggestive of a decreased renal reuptake. Commercially available amino acid mixtures have a high osmotic load and cause significant nausea and vomiting. A combination of arginine and lysine appeared to be the most tolerated and effective in the inhibition of renal uptake of the radiolabeled octreotide. 24 All of our patients in this cohort received a 4 h infusion of this lysine + arginine (2.5%) amino acid mixture, prepared specifically at our pharmacy, during each of their 177Lu-doatate infusions. Future studies will be needed to consider possibly up-titration of amino acids in high risk patients. Also possibly the role of captopril based on the work by Cohen et al. 25 in EBRT.
The appropriate dosing of 177Lu-dotatae patients in advanced CKD is an ongoing challenge. Unfortunately, clinical trials do not provide us guidance. In the patients that we have cared for the doses have been overall individualized to patients based on the their stage of CKD, prior chemotherapy, possibilities of reversibility of their renal function especially in patients that had undiagnosed enteric hyperoxaluria or dehydration; and their future treatment options. A multidisciplinary approach is a must in caring for these complex patients.
Being a retrospective cross-sectional review, our study has many limitations. Firstly, we had a small sample size and handful patients with advanced CKD stage 4 and above. Secondly, being a referral center, we were also limited by the short follow up of just 6 months. Many of whom were followed up locally and their data was not available for us to review. Thirdly, due to the small number of AKI events we were unable to make any statistical associations that would help us predict such an event.
In Summary, in this cohort of patients undergoing PRRT therapy with 177Lu-dotatate we found that incidence of Aki was low at 4.6%. We also found that the renal function after the first cycle showed a statistically significant improvement and there was no overall deterioration of renal function at the 6 months follow up. Patients with CKD did have more hematological toxicity especially with thrombocytopenia and this was despite receiving an adjusted low dose. We need ongoing long term follow up data in these patients to better understand the overall long-term kidney risk in these patients.
Supplemental Material
sj-pdf-1-jnp-10.1177_23993693211050410 – Supplemental material for 177Lu-dotatate use in chronic kidney disease patients: A single center experience
Supplemental material, sj-pdf-1-jnp-10.1177_23993693211050410 for 177Lu-dotatate use in chronic kidney disease patients: A single center experience by Sandhya Manohar, Panagiotis Kompotiatis, Thorvardur R Halfdanarson, Timothy J Hobday, Matthew Thorpe, Geoffrey B Johnson, Ayse Tuba Kendi and Nelson Leung in Journal of Onco-Nephrology
Footnotes
Author contributions
All authors have had equal contribution in the preparation of the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SM, PK, TH, MT, GJ, and NL with no conflict of interest. TH declares Research Support from Thermo Fisher Scientific, Avanced Accelerator Applications (a Novartis company), Basilea, Turnstone Biologics, Agios. TH also declares Consultancy/Advisory Board – Money paid to institution from Ipsen, Advanced Accelerator Applications (a Novartis company), ITM and Consultancy/Advisory Board – Money paid to me from Curium and Crinetics. AK is the PI of LuPSMA VISION trial at Mayo Clinic Rochester.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Mayo Clinic IRB approved this study (IRB number: 18-010667).
Informed consent
Only patients that provided Research Consent were included in this study.
Guarantor
SM.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.