
Abstract
Background:
The prevalence of hallux valgus is up to 22% in Asia, making it the second-highest in the world. Iatrogenic transfer metatarsalgia is a known complication of hallux valgus correction from excessive shortening of the first metatarsal. Most studies show that first metatarsal shortening should be less than 4.0 mm to avoid such complications. This study aims to compare the risk of first metatarsal shortening, radiologic, and clinical outcomes among surgical procedures used to treat symptomatic hallux valgus.
Methods:
A retrospective study was conducted at a single tertiary hospital using data on patients who underwent minimally invasive metaphyseal extra-articular transverse and Akin osteotomy (META), Lapidus, and scarf procedures. Radiologic outcomes collected include the hallux valgus angle (HVA), intermetatarsal angle (IMA), and first metatarsal shortening measured using the Maestro method. The visual analog scale (VAS) was used to evaluate improvement in patients’ symptoms. Analyses were performed using IBM SPSS version 25.0
Results:
A total of 134 feet were included in this study, with 66 META, 37 Lapidus, and 31 scarf procedures performed. All 3 techniques demonstrated significant improvements in VAS, HVA, and IMA compared with their preoperative measurements (P < .05). In terms of first metatarsal shortening, both META and Lapidus were significantly less than that of scarf (P < .05). In our study, both META and Lapidus demonstrated the least first metatarsal shortening. A significant first metatarsal shortening of more than 4 mm was observed in 7 cases who underwent scarf, whereas none were observed in the META and Lapidus groups.
Conclusion:
All 3 surgical techniques have been shown to provide adequate correction of hallux valgus deformity. Based on our study, scarf has the highest risk of radiologic metatarsal shortening among the 3 procedures, which may potentially lead to transfer metatarsalgia. Care should be taken during the scarf procedure to minimize shortening of the first metatarsal.
Keywords
Introduction
Hallux valgus is one of the most commonly treated forefoot deformities, and its prevalence in Asia remains among the highest worldwide. 1 More than a hundred surgical techniques have been documented for the management of symptomatic hallux valgus, with scarf, Lapidus, and various keyhole procedures, including the third-generation minimally invasive chevron and Akin (MICA) described by Redfern and Vernois, 2 and the fourth-generation minimally invasive technique that involves a metaphyseal extra-articular transverse osteotomy (META) as described by Lam et al, 3 being particularly prominent. 4
The current literature reports complication rates ranging from 10% to 55% for hallux valgus interventions.5,6 Iatrogenic transfer metatarsalgia (ITM), an undesirable complication after hallux valgus surgery, has been cited in current literature to be on average 6.3%,7,8 with higher incidences seen in scarf procedures at around 8.9%. 9 Excessive shortening of the first metatarsal is a leading cause of ITM. Various studies have shown that shortening of more than 4 mm between the first and second metatarsal heads should be avoided to minimize the risk of painful transfer metatarsalgia.9 -11
To date, there is a paucity of studies examining the prevalence of first metatarsal shortening across different methods of hallux valgus correction, particularly in Asian populations. This study aims to compare the extent of first metatarsal shortening and radiologic outcomes across 3 of the most performed procedures for the management of symptomatic hallux valgus.
Methodology
Three surgical methods for hallux valgus correction performed at our center, which include (1) fourth-generation MIS hallux valgus surgery (ie, META), (2) scarf and Akin osteotomy, and (3) Lapidus, are described below.
Fourth-Generation MIS Hallux Valgus Surgery—META
This form of fourth-generation percutaneous bunion surgery involves performing a distal first metaphyseal extra-articular transverse osteotomy using a 2.0 × 20-mm Shannon burr, followed by a multiplanar rotational deformity correction through an adequate shift of the distal metatarsal fragment.3,12,13 The correction is held rigidly by 2 fully threaded screws. The direction of osteotomy is typically angled perpendicular to the metatarsal shaft but may also be angled slightly, distally, or proximally to prevent overshortening or lengthening, respectively. Also, care must be taken to avoid excessive dorsiflexion or plantarflexion of the distal fragment to prevent transfer metatarsalgia or painful first ray, respectively. Intraoperative radiographs should be used after the osteotomy shift to ensure appropriate alignment of the metatarsal shaft. An Akin procedure using a 2.0 × 12-mm Shannon burr is then performed where a medial closing wedge osteotomy is made over the first toe proximal phalanx. This is followed by an optional minimally invasive lateral release procedure to achieve the final desired correction.
Scarf and Akin Procedure
In this procedure, a Z-shaped osteotomy is performed over the first metatarsal bone.14,15 The distal fragment is laterally translated, and the metatarsal head is rotated to correct the bunion deformity. This correction is likewise held with 2 interfragmentary screws. An Akin procedure, as well as the modified McBride procedure, may be added to achieve the final desired correction.
Lapidus Procedure
In this procedure, the incision and corrections are made more proximally at the level of the first tarsal-metatarsal joint (TMTJ).16,17 The TMTJ is identified, and the articular surfaces are prepared with the removal of cartilage and soft tissue. The first and second metatarsal shafts are reduced to correct the deformity. Arthrodesis of the first TMTJ is then performed with the use of a plate-and-screw construct to hold the correction. Bone grafts may be used to promote fusion.
Data collection
Institutional review board approval was obtained before the start of the study.
A retrospective study was conducted using data from a single tertiary hospital, involving 134 feet who underwent either a META, scarf, or Lapidus procedure (Table 1). The indications for surgery were symptomatic hallux valgus that had failed conservative treatments.
Breakdown of Cases.
Abbreviation: META, metaphyseal extra-articular transverse osteotomy.
The inclusion criteria were patients who underwent hallux valgus surgery and whose data were collected in our Orthopedic Diagnostic Center database. This study excluded patients with rheumatic arthritis, traumatic hallux valgus, and recurrent hallux valgus. All patients were assessed by an independent allied health staff preoperatively and at 6 months postoperatively. Patient demographic data were collected, including age, gender, and body mass index.
Clinical outcomes were measured using VAS scores. Radiologic measurements included pre- and postoperative weight-bearing views of the affected foot, and the parameters assessed were hallux valgus angle (HVA), intermetatarsal angle (IMA), and first metatarsal shortening.
On anteroposterior radiographs of the foot, all 3 values were measured. HVA was measured as the angle between the long axis of the first metatarsal and the long axis of the proximal phalanx. IMA was measured as the long axis of the first and second metatarsal bones.
First metatarsal shortening was measured using the Maestro method, 18 where, with reference to the long axis of the second metatarsal bone, a perpendicular line was drawn from the distalmost point of the second metatarsal and extended medially toward the first metatarsal. The relative metatarsal length (RML) of the first metatarsal bone was measured from the distal tip of the first metatarsal head to the perpendicular line, parallel to the long axis of the second metatarsal bone. First metatarsal shortening was then calculated as the difference between the relative length pre- and post-correction. A negative value suggested an increase in the relative length of the first metatarsal (Figure 1).
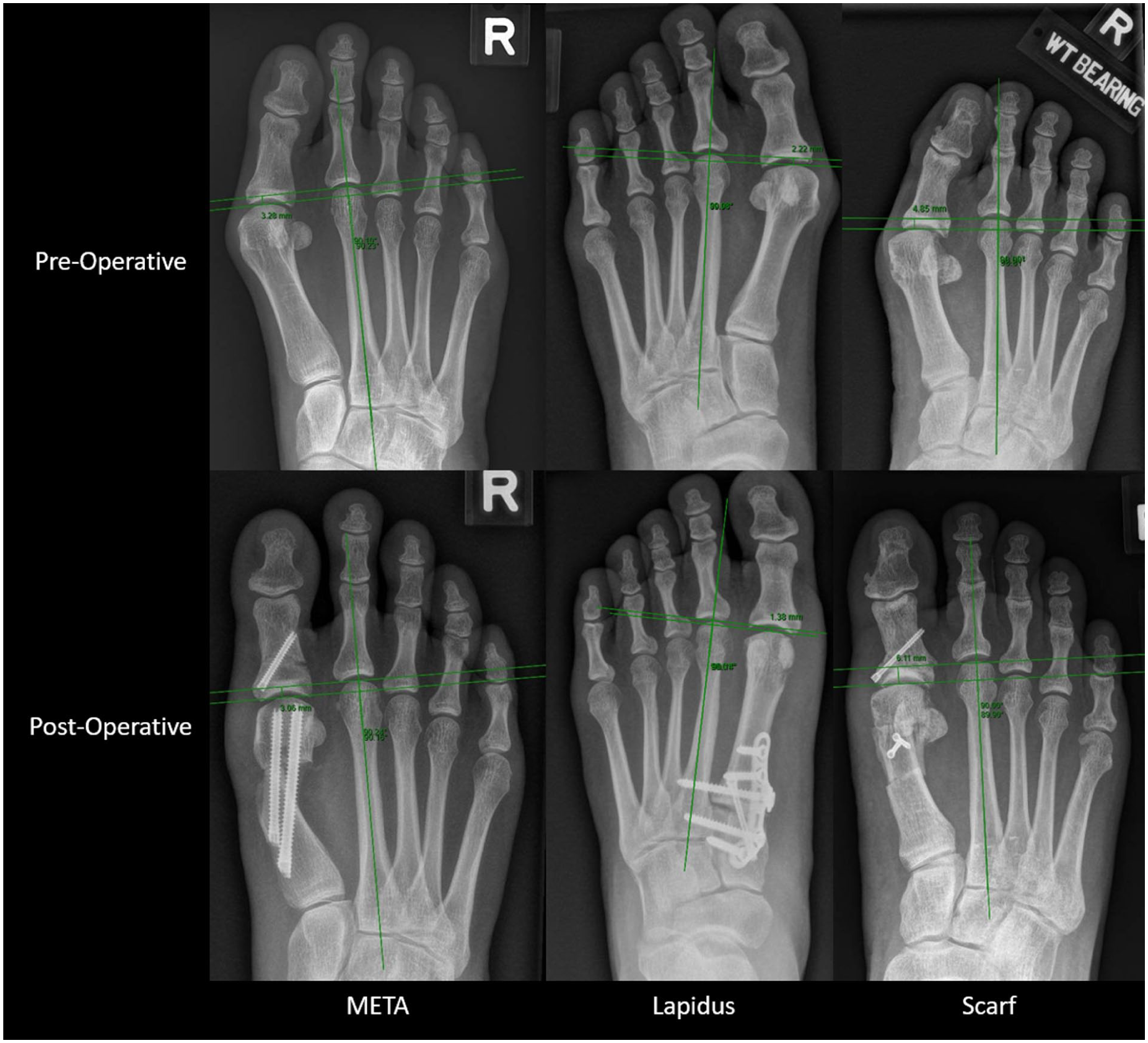
Measurement of first metatarsal shortening via the Maestro method in 3 different hallux valgus correction procedures.
Findings and Results
All analyses were performed using IBM SPSS V.25.0. One-way analysis of variance indicated that there were no significant differences in mean age (P = .250) or body mass index (P = .360) between the 3 groups. The results of the study are shown below (Table 2).
Table of Results.
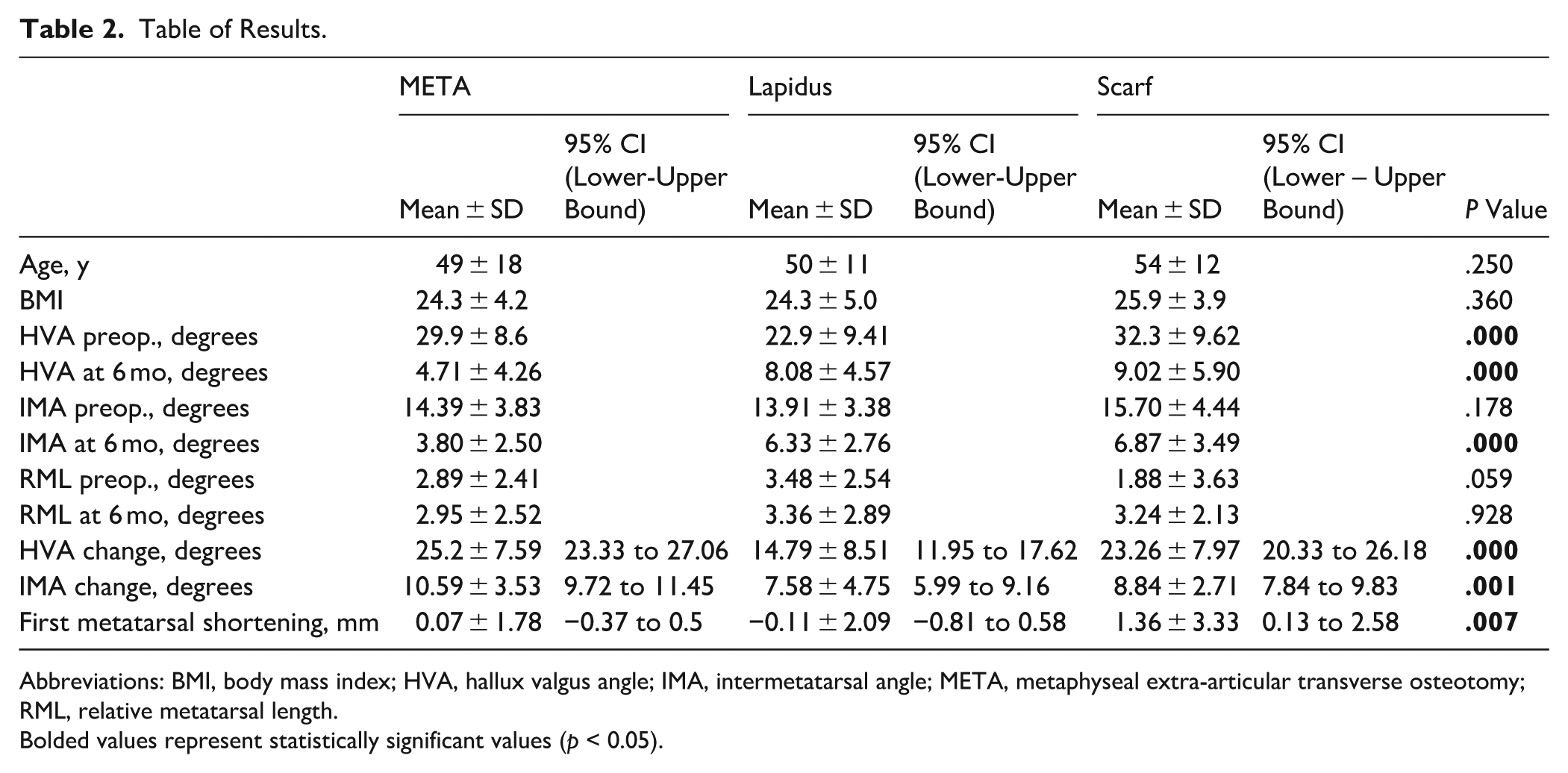
Abbreviations: BMI, body mass index; HVA, hallux valgus angle; IMA, intermetatarsal angle; META, metaphyseal extra-articular transverse osteotomy; RML, relative metatarsal length.
Bolded values represent statistically significant values (p < 0.05).
Radiologic Outcomes
All 3 methods showed a statistically significant improvement in both the HVA and IMA angles (P < .05). In the META group, the mean improvement for HVA and IMA was the greatest among the 3, at 25.2° ± 7.59° (P < .05) and 10.59° ± 3.53°, respectively. In the Lapidus group, the mean improvement for HVA was 14.79° ± 8.51° (P < .05), and IMA was 7.58° ± 4.75°. In the scarf group, the mean improvement for HVA was 23.26° ± 7.97° (P < .05), and IMA was 8.84° ± 2.71°.
A Kruskal-Wallis test was conducted to compare radiologic corrections across the 3 groups and to assess whether improvement differed significantly. Results of the test indicated a significant difference in HVA correction across all 3 procedures, χ2(2) = 31.69, P < .001. The mean rank of HVA correction was 81.59 for META, 37.38 for Lapidus, and 73.45 for scarf. Post hoc comparisons using the Dunn method with a Bonferroni correction indicated that the mean rank HVA correction of Lapidus was significantly lower than that of META (P < .001) and scarf (P < .001). However, there was no significant difference between the mean rank HVA correction of META and scarf (P = .34).
As for IMA correction, the Kruskal-Wallis test indicated a significant difference across the 3 procedures, χ2(2) = 13.96, P < .001. The mean rank of IMA correction was 79.67 for META, 51 for Lapidus, and 61.29 for scarf. Post hoc comparisons using the Dunn method with a Bonferroni correction indicated that the mean rank IMA correction of META was significantly higher than that of Lapidus (P = .00) but not statistically significant when compared to scarf (P = .09). There was no significant difference between the mean rank IMA correction between scarf and Lapidus (P = .83)
First Metatarsal Shortening
The mean first metatarsal shortening was 0.07 ± 1.78 mm for META, −0.11 ± 2.09 mm for Lapidus, and 1.36 ± 3.33 mm for scarf.
The Kruskal-Wallis test indicated a significant difference in first metatarsal shortening across all 3 procedures, χ2(2) = 9.81, P = .01. The mean rank of first metatarsal shortening was 62.67 for META, 60.16 for Lapidus, and 86.55 for scarf. Post hoc comparisons using the Dunn method with a Bonferroni correction indicated that the mean rank first metatarsal shortening of scarf was significantly higher than that of both Lapidus (P = .02) and META (P = .01). However, there was no significant difference between the mean rank first metatarsal shortening between META and Lapidus (P = .75).
Significant metatarsal shortening, defined as more than 4 mm, was observed in 7 patients, all of whom had undergone the open scarf and Akin procedure. No significant metatarsal shortening was observed in either the META or Lapidus groups. However, in this study, we did not investigate whether a threshold of 4 mm shortening is associated with an increased risk of symptomatic transfer metatarsalgia.
Functional Outcomes
All 3 procedures demonstrated significant improvements in preoperative and postoperative VAS scores at 6 months (P ≤ .001). A Kruskal-Wallis test was performed, and no significant differences in postoperative VAS scores at 6 months were found among the 3 procedures, χ2(2) = 0.867, P = .648 (Table 3).
Visual Analog Score.

Abbreviation: META, metaphyseal extra-articular transverse osteotomy.
Discussion
This study found that all 3 procedures were equally effective in correcting hallux valgus deformity, yielding good radiographic improvements and clinical outcomes. Lapidus had the lowest HVA correction potential among the 3. IMA correction potential was greater in META than in Lapidus. Of particular interest is that the scarf procedure showed a significantly greater risk of first metatarsal shortening than the other 2 methods, with 7 patients in the scarf group experiencing shortening of more than 4 mm. META did not show any significant metatarsal shortening even in cases of both moderate and severe hallux valgus (Figure 2). As such, the radiologic risk of excessive shortening leading to iatrogenic transfer metatarsalgia is probably higher with the scarf procedure. Although this study did not evaluate symptomatic metatarsalgia, we opined that the understanding of radiologic risk can mitigate possible causes of iatrogenic transfer metatarsalgia.
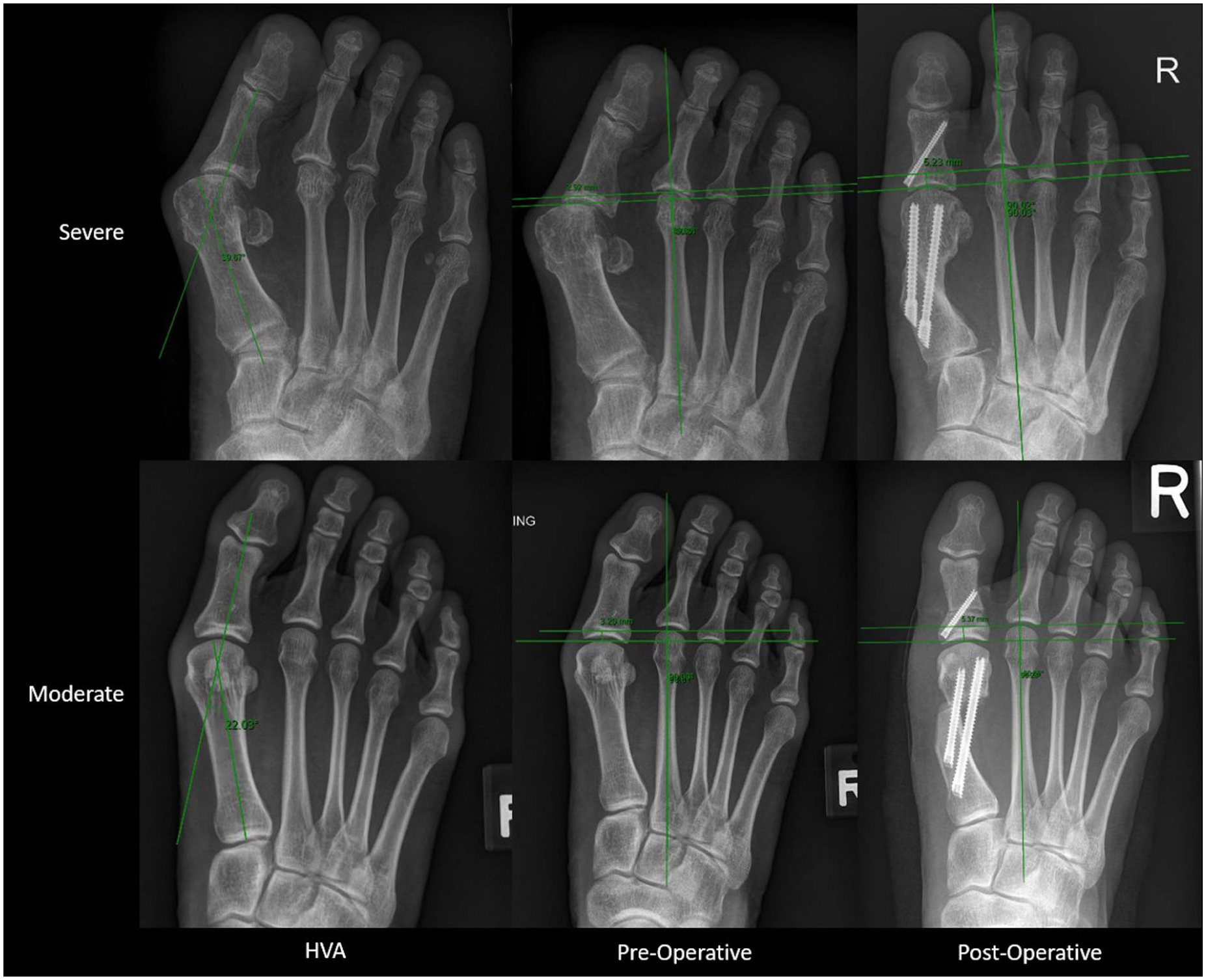
Example of severe vs moderate hallux valgus showing first metatarsal shortening of 2.31 and 2.17 mm, respectively.
Iatrogenic Transfer Metatarsalgia
Iatrogenic transfer metatarsalgia caused by excessive shortening of the first ray is an avoidable complication that may lead to poor outcomes and dissatisfaction among patients.8,19 Although all procedures have the potential to shorten the first ray, minimizing the risk of iatrogenic transfer metatarsalgia requires careful identification of factors inherent to each technique. This approach helps prevent unnecessary shortening and optimizes patient outcomes.
Minimally Invasive Metaphyseal Extra-Articular Transverse and Akin osteotomy (META)
Burr tools used in minimally invasive surgeries may be associated with greater bone loss, up to 3 times that of saw blades. 20 Conventionally, a Shannon burr is used and has a thickness of 2 mm. Hwang et al 21 described a modification using a 1.1-mm Midas burr, with good surgical and functional outcomes. They also emphasized the importance of adequate penetration and bone purchase of the proximal lateral cortical bone, as this significantly reduces the odds ratio for excessive postoperative first metatarsal shortening. Careful consideration of the osteotomy orientation is necessary to achieve the desired correction while avoiding excessive first metatarsal shortening. 22 The authors opined that META resulted in less metatarsal shortening than the other 2 procedures because the osteotomy direction can be angled slightly to maintain the desired length relative to the second metatarsal. In addition, proper handling of the Shannon burr to achieve a single-sweep osteotomy cut is also important for preventing excessive bone loss.
Scarf and Akin Procedure
Several studies have shown that this procedure was associated with significantly greater shortening of the first metatarsal.23,24 However, only a few have examined the biomechanical etiology of first metatarsal shortening in the scarf and Akin procedure.25,26 Law et al 27 describe 2 possible maneuvers to mitigate first metatarsal shortening during surgery. First, with the Kirschner wires being placed perpendicular to the long axis of the first metatarsal instead of the second metatarsal, this may allow lengthening of the first metatarsal on lateral translation of the distal fragment. Second, additional lengthening of the first metatarsal can be achieved by directly translating the distal fragment distally and using a bone graft to fill the gap at the osteotomy site, thereby promoting bony union.
Although the radiologic risk of metatarsal shortening was highest in scarf, we did not demonstrate significantly poorer VAS scores. This apparent paradox may be explained by the study’s short-term follow-up period, suggesting that transfer metatarsalgia, if present, may take longer to manifest. In addition, our use of the VAS score as a surrogate for functional outcome may not be sufficiently sensitive to detect complications of transfer metatarsalgia. Future studies should therefore use other, more sensitive functional outcome measures and a longer-term follow-up duration to determine their correlation.
Lapidus
Several studies corroborate that first metatarsal shortening may be significant with the Lapidus procedure.28,29 This was dependent on the method used to prepare the tarsometatarsal joint for fusion, with some estimates as high as 7.5 mm with osseous resection and 5.0 mm with curettage.17,30,31 To mitigate this, Hatch et al 30 describe the use of a cutting jig to enable precise resection of the first tarsometatarsal joint surfaces, yielding promising results and reducing the mean first metatarsal shortening to 3.1 mm. Other measures discussed in literature include the use of the resected medial eminence as an interpositional autograft together with the Lapidus arthrodesis to achieve bony union and reduction in undesirable first metatarsal shortening. 32 Although not directly linked to first metatarsal shortening, failure to achieve plantarflexion at the arthrodesis during Lapidus arthrodesis has been shown to elevate the first ray, inducing a lateral shift in plantar loading and resulting in transfer metatarsalgia. 28
Limitations
We caveat that the findings are subject to the limitations of this research as listed:
This is a retrospective comparative study with a limited sample size and short follow-up duration, which may limit the generalizability of our results.
This study included only patients whose clinical data were collected by our ODC and may not represent all cases performed at the institution.
There were no intra- or interobserver reliability tests performed for the radiologic outcomes, and only the VAS score was used in our clinical outcome.
The primary outcome studied in this research was radiologic risk of metatarsal shortening, and information of symptomatic transfer metatarsalgia was not available across the study cohort.
The choice of surgical technique used was surgeon-dependent, nonrandomized, and may not always be clearly documented in the operative notes. However, this article aims to focus on comparing each procedure with its risk of metatarsal shortening.
Further studies, including larger population-based or randomized controlled trials, may be conducted to strengthen comparisons across procedures. In addition, specific foot and ankle functional outcome scores should be used, and complications, including symptomatic transfer metatarsalgia, should be collected and investigated in subsequent studies.
Conclusion
All 3 surgical techniques showed significant correction of hallux valgus deformity. Our findings in the Asian population corroborate with the current European literature, indicating that the scarf procedure has the highest radiologic risk of first metatarsal shortening among the 3 procedures.24,33 Consequently, we recommend incorporating additional care and planning when performing the scarf procedure to minimize shortening of the first metatarsal.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261445962 – Supplemental material for Comparison of Radiographic Outcomes and Risk of First Metatarsal Shortening Between different Hallux Valgus Surgeries: An Asian Perspective
Supplemental material, sj-pdf-1-fao-10.1177_24730114261445962 for Comparison of Radiographic Outcomes and Risk of First Metatarsal Shortening Between different Hallux Valgus Surgeries: An Asian Perspective by Bryan Hon Keng Pui, Teddy Cheong Yao Wen, Png Wenxian, Inderjeet Singh Rikhraj and Eric Cher Wei Liang in Foot & Ankle Orthopaedics
Footnotes
Ethical considerations
This is a retrospective study with deidentified patient data. Reference number for the ethical approval: CIRB 2020/2381.
Consent for publication
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to personal data protection laws.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.