
Abstract
Introduction
A new coronavirus, named SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2) by the World Health Organization (WHO), has spread rapidly around the world since its first reported case in late December 2019 in Wuhan, China. 1 As of March 2020, this virus has affected more than 200 countries and territories, infecting more than 800,000 people and causing more than 40,000 deaths.1,2
In Brazil, the evolution of the pandemic was characterized by three peaks in deaths: in the 30th epidemiological week of 2020, in the 14th of 2021, and in the 6th of 2022, which generated three waves of cases, starting in the North and Northeast regions. In any case, the presence of these three waves of COVID-19 was clear, as well as the effect of immunization in reducing mortality in the second and third waves, attributed to Delta and Ômicron variants, respectively. Despite this, there was no effect on reducing morbidity, which peaked in the third wave with the predominance of the Ômicron variant. 3
Individuals affected by cancer are more susceptible to infections due to coexisting chronic diseases, poor general health, and systemic immunosuppressive states caused by cancer and anticancer treatments. Therefore, cancer patients infected with the SARS-CoV-2 coronavirus may present a more complicated evolution than other populations. 1
The ICU admission rate for patients with cancer was 40% compared to patients without cancer, giving a pooled estimate of the average rate of 8.42%. The mortality rate of patients with cancer was 20.83%, while that of patients without cancer was 7.82%, so the presence of cancer has a significant impact on death in patients with COVID-19. 4
Cancer treatment, such as chemotherapy, radiotherapy, targeted therapy, and immunotherapy, by suppressing the patient’s immune system, compromises their ability to fight viral infection. Studies show that these patients have a high risk of developing multiple organ failure, the need for mechanical ventilation, and death, when compared to patients without cancer. The mortality risk of patients with cancer and COVID-19 is about 25.6% compared to 2.3% in the normal population.1,5,6
In another study with a total of 4966 patients with COVID-19 and a history of active cancer, 58% were hospitalized and 14% died within 30 days. Of these, 61% had cancer present, diagnosed, or treated in the year before their COVID-19 diagnosis.7–9
Studies show that older individuals are more commonly affected by cancer and are more likely to develop serious complications due to COVID-19. This occurs because the aging of the immune system and the presence of comorbidities associated with aging can aggravate the inflammatory response caused by the virus. 10
According to the Centers for Disease Control and Prevention (CDC), people over the age of 65 account for 31% of COVID-19 infections, 45% of hospitalizations, and 80% of deaths caused by COVID-19.11,12
The study aims to investigate the incidence, risk factors, and evolutionary factors associated with AKI in COVID-19 patients with cancer. This is important because AKI is a major complication in these patients and is strongly associated with higher mortality rates. The study also seeks to examine any potential urinary changes such as proteinuria and hematuria in infected patients and correlate clinical factors with the presence of AKI in SARS-CoV2 infection. The goal is to outline the best prevention strategies, even with available vaccination coverage, and organize nephrology, oncology, and intensive care services for the most appropriate support measures available for these patients.
Methodology
This is an observational, retrospective clinical study of patients with a diagnosis confirmed by RT-PCR for SARS-CoV2 admitted to an oncology hospital, with associated AKI and admitted to the ICU.
Case selection
The data were obtained by consulting the electronic medical records of patients hospitalized with COVID-19 admitted to the ICU from 03/2020 to 07/2021. The inclusion criteria were patients over 18 years of age; with a confirmed diagnosis of COVID-19 by RT-PCR; admitted to the ICU; and patients with an oncological diagnosis during or after previous cancer treatment. The exclusion criteria were patients with chronic kidney disease (CKD) on dialysis or undergoing previous kidney transplantation, who did not meet the diagnostic criteria (RT-PCR SARS-CoV2 negative) for COVID-19 and admitted to the ward with COVID-19 without being in the ICU.
Definitions
COVID-19 case patient with a positive real-time RT-PCR test, carried out with a sample collected by nasopharyngeal swab.
Acute kidney injury: according to the KDIGO 2012 criteria: (1) increase in serum creatinine (SCr) ⩾0.3 mg/dL in 48 h or (2) increase in SCr ⩾50% to the reference SCr, in the 7 previous days, or (3) urine output <0.5 mL/kg/hour for at least 6 h or <400 mL/day. In this study, we prioritized the diagnosis and classification of AKI based on changes in serum creatinine to the baseline creatinine at admission due to the difficulty in controlling urine volume/weight/hour. 13
Bioethical aspects
Data collection began after authorization from the Research Ethics Board and was registered under nº 34578120.0.0000.5432. Because this is research with routine clinical, observational, and retrospective data, patients were asked to waive the free and informed consent form. All data was stored without identification, on a secure data platform (REDCap) to avoid loss of data confidentiality.
Data collect
Data were collected from patients admitted to the hospital during 03/2020 and 07/2021, such as sex, age, underlying kidney disease, associated morbidities (diabetes mellitus, arterial hypertension, liver cirrhosis), and location of the cancer described in the medical records. electronics. The results of the laboratory tests included serum urea and creatinine, C-reactive protein, BNP, troponin d-dimer, pro-calcitonin, and urine.
About previous treatment, it was described whether they underwent at least one of the treatments used in cancer, grouped into treatments with chemotherapy, immunotherapy, combined therapy (CT and immunotherapy), radiotherapy, and surgery.
The outcomes considered were survival after ICU, hospital discharge with and without dialysis, and completion of dialysis.
Statistical analysis
Initially, a descriptive analysis of the variables was carried out, in which the absolute (n) and relative (%) frequency distributions for the qualitative variables were presented, and the main summary measures, such as the mean, standard deviation, median, minimum, and maximum values, for quantitative variables.
To evaluate the association between qualitative variables and AKI, the chi-square test or Fisher’s exact test was used, when appropriate. To compare the AKI with the distribution of quantitative variables, the student’s t-test for independent groups or the non-parametric Mann-Whitney test was used.
Logistic regression models were used to evaluate possible risk factors for AKI, in which the OR (Odds Ratio) values were evaluated. The significance level adopted is 5% and statistical analyses were carried out using SPSS version 20 software.
Results
Initially, 615 patients were admitted due to confirmed SARS-CoV2 infection in the period from 01/03/2020 to 07/31/2021 in a cancer treatment hospital in Sao Paulo, Brazil. The hospitalization period of the patients in this study occurred during the first and second waves of COVID-19 infection in Brazil.3 Of these patients, 158 were admitted to the ICU due to some clinical complication (25.6%) and 15 patients were removed according to the exclusion criteria of this study, as shown in Figure 1.
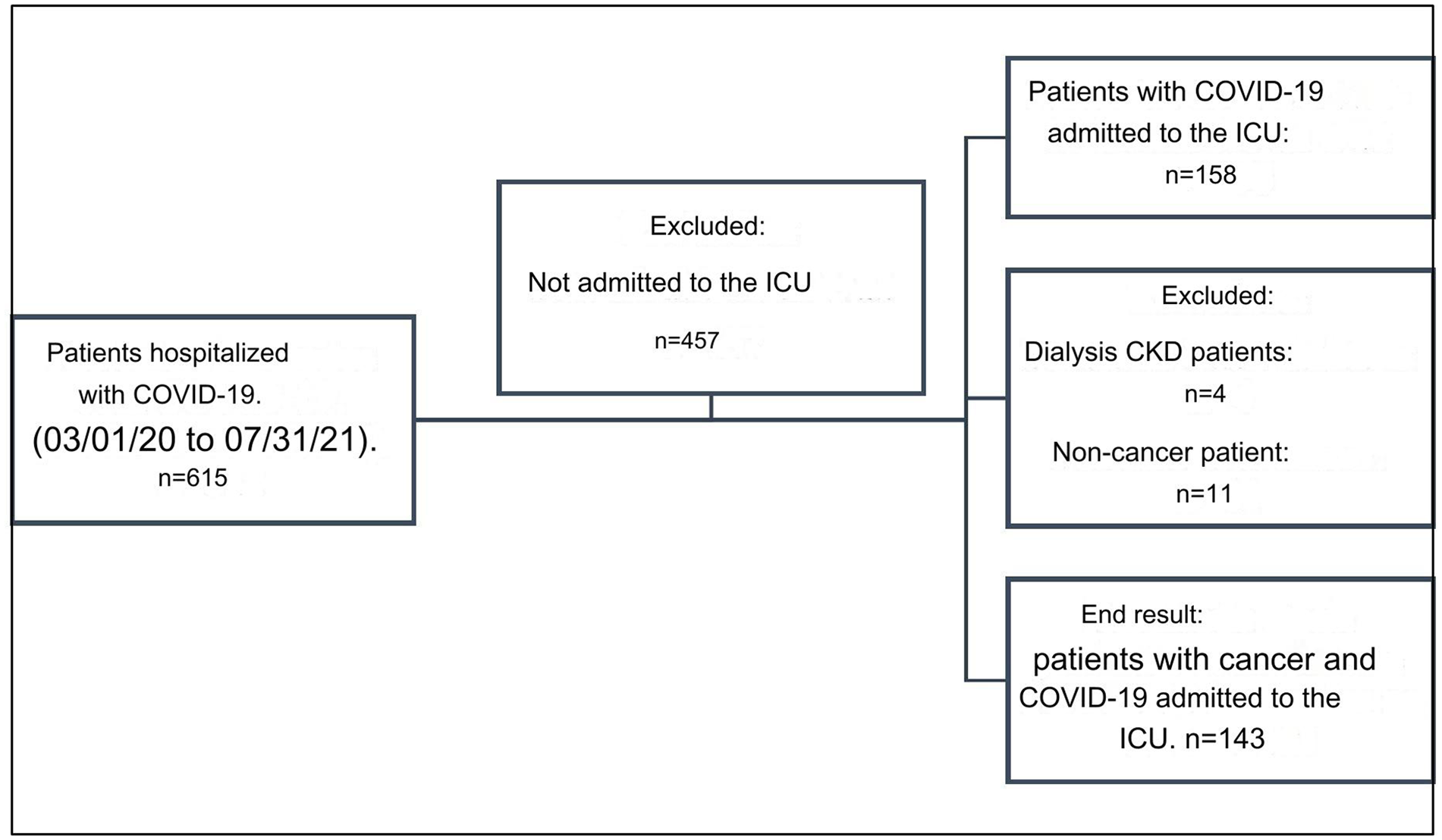
Flowchart of the selection and inclusion process of patients with cancer and COVID-19.
Clinical and laboratory characteristics of the patients studied
Among the 143 cancer patients admitted to the ICU, 59.4% were men, aged 65.5 ± 12.8 years, with 81.1% having one solid tumor and 25.2% hematological. The most frequent symptoms reported by patients in the initial assessment were dyspnea (62.2%), cough (54.5%), fever (52.4%), and myalgia (24.5%). The most frequent indication for ICU admission in this population was the clinical complication of acute respiratory failure (ARF)/COVID-19 in 79.7% of cases, followed by sepsis (7.7%), immediate postoperative period (2.8%), and decompensation of heart disease (1.4%).
The most frequent anatomical locations of cancer were prostate (19.8%), breast 16.4%, colon/rectum (14.7%), lower respiratory tract cancer (9.5%), and gynecological system (6.9%), urinary tract (6.0%), head and neck (5.2%), pancreas (3.4%), stomach (3.4%), central nervous system (2.6%), liver (2.6%), non-melanoma skin (1.7%), and others (4.3%).
Regarding previous cancer treatment: 73.4% underwent chemotherapy, 58% surgery, 29.4% radiotherapy, and 8.4% immunotherapy.
Incidence and clinical evolution of AKI
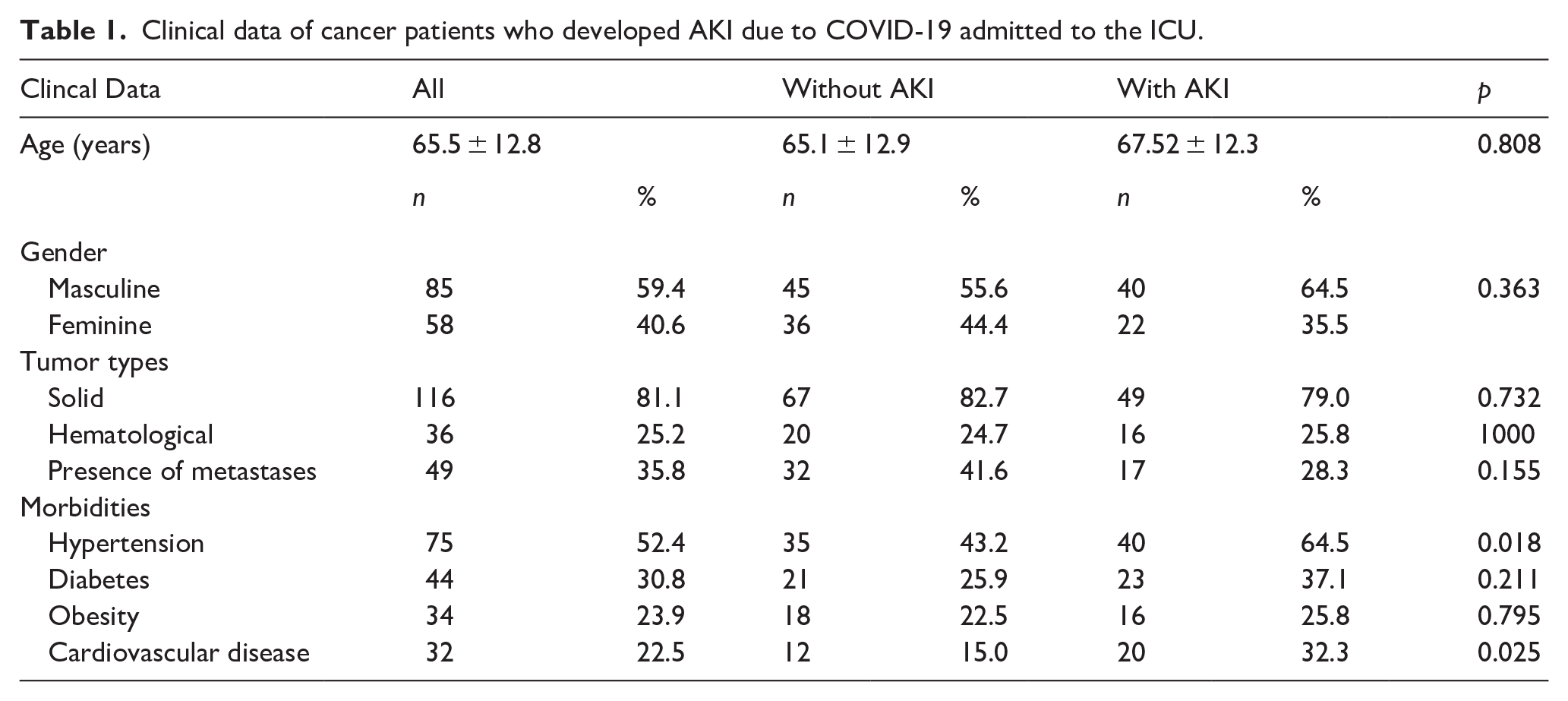
During evolution, 43.3% (n = 62) AKI. When we categorized the severity of patients’ AKI using the KDIGO criteria, we observed that the presence of patients with AKI in KDIGO 3 was more frequent in 87% of cases (n = 54), of which 62.5% (n = 10) used the continuous method and 37.5% (n = 6) SLED (Sustained Low-Efficiency Dialysis). The most common associated morbidities were arterial hypertension (52.4%), diabetes mellitus (30.8%), obesity (23.9%), and heart disease (22.5%). Of these morbidities, arterial hypertension was more common among patients who developed AKI (64.5% vs 43. 2% without AKI, p = 0.018).
Regarding laboratory data from the entire group with and without AKI, patients were hospitalized with an average serum creatinine (SCr) of 1.11 ± 0.55 mg/dL, reaching the highest serum level of 2.19 ± 1.63 mg/dL. Others verified the presence of leukocytosis 17,040 ± 8664 mm3 and elevated d-dimer 16,143 ± 6,922 ng/mL.
Regarding the most frequent associated morbidities of patients who developed AKI, it is noted that 64.5% were hypertensive and 37.1% diabetic (Table 1).
Clinical data of cancer patients who developed AKI due to COVID-19 admitted to the ICU.
Patients who developed AKI had higher leukocytes, troponin, CRP, pro-calcitonin, and d-dimer levels than patients without AKI (Table 2).
Laboratory data from cancer patients who developed AKI were admitted to the ICU.

It is observed in Table 3 that among the 105 patients who underwent Qt, the development of AKI was more frequent during COVID-19 infection in the ICU. Likewise, patients who used ARBs had more AKI (43.1%). More AKI was also observed among patients who used antibiotics/antifungals, such as meropenem, polymyxin B, and micafungin.
Treatment data of cancer patients who developed AKI admitted to the ICU.

It can be seen in Table 3 that patients with AKI used more indwelling urinary catheters (81.7%) and had more hematuria (42.3%) and leukocyturia (53.2%).
Characteristics of ICU treatment offered to patients with COVID-19
Also, patients who developed AKI used more mechanical ventilation (71.7%), as well as needed to be treated with the prone position (18%) when compared to those who did not have AKI during COVID-19 infection, p < 0.001 and p = 0.059 respectively.
Patients who used norepinephrine developed more AKI, 75.8% (n = 47), with p < 0.001.
When we evaluated the ICU outcome, the mortality of patients who developed AKI, 63.9% (n = 39) died versus 28.4% (n = 23) of patients without AKI (p < 0.001). In hospital outcome, 72.6% (n = 45) of patients with AKI died versus 39.5% (n = 32) of those who did not have AKI (p < 0.001), Table 4.
Mortality data on cancer patients who developed AKI admitted to the ICU.
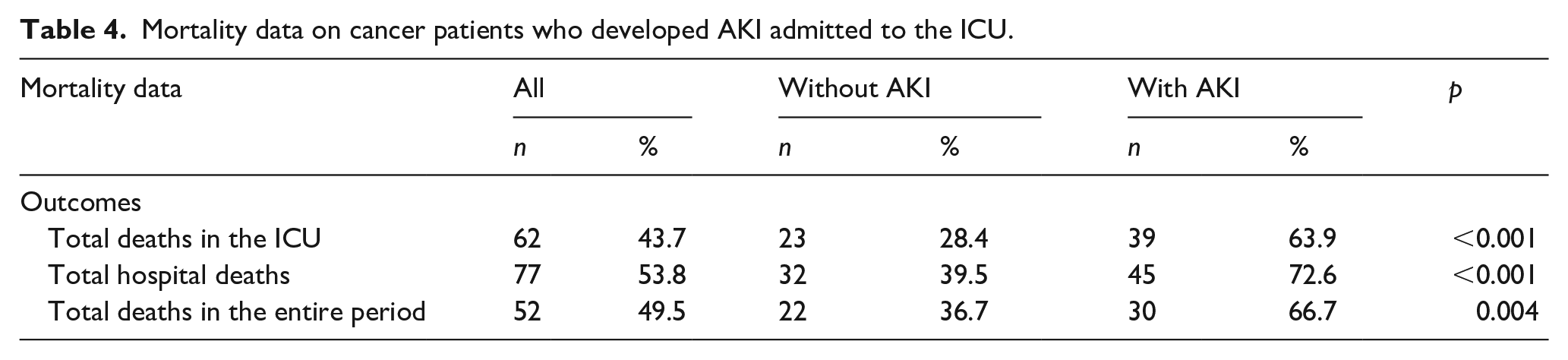
Of the 81 patients who were discharged from the ICU, 18.5% (n = 15) patients died in the ward, of which 40% had AKI (n = 6).
Logistic regression of the variables to measure the independent risks of the AKI
In the logistic regression to measure the risks of death (outcome) ICU and hospital, a risk of death in the ICU was observed with OR = 4.47 (95% CI 2.19–9.10) and in the hospital OR = 4.05 (95% CI 1.98–8.27).
In Table 5, we use logistic regression of the variables to measure the independent risks of the AKI event occurring, with the risk being higher in patients aged >60 years, with hypertension, cardiovascular disease, who had previous treatment with chemotherapy, use of ACE inhibitors/ARBs, used indwelling urinary catheter, developed hematuria, leukocyturia, underwent IMV, required the prone position and used vasoactive drugs.
Logistic regression of risk factors for AKI in patients with cancer and COVID-19 in the ICU.

Patient outcomes 1 year after COVID-19 infection
After 12 months of hospitalization, 66 patients were discharged from the hospital. Among them, we were able to identify that 66.6% (n = 44) of the patients had continuous monitoring in the hospital. Out of these, 84% (n = 37) did not have AKI, and 16% (n = 7) had AKI during their hospitalization for COVID-19 in the ICU (Intensive Care Unit). It was found that the SCr (Serum Creatinine) value 12 months after admission to the ICU was 1.32 ± 0.39 mg/dL for patients who had AKI and 1.11 ± 0.69 mg/dL for those who did not have AKI. However, it was not possible to verify the 1-year progression of the patients who were discharged from dialysis due to the loss of follow-up of these patients.
Discussion
The data presented in this study show patients admitted to the ICU during the hospitalization period coinciding with the first and second waves of COVID-19 infection in Brazil in the years 03/2020 and 07/2021, consisting mainly of male adults, aged 65.5 years, which consistent with other studies carried out, such as in the United Kingdom in 2020 where 56.9% were male and an average age of 70 years among hospitalized patients with cancer and COVID-19 in 61 hospital centers.12,14 In Brazil, a university hospital in the city of Sao Paulo analyzed 347 patients admitted with COVID-19 without cancer in 2020, 57.6% of whom were male with an average age of 59.8 years. 15 However, unlike the findings, the female sex was prevalent in 60.8% of a cohort of 181 patients with cancer and COVID-19 admitted to the National Cancer Institute. 16 The reasons why males are more affected by more severe forms are not so clear. One of the reasons would be the greater exposure to contagion in the first waves when there was still no vaccination for all groups. The older age group had a greater frequency in studies, as groups with a lower response to infection had been considered.
The most common characteristic symptoms at hospital admission were dyspnea, cough, fever, and myalgia. These symptoms have been reported in research since the beginning of the pandemic in China in 2020 in patients with cancer and COVID-19. 1 Another study in New York City in 2020, with 423 cases of cancer and COVID-19, showed that the prevailing symptoms were cough 82%, followed by fever 78% and dyspnea 44%. 17
Among the total number of patients hospitalized for COVID-19 in this period, it was observed that 25.6% needed ICU. The most frequent ICU admission diagnoses were: ARF/COVID-19, followed by sepsis, post-operative, and heart disease, in agreement with the reports found in other cases that already demonstrated the impact of severe acute respiratory syndrome on these patients. In our study, AKI was more frequent, with 43.3% of patients developing AKI, while de Melo et al. 16 had acute kidney injury in 18.2%, with 10.5% requiring support dialysis.
Regarding the most prevalent types of neoplasms in this study, prostate, followed by breast, and colon/rectum, possibly related to the prevalence of the most common types of cancer in Brazil. 18 The report from the National Cancer Institute of Brazil in 2020 with 181 patients reported solid tumors, the most frequent being: breast 22.1%, gastrointestinal 13.3%, and gynecological 12.2%. 16 A study with 928 cancer patients from the United States of America, Canada, and Spain in 2020, showed the most prevalent malignancies in the breast 21%, and prostate 16%. 10 In studies that evaluated cancer patients infected with SARS-COV 2, similar prevalences of these types of cancer were observed. 16
We found in this study that 81.1% had a solid tumor and 35.8% had metastases. de Melo et al. 16 also showed parallel data regarding tumors with 181 patients with COVID-19, 81.2% solid tumors and 18.8% hematological malignancies, of which 49.7% presented metastases. Patients with hematological cancer, lung cancer, or metastatic cancer (stage IV) had the highest frequency of serious events and a relatively high mortality rate 33.3%, high ICU admission rate 44.4%, high risk of serious symptoms/critical 66.6% and a high chance of using invasive mechanical ventilation in 22.2%. 1
The most prevalent morbidities in this study were hypertension, diabetes, obesity, and cardiovascular diseases. In the logistic regression of the variables, both hypertension and cardiovascular disease were factors associated with AKI and mortality. Published studies also associate these morbidities with adverse outcomes and mortality. Kidney disease is an important complication of COVID-19 and a significant risk factor for death, especially if associated morbidities like these are present.15,17,19,20 The explanations for why these morbidities are closely associated with AKI may be linked to pathologies that are very prevalent in the population and a higher-risk age group as well. 21
Of this population, 34.6% used some immunosuppressant in less than 30 days. Consistent with a multicenter study carried out in the city of Wuhan, China in 2020, with patients with cancer and COVID-19, whose most frequent therapy was chemotherapy 16.19%, and less immunotherapy 5.71%. 21 Regarding the type of QT or immunotherapy, as there was a great variability of drugs and associated therapeutic regimens, it was not possible to distinguish an association from a specific therapeutic agent.
The percentage of categorization of patients who presented AKI by the KDIGO 3 guidelines was very high, even higher than the data found in a study at the Brazilian university hospital in Sao Paulo 2020 that showed KDIGO stage 3 AKI was more frequent (53.4%). 15 One reason for this may be related to the fact that our study focused on evaluating only patients with COVID-19 who were referred to the ICU and who were therefore more seriously ill. 22
The risk factors most associated with AKI in patients with COVID and cancer admitted to the ICU were advanced age, morbidities such as hypertension and cardiovascular disease, using medications such as ACE inhibitors and ARB, mechanical ventilation treatment, prone, and use of vasoactive drugs. A similar study has demonstrated a strong association between AKI and advanced age, proteinuria, mechanical ventilation, and vasoactive drugs. 15 The presence of the use of ACE inhibitors or ARBs was a finding that can be explained by the higher incidence of hypertension and, as they are first-line treatment medications, they had a higher incidence linked to the risk of ARD. Other studies have shown that older patients have a high incidence of COVID-19 and associated mortality. 22
The presence of hematuria, leukocyturia, and the use of indwelling urinary catheters are associated with AKI and mortality. The explanations may be more related to the mechanical presence of indwelling urinary catheters than urinary changes secondary to COVID-19, although some studies have verified the presence of glomerulitis, or interstitial nephritis associated with SARS-COV-2. In our study, it would not be possible to evaluate this component accurately, as it is a retrospective study and did not include patients undergoing extensive investigation with confirmation by renal biopsy, as demonstrated in the study that verified renal abnormalities in 26 autopsies of patients with COVID-19.23,24
Among those patients who underwent RRT, seven patients (43.8%) were discharged on dialysis. Furthermore, complete recovery is not always achieved, which increases the risk of developing CKD. CKD is a common complication that occurs in 50%–70% of ICU patients and is associated with a worse clinical outcome with mortality rates of almost 50%. 25
Regarding long-term evolution, with the analysis over 12 months, we were able to contact and evaluate 44 patients who were being monitored in the hospital and observed that they had a higher mean SCR value in those who presented AKI than those who did not present AKI upon admission. This suggests that recovery was not complete or maintained some long-term loss, as observed in several studies linked to the evolution of AKI to CKD. 26 Monitoring these patients who develop AKI during hospitalization to check or even perhaps intervene in the evolution of renal dysfunction after hospital discharge is something that still needs to be encouraged in this and other causes of AKI.
We acknowledge that this study has certain limitations. Since it was retrospective, it was not possible to evaluate all the data that could help determine the progression of patients who experienced AKI complications. For instance, we could not identify which chemotherapy and immunotherapy drugs were most frequently used in different combined regimens and treatment lines or assess the severity scores of hospitalized patients. Additionally, we were unable to obtain more information about the long-term evolution of patients beyond 12 months, since 66.6% of those who were discharged from the hospital were lost to follow-up. It was found that the severity of patients in the ICU was very high, and advanced life support was required, leading to a high mortality rate and incidence of AKI with KDIGO 3. We add that in our study there are also other limitations such as cystatin C data, renal biopsies were not performed, and we were unable to establish causality with a retrospective design.
In summary, this study has revealed that older patients with hypertension or some form of cardiovascular disease who were being treated for cancer were more likely to develop AKI during their COVID-19 infection. This was observed regardless of the specific type of cancer, cancer treatment, or presence of metastases, and is consistent with earlier studies that have also reported a high incidence of AKI in ICU patients. Most AKI cases were classified as KDIGO 3, indicating severe AKI. This was particularly correlated with the need for mechanical ventilation, vasopressors, and pronation. The presence of indwelling urinary catheters in most patients made it difficult to accurately correlate urinary changes such as proteinuria and hematuria with the development of AKI. Mortality rates were high among COVID-19 patients who developed AKI, even after being discharged. After 12 months of hospitalization, those who had developed AKI still had higher creatinine levels compared to those who did not have AKI.
Footnotes
Acknowledgements
We would like to acknowledge the statistical and technical support provided by the Antônio Prudente Foundation Postgraduate group, particularly Barbara Beltrame Bettim and Dr. Antônio Paulo Nassar.
Data availability
Yes.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations (include full name of committee approving the research and if available mention reference number of that approval)
FUNDACAO ANTONIO PRUDENTE. No: 34578120.0.0000.5432.
Ethical approval
This study was approved by Fundacao Antonio Prudente Ethics Committee (approval no 34578120.0.0000.5432). All ethical measures were taken, and the collection of the data presented was initiated only after approval by the Research Ethics Committee of this institution.
Consent to participate
NA.
Consent for publication
Yes.
Trial registration
NA.
Guarantor
B.J.P.
Contributorship
Joubert Araújo Alves was involved in this study’s conceptualization, methodology, and use of the software. Germana Alves de Brito, Alexandre Ricardo da Silva Fernandes, Elaine Alexandre Gomes, Aline Lourenço Baptista, Luis André Silvestre Andrade and helped write the manuscript; Marina Harume Imanishe supervised this study; and Benedito Jorge Pereira participated in writing, reviewing, and editing the manuscript.