
Abstract
The incidence of malignancy is increased in systemic sclerosis (SS). Nevertheless, only a few cases of paraneoplastic SS (pSS) have been described. Scleroderma renal crisis is an uncommon but severe complication of SS, with acute kidney failure, abrupt onset of hypertension and microangiopathy. We present the case of a previously healthy patient who was diagnosed with ovarian carcinoma and underwent chemotherapy with carboplatin and paclitaxel. In association with the cancer, she developed SS and scleroderma renal crisis. She received initial supportive treatment, but her renal function worsened, and she started on hemodialysis. Furthermore, she received adjuvant surgical treatment for the cancer. Eighty-four days after cytoreductive surgery, her renal function recovered, and her SS manifestations improved.
Introduction
The incidence of malignancy is increased in systemic sclerosis (SS). The most frequent cancers related to this disease are breast cancer and pulmonary carcinoma, but a wide range of malignancies have been reported. 1 Nevertheless, only a few cases of paraneoplastic systemic sclerosis (pSS) have been described. 2 Scleroderma renal crisis is an uncommon but severe complication of SS, with acute kidney failure, abrupt onset of hypertension and microangiopathy. 3 We present the case of a patient with ovarian carcinoma who developed pSS and scleroderma renal crisis.
Case report
In October 2017, a 42-year-old previously healthy woman was diagnosed with ovarian carcinoma of clinical stage IV under the American Joint Commission of Cancer classification, with lymph node metastasis.
She underwent chemotherapy with carboplatin and paclitaxel 1 month after the diagnosis.
One month after the onset of treatment, she complained of nausea and vomiting; skin thickening on the forearms, legs and abdomen; and telangiectasia of the nails. Although the skin symptoms worsened after chemotherapy, they were already present before the tumor was diagnosed. Also, she reported acrocyanosis, arthralgia, and dysphagia for the past 6 months. At this time, the hypothesis of pSS was made, since paclitaxel-induced SS would be unlikely because her symptoms appeared before chemotherapy. The antibody anti-topoisomerase-1 was negative, and unfortunately anti-centromere and anti-RNA polymerase III were not available. Nailfold capillaroscopy found microangiopathy with scleroderma patterns of capillary dilatations and dropout. Moreover, a skin biopsy established the diagnosis of scleroderma.
She was kept on chemotherapy for the next 5 months without any specific treatment for SS, which was assumed to be a paraneoplastic phenomenon. Due to a good tumor response, adjuvant cytoreductive surgery was proposed.
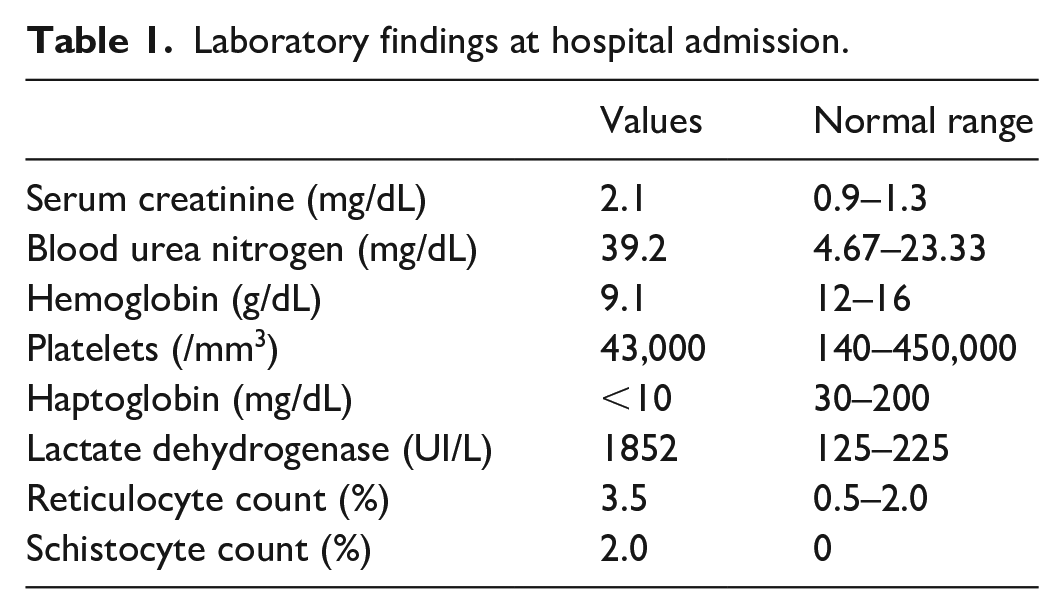
Nine months after the cancer diagnosis, she was admitted with headache, blurred vision, purpuric lesions on her feet, and blood pressure of 180/100 mmHg. Laboratory tests showed acute kidney injury, microangiopathic hemolytic anemia, proteinuria and hematuria with dysmorphic red blood cells (Table 1). The spot urinary protein-to-creatinine (CR) ratio was 5.29 g/g, and kidney ultrasound was otherwise normal, without signs of hydronephrosis, calculi or renal artery stenosis. Brain CT was also unremarkable. She was admitted to the intensive care unit (ICU) and soon developed hemoptysis and dyspnea. Therefore, her pulmonary-renal vasculitis was considered beyond scleroderma renal crisis. Due to the severity of the manifestations, she received empiric pulse therapy with methylprednisolone 1 g/day for 3 days associated with four sessions of therapeutic plasma exchange. Despite pulmonary improvement, her renal function worsened. Further investigation showed a positive antinuclear factor titer of 1/1280 with a speckled pattern and a positive anti-smooth muscle antibody titer of 1/40 with a vascular pattern. Anti-Ro, anti-La, anti-Jo, anti-Sm, anti-RNP, anti-topoisomerase antibodies, serum antineutrophil cytoplasmic antibody (ANCA) and double-stranded DNA antibodies were all negative. Rheumatoid factor and complement were normal. A kidney biopsy was performed after discharge from the ICU and 20 days after methylprednisolone pulse, which showed prominent arteriolar myointimal proliferation, mesangiolysis, and capillary loop collapse; all of these confirmed the diagnosis of scleroderma renal crisis (Figures 1 and 2). Hence, her corticosteroid was tapered down, and oral captopril 125 mg thrice a day was initiated.
Laboratory findings at hospital admission.
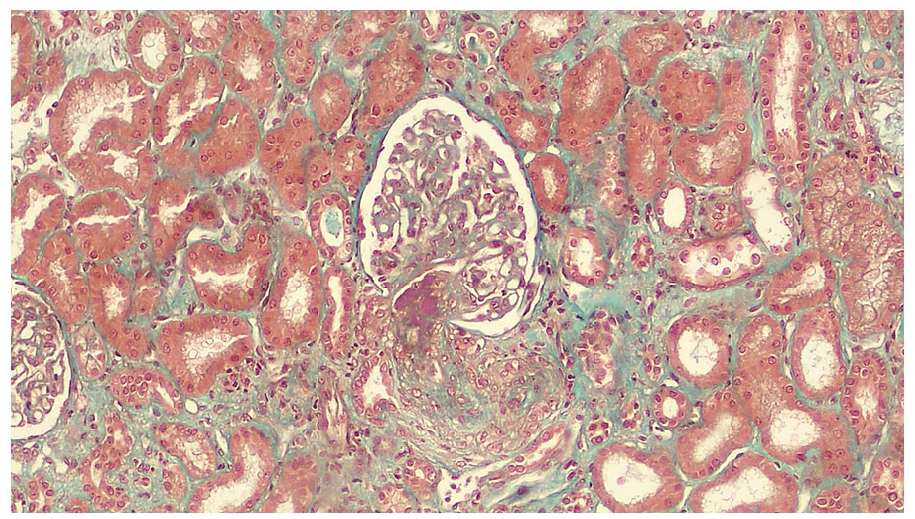
Hilar arteriole displaying acute thrombosis and intimal proliferation. The glomerulus shows ischemic changes (Masson’s trichrome, 200×).
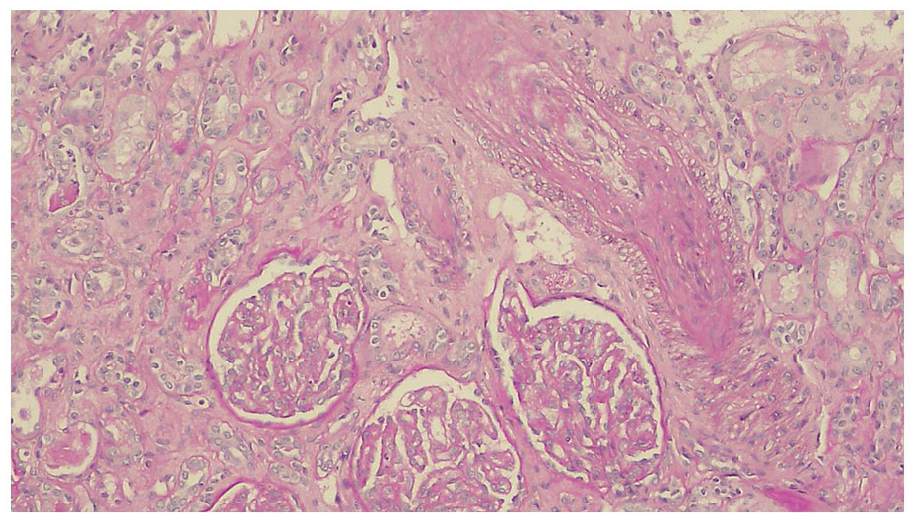
Luminal obliteration of interlobular artery and arteriole due to intimal fibrous proliferation (top right). Glomeruli presenting mesangiolysis and segmental basement membrane duplication (bottom). (PAS, 100×).
As the renal function further deteriorated (serum CR 5.6 mg/dL and daily urinary output 500 mL), she started hemodialysis therapy. Two months later, she underwent adjuvant cytoreductive surgery without any postoperative complications. She remained on dialysis for the next 3 months with fair blood pressure control under captopril 100 mg thrice a day. Due to Raynaud’s symptoms the patient was kept on diltiazem. Eighty-four days after the beginning of hemodialysis, her urine output increased, and her glomerular filtration rate (GFR) measured by Cr-EDTA was 14 mL/min/1.73 m2, so hemodialysis was halted.
For the next 2 months, treatment with captopril 300 mg/day was sustained, and her renal function fully recovered (serum CR 1.2 mg/dL), Furthermore, the changes in the nailfold capillaries (scleroderma pattern) regressed as well as the Raynaud’s symptoms improved.
Discussion
SS is a connective tissue disease characterized by microangiopathy and progressive fibrosis of the skin and internal organs. It is a clinically heterogeneous disorder associated with high mortality, and internal organ involvement can affect patient prognosis. 4 Scleroderma renal crisis is an uncommon (incidence of 5%–13%) 3 but severe complication of SS, with acute kidney failure, abrupt onset of hypertension and microangiopathy. It is associated with high mortality and progression to end-stage renal disease (ESRD). The patients have marked elevation of serum renin levels at the onset of scleroderma renal crisis, which supports the treatment with angiotensin-converting enzyme (ACE)-inhibitors, as a consistent rate of dialysis discontinuation (40%–50%) has been reported after a mean ACE treatment period of 8–11 months. 3 Exposure to steroids is known to be a risk factor for the development of SRC, however in our patient the onset of kidney dysfunction occurred before the use of corticosteroids.
Several reports have shown an increased risk of malignancy in patients with SS. 1 Fibrosis, chronic inflammation and B-cell stimulation may play a role, but the physiopathology is not fully elucidated³. Cancers more correlated with SS are breast and pulmonary carcinomas, the latter being more often described in the literature due to lung fibrosis, chronic inflammation and immunosuppressive therapy. 4
Few cases of pSS have been described, and its pathogenesis is linked to the development of cancer-induced autoimmunity.1,2 Cancer cells may produce biologically active cytokines and growth factors that are considered profibrotic, such as transforming growth factor-β (TGF-β). Interestingly, TGF-β is elevated in several malignancies, notably breast, renal, and ovarian cancers. 1 Many chemotherapies also contribute to SS, such as paclitaxel, docetaxel, and bleomycin. 1
The clinical and laboratory findings in patients with pSS are similar to those in patients with idiopathic SS, but the following characteristics deserve attention in pSS: close temporal association between the SS symptoms and the cancer diagnosis; prompt response to chemotherapy; and recurrence with cancer relapses. Additionally, the absence of regression after surgery or chemotherapy virtually excludes the diagnosis of pSS. 2
Samotij et al. 5 described a case of pSS in a patient with colon adenocarcinoma 8 weeks after cancer surgery, characterized by skin and digital thickening, pulmonary fibrosis and dysphagia; all of these symptoms improved within 2 years. As the cancer relapsed, the symptoms were aggravated, and the patient eventually died. Crosnier et al. 6 reported on two cases of pSS whose initial manifestation was scleroderma renal crisis months before the cancer diagnosis. These case reports are summarized in Table 2.
Previous case reports of pSS.

Drug induced scleroderma is a rare condition reported after chemotherapy with bleomycin, paclitaxel, and docetaxel. Classically, the cutaneous changes are prominent, with panniculitis or cellulitis-like reactions, autoantibodies are negative, and systemic involvement is not usually reported. 8 In our patient, the symptoms started before chemotherapy, the visceral involvement (scleroderma renal crisis, Raynaud’s phenomenon) were exuberant, and nonspecific autoantibodies were present. However, we could not exclude that chemotherapy, as a second hit, accelerated the fibrotic process.
Conclusion
In this case report, the diagnoses of ovarian carcinoma, SS and scleroderma renal crisis were made within 12 months, and this close temporal association strengthened the likelihood of pSS. Additionally, the marked regression of symptoms after resection of the tumor reinforced this diagnosis. To the best of our knowledge, this is the first description of pSS where the patient was alive and dialysis independent.
Footnotes
Acknowledgements
None to declare.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This case report was approved by the local ethical committee of the Faculty of Medicine of University of São Paulo (CCEP 1964/21).
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Trial registration
NA.
Guarantor
ECC.
Contributorship
Conception: MM, FZM. Collection of data: MM, FZM, LBC. Manuscript writing: All authors. Final approval of manuscript: All authors. Accountable for all aspects of the work: All authors.