
Abstract
Maternal health constitutes a pivotal aspect of the healthcare system, bearing immense significance for the future of a nation. But in lower-middle income countries like India, maternal health has always been a matter of concern, especially among the tribal population. It has been observed that in numerous tribal regions, the effective utilization of maternal health services remains elusive, due to different determinants at both community and individual levels. This study aims to explore the maternal healthcare provisions among the Oraon community of Jalpaiguri district, West Bengal, to provide a clear representation of the present scenario. The findings of this study disclose an increasing inclination towards modern healthcare facilities, coexisting with the age-old traditional healthcare practices. The choice of antenatal care providers and delivery place is considered as two essential health inputs to portray the community perspectives. Sociocultural and religious beliefs within the community also emerged as key influencers in shaping maternal healthcare practices.
Introduction
Maternal health research is of paramount importance for several reasons, as it has a direct impact on the well-being of mothers and newborns and the overall health of societies. It is a critical aspect of any society, and among indigenous communities with rich cultural heritage residing in remote and often marginalized areas of the country, it takes on unique dimensions. Their maternal health challenges are distinct, rooted in a blend of traditional practices and socio-economic factors. Among the tribal communities, pregnancy and childbirth are deeply ingrained in their cultural fabric. Motherhood and the process of childbirth are viewed as a sacred journey, involving rituals, customs and the presence of traditional birth attendants (TBAs). Cheyney (2011) introduced the idea that childbirth is not just a biological process but also a cultural and political act. Davis-Floyd (2004) emphasizes that childbirth extends beyond its biological dimension and serves as a culturally significant, ritualized experience. Building on Gennep’s (1960) model of rites of passage—which includes the phases of separation, transition (liminality) and reintegration—she explains how even modern clinical birth settings are structured around symbolic rituals and hierarchical authority. Following Davis-Floyd’s (2004) and Cheyney’s (2011) critiques of technocratic birth, this study explores maternal health as a culturally embedded experience among the Oraon community in Jalpaiguri. The community’s reverence for their customs adds a layer of complexity to modern maternal healthcare practices. This article delves into the state of maternal health among the Oraon, shedding light on the complexities and advocating for comprehensive interventions to nurture a healthy future. The Oraon is a culturally enriched community that migrated from the Chotanagpur regions and settled in different parts of India, including West Bengal (Bhowmik, 2016; Mondal, 2000; Roy, 1915). This migration process from Chotanagpur and its adjoining regions of neighbouring states took place during the time of British colonial rule, and a large number of those migrated people were recruited to various tea plantations as tea labourers. After migration, these tribal people started to inhabit a new ecological condition and sociocultural milieu completely different from that of Chotanagpur. These changes in habitation caused a disconnection from their own age-old traditions, and this distance from their own traditions influences their healthcare practices, as culture is an important element in determining the health status of a community (Tarafdar, 2020). This study elucidates the brief idea of how culture plays a crucial role in maternal healthcare practices. The overall aim of this study is to explore maternal health and healthcare provision among the Oraon of Jalpaiguri district, West Bengal, and to present a clear representation of the present scenario. The research objectives of the study are as follows:
To explore the experiences and perceptions of community members about maternal healthcare To estimate the effects of individual and community-level efforts and the utilization of both traditional and modern healthcare systems in the context of maternal health To examine the important factors regulating the perspective of maternal healthcare among the members of the Oraon community To analyse the changing aspects of the Oraon community, highlighting the urban influence and its effect on maternal health
Area Profile
The current study is a part of a master’s dissertation paper and further relevant extension aimed at assessing the maternal and child health status among the Oraon people in the Jalpaiguri district of West Bengal. The study area has been divided into two segments for the purpose of fieldwork, based on proximity to the district headquarters and the degree of urban influence. The urban segment of the study area falls within the Jalpaiguri Sadar subdivision, located approximately 2 km away from the district headquarters. This urban segment was chosen to reflect urban influence and was selected due to the notable concentration of the Oraon population near the district headquarters. In contrast, the rural segment of the study area is situated in the Malbazar subdivision and is characterized by a relatively lesser level of urban influence. This segment covers a portion of the Baintgoori Tea Estate and is considered rural, situated quite far from the nearby urban centre. The decision to include this area in the study was influenced by references of Oraon community members from the urban segment. The division of the study area into two distinct groupings based on proximity and remoteness serves the purpose of investigating and documenting factors that affect availability and accessibility. This division aims to facilitate optimal and enhanced utilization of healthcare services while also shedding light on the contributing factors to suboptimal utilization and the barriers that impede the integration of contemporary healthcare services.
Methodology
This article exclusively relies on a diverse range of qualitative data along with some basic quantitative data gathered using a range of prominent research techniques to explore maternal health–related issues on the Oraon community. The study employed a qualitative research design with limited quantitative support to examine the maternal healthcare situation. The qualitative aspect involves the use of intensive observation techniques and open-ended questions, while the quantitative component consists of basic healthcare-related statistics regarding antenatal care and delivery place. In the pursuit of this research, fieldwork was conducted in two distinct areas within the Jalpaiguri district. These two areas were carefully selected to provide a comprehensive representation of the current scenario. The study included 62 households with a total population of 304. A purposive sampling method was administered to select participants who have experienced motherhood. The total sample comprised 76 women from the selected female population. This sampling approach ensured that participants with relevant experiences in maternal health were included in the study. In addition, a case study method was applied to gather in-depth insights, selecting seven cases from different age groups and social backgrounds to present a detailed scenario of the current situation. While the sample size is modest, it is adequate for qualitative exploration, allowing for in-depth interviews and repeated interactions with the participants.
Data Collection Methods
Household Schedules
Relevant information was obtained through household schedules that documented basic demographic and healthcare data.
Unstructured Interviews
The primary data collection was done through unstructured interviews, employing open-ended questions to encourage participants to share their experiences freely. The interviews allowed for the exploration of maternal health issues from the perspective of the Oraon women.
Case Study
Seven individual cases were studied in-depth, representing a range of age groups to provide detailed accounts of maternal healthcare practices and challenges. The seven cases were strategically selected to provide a comprehensive understanding of maternal healthcare experiences among Oraon women over the years. The selection criteria ensured diversity in age, residence, healthcare access and traditional practices.
Secondary Data
Secondary data were also gathered to support the research, sourced from a wide range of books, academic journals and relevant information from the internet. These secondary data provided contextual information and supplemented the findings from the primary data collection.
Result and Discussion
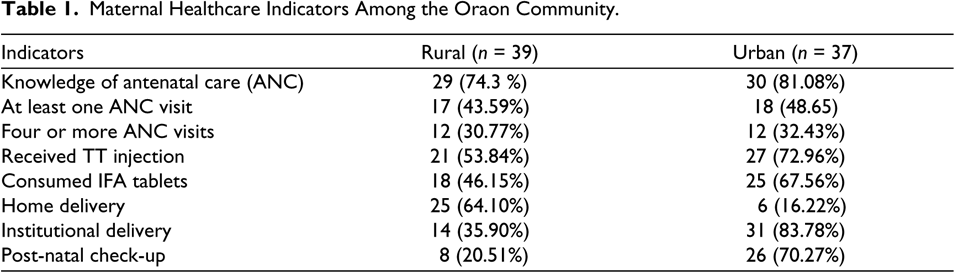
Antenatal care, commonly known as prenatal care, involves medical supervision and support provided to pregnant women to ensure a healthy pregnancy and safe delivery. It is a crucial component of maternal healthcare aimed at monitoring both the mother’s and the foetus’s well-being. This care includes identifying potential risks, addressing complications and promoting overall health throughout pregnancy (World Health Organization [WHO], 2016). The present study examines various aspects of antenatal care, including awareness, the frequency of check-ups, healthcare providers and maternal experiences during pregnancy. For the purpose of exploring these issues, data were collected from 76 women out of the total female population selected through purposive method of sampling who have experienced the journey of motherhood. Among these 76 women, 39 are from the rural segment of the study area and 37 are from the urban segment of the study area. Information collected from these respondents of both the segments is provided in Table 1.
Maternal Healthcare Indicators Among the Oraon Community.
Understanding Motherhood Through Narratives: Practices, Beliefs and Experiences of Oraon Women
The data collected from 76 women, spanning both rural and urban populations, paint a vivid picture of maternal healthcare practices in the study area. However, beneath the numbers lie individual stories and experiences, which reveal the challenges these women face during their journeys through motherhood. Each woman’s story offers a unique lens into the journey of pregnancy, reflecting resilience, resourcefulness and the blending of indigenous and institutional care.
The Enduring Role of Traditional Knowledge
For many rural Oraon women, maternal care is deeply rooted in traditional practices, where family members—especially mothers-in-law and TBAs, known as Aayo (means mother in Kurukh language)—play a pivotal role in guiding expectant mothers. Sukurmoni Oraon (41 years old), a mother of three, recalls her first pregnancy at 19, when she had no knowledge of antenatal care. Living in a remote tea garden, she depended entirely on her mother-in-law’s wisdom. ‘She told me to eat boiled greens, rest often, and avoid heavy lifting. I didn’t question her; I trusted her’, Sukurmoni reminisces. With no access to institutional healthcare, she delivered at home under the care of a TBA, an experience she describes as both ‘terrifying yet comforting’. Similarly, Muno Oraon (56 years old) relied exclusively on traditional birth attendant during her pregnancies. She fondly remembers how the TBA massaged her swollen legs and prepared herbal concoctions to ease her dizziness and fatigue. The deep trust in traditional healers highlights how, for many Oraon women, pregnancy care extends beyond physical well-being to emotional and communal support. These experiences are not merely pragmatic but culturally significant. Drawing on Bell’s (1992) theory of ritualization, such maternal care routines can be interpreted as structured actions through which social norms, identity and power dynamics are reinforced. By adhering to these routines, Oraon women are not just being cared for but are participating in ritualized performances that affirm their roles within kinship, community and motherhood.
Struggles and Adaptations in Urban Settings
In contrast, Oraon women in urban areas, despite greater exposure to modern healthcare, often face financial barriers and fragmented support systems. Everensia Oraon (47 years old), living in a town with access to hospitals, could not afford medical visits. ‘The hospitals were there, but how could I go when I didn’t even have money to buy medicines?’ she says. Instead, she turned to a traditional healer in her native village, Rangalibajna. Her husband would bring back herbal medicines, which she used in place of costly medical treatments. Her story highlights how economic constraints push even urban women towards indigenous healthcare solutions.
Bridging Traditional and Modern Care
For some women, institutional healthcare and traditional remedies coexist, forming a hybrid approach to maternal care. Sunam Oraon (29 years old) had a positive antenatal experience, thanks to ASHA workers who guided her through six antenatal check-ups. ‘They explained why I needed vaccines, what foods would make my child strong, and even simple exercises to do at home’, she shares. Despite embracing modern healthcare, she continued drinking her mother-in-law’s homemade herbal drink, believing it contributed to her child’s strength. Similarly, Kiran Oraon (39 years old) relied on both biomedical treatment and traditional healing for pregnancy-related discomfort. Suffering from severe back pain and swelling, she took doctor-prescribed tablets, but her grandmother insisted on herbal oil massages. ‘Was it the medicine or herbal oil that cured me? I didn’t know’. Over time, her health issues resolved, but she remains uncertain about the specific factors that contributed to her recovery. Her experience emphasizes the cultural continuity of traditional remedies even among younger generations.
While awareness of antenatal care is growing, logistical barriers prevent many rural women from accessing institutional healthcare. Jalhi Oraon (23 years old) understood the importance of antenatal check-ups, but the treacherous roads and long distances to the nearest hospital meant she could only visit a few times. ‘Each visit felt like a victory’, she says. Fortunately, the local ICDS centre provided food supplements and basic medicines, helping her manage her pregnancy despite limited healthcare access. However, some women face more than just physical challenges—social and cultural beliefs also shape their pregnancy journey. Fagni Oraon (35 years old) experienced severe swelling, nausea and fatigue during her third pregnancy. Her family initially attributed her condition to an evil eye (bishahi) and conducted magico-religious rituals, burning incense and chanting prayers. ‘They believed something bad had fallen upon me’, she recalls. When her condition worsened, they rushed her to Bagan Hospital, which later referred her to Malbazar hospital, where doctors diagnosed her with severe anaemia. Timely medical intervention saved both her and her baby. ‘I was so scared, but the doctors and my family’s prayers saved me’, she says, reflecting on the interplay of faith and medicine in her survival.
Challenges
While a considerable portion of individuals residing in the study area still resort to indigenous treatment methods, there exists a burgeoning progressive mindset within tribal communities towards contemporary healthcare practices. Despite witnessing an increasing positive mindset towards modern healthcare facilities within the rural segment of the study area, impediments such as poverty, sociocultural belief and geographical remoteness continue to create obstacles for the complete adoption of modern treatment modalities. In the rural sector of the current study area, a combination of sociocultural and geographical impediments has presented challenges in accessing appropriate healthcare facilities; however, the prominence of the geographical barrier is somewhat greater. The distance to the hospital and the subpar road conditions pose significant issues within this region. Furthermore, the lack of available transportation further compounds these circumstances. Jalhi Oraon, residing in the rural region, attempted to follow modern antenatal care practices. However, poor infrastructure at the local Bagan Hospital and the long, poorly connected route to Malbazar Government Hospital made consistent visits nearly impossible. She managed only three to four visits during her pregnancy. Despite understanding the importance of check-ups, logistical hurdles remained insurmountable. Her experience illustrates how geographical barriers, combined with poor infrastructure, hinder the effective utilization of maternal health services, even when awareness exists.
Like geographical barriers, sociocultural norms also remain a subtle yet powerful deterrent to the timely utilization of modern healthcare services (Chandra et al., 2016; Tarafdar, 2022) The sociocultural beliefs are evident in cases such as that of Fagni Oraon, who experienced serious complications during her third pregnancy. Despite alarming symptoms, her condition was initially attributed to the evil eye, leading the family to rely on magico-religious healing rather than seeking medical care. Only after her health condition became worsened, she was referred to a higher tier of biomedical health facility, where she was diagnosed with anaemia and treated successfully. This delay in accessing biomedical care highlights how traditional belief systems continue to shape health-seeking behaviour. This one is a classic case of competing explanatory models (Kleinman, 1980) where illness is interpreted within both spiritual and biomedical domains.
The urban sector of the study area portrays a more favourable scenario, with the absence of both geographical and social barriers. The impact of urban influence on this study segment alleviates the issues associated with both types of barriers. This has translated into improved maternal care practices. Sunam Oraon, from the urban sector, underwent seven antenatal check-ups with minimal discomfort during her pregnancy. Her experience was shaped not just by proximity to healthcare but also by the persistent efforts of ICDS and ASHA workers, who guided her dietary and medical routines. Her case stands as an example of how government health initiatives can effectively transform maternal outcomes when coupled with accessibility and community support. Yet, access does not always guarantee utilization. Everensia Oraon, another woman from the urban segment of the study, represents the complexities that persist even in better-equipped areas. Despite being surrounded by healthcare facilities, she could not fully utilize them due to financial constraints and limited health literacy. In the face of these barriers, she turned to traditional herbal remedies sourced from a healer in her native village, miles away from the town. In times of extreme need, when neither traditional nor modern resources were available, she fell back on home remedies. Her case underscores how economic and educational shortcomings can limit health choices, regardless of geographic location (Balgir, 2006; Ghosh & Malik, 2009).
Economic hardship emerged as a shared challenge across both rural and urban segments of the study area. In both contexts, limited financial resources act as a major barrier to accessing and utilizing healthcare services effectively. During the field survey, key economic indicators—such as monthly income and expenditure patterns, levels of education, housing and sanitation conditions, and employment opportunities—were closely examined. These factors, deeply intertwined with broader socio-economic conditions, were found to significantly shape health outcomes and influence healthcare-seeking behaviour (Balgir, 2006; Ghosh & Malik, 2009). The economic landscape of the population exhibited clear contrasts between rural and urban settings. In rural areas, the majority of individuals are employed as tea garden labourers, earning minimal and unstable wages. Urban migrants, while having greater exposure to healthcare facilities, often work in informal sectors such as construction, with similarly limited financial security. A small segment of the urban population has managed to attain government employment, offering relatively more stability. However, the overall urban economic condition, though better than that of rural areas, is not strong enough to ensure equitable access to healthcare for all. These financial constraints have a direct impact on maternal healthcare practices and decision-making. In rural areas, economic limitations lead many to regard pregnancy and childbirth as natural processes that do not require medical attention. Women continue with their regular domestic and labour activities throughout pregnancy, often without seeking antenatal care. In contrast, urban areas offer a wider range of healthcare services, and women with relatively better financial means are more likely to attend regular prenatal check-ups and seek professional medical support during childbirth. Yet, for many others in urban areas, economic hardship continues to limit access to these services. This disparity in economic conditions between the two segments significantly influences the utilization of maternal healthcare. While infrastructure may be more developed in urban areas, economic inequality remains a persistent barrier. Addressing these underlying socio-economic factors is essential to ensuring more equitable and effective healthcare delivery for all women, regardless of their geographic or economic context.
Tribal Approach to Pregnancy and Motherhood
In tribal societies, the essence of motherhood and childbirth intertwines seamlessly with their culture and community fabric. Within these societies, distinct customs and beliefs enshroud these pivotal moments. The act of childbirth transcends individuality, morphing into a communal endeavour where the entire community unites to bolster and aid the anticipating mother. Age-old rituals and ceremonial practices collectively steer and support women through the transformative journey of pregnancy and childbirth. According to Turner, ‘we must regard the period of margin or liminality as an inter-structural situation, periods of transition during rites of passage or other rituals or during pilgrimages are similar in that they are neither here nor there’ (Moore, 2011; Turner, 1967, 1984). This approach not only underscores the significance of shared insights but also illuminates the profound intergenerational bond thriving within the tribe’s embrace. Similar to other tribal communities, the Oraon people possess distinct beliefs and practices surrounding motherhood and childbirth.
Cultural Restrictions/Taboos
From the moment a woman shows signs of pregnancy, she is advised against attending cremations or touching a dead body, as such actions are thought to carry negative spiritual energy that could harm the foetus. Kiran Oraon recounts her own experience:
When my uncle passed away, I was in my second month. I felt guilty for not being able to pay my respects. But my grandmother firmly said, ‘Your child comes first now. The spirits of the dead can disturb the living ones inside you’. Her words stayed with me, and I realized how seriously they protect both mother and child.
Protective Measures Against Thunderstorms
The fear of lightning and thunder is deeply rooted in the community. Pregnant women are not allowed to remain outside when lightning flashes or thunder roars. Fagni Oraon, who has lived in a rural village her whole life, described the feeling:
Once, during my first pregnancy, I was sitting outside under a tree when the sky turned dark. Suddenly, thunder cracked, and my mother-in-law came running out of the house, yelling for me to come inside. She wouldn’t let me go back out until the storm passed. I didn’t understand then, but now I feel it was their way of making me feel safe from the unknown.
Covering to Ward Off Evil Eyes
There is a strong belief in the Oraon community that the evil eye or malicious intent from others can affect a pregnant woman and her unborn child. Therefore, the expectant mother is told to cover herself fully, especially when outside the home. Jalhi Oraon spoke of her experience with this custom:
My sister-in-law had suffered a miscarriage once, and my family believed it was because of an evil glance from a woman in the village. So, during my pregnancy, they made sure I was always fully covered. At first, it felt restrictive, but soon I realized it was their way of showing love and concern.
The Emotional Weight of Tradition
While these rituals are rooted in community and protection, they also carry a heavy emotional influence for the women. Cheyney (2011) argues that childbirth rituals can act as both empowering performances and sources of control, depending on how they are interpreted and enacted. Furthermore, Butler (1997) suggests that such ritualized practices can reinforce gendered norms through performative repetition, creating internal conflict between social belonging and personal autonomy. Muno Oraon shared the complexity of her feelings:
There were moments when I felt overwhelmed by the restrictions—being wrapped up, staying indoors, not being able to attend important events. But at the same time, it felt like everyone was investing their energy in me and my child. It involved both restrictions and reassurance.
Adapting Tradition in Modern Times
As the Oraon women navigate between tradition and modern healthcare, some practices have evolved. Sunam Oraon who now lives in a more urban setting, mentioned how she balances both worlds:
In my village, childbirth is accompanied by several taboos, such as staying indoors, avoiding strangers, and refraining from attending funerals. After the birth of the first child, a goat sacrifice to the village deity is an important ritual. However, in the city, doctors prioritize medical care over these traditional practices. Despite this, we make an effort to follow some of these customs.
From Narratives to Themes
Coding of Narratives and Emergent Themes Related to Maternal Healthcare Practices.
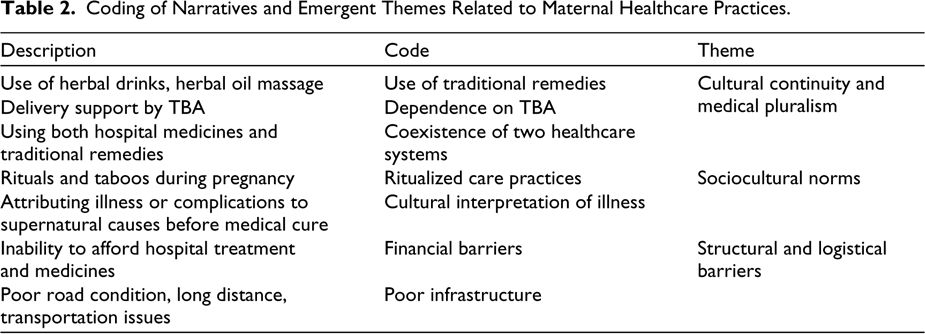
The codes generated from the narratives and the resulting thematic categorization are presented in Table 2. The narratives, when coded, revealed repeated patterns—dependence on TBAs, herbal remedies, protective taboos, decisions made by elders and difficulties in accessing healthcare facilities. Clustering these codes brought out three broader themes. The first is cultural continuity and medical pluralism. Sukurmoni’s reliance on her mother-in-law and the TBA during her first pregnancy, and Muno’s account of herbal massages and remedies, highlight the enduring place of traditional knowledge. At the same time, Sunam’s and Kiran’s experiences illustrate how biomedical treatment and traditional practices often coexist—medicines prescribed by doctors were combined with herbal drinks or oil massages. These cases show how women negotiate between two systems of care rather than replacing one with the other. The second is sociocultural norms. Authority of elders, gendered expectations and ritual taboos shape maternal care across both rural and urban contexts. Kiran recalled being prohibited from attending her uncle’s funeral, while Fagni described how her illness was initially explained through the evil eye. Jalhi’s family ensured she remained covered to ward off harmful glances, and Muno reflected on the emotional impact of these restrictions. These examples demonstrate how norms regulate behaviour, provide protection and sometimes create inner conflict. The third is structural and logistic barriers. Distance, poor infrastructure, poverty and limited health literacy remain persistent challenges. Jalhi managed only a few antenatal visits because of bad roads and poor transport. Everensia, despite living near hospitals in town, could not afford consistent medical treatment and turned instead to a traditional healer in her native village. These cases highlight how both rural and urban women confront barriers—geographical in one case, economic in another—that restrict their access to biomedical care. These themes are interconnected rather than separate. Traditional practices (Theme 1) are reinforced through sociocultural norms (Theme 2). These norms influence how women respond to barriers (Theme 3). Conversely, when barriers block access to biomedical facilities, women often return to cultural practices, creating a cycle that sustains tradition within modern contexts.
Integration of Traditional and Biomedical Maternal Healthcare
Collaborative Care Pathways
Field narratives reveal that TBAs are still trusted cultural figures, offering both physical care and emotional guidance. Sukurmoni Oraon relied on her mother-in-law and a TBA during her first pregnancy, while Muno Oraon described herbal massages that relieved dizziness. These accounts illustrate how TBAs embody social trust and symbolic authority.
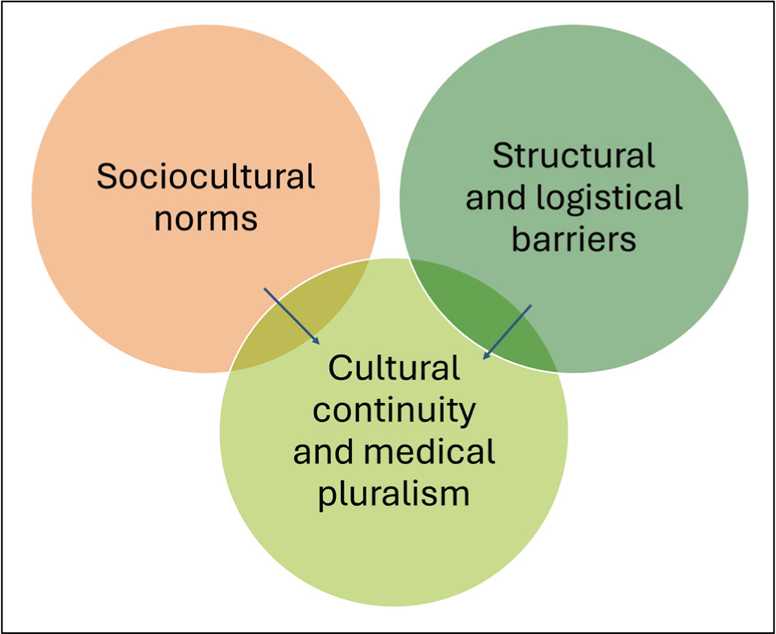
From a theoretical perspective, this reliance need not be treated as an obstacle to modern healthcare. Instead, the concept of medical pluralism (Kleinman, 1980) offers a solution: by recognizing the coexistence of biomedical and traditional systems, maternal healthcare can be made more effective through collaboration rather than replacement. A pluralistic approach accepts that women often value TBAs for emotional, social and cultural reasons, while also recognizing the life-saving potential of biomedical interventions. Critical medical anthropology strengthens this solution by showing that maternal health behaviours are embedded in structural and household hierarchies. Formal collaboration—such as training TBAs to identify risk and refer cases—can bridge these hierarchies, ensuring timely biomedical intervention without undermining the trust and social support that TBAs provide (Figure 1).
Conceptual Framework Showing the Interaction Between Traditional and Biomedical Maternal Healthcare Practices.
Ritual-sensitive Practices
Pregnancy among the Oraon is saturated with rituals that provide both physical healing and symbolic protection. Oraon women emphasized dietary rules that strengthened their body and kinship bonds. Taboos—such as avoiding funerals or storms—express culturally encoded anxieties around vulnerability. Following Geertz’s interpretive anthropology, these are not arbitrary customs but symbols that make experience intelligible, providing women with frameworks to navigate uncertainty. Scheper-Hughes and Lock’s embodiment lens shows how these values are literally inscribed onto the body. CMA adds that ritual practices can also be seen as subtle acts of resistance to biomedical dominance, asserting the relevance of cultural worlds even under structural inequality.
Taken together, these perspectives suggest that maternal healthcare interventions should adopt a ritual-sensitive approach. By acknowledging the symbolic and embodied significance of such practices, programmes can integrate biomedical safety with cultural legitimacy, ensuring that women’s lived realities are not undermined but strengthened.
Community Health Mediation
Accessing biomedical care often requires negotiation across household hierarchies. CMA situates this within structural violence and the political economy of health, showing how poverty, gender inequality and kinship authority constrain maternal autonomy. Geertz’s perspective clarifies why mediation matters: in the Oraon context, health advice gains traction only when embedded in shared symbols and narratives that families recognize as legitimate. Thus, community workers are not simply ‘health messengers’ but translators of meaning, whose symbolic reassurance activates trust—what biomedicine might call ‘placebo’, but which anthropologists recognize as cultural efficacy.
Together, these perspectives show that community health workers are more than conveyors of medical information. Their effectiveness lies in their ability to negotiate household dynamics and present care in culturally meaningful ways. Recognizing and strengthening this mediating role can make maternal healthcare both structurally feasible and socially acceptable.
Conclusion
This research sheds light on the changing dimensions of maternal healthcare practices among the Oraon community in Jalpaiguri district, West Bengal, demonstrating a dynamic interaction between traditional customs and modern medical services. While a growing number of women are turning to institutional healthcare, many continue to rely on indigenous knowledge and TBAs due to cultural beliefs, financial challenges and geographical barriers. This dual reliance reflects what Kleinman (1980) terms the coexistence of distinct ‘healthcare sectors’—the popular and folk sectors—where explanatory models rooted in cultural meaning often guide maternal care decisions more than biomedical logic. Geertz’s (1973) view of culture as ‘webs of significance’ further helps us understand how these practices are not just choices but also deeply embedded symbolic actions.
The findings suggest that maternal healthcare choices are shaped by a combination of socio-economic conditions, access to medical facilities and deeply ingrained cultural traditions. In rural areas, inadequate transportation, limited healthcare infrastructure and economic difficulties remain significant obstacles to institutional maternal care. Many women still prefer traditional childbirth methods, viewing them as an essential part of their maternal experience. This aligns with Davis-Floyd’s (2004) argument that childbirth, whether traditional or institutional, is a culturally constructed rite of passage, and for many women, traditional practices offer emotional safety, symbolic continuity and communal affirmation. In contrast, urban women show greater acceptance of modern biomedical interventions, with higher rates of antenatal visits and institutional deliveries. However, financial limitations persist as a common factor influencing healthcare decisions across both rural and urban settings.
The study also highlights a gradual shift in maternal health awareness within the Oraon community. Increased outreach by healthcare workers has led to growing acceptance of antenatal care, hospital deliveries and post-natal services. Despite these advancements, some long-standing cultural beliefs and rituals related to pregnancy and childbirth continue to shape maternal healthcare behaviours. While these traditions provide emotional and social support, they may sometimes delay or hinder timely medical assistance. To improve maternal healthcare access for Oraon women, a comprehensive approach that respects cultural traditions while promoting modern medical care is essential. Strengthening healthcare infrastructure, enhancing transportation networks and implementing community-based awareness programmes can help bridge the gap between traditional and institutional healthcare systems. Moreover, fostering education and financial independence among tribal women can empower them to make well-informed maternal healthcare decisions. Ultimately, this study emphasizes the need for culturally inclusive maternal healthcare policies that integrate indigenous practices with scientifically proven medical interventions. By valuing traditional healthcare knowledge while ensuring better access to institutional facilities, a more effective and equitable maternal healthcare framework can be developed for the Oraon community and similar indigenous populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.