
Abstract
The unequal sharing of healthcare resources between different socioeconomic groups can lead to worsened health outcomes, financial strains for low-income individuals, and broader social and economic issues. While the link between healthcare service accessibility and socioeconomic factors has been widely explored, the spatiotemporal evidence based on government-funded and self-funded healthcare facilities remains limited. Focusing on public and private services is crucial for ensuring efficient and equitable healthcare for diverse social strata. Drawing on the representative travel data from the Travel Characteristics Survey (TCS), this study employed the enhanced two-step floating catchment area (E2SFCA) method and Gini index to assess the spatiotemporal patterns of healthcare accessibility and inequality in Hong Kong, including public hospitals, public general outpatient clinics, private hospitals, and private clinics. The geographically and temporally weighted regression (GTWR) model was used to unravel the spatiotemporal patterns of socioeconomic inequalities in healthcare accessibility. We found that (1) in high-complexity healthcare services (i.e., hospitals), accessibility to government-funded hospitals was higher than to self-funded ones, while in primary services (i.e., clinics), the opposite was true; (2) there was significant spatial autocorrelation in healthcare accessibility in Hong Kong, and the high-high and low-low clusters of high-complexity medical facilities shrunk over time; (3) in downtown areas, the positive correlation between median household income, the older population ratio, and healthcare accessibility shifted to negative, and the negative correlation between population density and healthcare accessibility strengthened. These findings may inform policymakers in implementing effective strategies for increasing the accessibility and equality of healthcare services.
Keywords
Introduction
Many countries are struggling with unequal distribution of healthcare services, notably evident during the outbreak of the COVID-19 pandemic. The less affluent people face a heightened risk of disease burden (Sabharwal et al., 2022), resulting in reduced workforce productivity and even heightened social and economic instability (Salisu et al., 2023). Evidence in developed countries, such as the United States and Australia, demonstrated that the unequal sharing of healthcare resources between the affluent and the less affluent groups may result in disparities in life expectancy (Atalay et al., 2023; Baker et al., 2017). Equality in accessing healthcare services refers to the level to which every person has an equal opportunity to access healthcare services, free from discrimination, socioeconomic status (SES), or geographic location (Donabedian, 2005). Studying the level of equality or inequality in healthcare service access can aid policymakers in formulating fair and effective strategies to improve the healthcare environment and benefit human well-being (Neutens, 2015). Moreover, an equitable healthcare environment significantly benefits marginalized and vulnerable groups, fostering social stability and environmental fairness (Zhao et al., 2020).
Accessibility refers to the ease with which an individual or a group can conveniently reach or obtain resources, which was first proposed in the 1960s (Hansen, 1959). Healthcare service accessibility, hence, refers to the convenience for a resident to access healthcare services. It includes factors such as geographic location, transportation availability, and population distribution. Many studies have proposed methods for evaluating healthcare service accessibility. For example, it can be assessed by the availability of healthcare services, including the number and density of healthcare facilities in different areas and the number of healthcare services per capita in each planning unit (Van Gaans and Dent, 2018). Areas with a higher density of healthcare services generally exhibited more medical resources (Mohan et al., 2019). However, residents always go across administrative boundaries to those hospitals or clinics, considering factors such as expenditure, transportation, level of medical service, familiarity, or service quality. Hence, it is vital to consider human travel behavior in assessing healthcare service accessibility. Researchers have recently developed more advanced methods to assess it, such as the two-step floating catchment area (2SFCA) (Luo and Wang, 2003), which was used to assess the accessibility to services or resources by considering both the supply of facilities and the demand of residents in a particular area. This method was more refined than assessing per capita resources, as it provided a more accurate analysis by considering spatial distance and transportation accessibility. An Enhanced 2SFCA (E2SFCA) was also proposed (Luo and Qi, 2009), which used a distance decay function to conceptualize travel cost by combining the two-step floating catchment area method with a gravity-based model (Zhao et al., 2020).
Spatial inequality of healthcare accessibility refers to the uneven distribution of healthcare service accessibility across different geographic areas or for different population groups. Rural and peripheral areas often experience lower healthcare accessibility compared to urban centers (Deborah et al., 2018). Higher-tier hospitals were more concentrated in urban areas and tended to exhibit greater inequality compared to the spatial distribution of primary healthcare facilities (Cheng et al., 2020). People of less influential communities tend to suffer from greater SES inequality in healthcare service accessibility. Many studies discussed the social and economic factors that affected the opportunity to access healthcare resources. For example, the cost of healthcare services and the financial burden of transportation significantly affected the opportunity to access healthcare resources for low-income people (Levesque et al., 2013). Evidence from Southern Brazil also demonstrated that low-income people usually had low opportunities to access healthcare services (Wendt et al., 2022). Residents from low-income areas experienced nearly double the travel time compared to those from high-income areas to access the nearest primary healthcare services in Beijing, China (Zhao et al., 2020). As healthcare service level improves, the inequality between low and high-income groups increases (Jin et al., 2022). In terms of methodology, the Gini coefficient was used to measure the degree of inequality distribution, with higher values indicating greater inequality. It has been widely used to assess geographic inequalities of healthcare accessibility between populations or areas and was considered to have strong interpretability and was easily understood by policymakers (Shinjo and Aramaki, 2012).
Even though many studies have investigated spatial and socioeconomic inequality in accessing healthcare resources, there are three major gaps to be filled. First, previous research overlooked the differences in healthcare accessibility between government-funded and self-funded facilities, focusing only on the disparities between primary care facilities and high-complexity medical facilities. For example, studies in China and Japan typically focused on public hospitals, categorizing them into primary, secondary, and tertiary facilities based on their medical capabilities (Hosokawa et al., 2020). Similarly, investigations in Brazil concentrated on primary and specialized healthcare centers (Akakba and Lahmar, 2023). However, in most regions and countries, private hospitals and private clinics offer self-funded services, running parallel to public healthcare services. Self-funded healthcare facilities supplement the high-level medical service that government-funded healthcare facilities cannot meet, primarily serving high-income groups. This complementarity is crucial for the allocation and optimization of healthcare resources in different socioeconomic groups. Second, urban transportation characteristics and residents’ travel habits vary across different regions. Similarly, the distances traveled to access various services differ among individuals. However, many studies neglected the varying travel distance to healthcare facilities among residents of different areas (Tomasiello et al., 2024). Such neglect will lead to a biased estimation of healthcare service accessibility. Third, few studies concerned with both the spatial and temporal heterogeneity of the relationship between healthcare service accessibility and socioeconomic factors. Regarding methodology, some studies used global regression models with the assumption of isotropic association between SES and healthcare accessibility, failing to reveal the local situation. Besides, most previous studies used cross-sectional data from a single year (Cheng et al., 2020; Jin et al., 2022; Zhao et al., 2020). While this approach can reveal healthcare accessibility at a specific point in time, it lacked stability over time and fails to comprehensively reflect the dynamic changes in healthcare resources. Studying longitudinal data enables the capture of sustainable trends between healthcare resource accessibility and income inequality, revealing potential fluctuating or stable patterns and assisting decision-makers in formulating future plans and policies to enhance the allocation of healthcare resources and promote fairness.
To fill the gaps, this study aims to (1) assess the spatiotemporal disparities in healthcare accessibility based on government-funded and self-funded healthcare facilities and realistic residents’ travel (HKTCS, 2011) data in Hong Kong; (2) evaluate the spatial inequality in the healthcare accessibility of Hong Kong eighteen districts across 10 years; (3) use the GTWR model to unravel the associations between SES factors and healthcare accessibility and their spatiotemporal heterogeneity. This study is novel and significant in two ways. First, this is among the first studies to assess healthcare accessibility using realistic travel data under the context of a government-funded and self-funded medical system in a major Asian metropolis with a highly developed healthcare system. Second, drawing on longitudinal data and the spatiotemporal analysis technique, our study provides valuable insights into the spatiotemporal associations between SES factors and healthcare accessibility over 10 years. Our study may inform the government to enhance the effective and equitable development of healthcare resources.
Methods
Study materials
This study was conducted in Hong Kong, a highly urbanized metropolis with 7.4 million residents in a total land area of 1102 km2 (Census & Statistics Department of Hong Kong, 2020). The territory is divided into three major regions: Hong Kong Island, Kowloon, and the New Territories. We chose Hong Kong as the study area because it boasts one of the highest life expectancy in the world. It has advanced health education, expert healthcare services, and a mature healthcare infrastructure. A total of five datasets were collected in this study (Table S1): planning units, healthcare services, the road network, the 2011 Travel Characteristics Survey (HKTCS, 2011), and SES.
Planning units
Small Tertiary Planning Unit Groups (STPUGs) were applied as units of analysis in this study. To calculate the healthcare service accessibility on multiple time scales, longitudinal data from 2012 to 2021 was utilized. It was worth noting that some STPUGs were integrated into others during the study period. We standardized the STPUGs boundaries to those of 2016 across the 7 years. The whole territory of Hong Kong was divided into 179 STPUGs in the 2016 Population By-census.
Healthcare services
The market shares of public and private healthcare services vary across countries and regions. For instance, the United States mainly relies on private hospitals and private clinics, while the United Kingdom and Hong Kong SAR, China, are mainly oriented towards public healthcare, with private healthcare holding a noteworthy market proportion. Healthcare services in Hong Kong are mainly divided into four sectors: public hospitals, public general outpatient clinics, private hospitals, and private clinics. Public hospitals and public general outpatient clinics provide government-funded medical services, which means it is almost free to the citizens. Private hospitals and private clinics are self-funded medical services. However, private healthcare services provide better care experiences than those public-funded. Furthermore, public hospitals and private hospitals provide high-complexity medical services, while public general outpatient clinics and private clinics provide primary healthcare services.
Travel and road network data
To accurately assess healthcare accessibility, we needed to understand the characteristics of residents’ travel patterns to healthcare services. The newest travel characteristic survey, Travel Characteristics Survey 2011, offered the best available dataset. HKTCS 2011, carried out in 2011, was used to investigate the travel characteristics of Hong Kong residents (Jiang et al., 2021). The survey, conducted through face-to-face interviews, documented participants’ travel records taken on the day before the survey, including travel characteristics, origin STPUGs, destination STPUGs, distance, time, and destination type. Travel records with healthcare services as the destination were selected and categorized based on service types. Existing studies have shown that 84.5% of individuals in Hong Kong opt for primary care when ill, while 15.5% utilize high-tier medical healthcare (Leung et al., 2005). This aligned closely with the findings of HKTCS 2011, affirming the accuracy of the dataset (18.3% vs 81.7%). Taking into account the variations in travel time caused by differences in transportation modes, we chose the median travel distance as the threshold for calculating E2SFCA (Table S2) (Cheng et al., 2020). This approach ensures consistency, as it includes all transportation modes, providing a more comprehensive measure. The specific distances for each healthcare facility are as follows: public hospital (d0 = 7.416 km), public general outpatient clinic (d0 = 6.339 km), private hospital (d0 = 9.846 km), and clinic (d0 = 6.676 km). The road networks from 2012 to 2021 were used to calculate the shortest path from trip origin to destination, respectively. Compared to straight-line distance, the road network can more accurately assess the actual accessibility to healthcare services.
Socioeconomic factors
We used the median household income of each STPUG for 2011, 2016, and 2021 to assess socioeconomic attributes, rather than housing prices, as it provides a more accurate measure. Besides, population density and the older population ratio of each STPUG for 2011, 2016, and 2021 were utilized to evaluate sociodemographic factors. These three variables were the most important factors for targeted policymaking. Linear interpolation was employed to estimate data for intervening years, aligning with the five-year demographic data cycle. Moreover, we controlled education level, sex ratio, labor force participantion rate, and average domestic household size in the model to generate more accurate results. The summary statistics of explanatory variables and control variables are presented in Table S3.
Accessibility assessment
The study employed the E2SFCA method to assess the accessibility to healthcare services of each STPUG. Compared to the original two-step floating catchment area (2SFCA) method proposed by Luo and Wang (2003), E2SFCA increased a Gaussian distance decay function to address the distance change sensitively (Luo and Qi, 2009). The catchment area of E2SFCA in our study was calculated by the HKTCS 2011. The calculation consisted of two steps. The first step was to identify the planning units within the catchment area of each healthcare service to acquire the supply-demand ratio (equation (1)). The second step was to assign healthcare services to the planning units by identifying the healthcare services within the catchment area of each planning unit and then summing up the supply-demand ratio computed in step 1 (equation (2)). A Gaussian function was included to gradually decrease accessibility based on distance decay (equation (3)).



To assess whether the characteristics of healthcare service accessibility are spatially clustered, Global Moran’s I was employed to uncover the spatial autocorrelation. Furthermore, Local indicators of spatial association (LISA) were used to examine whether the characteristics of healthcare service accessibility existed high-high clusters, high-low clusters, low-low clusters, and low-low clusters (Anselin, 1995).
Equality assessment
The Gini coefficient and the Lorenz curve were used to evaluate the equality of healthcare service accessibility (Ceriani and Verme, 2012). The Gini coefficient was defined as the ratio of the area between the diagonal and the Lorenz curve to the total area beneath the diagonal, ranging from 0 to 1. Zero represents perfect equality (i.e., everyone has the same income or wealth), and one represents perfect inequality (i.e., all income or wealth is concentrated in one person’s hands). A higher Gini coefficient indicates greater inequality. In this study, it was employed to assess the spatial equality of each STPUG to healthcare services accessibility (equation (4)). A bootstrap method was used to provide 95% confidence intervals (CI) for the Gini coefficient.

The GTWR model and the Mann-Kendall tests
Previous studies used traditional econometric regression models, such as multiple regression analysis (Shinjo and Aramaki, 2012), to evaluate the relationships between healthcare resources and SES variables. However, the model is suitable for scenarios where there are no spatial or temporal heterogeneity effects, as it only considers global relationships. Most geographical phenomena, including the distribution of healthcare facilities, are sensitive to spatial and temporal factors, and the regression coefficients vary with changes in space and time. The Geographically and temporally weighted regression (GTWR) model (Huang et al., 2010) combined the Geographically weighted regression (GWR) model and temporal weighting factors, allowing each sample to reflect dynamic relationships at different times and locations. Thus, this study employed the GTWR model to uncover the spatiotemporal relationships between multitier healthcare accessibility and SES (equation (5)).

To examine potential multicollinearity among the explanatory variables and control variables, the Variance Inflation Factor (VIF) was employed, with all variables exhibiting a VIF value below 4, indicating there is no multicollinearity among variables. To assess whether the coefficients representing the relationship between healthcare accessibility and SES, as estimated by the GTWR model, exhibit statistically significant temporal trends, we conducted the Mann-Kendall test (Kendall, 1948; Mann, 1945). This non-parametric method was widely applied in trend analysis across various fields, including urban studies (Sk et al., 2025). A p-value less than 0.05 indicates statistical significance. The overall workflow of this study is presented in Figure 1. The overall workflow of the research.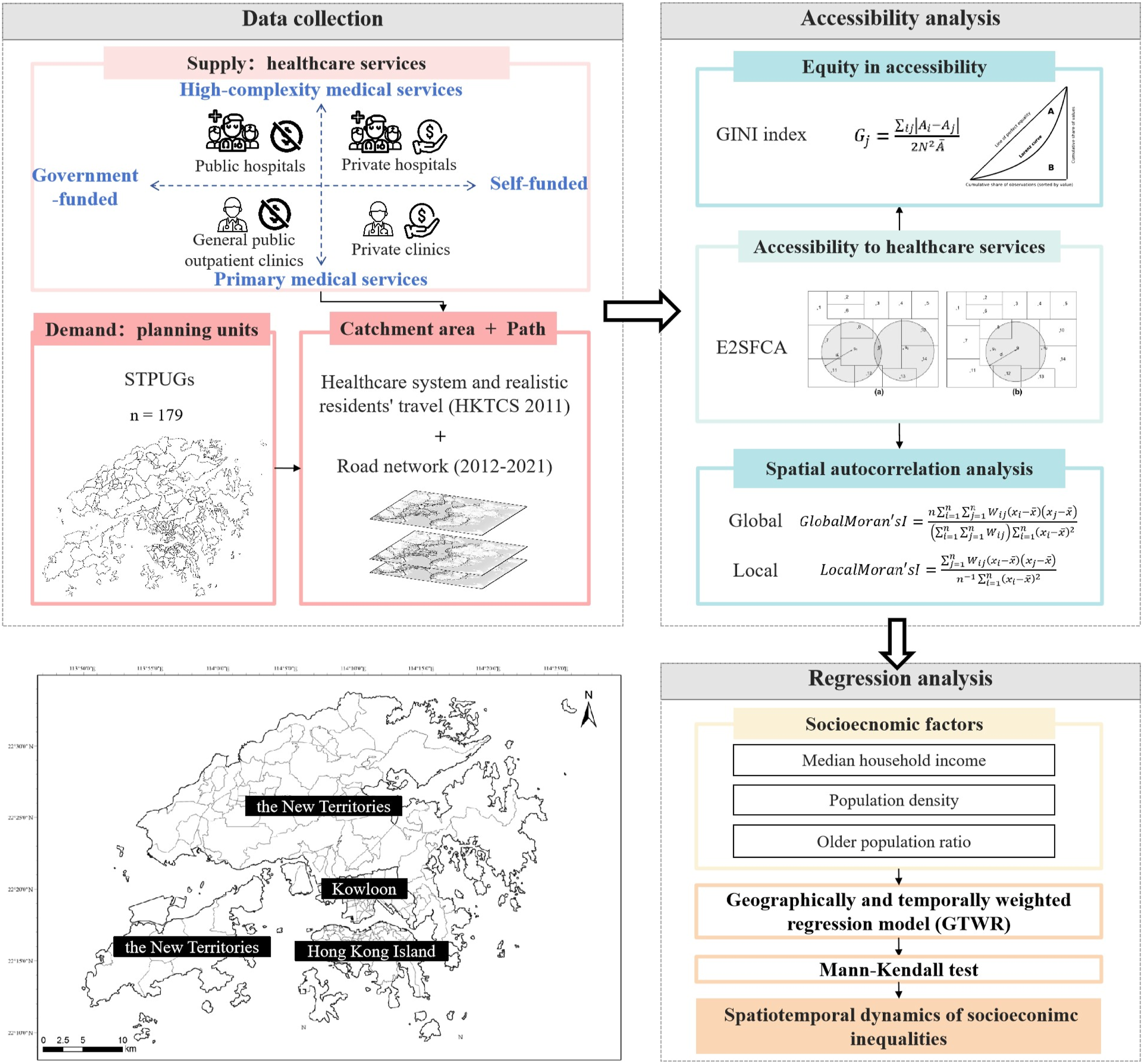
Results
Accessibility to multitier healthcare services
Healthcare accessibility was unevenly distributed. Figure S1 shows the average accessibility trends across STPUGs from 2012 to 2021. Overall, the average level of accessibility to all four healthcare types increased over the period, though with some fluctuations. A closer examination of each STPUG within the districts, using the Mann-Kendall test, revealed that most STPUGs in Hong Kong Island and Kowloon experienced a statistically significant increase in the four types of healthcare accessibility over time. However, most of the STPUGs in the New Territories showed a significant decreasing trend in the accessibility of public hospitals, private hospitals, and public general outpatient clinics (Figure S2). Public hospitals had higher accessibility than private hospitals, while private clinics surpassed public outpatient clinics. High-complexity medical services (hospitals) were more unevenly distributed than primary healthcare services (clinics) due to their spatial concentration. In 2016, urban areas (Hong Kong Island and Kowloon) had better accessibility to public hospitals, outpatient clinics, and private clinics than the New Territories, where private hospitals were largely absent (Figure S3). Public hospitals were more evenly distributed than private hospitals, while public outpatient clinics had a more balanced distribution than private clinics.
We observed significant spatial autocorrelation for healthcare accessibility in each year from 2012 to 2021 (Table S4). Figure 2 displays the local autocorrelation outcomes of healthcare service accessibility in 2012, 2015, 2018, and 2021. High-high agglomerations were predominantly situated in the Hong Kong Central Cluster and Kowloon Central Cluster, suggesting a clustering of high healthcare service accessibility in these areas. Conversely, low-high outliers were mainly observed in the surrounding regions, such as the Hong Kong East Cluster, Kowloon West Cluster, and Kowloon East Cluster, indicating that they were surrounded by areas with high accessibility. Low-low clusters were chiefly concentrated in the New Territories, signifying a clustering of low healthcare service accessibility in these regions. Over the 10 years, the cluster areas of public hospitals and private hospitals diminished in size, indicating a trend towards more equality in the high complexity of medical resources. Local indicators of spatial association map of healthcare accessibility in 2012, 2015, 2018, and 2021.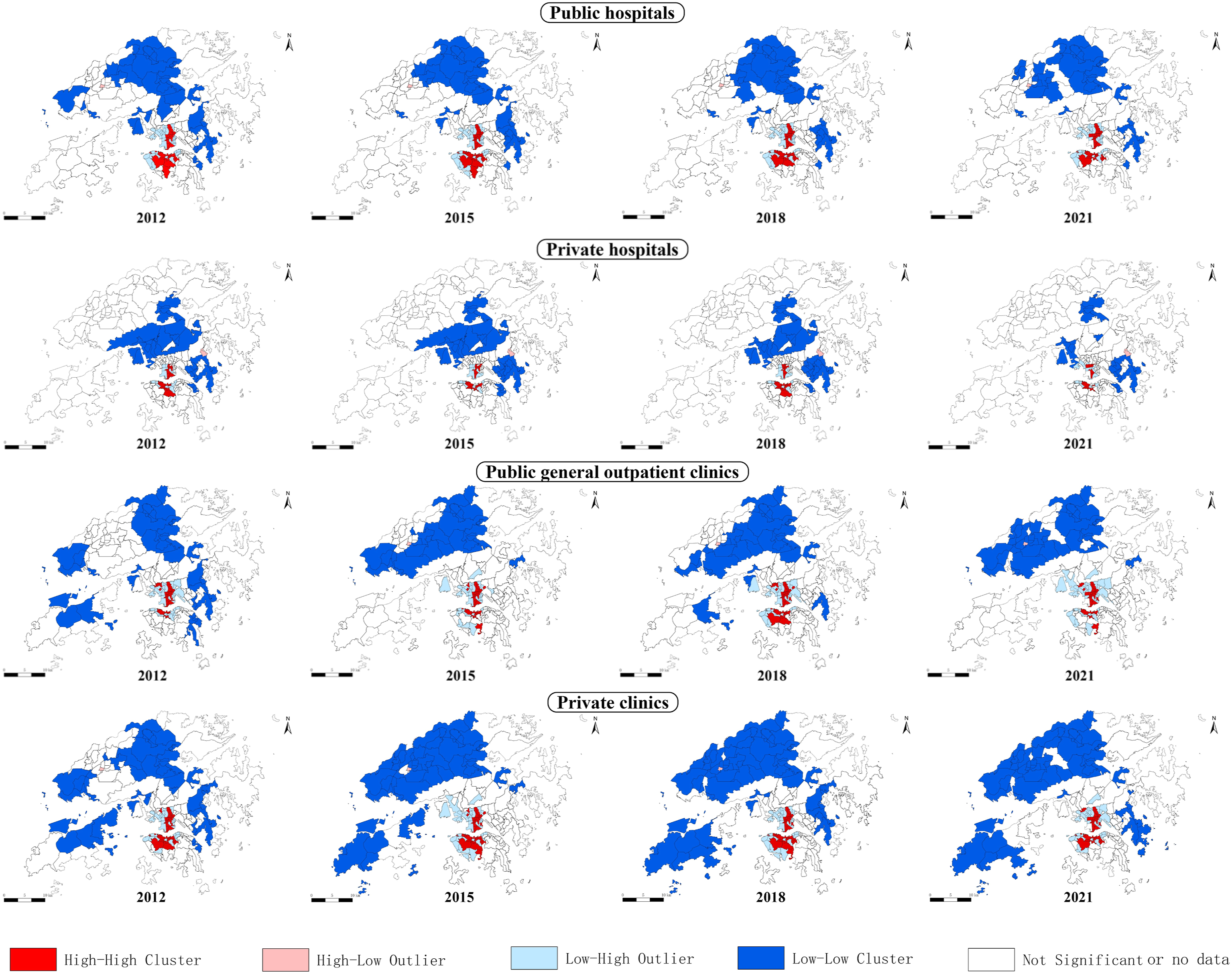
Equality in accessibility
The Gini coefficient was used to analyze the equality of healthcare resource accessibility at both the whole Hong Kong territory and district scales. The spatiotemporal equality of healthcare accessibility of the whole Hong Kong territory is shown in Figure 3. Spatial inequality existed across different types of healthcare service accessibility. The closer the Lorenz curve is to the equality line, the higher the equality in the accessibility of healthcare services. The Gini coefficients of government-funded facilities, including public general outpatient clinics and public hospitals, exhibited relatively higher levels of equality over the past decade. The Gini coefficients of self-funded facilities, including private clinics and private hospitals, demonstrated lower equality. Thus, government-funded healthcare service accessibility presented a better equality pattern than the self-funded healthcare service. Lorenz curves and Gini coefficients of the geographic distributions of healthcare service accessibility across STPUGs from 2012 to 2021.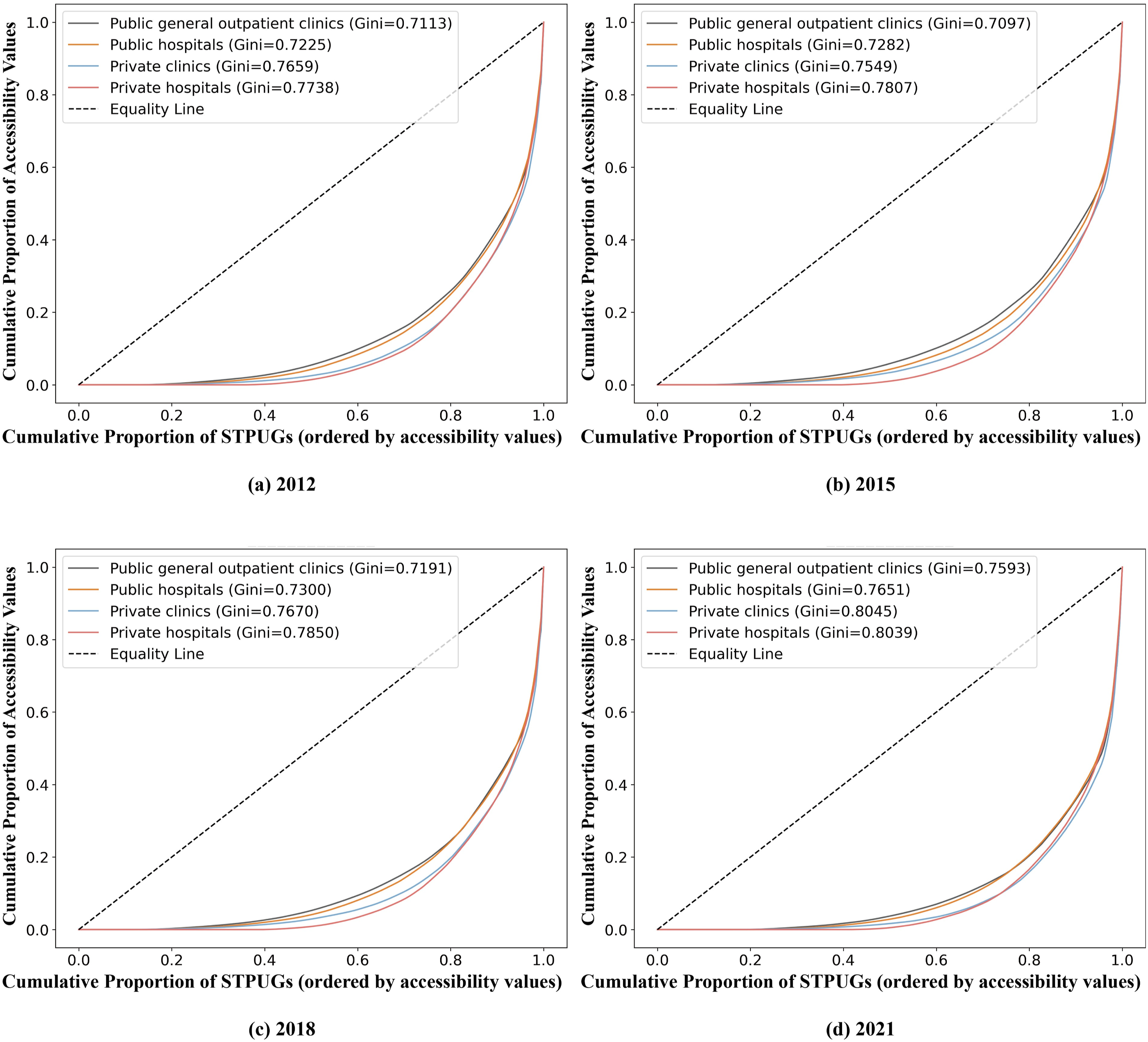
The GTWR model and the Mann-Kendall test results
The model fitting results are presented in Table S5. Compared to other models, the GTWR model demonstrated the highest R2 and the lowest AICc across all categories of healthcare services, indicating the best performance. Table S6 shows the summary of coefficients in the GTWR model, with all the variables exhibiting heterogeneity of coefficients. Figure S4 shows the coefficients for median household income and the older population ratio shifted from positive to negative over time, based on the average values across all STPUGs in Hong Kong. Population density consistently exhibited a negative relationship with accessibility across all types of healthcare services, and this negative trend becomes more pronounced over time. Figure S5 shows the Mann-Kendall test results of the coefficients. Most STPUGs significantly decreased over the time series, especially in Hong Kong Island and Kowloon. Some of the STPUGs in the New Territories presented an increasing trend over the period.
We further mapped the spatiotemporal heterogeneity of the associations between SES factors and healthcare accessibility. Figure 4 presents the results for median household income. As for public hospitals, the positive relationship between healthcare accessibility and median household income has gradually weakened in the time series, and in some cases, especially in Hong Kong Island and Kowloon, even shifted to a negative correlation. This suggests a decreasing trend of income-related inequality in public hospital accessibility across both urban and rural areas over time. As for private hospitals, most regions in the New Territories were not covered by private hospital resources, except for Sha Tin and Tai Po Districts. In covered areas, the positive relationship between healthcare accessibility and median household income shifted from positive to negative in the past decade, with the change occurring earlier in Kowloon than on Hong Kong Island. As for public general outpatient clinics, Hong Kong Island and most regions in the New Territories had a positive relationship between accessibility and median household income in 2012. However, this shifted to a negative relationship over the decade. Public general outpatient clinic accessibility in Kowloon was negatively related to median household income, with the negative trend strengthening over the period. As for private clinics, the relationship between median household income and private clinic accessibility was positive in 2012 and 2015, but this trend gradually shifted to negative after 2018, especially in downtown areas (Kowloon and Hong Kong Island), which indicates that private clinics were gradually servicing toward areas with lower median household income in downtown areas over time. Spatial heterogeneity of correlation between healthcare accessibility and median household income.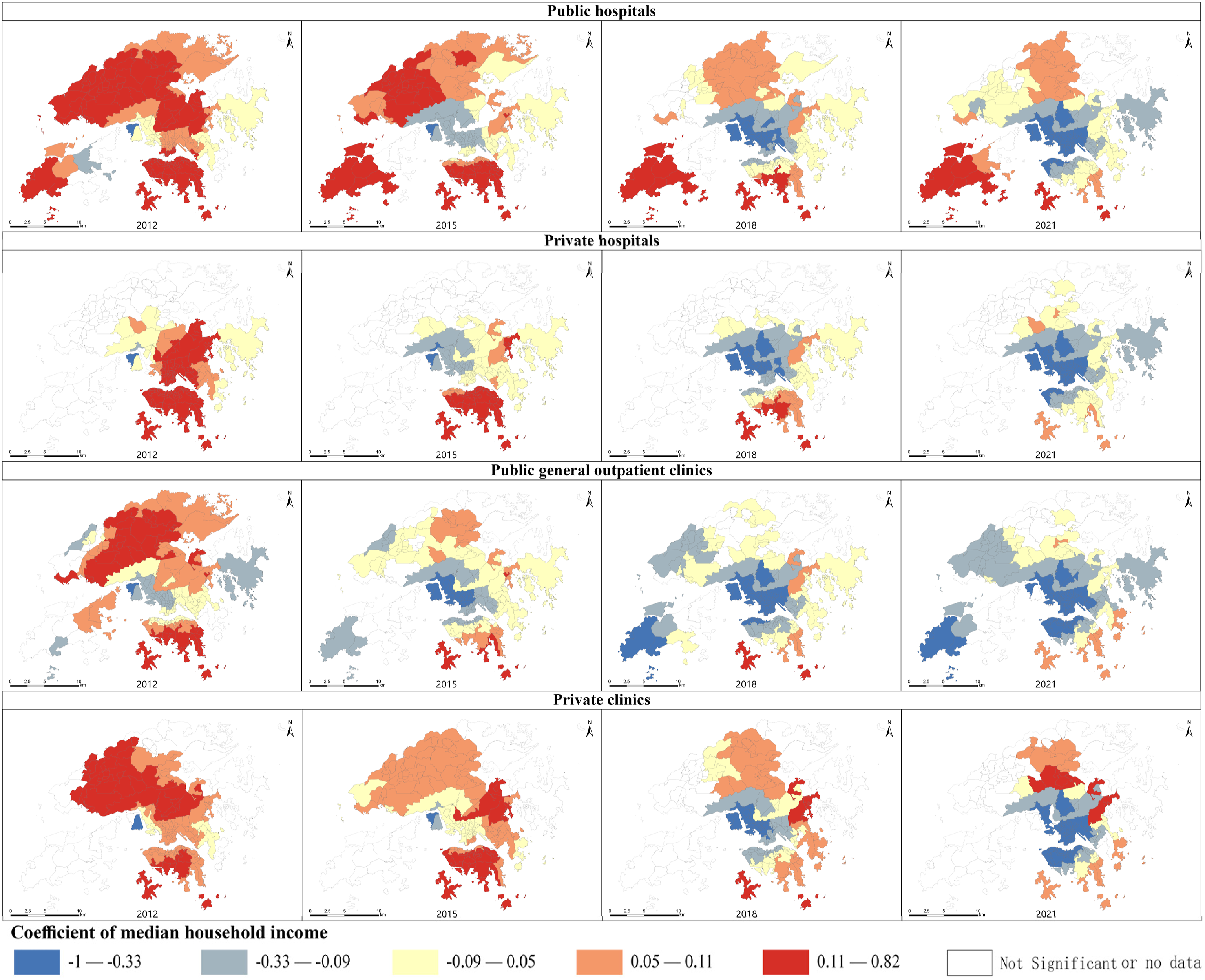
Results for population density are presented in Figure S6. As for public hospitals and private hospitals, the coefficients of population density in Hong Kong Island and Kowloon were negative, and the negative trend has strengthened over the period. This may be due to the public hospital resources not keeping pace with the population growth in these two regions. The trend in the New Territories were not significant. As for public general outpatient clinics, in downtown areas, population density was negatively related to healthcare accessibility, and this relationship strengthened gradually. As for private clinics, the population density was positive with healthcare accessibility in the New Territories and negative with healthcare accessibility in Hong Kong Island and Kowloon, and the negative trend in Hong Kong Island and Kowloon was strengthened over the decade.
Figure S7 presents the results for the older population ratio. As for public hospitals, in downtown areas (Hong Kong Island and Kowloon), the positive association between public hospital accessibility and the older population ratio has weakened, even gradually turning to negative after 2018. The possible reason was that the public hospital resources were not keeping pace with the growth of the older population ratio in these two areas. In suburban areas (the New Territories), however, the trend was unclear. As for private hospitals, the older population ratio in most regions had a positive impact on healthcare accessibility before 2015. However, this trend shifted to negative starting in 2018, particularly in the Kowloon central cluster and the western cluster of Hong Kong Island. As for public general outpatient clinics, except for Tuen Mun District and Yuen Long District in the New Territories, the coefficients of the older population ratio were consistently positive before 2015. However, these coefficients shifted to negative after 2015, especially in downtown areas. As for private clinics, the main change in the coefficient of the older population ratio occurred in Kowloon and Hong Kong Island after 2012, where the positive impact on private clinic accessibility shifted to negative.
Sensitivity check
Considering that COVID-19 may have affected residents’ travel behavior in 2020 and 2021, which could influence the estimated coefficients, we conducted a sensitivity analysis to ensure the robustness of our findings. We re-estimated the GTWR model using healthcare accessibility data and SES data from 2012 to 2019. The spatial distribution of the coefficients from 2012 to 2019 was presented, focusing on the correlation between median household income, population density, older population ratio, and multitier healthcare accessibility (see Figure S8-S10 in Supplementary Materials). The results showed that the overall trend of the coefficients remains consistent with the main findings.
Discussion
In this research, we examined the accessibility of multitier healthcare services in Hong Kong from 2012 to 2021 and revealed the relevant spatial autocorrelation. Then, we assessed the spatial equality of the healthcare service accessibility and its temporal dynamics. Most importantly, we further investigated the spatiotemporal heterogeneity of the associations between healthcare service accessibility, median household income, population density, and the older population ratio. Our study developed a holistic framework to comprehensively understand the allocation of multitier healthcare services in Hong Kong and its spatiotemporal associations with different SES factors, which provide valuable insights for policymakers and urban planners to establish a more equitable and inclusive healthcare service system.
Accessibility and equality to multitier healthcare services
Firstly, different types of healthcare services have different accessibility distributions. In high-complexity medical services, the average level of accessibility to government-funded facilities was higher than that of self-funded ones. In primary medical services, the average level of accessibility to government-funded facilities was lower than that of self-funded. From the perspective of equality, government-funded healthcare service accessibility presents a better equality pattern than self-funded healthcare service. A study from South Korea found that government-owned hospitals have better equality than private hospitals (Kang et al., 2020). The factor is that private hospitals cater to individuals with higher incomes, offering a more comfortable healthcare environment compared to public hospitals, so they tend to be clustered in areas with higher economic prosperity. Besides, accessibility to primary healthcare services exhibited a better performance compared to the accessibility to high-complexity medical services, which is aligned with a previous study, indicating that inequality between groups increases with the tier of healthcare services (Jin et al., 2022). A study from Nanjing, China, also confirmed this viewpoint (Cheng et al., 2020), suggesting that upper-tier hospitals tend to be more clustered and have less even accessibility compared to lower-tier hospitals. Another previous study suggested that community healthcare services balanced the regional inequality of hospitals (Meng et al., 2022).
Second, spatiotemporal disparities were evident in both healthcare service accessibility and equality. Hong Kong Island and Kowloon have high healthcare accessibility, while the New Territories have low healthcare service accessibility. It is consistent with previous research findings (Liu et al., 2024), which indicated that the living amenities of the New Territories, including healthcare facilities, exhibited a higher degree of inconvenience compared to those in Hong Kong Island and Kowloon. Two primary reasons may account for this result. One is healthcare services tend to cluster in the established urban areas, i.e., Hong Kong Island and Kowloon, resulting in higher density compared to the New Territories. The other reason is that the established urban areas may potentially benefit from more mature road and transit infrastructure, facilitating more convenient transport to healthcare services (Zhao et al., 2020). It is demonstrated that the geographical accessibility to healthcare services depends on transportation availability (Silva et al., 2023).
Advantages of the GTWR model in revealing spatiotemporal associations
This paper employed the GTWR model to explore the spatiotemporal impact mechanisms of SES factors on healthcare accessibility. Compared to previous studies, there are two advantages. Firstly, the GTWR model can analyze the nuanced impact of SES and demographic factors on healthcare accessibility, revealing spatial heterogeneity. The results reveal that the relationship between accessibility and socioeconomic status differs across regions, such as downtown and suburban areas, established and establishing areas. This regional analysis helps policymakers optimize resource distribution more effectively in diverse socio-economic contexts, aiming for equitable healthcare coverage. Secondly, the GTWR model revealed temporal dynamic patterns in the correlation between healthcare accessibility and SES when applied to long-term time-series data. For instance, between 2012 and 2021, the number of public hospitals in Hong Kong increased from 39 to 41, private hospitals from 10 to 13, and the number of public general outpatient clinics and private clinics also increased in response to market demand. At the same time, socioeconomic factors, population density, and the older population ratio have been changing every year, forming a continuous and long-term dynamic process. Most existing studies focus on data from a single year (Cheng et al., 2020; Jin et al., 2022; Zhao et al., 2020), which can lead to instability and bias in the results. By incorporating the GTWR model, we can comprehensively analyze how healthcare accessibility is influenced by economic growth and changes in population structure, providing valuable policy recommendations for future healthcare planning.
Dynamic socioeconomic inequalities in healthcare accessibility
Socioeconomic inequalities in healthcare accessibility are evident in Hong Kong. Around 2012, healthcare accessibility was mainly positive with median household income, which indicated that people with higher incomes possessed more healthcare resources, whether it was public hospitals, private hospitals, public general outpatient clinics, or private clinics. However, the positive correlation between healthcare accessibility and median household income has been reversed in downtown areas (Hong Kong Island and Kowloon) after 2015, and the inequality among people with lower incomes has gradually reduced. There are two main reasons. One reason is population changes. The population in low-income areas grows slower than that in high-income areas, leading to an increase in healthcare accessibility in low-income areas and a decrease in that of high-income areas. As a result, healthcare service accessibility has become more equitable across income levels. Another reason is the increase in hospitals in low-income areas, such as the Tin Shui Wai Hospital, which opened in Yuen Long District in 2016, and the Hong Kong Children’s Hospital, which opened in Kowloon City District in 2017. This has improved healthcare accessibility in low-income areas. Previous studies often stressed that there were significant spatial and income inequalities in healthcare accessibility between high-income and low-income groups (Jin et al., 2022; Zhao et al., 2020). However, in the past decade in Hong Kong, we have observed that these inequalities are gradually diminishing, with healthcare resource distribution becoming more equitable in terms of spatial distribution and economic levels.
The relationship between population density and healthcare accessibility exhibits dynamic changes. In downtown areas, the negative correlation between population density and healthcare accessibility has strengthened. This may be due to the population growth of the downtown areas of Hong Kong in the past decade, while the expansion of healthcare facilities has not kept pace with this population increase, resulting in a more negative association between population density and healthcare accessibility. In suburban areas, the negative correlation between population density and public hospital accessibility has strengthened. The private hospital accessibility in suburban areas was very low. The trends of public general outpatient clinics and private clinics fluctuated slightly. This suggests that the growth of high-complexity medical services in suburban areas did not keep up with the population growth, while the increase in primary medical services has met the healthcare demand of population growth. Therefore, the expansion of high-complexity medical resources in suburban areas should be prioritized.
The relationship between healthcare accessibility and the older population ratio shifted from positive to negative across four types of healthcare services. The main reason is the severe aging population of Hong Kong. The proportion of individuals aged 65 and above increased from 13.3% in 2011 to 19.6% in 2021, and this trend is expected to continue. Due to the higher demand for primary healthcare (Chi and Chui, 1999) and high-complexity medical services (Wong et al., 2021) among the older population, this widespread societal phenomenon presents a significant challenge to the healthcare system.
Implication
Firstly, the disparities in healthcare accessibility between low-income areas and high-income areas in Hong Kong have decreased. Hence, policymakers should pay more attention to healthcare resource allocation in areas with high population density and the older population ratio. Secondly, the disparities in accessibility and equality across multitier healthcare services highlight the need for a comprehensive analysis of multitier healthcare services tailored to the local healthcare system. For high-complexity medical services, constructing new public hospitals (Jin et al., 2022) or expanding public general outpatient clinics within hospitals in low-accessibility areas can all help alleviate inequalities in healthcare accessibility. For primary medical services, public general outpatient clinics should be strengthened, particularly in low-income areas, as equitable distribution of primary healthcare services is an effective way to reduce health disparities (Kawakami et al., 2011; Kirby and Kaneda, 2005). Thirdly, the expansion of healthcare resources should consider the rapidly aging population of Hong Kong society. In the past decade, due to the severe aging of the population, the inequality in healthcare resources for the elderly has become more pronounced. The demand for healthcare facilities among the older population is greater than that of younger people. Thus, healthcare resources should be allocated more towards the groups with higher demand.
Limitations and future works
There are several limitations in this study. First, this study analyzes healthcare accessibility over the period from 2012 to 2021; however, the travel behavior input is derived from the HKTCS 2011, without dynamic adjustments throughout the decade. This may introduce potential bias, such as the expansion of the MTR network could have altered residents’ travel behavior. Nevertheless, HKTCS 2011 remains the most recent publicly available, large-scale, and government-led dataset reflecting residents’ travel patterns. The latest HKTCS 2021 data has not yet been completed. Once it becomes available, we plan to update the analysis to improve the temporal precision and overall robustness of our findings. Second, although our study takes into account residents’ actual travel patterns, there remains a lack of residents’ subjective understanding of healthcare service accessibility (i.e., motivations and barriers), which is as important as the actual geographical accessibility of these facilities (Wu et al., 2022). Third, due to the lack of historical data, the capacity of healthcare facilities, such as the number of beds and healthcare personnel, was not taken into consideration. Such variables should be incorporated in future studies if relevant data is available. Finally, it should be noted that there might be disparities between accessibility and the real utilization of healthcare services. Due to the data limitation, our study failed to compare such differences, which should also be addressed in future studies.
Supplemental Material
Supplemental Material - Spatiotemporal patterns of accessibility and inequality in Hong Kong’s public and private healthcare system: A ten-year longitudinal study
Supplemental Material for Spatiotemporal patterns of accessibility and inequality in Hong Kong’s public and private healthcare system: A ten-year longitudinal study by Xinyi Zou, Ying Zhou, Yuxuan Zhou, Yi Lu in Environment and Planning B: Urban Analytics and City Science
Footnotes
Author contributions
Zou Xinyi: Conceptualization, Methodology, Formal analysis, Investigation, Writing - Original Draft, Visualization
Zhou Ying: Formal analysis, Supervision
Yuxuan ZHOU: Conceptualization, Methodology
Lu Yi: Conceptualization, Methodology, Writing - Review & Editing, Supervision
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key R&D Program of China [grant number 2022YFF0607003].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.