
Abstract
Introduction:
Monoclonal gammopathy of renal significance (MGRS) is characterized by clonal cell deposition of monoclonal immunoglobulin causing renal manifestations without overt malignancy. MIDD is a subtype of MGRS characterized by deposition of monoclonal light (LCDD), heavy chains (HCDD), or both (LHCDD) along the renal glomerular and tubular basement membranes. Virtually all organs can be involved, and if left untreated, MIDD can progress to MM and end stage renal disease. Although these patients classically did not receive treatment, current MIDD management is primarily focused on controlling the underlying clonal plasma cell disorder.
Case description:
We present a 56-year-old male with atypical MIDD treated successfully with plasma cell directed therapy consisting of daratumumab, cyclophosphamide, bortezomib, and dexamethasone (DARA-CYBOR-D). Despite a primary diagnosis of diabetic kidney disease, renal biopsy suggested myeloma-related MIDD based on linear immunofluorescent staining for IgG and kappa light chains along the tubular and glomerular basement membranes. Notably there were no electron dense deposits in the mesangium or tubular basement membranes typical to MIDD electron microscopy. Despite the presentation of MIDD on IF only, DARA-CYBOR-D treatment led to hematologic and renal improvement and remission from MIDD, with a GFR increase from 22 to 59 mL/min/BSA and a drop in urine protein from up to 9 to 0.6 g/dL.
Conclusions:
In conclusion, our case illustrates the efficacy of the DARA-CYBOR-D regimen in a patient with IF-only MIDD. We highlight the importance of obtaining a kidney biopsy when there are other potential causes for real decline and enhance our understanding of pathological and clinical spectrum of MIDD.
Introduction
Monoclonal Gammopathies (MG) are a spectrum of disorders that result from clonal proliferation of plasma or B cells, ranging from pre-malignant monoclonal gammopathy of undetermined significance (MGUS) to the hematological malignancy multiple myeloma (MM). Monoclonal gammopathy of renal significance (MGRS) lies within this continuum and is characterized by clonal cell deposition of monoclonal immunoglobulin or fragments causing renal manifestations.1,2 These patients do not have features of an overt malignancy like MM and historically did not receive clone directed therapy.3,4 Although many patients with monoclonal immunoglobulin never develop renal disease, others manifest specific patterns of renal injury such as monoclonal immunoglobulin deposition disease (MIDD). MIDD is characterized by congo red-negative deposition of monoclonal light (LCDD), heavy chains (HCDD), or both (LHCDD) especially along the renal glomerular and tubular basement membranes. 3 Although virtually all organs can be involved in MIDD, most patients have renal manifestations, including hypertension, nephrotic syndrome, and decline in glomerular filtration rate (GFR). Untreated MGRS can progress to MM and end stage renal disease (ESRD).
Current MIDD management, based on limited evidence, is primarily focused on controlling the underlying clonal plasma cell disorder. 4 In a retrospective nationwide cohort of 255 patients, bortezomib based chemotherapeutic approaches showed promising results, with 67% and 36% of patients achieving a hematologic and renal response respectively. 5 Recently a novel regimen combining daratumumab, cyclophosphamide, bortezomib, and dexamethasone (DARA-CYBOR-D) has improved patient response rates and renal outcomes.6,7
Here we report the presentation and treatment of a unique histological variant of MIDD co-morbid with diabetic kidney disease. Alongside management of his diabetes, the patient responded to a therapeutic regimen of DARA-CYBOR-D and is in complete remission from MIDD. This case highlights a pathology of MIDD that has been sparsely reported in the literature, the importance of obtaining a renal biopsy, and the response to tailored patient treatment.
Case description
A 56-year-old male with diabetes mellitus (DM) and MGUS has worsening chronic kidney disease (CKD) for at least a year, with a creatinine of 3.13 mg/dL and 24-h urine protein up to 9 g/dL albuminuria. The renal decline appeared to be secondary to DM. Additional workup revealed an M-spike of 2.3 g/dL, elevated Kappa/Lambda Free light chain ratio of 38.7 (Kappa 29.4 and Lambda 0.76), and an isotype of IgG Kappa on mass spectrometry. Bone marrow was consistent with 30% kappa restricted plasma cells.
The patient was referred to onco-nephrology and hematology teams for further evaluation of his chronic kidney disease and to rule out MGRS. An outside renal biopsy demonstrated several key findings consistent with diabetic glomerulosclerosis and severe arteriosclerosis, including thickened glomerular basement membranes, mesangial expansion and focal segmental, and global glomerulosclerosis (Figure 1(a)–(c)). However, upon further review at our center there was identification of linear staining for IgG and kappa light chains along the tubular and glomerular basement membranes via IF (Figure 1(d)–(f)). This unique finding raised suspicions of an unusual presentation of MGRS, particularly MIDD. On EM, the glomerular basement membranes appeared thickened and mesangium showed an increase in matrix material, albeit without electron dense deposits expected in MIDD (Figure 1(g)–(i)).
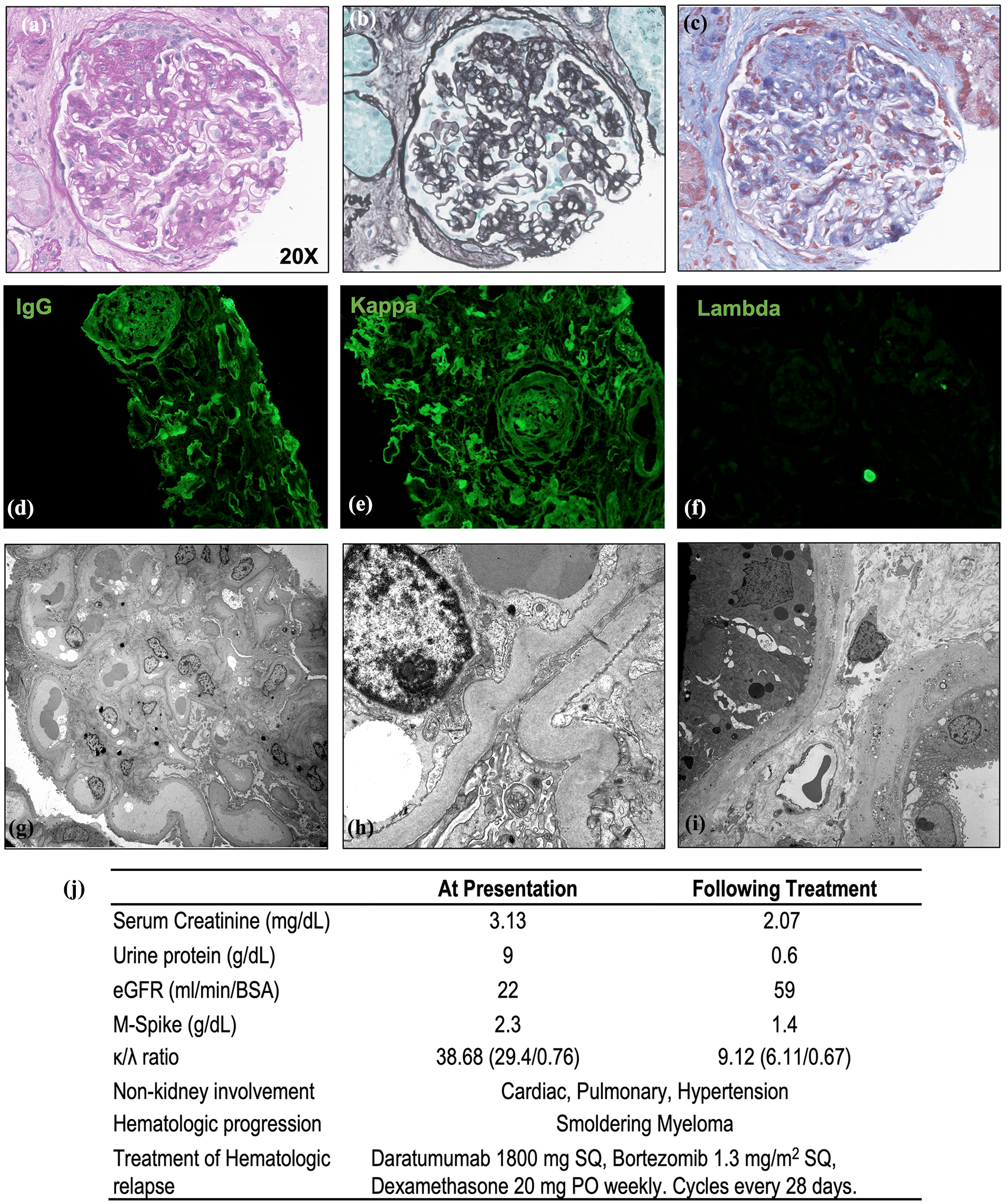
Light microscopy highlighting a glomerulus on renal cortex biopsy with PAS (a), Bence-Jones (b), and Trichrome (c) staining. Glomeruli show segmental sclerosis with segmental consolidation of the capillary tufts and adhesion of the sclerosed segments to the Bowman’s capsule. Glomeruli also display mesangial expansion with an increase in mesangial matrix and a mild increase in the cellularity of the mesangium. IF staining for (d) IgG and (e) Kappa light chains showing linear staining of glomerular basement membranes, Bowman’s capsule, and the tubular basement membranes. (f) Lambda light chains are negative. EM of the (g, h) glomerulus and (i) tubular basement membranes showing no punctate powdery deposits in the mesangium or along the glomerular and tubular basement membranes. (j) Summary of patient baseline characteristics and treatment progression.
The patient’s deteriorating kidney function and new findings prompted the initiation of an eight-cycle treatment regimen of DARA-CYBOR-D (daratumumab, cyclophosphamide, bortezomib, and dexamethasone). The patient exhibited a positive hematological and renal response to DARA-CYBOR-D, with a reduction in monoclonal protein levels, GFR increase from 22 to 59 mL/min/BSA, and a significant drop in urine protein to 0.6 g (previously 9 g/dL). (Figure 1(j)). He is currently in remission from MIDD.
Conclusions
Differentiating MIDD from other subtypes of MGRS and the spectrum of MIDD-related lesions requires the integration of morphological alterations seen on LM, IF, and EM. 2 Classic MIDD can be distinguished from a rare subtype of MIDD identified by IF-only, as the latter lacks the characteristic punctate, dense immunoglobulin deposits seen on the tubular basement membranes via EM. 8 Ancillary diagnostic workup of MGRS lesions with more sensitive techniques such as liquid chromatography and tandem mass spectrometry (LC-MS/MS) or immunogold EM has been proposed for individuals with inconclusive findings on IF or EM. 2 The presentation of IF-only MIDD has been sparsely described and may represent an early LCDD lesion which can progress to classic LCDD if left untreated.7 –9 Our case supports that MIDD may be on a continuum of histological patterns that evolves with disease progression.
While treatment guidelines based on controlled trials are still lacking for MIDD, current management involves the regulation of the underlying plasma cell disorder. 5 Before the practice of clone directed therapy, median patient survival was 2 years following diagnosis of MIDD. 7 Achieving hematological response was the main prognostic factor linked to overall survival (OS) in the largest MIDD cohort to date, with OS at 36 months 44% higher in these patients compared to those who did not respond favorably to treatment (88% vs 44%). Moreover, OS was 27% higher in patients with renal response to therapy (87% vs 60%), defined by decrease in proteinurea and increase in GFR. Use of bortezomib based regimens was associated with higher renal and OS. 5 Other studies have also highlighted the potential of this bortezomib-based approach for MGRS and specifically for LCDD in combination with the anti-CD38 monoclonal antibody daratumumab. 10 Our case, which utilized the DARA-CYBOR-D regimen to achieve CR, supported the effectiveness of such a treatment approach, even in a patient whose kidney manifestations did not fit all the criteria expected in MIDD.
The challenge of treating MIDD comes from its heterogeneous presentation, ancillary workup needed for inconclusive findings and the current limited evidence-based therapeutic regimens. IF-only LHCDD MIDD is a pathology scarcely reported and mandates early initiation of treatment to prevent progressive decline in renal function. Our case demonstrates the potential effectiveness of the DARA-CYBOR-D regimen in managing comorbid MIDD, presenting a treatment option that can positively impact hematological and renal outcomes in such patients. Further research and larger-scale studies are necessary to validate the efficacy of the DARA-CYBOR-D regimen and its role in the management of IF-only LHCDD MIDD and other MGRS subtypes. This report serves as a valuable contribution to the diagnosis and treatment of complex MIDD cases, even when all the classical manifestations of MIDD are not present.
Footnotes
Acknowledgements
NA.
Author contributions
MD and RC composed the manuscript. RC, NL, and SS provided expertise in interpretation of pathology images, mentorship, and review of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
NA.
Informed consent
Consent was obtained for using patient information and samples for research.
Guarantor
RC.