
Abstract
Fibrolamellar hepatocellular carcinoma (FL-HCC) is a rare liver cancer variant, accounting for less than 1% of primary hepatic malignancies, predominantly affecting young adults. This case report presents a 24-year-old patient with altered mental status, ultimately diagnosed with metastatic FL-HCC and secondary hyperammonemic encephalopathy, a rare but critical complication. Management involved continuous renal replacement therapy (CRRT), ammonia-scavenging agents, and targeted radiotherapy for the primary tumor. This report elucidates the clinical presentation of FL-HCC, explores the pathophysiology of hyperammonemia-induced encephalopathy, and discusses management strategies, emphasizing the therapeutic role of dialysis modalities.
Keywords
Introduction
Liver cancer is the sixth most prevalent cancer globally, accounting for 7% of all cancer diagnoses. 1 Hepatocellular carcinoma constitutes over 90% of primary liver cancers. 2 Fibrolamellar hepatocellular carcinoma (FL-HCC) is a rare and distinct subtype, comprising 1%–5% of all hepatocellular carcinomas. 3 Unlike conventional hepatocellular carcinoma, FL-HCC typically occurs in individuals without pre-existing liver disease or cirrhosis and predominantly affects adolescents and young adults, with over 60% of cases diagnosed before the age of 40 years. 4
The etiology of FL-HCC is not fully understood. Tumor cells exhibit markers of both hepatocyte and biliary differentiation. Although not specific, the recurrent DNAJB1-PRKACA fusion gene, resulting from a unique deletion on chromosome 19, is identified in most cases through molecular diagnostics. 5
Diagnosis is usually based on clinical presentation and imaging studies, which reveal a large, sharply defined, heterogeneously enhancing mass in a noncirrhotic liver. The tumor marker alpha-fetoprotein (AFP) is typically normal. Pathology remains the gold standard for diagnosis. 6 Abdominal pain is mostly the presenting symptoms and followed by abdominal distention or mas. Jaundice is also frequently observed, and 60% of patients present with extrahepatic metastases. 7
Surgical resection is the only curative treatment for resectable fibrolamellar carcinoma. Despite the use of various chemotherapeutic agents, there is no consensus on the optimal regimen for unresectable disease, and FL-HCC often resists systemic chemotherapy. Radiotherapy has been used to reduce tumor size, with varying success.2,8
Fibrolamellar hepatocellular carcinoma can induce hyperammonemia through diverse mechanisms, as detailed in subsequent sections. Although hyperammonemic encephalopathy is documented in the literature, this case report is among the few that elucidate the use of renal replacement therapy as a treatment strategy for hyperammonemia associated with FL-HCC.
Case presentation
A 25-year-old male with no significant medical history presented to urgent care with symptoms of cough and abdominal distension. Initial investigations included a chest X-ray revealing pulmonary nodules and a computed tomography (CT) scan of the abdomen and pelvis, which identified a large mass in the right liver lobe. He was urgently referred to hepatology and pulmonology clinics for further evaluation.
The patient returned with progressive abdominal pain. A repeat chest CT with contrast demonstrated heterogeneous masses in the right liver lobe and bilateral pulmonary nodules, raising suspicion for malignancy (Figure 1(a)). While awaiting clinic appointments, a magnetic resonance imaging (MRI) of the liver was performed, revealing a large 19.5 cm malignant mass with a tumor thrombus extending into the inferior vena cava (Figure 1(b)). A positron emission tomography (PET) CT was also obtained, which later showed a hypermetabolic lesion in the right hepatic lobe (Figure 1(c)).
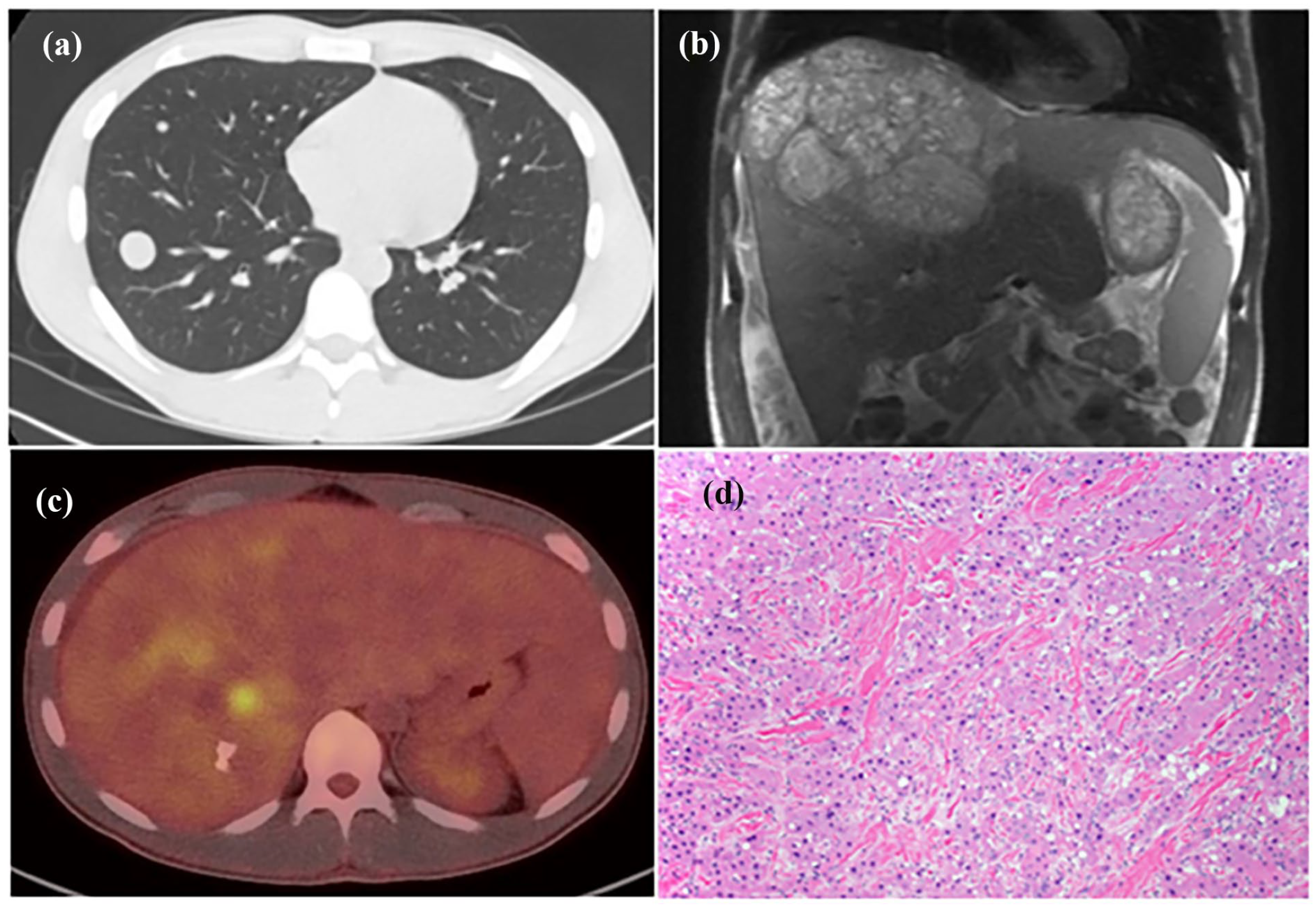
(a) Lung nodules on CT scan concerning metastasis, (b) characteristic heterogeneous, well-defined mass with a lobulated outline on T2 MRI, (c) PET-CT scan demonstrating diffuse uptake of radioactive tracer in the liver, and (d) histologic demonstration of FLHC with neoplastic cells with abundant cytoplasm in a background of dense collagen bundles arranged in parallel lamellae (Gonzalez and Graham, 2021). 9
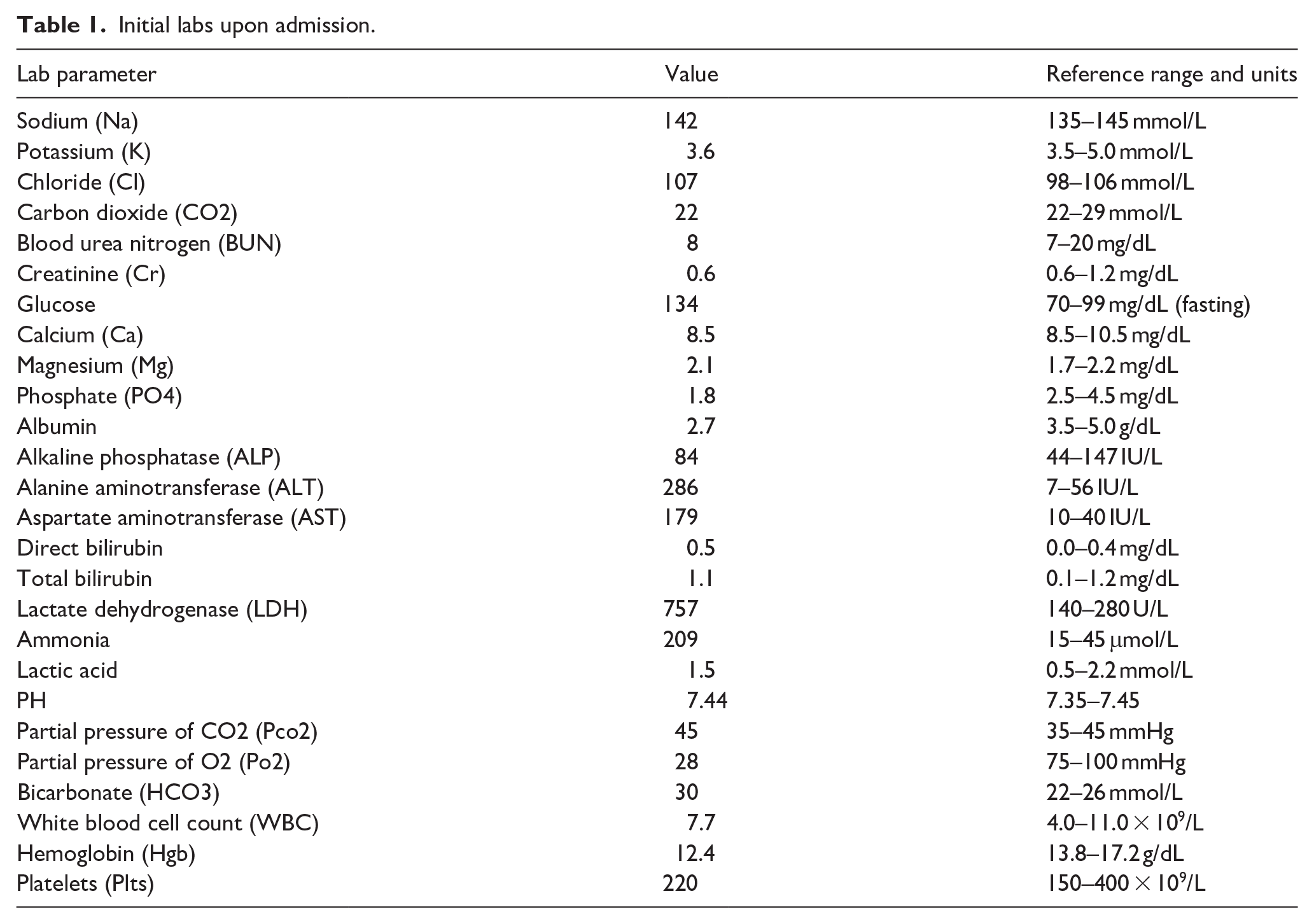
He was subsequently brought to the emergency department by his family due to worsening altered mentation. On examination, the patient was somnolent and disoriented, with a distended abdomen and positive asterixis. Laboratory investigations showed ammonia levels exceeding 200 micromoles per liter (μmol/L; see Table 1 for full lab results).
Initial labs upon admission.
He was admitted to the ICU, and treatment was initiated with rifaximin and lactulose for suspected hepatic encephalopathy. Diagnosis was confirmed by inpatient liver biopsy, with fluorescence in situ hybridization (FISH) testing positive for PRKACA/DNAJB1 fusion protein rearrangement, consistent with the fibrolamellar variant (Figure 1(d)).
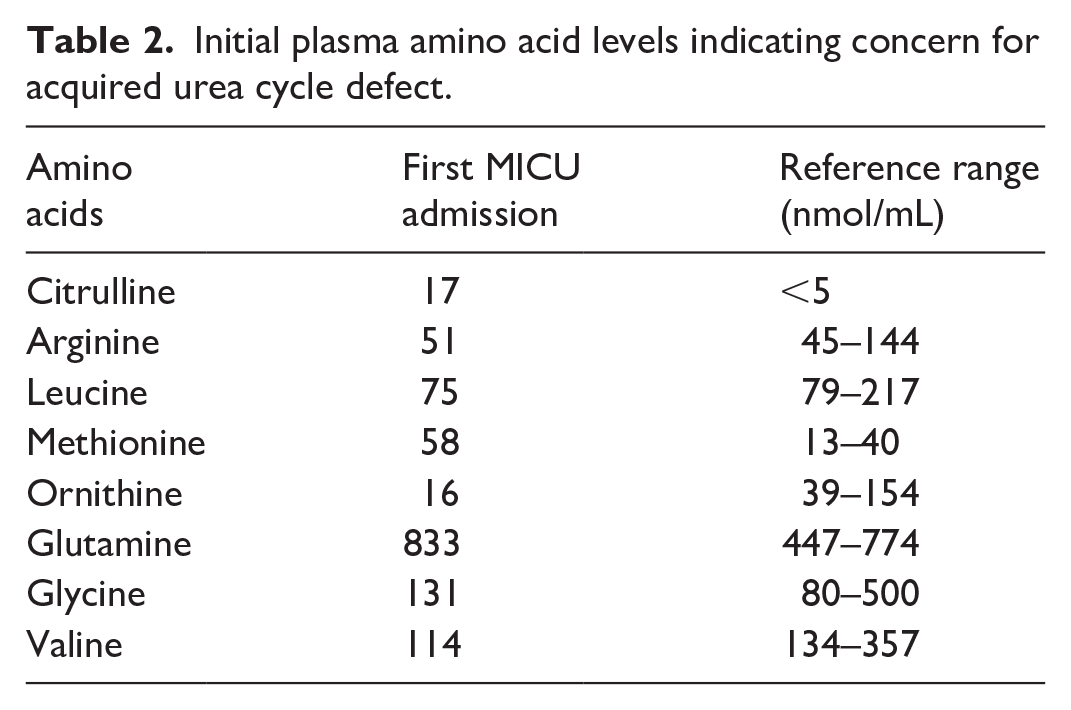
Quantitative amino acid analysis indicated low citrulline (17 nmol/mL), ornithine (16 nmol/mL), and borderline arginine (51 nmol/mL); urine orotic acid was not assessed (see Table 2 for full analysis).
Initial plasma amino acid levels indicating concern for acquired urea cycle defect.
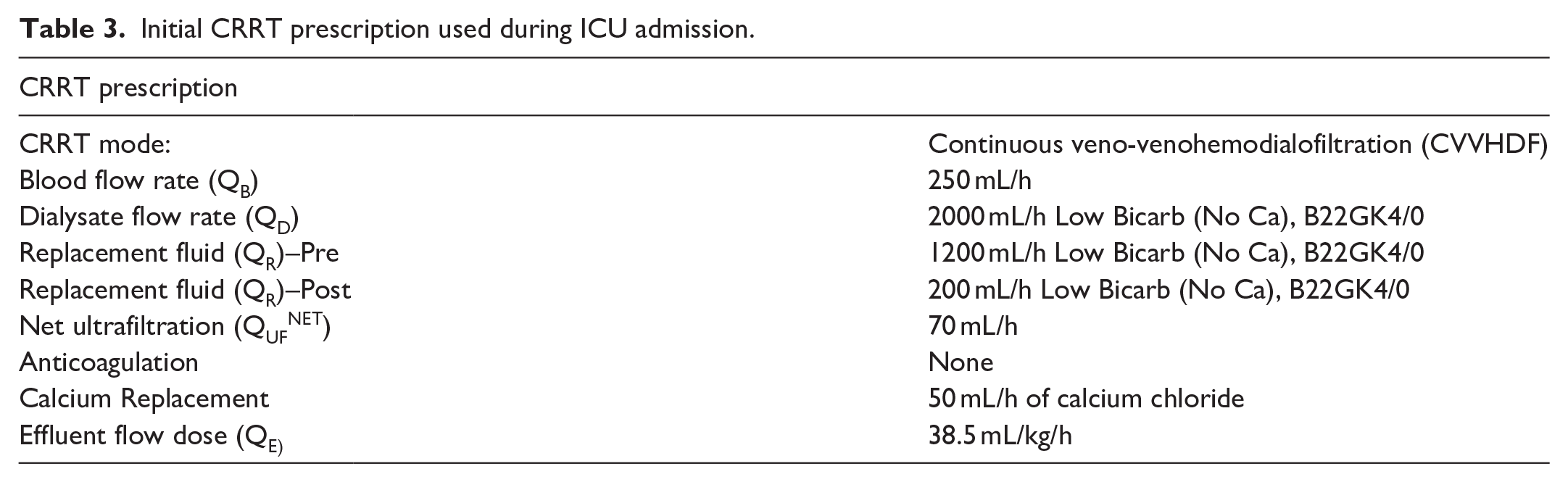
A CT scan showed no signs of cerebral edema or other pathologies. Due to the worsening mental status and concerns of acquired hyperammonemic encephalopathy secondary to fibrolamellar hepatocellular carcinoma (FL-HCC), treatment with intravenous arginine, oral citrulline, and intravenous dextrose was initiated to reduce gluconeogenesis and ammonia production. Additionally, intravenous ammonia scavenging therapy with sodium phenylacetate, and sodium benzoate was administered. Given the high initial ammonia levels (>200 μmol/L) and the patient’s comatose status, the decision was made to start continuous renal replacement therapy (CRRT) to clear excessive ammonia. CRRT was chosen over intermittent hemodialysis due to vasodilatory shock and norepinephrine requirement. Concurrently, the patient received 5 days of radiotherapy for the liver mass as initial debulking therapy.
The CRRT modality employed was continuous venovenous hemodiafiltration (CVVHDF) with high effluent dose (see full prescription in Table 3). Mental status improved as ammonia levels decreased over 3 days. He was extubated and returned to near-baseline mentation. CRRT was discontinued, and he was treated with intravenous diuretics and albumin for generalized edema due to hypoalbuminemia. He was transferred to the medical floor after stabilization.
Initial CRRT prescription used during ICU admission.
Regrettably, his condition deteriorated again within 72 h, with worsening somnolence and rising ammonia levels, necessitating readmission to the medical intensive care unit. He was intubated, and CRRT was restarted after about a week of discontinuation. A trial of single-pass albumin dialysis (SPAD) was conducted to enhance ammonia clearance. Despite maximal treatment measures, including CRRT and ammonia scavenger therapies, fluctuating mentation and ammonia levels persisted. Gemcitabine-Oxaliplatin (GemOx) chemotherapy was initiated 2 days after restarting CRRT (see changes in ammonia levels in Chart 1).
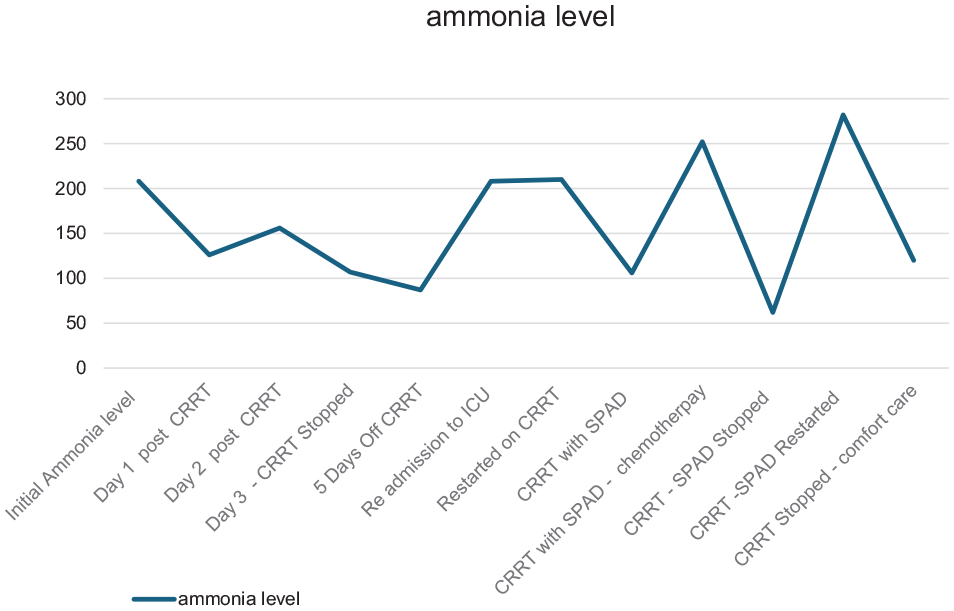
Interval changes in ammonia levels throughout hospitalization.
Despite ongoing CRRT and SPAD trials, the patient’s neurological status remained poor. Electroencephalogram (EEG) findings suggested non-convulsive status epilepticus, and there was concern for sepsis, which led to the initiation of broad-spectrum antibiotics. Blood cultures confirmed the presence of Haemophilus influenzae. The hospital course was further complicated by a pulmonary embolism, for which anticoagulation was started but later held due to heparin-induced thrombocytopenia (HIT) and thrombocytopenia. A suspected basilar artery occlusion could not be confirmed due to the patient’s unstable condition, raising concerns about a new-onset stroke contributing to his altered mentation. Following multidisciplinary discussions, the family opted for comfort care. The patient was compassionately extubated and passed away shortly thereafter.
Discussion
Hyperammonemia-induced encephalopathy results from the toxic accumulation of ammonia, which crosses the blood-brain barrier at high levels and conjugates with glutamate to form glutamine. 4 Glutamine can increase osmotic pressure in the brain, causing water to accumulate in the extracellular cerebral compartment. Additionally, glutamine can be recycled back to ammonia in the mitochondria, leading to mitochondrial dysfunction. This dysfunction can cause the release of free radicals, resulting in astrocytic swelling and brain edema. 10 Such pathophysiology leads to a wide range of symptoms, from subtle cognitive impairments like decreased attention, reaction time, and memory, to severe manifestations including somnolence, confusion, and unconsciousness. 11
Common etiologies of hyperammonemia include acute liver failure and urea cycle defects. Several drugs, including chemotherapeutic agents such as 5-fluorouracil, gemcitabine, cytarabine, cyclophosphamide, oxaliplatin, vincristine, etoposide, methotrexate, topotecan, and tyrosine kinase inhibitors, have also been implicated. 4 The association with fibrolamellar hepatocellular carcinoma (FL-HCC) is exceptionally rare and was first documented in 2009. 12
Several mechanisms have been proposed for hyperammonemic encephalopathy in FL-HCC patients. These include intrahepatic shunting of ammonia away from cancer cells, leading to elevated serum ammonia levels; chemotherapy-induced cell breakdown, which increases the nitrogen load and overwhelms the liver’s clearance capacity13,14; increased arginine utilization by cancer cells and decreased expression of the ornithine transcarbamylase gene due to the indirect action of the fusion protein DNAJB1-PRKACA, which leads to overexpression of c-Myc and upregulation of ornithine decarboxylase, causing a shift of ornithine from the urea cycle and subsequent decreased ammonia clearance 15 ; and a paraneoplastic process that disrupts the urea cycle, further increasing ammonia levels. 16
Diagnosis of urea cycle disorders involves measuring plasma ammonia levels, which usually begin to cause neurological symptoms at levels above 150 μmol/L, followed by comprehensive diagnostics such as blood gas analysis and specific assays for plasma amino acids, urine organic acids, and orotic acid. 17 Individuals with decreased ornithine transcarbamylase activity tend to have low citrulline and high glutamine levels in the blood, along with elevated orotic acid levels in the urine.4,14 Liver biopsy reveals a distinctive molecular profile with a focal deletion on chromosome 19 that encodes the functional transcript DNAJB1-PRKACA, found in 80% of fibrolamellar hepatocellular carcinoma cases. 2
Management focuses on treating acute episodes and preventing further attacks. The cornerstones of treatment are reducing nitrogen load, eliminating excess ammonia, and addressing precipitating factors. 2 Prompt intervention is crucial to prevent irreversible neurological damage. Strategies include adequate hydration using dextrose solutions and intralipids while maintaining low protein intake (approximately 60 g/day), and starting intravenous ammonia scavengers such as sodium benzoate and phenylacetate for ammonia levels above 100 μmol/L. 2 Amino acids, including intravenous arginine to generate urea cycle intermediates and oral citrulline if low levels are observed in labs, are also used.4,18
Renal replacement therapy (RRT) is crucial in managing severe hyperammonemia that is unresponsive to conventional treatments. Due to the rarity of this condition, there is no clear consensus on the precise indications and timing for initiating RRT. Nonetheless, it has been suggested that RRT should be considered when blood ammonia levels are three times above the upper limit of normal or when the patient exhibits severe encephalopathy. 19
Ammonia has low molecular weight and minimal protein binding. Efficiency of ammonia clearance during RRT is influenced by factors such as blood flow rate (Qb), dialysate flow rate (Qd), and the surface area of the dialyzer membrane. Intermittent hemodialysis (IHD) achieves higher clearance rates due to higher blood flow compared to continuous renal replacement therapy (CRRT). However, CRRT offers the advantage of fewer treatment interruptions and avoids the rapid fluid shifts associated with IHD, which can exacerbate cerebral edema. 20
Continuous renal replacement therapy is recommended following initial intermittent hemodialysis to prevent rebound hyperammonemia, given ammonia’s large volume of distribution. 21 Dialysis is typically discontinued once the patient’s mental status normalizes and ammonia levels stabilize, ideally below 150 μmol/L. However, if there is no improvement in mental status after 48–72 h of effective therapy, discontinuation is considered due to likely futility.22,23
Conclusions
This case emphasizes the critical aspects of diagnosing and managing fibrolamellar hepatocellular carcinoma (FL-HCC) complicated by hyperammonemic encephalopathy (HAE). Timely intervention is essential, as unchecked hyperammonemia may lead to cerebral edema and irreversible neurological injury. The primary management goal is rapid ammonia reduction through a combination of protein restriction, ammonia scavengers, and possibly renal replacement therapy (RRT). In this case, RRT played a pivotal role in metabolic stabilization; however, the patient’s clinical course was further complicated by superimposed sepsis and seizure activity, highlighting the multifactorial nature of deterioration and the importance of a coordinated, multidisciplinary approach to care.
Footnotes
Acknowledgements
None.
Data availability
Available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Verbal consent from patient’s wife.
Guarantor
Mohamed F Mudarres.
Trial registration
Not applicable.
Contributorship
Not applicable.