
Abstract
Background:
Kidney transplant recipients are at high risk of developing cutaneous squamous cell carcinoma (cSCC) due to prolonged immunosuppression. While most lesions can be managed with local therapy, a subset of patients develop advanced cSCC that is unresectable, recurrent or metastatic. Immune check point inhibitors (ICI) and chemotherapy may jeopardize the transplanted kidney. Cetuximab, an anti-epidermal growth factor receptor antibody, has demonstrated efficacy in advanced cSCC, but data regarding efficacy and safety in solid organ transplant recipients is lacking.
Methods:
This retrospective cohort study analyzed kidney transplant recipients diagnosed with locally advanced or metastatic cSCC who were treated with cetuximab.
Results:
Seventeen patients were included in the analysis. The median age was 57 years at the time of kidney transplantation and 62 years at diagnosis of index lesion. Cetuximab was administered with radiation therapy as a radiosensitizer in 58.8% of patients, as monotherapy in 17.6% of patients, and with chemotherapy in 23.5% of patients. Importantly, no detrimental impacts on kidney graft function were observed. The main toxicites were grade 1–2 skin reactions and electrolyte imbalance. Of the 10 patients receiving cetuximab with chemoradiotherapy as a radiosesnitizer, 2 were treated with definitive intent, 7 of them in the adjuvantsetting, and 1 for palliative pourpose. Over half of these patients achieved a complete response (37.29%) or no recurrence after resection (23.5%). Median time to disease progression was 10 months.
Conclusions:
This novel study suggests cetuximab has a reasonable safety profile and potential efficacy in kidney transplant recipients with advanced cSCC, without impairing allograft function. Further prospective research with larger sample sizes is warranted to confirm these findings. Cetuximab should be investigated as a systemic treatment option for this high-risk population of solid organ transplant recipientss with recurrent, metastatic, or unresectable cSCC.
Introduction
Solid-organ transplant recipients are subjected to long term immunosuppressive therapy, and are thus at an increased risk for cancer. Non melanoma skin cancer, and particularly cutaneous squamous cell carcinoma (cSCC), is the most common malignancy in solid organ transplant recipients, and accounts for about 50% of all cancers in this population.1,2 Furthermore, the risk for developing cSCC increases with the duration of the immunosuppressive therapy, and patients treated for 20 years have over 80% for developing cSCC. 3
In immunosuppressed patients, cSCC has high recurrence rates and displays a more aggressive behaviour including deep tissue involvement, perineural invasion, and lymphatic invasion. 4
The complex relationship involves factors such as UV exposure and the impact of immunosuppressive drugs on antiproliferative or cancer-promoting pathways. Evaluating specific immunosuppressive agents is crucial for assessing individual patient risk. A retrospective study showed that kidney-transplant recipients who were receiving prednisolone, azathioprine, and cyclosporine had a risk of squamous-cell carcinoma that was three times as high as the risk among those receiving prednisolone and azathioprine alone. 6 Mammalian target of rapamycin (mTOR) inhibitors, like sirolimus, everolimus, and temsirolimus, exhibit both immunosuppressive and antiproliferative effects.5 –7 Due to their antiproliferative and antineoplastic effects, these agents offer a valuable alternative for solid organ transplant recipients at high risk for skin cancer. Therefore, reducing and adjusting immunosuppressive therapy is essential. 7
For the majority of cSCC, the treatment of choice is surgery. A systemic review and pooled analysis assessing different treatment modalities found 5-year local recurrence rates of 3, 5.4, and 6.4% for Mohs procedure, local excision, and radiation therapy, respectively. 8
Approximately 8% of organ transplant recipients develop metastic cSCC, in which case prognosis is poor: in a retrospective study that included 58 organ transplant recipients with distant metastases of cSCC, the three-year disease-specific survival rate was 29%. 9
In a previous large cohort study conducted among solid-organ transplant recipients in the USA, the specific mortality rate attributed to skin cancer was approximately 35 per 100,000 person-years. This rate was nearly nine times higher than the mortality rate reported for the general population. It’s worth noting that this study was published before ICI treatment became a common therapeutic option. 10
Treatment options for metastatic or unresectable cSCC are limited. The use of chemotherapy, and platinum analogues in particular (mostly in doublet regimens, along with antimetabolites or antimicrotubule agents), has been reported with some success among immunocompetent patients.11,12 However, among renal transplant recipients these agents may jeopardize the transplanted kidney due to nephrotoxicity and may expose these immunosuppressed patients to infections due to myelotoxicity.
Recently, immune-checkpoint inhibitors cemiplimab and pembrolizumb have been introduced for the treatment of cSCC not amenable to curative intent treatment, showing promising results and a high response rate.13,14 However, clinical trials assessing ICI safety excluded organ-transplant recipients, due to concerns regarding allograft rejection. In a systemic review assessing the safety of ICI in transplant recipients nearly two-thirds of patients had allograft rejection. 15
The monoclonal antibody cetuximab, targeting the epidermal-growth factor receptor, has also been evaluated in patients with cSCC. In a phase II study of 36 patients with advanced cSCC, disease control rate was 69% with two complete responses and eight partial responses. 16 The relatively low toxicity profile of this agent makes it a reasonable treatment option for kidney-transplant recipients. However, to our knowledge, data regarding cetuximab in this population has not been published.
In this analysis, we aim to assess the safety and efficacy of cetuximab among kidney-transplant recipients with cSCC.
Methods
Design and patient sample
A retrospective cohort study was performed using the Rabin Medical Center (RMC) database. A list of consecutive kidney transplant recipients was cross referenced with a list of patients treated with cetuximab between the years 2011–2023. Patients were included in the analysis if they met the following criteria: (I) patients age > 18 years who underwent kidney transplant in RMC, (II) A biopsy confirmed cSCC post-transplant, (III), Treated with cetuximab in RMC for cSCC. Exclusion criteria were: (I) Pregnancy, (II) a malignancy other than cSCC. The study adhered to the Declaration of Helsinki Principles, and the medical ethics committee of RMC had approved the study design (RMC-077620). Due to the retrospective nature of the research, the requirement for informed consent was waived.
Data collection
Data was collected anonymously from the patients’ medical charts and included demographic data such as age at transplant and at diagnosis of cancer, sex, and ethnicity; as well as clinical variables such as reason for transplant, immunosuppressive regimen, sites of cancer and history of cSCC, concurrent cSCC to index lesion, intent of cetuximab treatment (i.e. concurrent with definitive/adjuvant radiotherapy or in the recurrent/metastatic setting) previous lines of treatment, time to progression, allograft function, and adverse effects.
Statistical analysis
Descriptive statistics, including frequency, percentage, mean, median, range, and standard deviation, were calculated with Microsoft Excel for Mac 2016 v16.16.
Results
A retrospective analysis was conducted on a cohort of kidney transplant recipients with metastatic or unresectable cSCC who received cetuximab treatment between January 2011 and December 2023 at Rabin Medical Center. Seventeen patients were included in the analysis.
Median follow-up was 21 months (range 6–35).
Sample characteristics
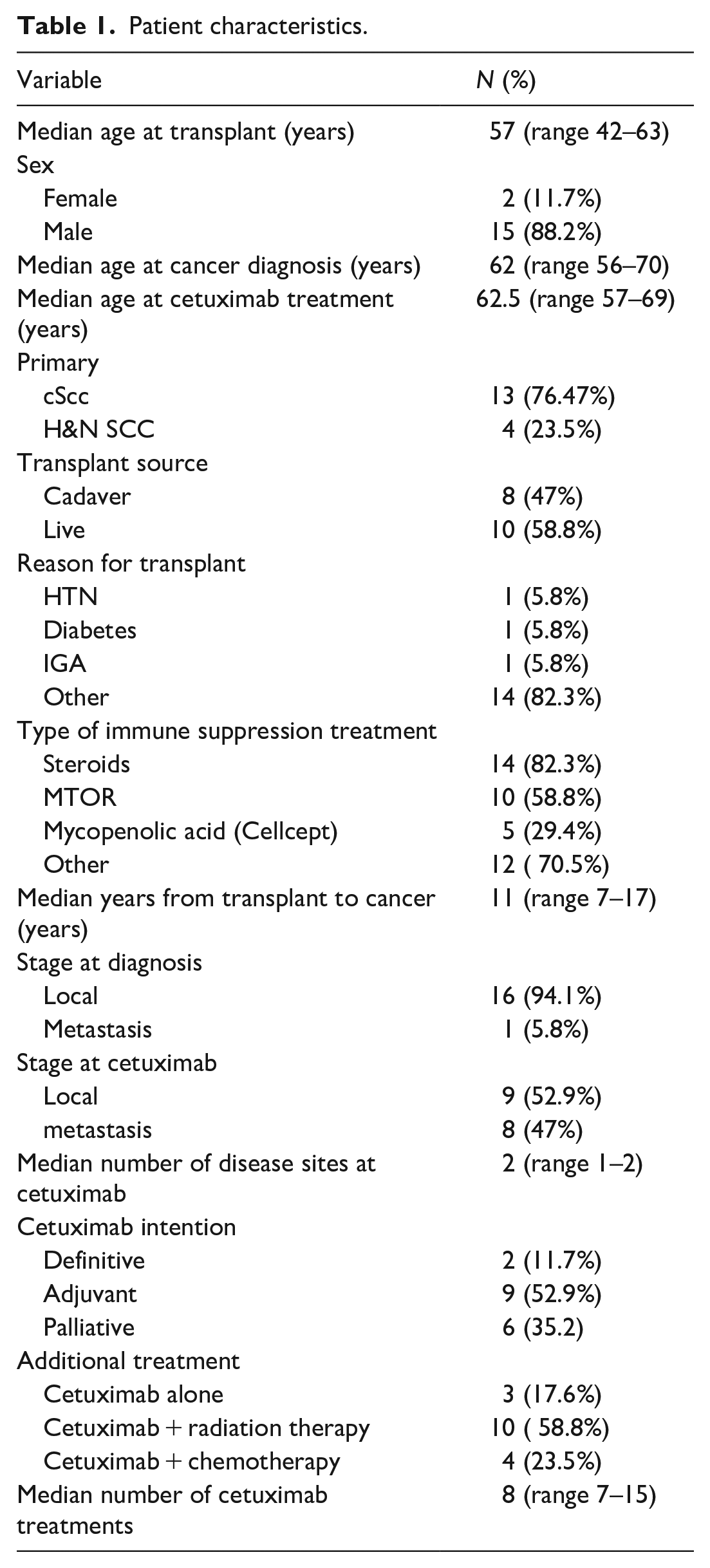
Patient characteristics are presented in Table 1. The median age at the time of transplantation was 57 years and the median age at cSCC diagnosis was 62 years. Majority of patients were male (n = 15). Sixteen patients (94.1%) presented with local disease. Two patients (11.7%) received cetuximab with a definitive treatment intent, while nine patients (52.9%) received it as an adjuvant therapy, both along with radiotherapy. In patients with local disease, the median number of weekly cetuximab cycles was 7 (range 5–8), whereas among those with metastatic disease, it was 16 (range 11.5–18.75). Cetuximab was given as a monotherapy for 3 patients (17.6%), combined with radiation for 10 patients (58.8%), and combined with chemotherapy for 4 patients (23.5%).
Patient characteristics.
Safety of cetuximab
Table 2 specifies adverse effects associated with cetuximab. Serum creatinine levels, used to estimate kidney function, remained stable throughout cetuximab treatment, with no significant changes observed. The median estimated glomerular filtration rate (eGFR) before the initiation of cetuximab treatment was 50.1 (range 39.1–69.4), and there was no significant change observed at the conclusion of the treatment, with a final median eGFR of 53.3 (range 43.2–86). It is noteworthy that a few patients presented with chronic rejection, as indicated by diminished eGFR at baseline. None of the patients experienced organ rejection or malfunction.
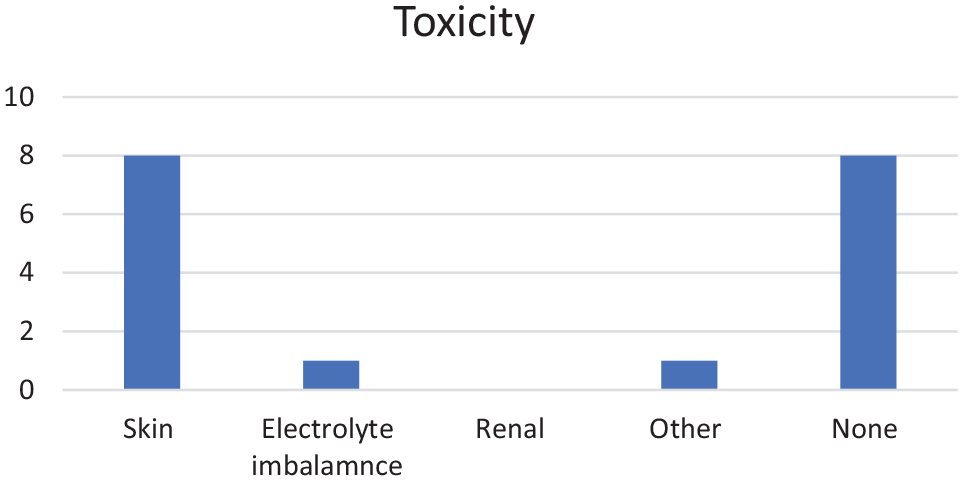
Other toxicities observed in this cohort included skin toxicity in eight patients (all were low grade events except for one that was grade 3). One patient developed grade 2 electrolyte imbalances, notably hypomagnesemia. Nearly half of patients did not develop any toxicity (Figure 1).
Adverse effects associated with cetuximab.

Adverse effects associated with cetuximab.
Cetuximab efficacy
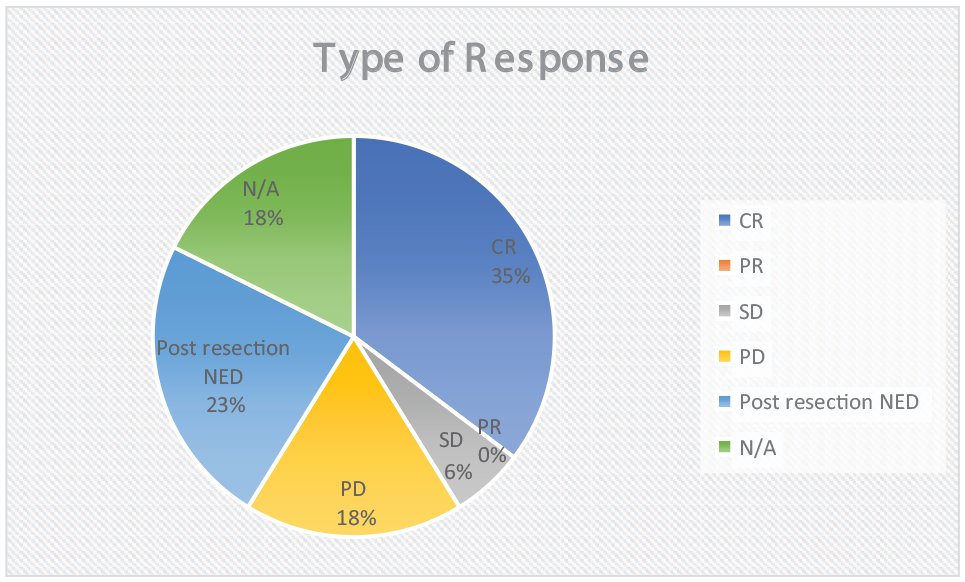
Response evaluation in presented in Figure 2.
Response to cetuximab.
Four patients (23.52%) achieved post-resection No Evidence of Disease (NED).
Six patients (37.29%) achieved a complete response, and three (17.64%) had progressive disease. Three patients could not be evaluated for efficacy (Figure 2). The median time to disease progression, among evaluable patients, was 10 months (range 8.5–20). Seven patients (41.17%) completed the planned treatment, while four (23.5%) discontinued treatment due to toxicity.
Patients received various immunosuppression therapies, including steroids, MTOR inhibitors, and Mycophenolic acid (Cellcept). The majority of patients underwent steroid treatment (82.3%), whereas 58% received mTOR inhibitors. Among the nine patients who received mTOR inhibitors, two achieved complete response (CR), and one patient had progressive disease (PD), as opposed to four and three out of eight patients, respectively, who did not receive mTOR inhibitors. However, there was no significant difference in the time to progression, with a median time of 14 months in the group receiving mTOR inhibitors compared to 10 months in the group without mTOR inhibitors.
Discussion
In this retrospective study, we assessed the safety and efficacy of cetuximab for the treatment of metastatic or unresectable cSCC in kidney transplant recipients. The current standard of care for patients with localized cSCC not amenable to curative intent resection, either due to disease extent or medical comorbidities, may involve a combination of radiation, chemotherapy, immune checkpoint inhibitors (ICI), or various therapies.18,19 As per the National Comprehensive Cancer Network (NCCN) guidelines, version 2.2022, systemic therapy options for cSCC may encompass different regimens, including immune checkpoint inhibitorssuch as cemiplimab and pembrolizumab, chemotherapy, or EGFR inhibitors like cetuximab. 20
Our results suggest that cetuximab may be a reasonable treatment option for this patient population, with no observed graft failures and manageable adverse events. This study adds to the limited data on systemic treatments for advanced cSCC in the immunosuppressed population. In spite of the antiproliferative and antineoplastic actions of mTOR inhibitors, there seems to be no significant difference concerning a positive treatment response.
To our knowledge, it is the first analysis focused on cetuximab in post-transplant cSCC.
Safety
The safety profile of cetuximab in our cohort appears consistent with what has been reported previously in non-immunosuppressed populations. For example, a trial by O'Bryan et al showed that cSCC patients treated with cetuximab had papulopustular (acneiform) rash classically described with EGFR inhibitors, which was able to be effectively treated. 20 The most common toxicity in our study was low grade skin reactions, which were seen in eight (47%) patients. Only one patient experienced a grade 3 skin toxicity. Grade 4 electrolyte imbalances (hypomagnesimia) were individually observed in one patient; however, these incidents, while severe, did not necessitate the discontinuation of treatment. Nearly half of the patients did not experience any cetuximab-related toxicity. Pulmonary toxicity, as described in other anti-EGFR agents like Gefitinib and Erlotanib,21,22 was not documented in our cohort.
Importantly, no detrimental impact on kidney function or graft survival was seen. These safety findings are encouraging given the concerns about increased treatment-related risks in transplant recipients receiving chronic immunosuppression. The lack of graft dysfunction indicates cetuximab may be less nephrotoxic than systemic chemotherapy agents.
In comparison, a large multi-center retrospective study on kidney transplant recipients revealed a high incidence of graft rejection (42%) among patients treated with ICIs, with a significant percentage experiencing allograft failure. The number of immunosuppressants administered at the time of ICI initiation was associated with a lower risk of acute rejection. 23 Two case reports document acute antibody-mediated rejection of a kidney allograft after the initiation of a PD-1 inhibitor in renal transplant patients.24,25
The benefits of tumor regression must be balanced against the risk of allograft rejection. Our study demonstrated the ability to deliver cetuximab without compromising the transplanted kidney making it a particularly appealing systemic therapy option in this population.
Efficacy
While limited by a small sample size and retrospective design, our results appear promising. Over half of the patients in the cohort exhibited no recurrence or progression following cetuximab treatment. Specifically, out of these patients, nine received a combination treatment of RT and cetuximab after surgical resection and one patient received cetuximab alone post-resection. These results are similar to those published by Preneau et al, which demonstrated a disease control rate of 78% among cSCC patients who were not eligible to local treatment. 25 The patient population in this trial, however, were not organ transplant recipients. The median time to progression in our study was 10 months, a result consistent with response durations reported in other trials using cetuximab for cSCC. 16 Compared to historical outcomes for metastatic cSCC in organ transplant recipients, cetuximab treatment in our cohort seems to be associated with favorable survival.16,17
Cetuximab is considered a radiosensitizer as it has a synergistic effect in combination with RT.26,27 According to the findings by Bonner et al., the application of concomitant high-dose radiotherapy alongside cetuximab for the treatment of locoregionally advanced head and neck cancer results in improved locoregional control and reduced mortality. 26 Indeed, most patients in our study received combined treatment with RT (58.8%). A prospective study of 20 patients with locally advanced cSCC compared cetuximab alone versus cetuximab combined with cisplatin or RT (60–70 Gy). Combination therapy had higher response rates versus cetuximab alone (disease control rate, 92% versus 50%, respectively, and response rates, 53% versus 33%, respectively). 26
Several limitations should be considered when interpreting our findings. The retrospective nature of the study introduces the possibility of selection bias, and suffers from a lack of randomization, blinding, or a true control arm. Additionally, the collection and analysis of patients’ medical charts from as far back as 2011 posed challenges, leading to limited availability of certain information. Moreover, the study’s small cohort size restricts the generalizability of the findings to the broader population.
Despite these limitations, our study was conducted at a tertiary medical center which is the largest transplant center in the country and thus has significant strengths. The inclusion of a diverse patient population enhances the robustness of our findings. Further research with larger cohorts and prospective study designs is warranted to validate our results and optimize the use of cetuximab in kidney-transplant recipients with cutaneous squamous-cell carcinoma.
Conclusion
In conclusion, our study demonstrated the safety of cetuximab treatment in kidney-transplant recipients, with no cases of graft rejection observed among the seventeen patients analyzed. This suggests that cetuximab, when used in this context, does not pose a significant risk of transplant rejection and may yield oncologic benefit. Further research is needed to better understand the risk factors associated with rejection and identify potential therapeutic targets. Prospective studies are warranted to provide more robust evidence in this field.
Footnotes
Acknowledgements
N/A
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study adhered to the Declaration of Helsinki Principles, and the medical ethics committee of RMC had approved the study design (RMC-077620).
Informed consent
Due to the retrospective nature of the research, the requirement for informed consent was waived.
Trial registration
N/A
Guarantor
N.K
Contributorship
All authors had a significant contribution to this study, as follows: H.N - data collection, writing and editing, statistical analysis; O.I—Conceptualization, writing and editing; N.B.D—writing and editing; A.P—data collection; L.G—data collection; B.D—writing and editing; R.R—Conceptualization, writing; N.K—Conceptualization,statistical analysis, writing andediting.