
Abstract
Background:
Lisfranc injuries are challenging presentations frequently encountered by foot and ankle and trauma surgeons, with no definitive consensus regarding the optimal fixation technique. This study aimed to evaluate the safety and efficacy of a modified stabilisation technique combining tarsometatarsal joint (TMTJ) bridge plating with a suture tape-endobutton construct for Lisfranc joint stabilisation, using patient-reported outcomes in a cohort of patients with acute injuries.
Methods:
A retrospective review was performed on 20 consecutive patients with acute Lisfranc injuries treated with open reduction and internal fixation (ORIF). Fixation involved TMTJ bridge plating and stabilisation of the Lisfranc interval using a suture tape-endobutton construct spanning the medial cuneiform (C1) and the base of the second metatarsal (M2). All patients underwent planned removal of bridge plates with retainment of the suture tape construct. Pre- and postoperative visual analogue scale (VAS) scores and American Orthopaedic Foot & Ankle Society (AOFAS) midfoot scores were collected, along with postoperative complication and reoperation rates.
Results:
The cohort comprised 9 males (45%) and 11 females (55%). Time to surgery ranged from 1.5 to 12 weeks. Mean follow-up was 31.8 months (range 12-61 months). At final follow-up, 18 of 19 patients (95%) who exercised preoperatively reported return to regular exercise or sporting activity. Mean AOFAS scores improved from 32.1 ± 19.9 preoperatively to 90.6 ± 9.4 postoperatively, and VAS scores improved from 6.2 ± 2.2 to 1.6 ± 0.8. There were no cases of unplanned reoperation, recurrent radiographic diastasis, or conversion to arthrodesis.
Conclusion:
Our study of combined TMTJ bridge plating and suture tape ligament augmentation provides preliminary evidence of safety and efficacy for acute Lisfranc injuries in a small retrospective series. It appears to be a safe and effective technique for acute Lisfranc injuries, demonstrating favorable patient-reported outcomes and maintenance of reduction at intermediate follow-up. The suture tape construct minimises transarticular instrumentation and may reduce iatrogenic articular injury, potentially lowering the risk of midfoot stiffness, pain, and posttraumatic arthrosis.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
Lisfranc injuries are often underdiagnosed and span high-energy mechanisms such as motor vehicle accidents to low-energy injuries in the athletic population.5,27,28,32,38,40 The latter, being the primary patient population of the present study, is often associated with purely ligamentous or low-grade bony pathology. A confirmed unstable Lisfranc injury typically serves as an indication for surgery; however, the optimal surgical technique remains the topic of debate.12,18,22,33,34 Traditionally, fixation has been achieved with transarticular screws, with subsequent popularisation of dorsal bridge plating and, more recently, flexible stabilisation techniques.2,3,22
Transarticular screw fixation remains a mainstay of treatment but carries risks including iatrogenic chondral damage, screw breakage, and recurrent displacement with hardware retention, as well as possible fracture following screw removal where hardware removal is undertaken.2,7 Reported rates of unplanned hardware removal, where not routinely performed, may be as high as 21%. 37 Advantages include lower cost and less soft tissue trauma. Dorsal bridge plating avoids chondral injury and is more suitable for managing comminuted fractures, although it requires a more extensile approach.13,39
There is a paucity of literature evaluating outcomes following flexible stabilisation techniques such as suture button constructs. Biomechanical studies demonstrate that suture button techniques have adequate restraint against diastasis with stability comparable to screw fixation.1,29,30 Cho et al 6 reported comparable American Orthopaedic Foot & Ankle Society (AOFAS) outcomes between suture button and screw fixation cohorts. Early single and dual suture button techniques (Figures 1 and 2) have demonstrated risks of creep and loss of stability. 41 Our study incorporates a third-generation technique using interference screw fixation within C1 and cortical endobutton fixation on M2, with optional intercuneiform stabilisation between C1 and C2.16,41 This approach may reduce implant subsidence while maintaining stability across the Lisfranc interval, although residual TMTJ instability remains a concern. Accordingly, we utilise a hybrid construct combining flexible ligament reconstruction with TMTJ bridge plating. We hypothesise this technique is safe and provides high functional outcomes with low complication rates.

Series of plain radiographs and a clinical photo demonstrating a single suture button technique (first-generation) for Lisfranc fixation. (A) Under fluoroscopic guidance, a reduction clamp was applied to reduce the interval between C1 and M2. (B) A guidewire was passed across the Lisfranc joint. (C) For fixation, an oblong button was positioned on the medial aspect of C1, and an endobutton was secured to the lateral cortex of the base of M2. Reproduced from Yi and Chaudhari, 41 used under the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).

Plain radiograph showing creep subsidence of the medial button and loss of reduction of the Lisfranc interval. Reproduced from Yi and Chaudhari, 41 used under the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Methods
We retrospectively analysed patients who underwent surgical fixation of Lisfranc injuries at a single hospital by a single fellowship-trained foot and ankle orthopaedic surgeon between June 2019 and September 2023, identified using relevant MBS codes in the surgeon’s database. Patients with a minimum 1-year follow-up were included, yielding a total of 27 patients with 27 Lisfranc injuries. All cases involved a low-energy injury mechanism in active patients, resulting in primarily ligamentous or low-grade bony Lisfranc injuries with avulsion fragments. Instability was defined by Lisfranc interval diastasis and/or TMTJ incongruity, including dynamic instability confirmed by weight-bearing imaging (bilateral radiographs and/or weight-bearing CT). Lisfranc interval diastasis was defined as asymmetry when compared with the contralateral foot.
All patients were referred via their local general practitioner or allied health practitioner. No presentations involved high-energy trauma, polytrauma, or acute midfoot dislocation. A summary of patient demographics, mechanisms of injury, associated injuries, and imaging findings is provided (Table 1).
Summary of the Patients Included in This Study Including Their Mechanisms of Injury, MRI Grading of Lisfranc Ligament Injury if Performed, and Associated Fractures Based on Weight-Bearing Radiograph or CT.
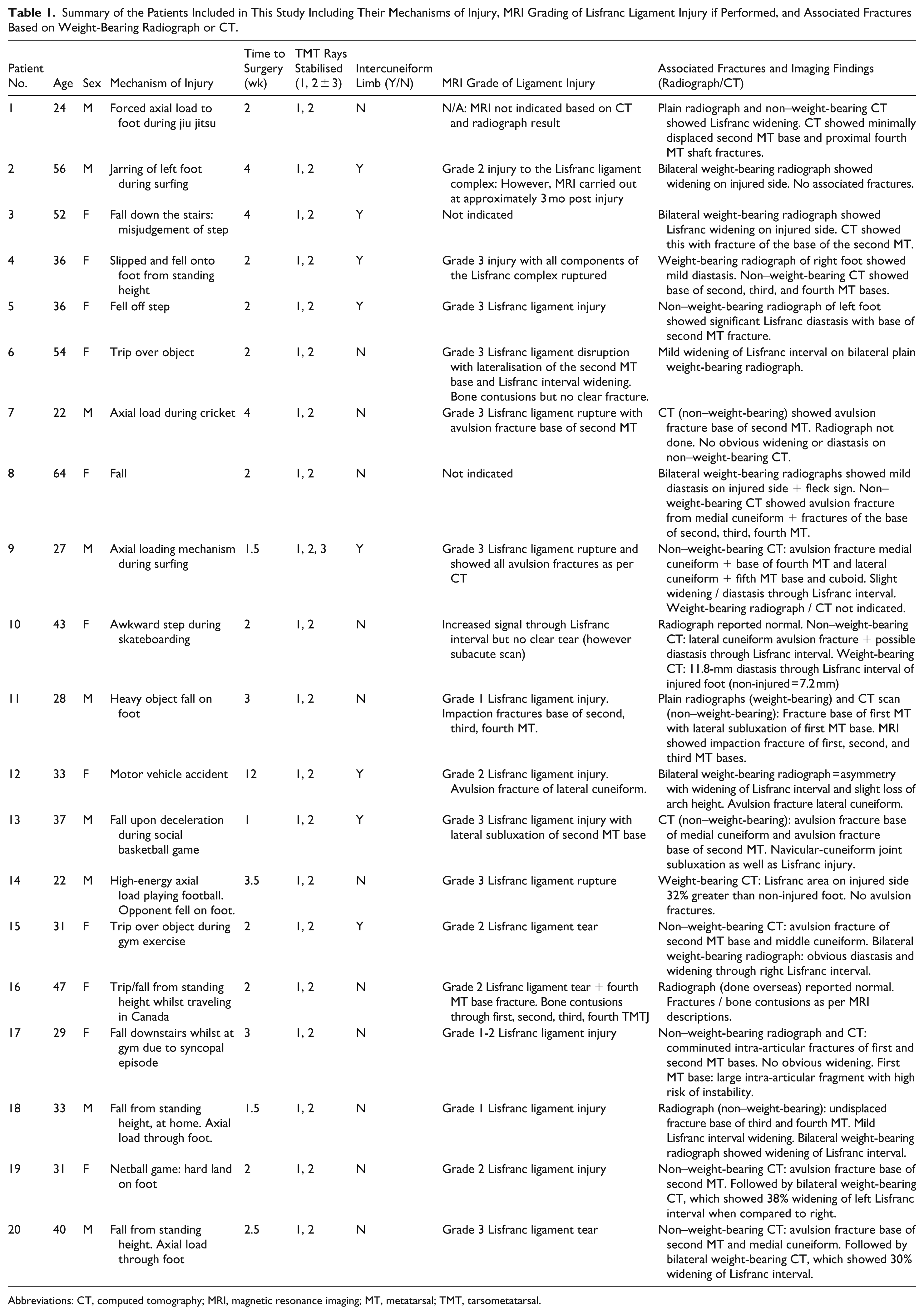
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; MT, metatarsal; TMT, tarsometatarsal.
Three patients were excluded as they underwent transarticular screw fixation because of delayed presentation (>4 months postinjury), where preoperative imaging demonstrated Lisfranc interval diastasis that was not readily reducible when comparing weight-bearing and non-weight-bearing images. These cases required formal open reduction with resection of interposed scar tissue. Arthrodesis was considered; however, primary fixation was undertaken following discussion regarding the risk of posttraumatic arthrosis and potential need for further surgery. A further four patients were lost to follow-up, leaving 20 patients meeting inclusion criteria. This cohort comprised 9 males (45%) and 11 females (55%), with a mean age of 37.3 years (range, 22-64 years) and a mean follow-up duration of 31.8 months (range, 12-61 months). The mean time from injury to surgery was 2.9 (range, 1.5-12) weeks. All patients provided informed consent. Primary arthrodesis was considered for subacute cases, including one patient who presented for surgery at close to 12 weeks post-injury. This outlier was selected for the hybrid technique, following an appropriate consenting process, due to the fact that pre-operative imaging confirmed diastasis only during weight-bearing and normal alignment at rest. Institutional ethics approval was obtained (ID: 23038), and the study was conducted in accordance with the Declaration of Helsinki.
Surgical technique
Diagnosis was established using clinical assessment, MRI, weight-bearing radiographs, and CT imaging (including weight-bearing CT) where indicated. MRI was frequently utilised given the predominance of ligamentous injury patterns. Instability was confirmed by static or dynamic Lisfranc interval diastasis compared with the contralateral foot. All acute presentations with confirmed instability were considered suitable for the hybrid fixation technique described. A preoperative radiograph is shown in Figure 3.

Plain radiograph showing a patient included in the study who sustained a primarily ligamentous Lisfranc injury.
The surgical approach involved either a single dorsal incision centred over the second ray or dual incisions incorporating a dorsal incision, biased slightly laterally, with a direct medial approach to the 1st TMTJ. Titanium alloy locking plates were used to bridge unstable tarsometatarsal joints, with 3.5 mm screws preferred unless anatomy dictated use of 2.7 mm screws (Paragon28). The lateral column, consisting of the cuboid and fourth/fifth rays, was not routinely stabilised.
Following reduction and stabilisation of the medial and middle columns, the Lisfranc joint was reduced using a bone reduction clamp. A 1.6 mm Kirschner wire (K wire) was passed across the Lisfranc joint from the medial cortex of C1 to the lateral cortex of the M2 base under fluoroscopic guidance using a triangular fibrocartilage complex (TFCC) aiming guide. No further drilling across Lisfranc joint was performed, thereby limiting articular violation to 1.6 mm. Suture tape (ultra-high molecular weight polyethylene) was shuttled along this trajectory.
Lateral fixation was achieved with a cortical endobutton on M2. Medial fixation was achieved using a bio-absorbable interference screw (3.5 or 4.75 mm) in C1 to a depth of approximately 13 mm (Arthrex). In cases of confirmed intraoperative intercuneiform instability, or where static Lisfranc diastasis was evident on preoperative imaging, a suture tape limb was passed from the medial cortex of C1 dorsally, deep to neurovascular structures, and secured into C2 or C3 using a second interference screw. Representative intraoperative and postoperative imaging, as well as schematic illustrations, are provided (Figures 4-7).

Series of intraoperative image intensifier films of the same patient who has undergone surgery using the described technique.

Series of plain radiographs showing the same patient day 1 postoperative.
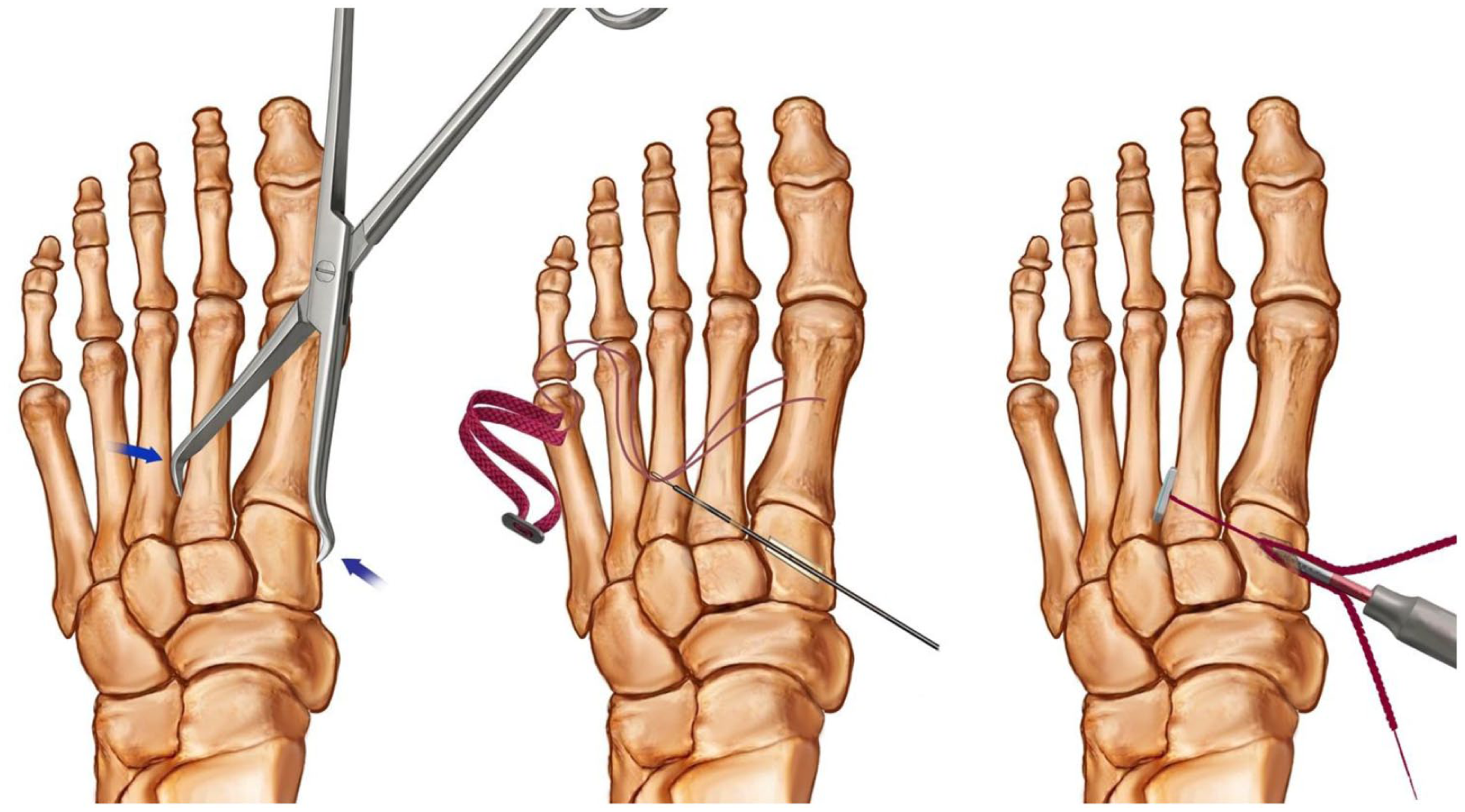
Series of schematics showing the reduction manoeuvre, drilling of Lisfranc interval using a 1.6-mm Kirschner wire, passing of the suture button construct through the Lisfranc interval, and securing the medial end with an interference screw.

Figure shows the technique whereby an intercuneiform limb of suture tape is passed dorsally over the C1-C2 interval and inserted via an interference screw into C2 or C3.
Postoperative Management
Patients were followed up clinically and radiographically at 2 weeks, 8 weeks, 3 months, 6 months, and 12 months at minimum. Radiographic parameters assessed included the distance between base of M1 and M2 (diastasis defined as ≥2 mm), and incongruity between the medial margin of the M2 base and medial margin of C2. Serial imaging was used to assess maintenance of reduction.
The postoperative protocol consisted of immobilisation in a posterior plaster splint for 2 weeks, followed by a controlled ankle motion (CAM) boot. Patients remained non–weight-bearing for 8 weeks, followed by progressive weight-bearing in the CAM boot. Thromboprophylaxis was administered for 6 weeks postoperatively.
Elective removal of bridge plates was performed at 14-16 weeks, with retention of the suture tape construct. At the time of this second procedure, stability of the Lisfranc joint was assessed under fluoroscopic guidance before wound closure. This protocol aligns with contemporary evidence supporting 6-8 weeks of non–weight-bearing followed by hardware removal at 3-6 months, although hardware retention strategies have also been described. A radiograph demonstrating Lisfranc interval stability post removal of bridge plates at 5 years, for the same patient, is shown in Figure 8.

Series of plain radiographs showing the same patient at 5-year follow-up after removal of tarsometatarsal bridge plates but retaining the suture button, demonstrating maintained reduction of the Lisfranc interval.
Clinical Outcomes
Clinical outcomes were analysed with the AOFAS midfoot score, VAS, as well as a sports participation questionnaire. The authors acknowledge that preoperative functional / pain scores have limited utility in a trauma setting. However, in the context of low-energy Lisfranc injuries whereby the initial diagnosis is missed in up to 20% of cases, and such patients attempt to persist with symptomatic management, we feel that these preoperative scores provide some baseline indication in relation to the severity of foot dysfunction.5,27,28
Any complications experienced by patients were also noted.
Sports and Physical Activities
Sports and physical activities were assessed with a similar questionnaire to that used by Mora et al. 26 We designed a 12-item sports questionnaire requiring patients to describe the exercise and sporting activities they participated in pre- and postoperatively and the frequency (times per week). Patients were also asked to record the difference between pre- and postoperative sporting ability, with responses being “no difference,” “mild difference,” “moderate difference,” and “significant difference.” Patients were also able to answer “yes” or “no” with respect to any restriction of activity postoperatively compared to preoperatively. Patients were able to provide “yes/no” answers to whether their foot felt unstable or weak when walking and exercising.
Statistical Analysis
Statistical analysis was performed using R (R Foundation for Statistical Computing, Vienna, Austria). The Shapiro-Wilk test was used to determine whether variables were normally distributed. When comparing the pre- and post-measurements, the paired t test was used when the normality assumption held; otherwise, the nonparametric Wilcoxon signed-ranks test was used. To compare postoperative outcomes across gender, age, and time to surgery, independent t tests were conducted for normally distributed variables, whereas the Mann-Whitney U test was applied when the assumption of normality was not met. All tests were performed at a 5% level of significance.
Results
Demographics
Of the 20 Lisfranc injuries, consisting of 9 male (45%) and 11 female patients (55%), low-speed motor vehicle accidents accounted for 1 injury (5%). Sporting injuries or injuries during exercise occurred in 7 patients (35%) and represented the most common mechanism. Two patients were smokers. There were no diabetic patients or patients with clinical or known radiologic evidence of peripheral vascular disease.
Sports Questionnaire
Nineteen patients participated in physical activity or sports on a weekly basis preoperatively (Table 2). Prior to injury, patients engaged in 43 different activities—ranging from low-impact exercise such as walking and swimming to high-impact pursuits such as running and basketball—whereas postoperatively they participated in 33 activities. The most common activities were walking, gym/weights, and cycling. Eighteen of nineteen (95%) patients who exercised preoperatively had returned to some level of physical activity at 1 year postoperatively. The frequency of exercise remained similar postoperatively (3.8 ± 2.0 times a week) compared with preoperatively (4.1 ± 1.8 times a week) (P = .49). Of the 3 patients who increased their frequency of exercise, 2 transitioned to lower impact activity. One patient (5%) ceased all sporting activity due to residual symptoms. This patient’s functional assessment occurred at 12 months postinjury, with radiographic assessment confirming stable anatomical alignment. The patient’s main reported limitation, at 12 months, was pain/clicking in the ipsilateral knee. At subsequent follow-up (18 months), the patient progressed to jogging with no residual foot symptoms.
Frequency of Preinjury and Postoperative Exercise.
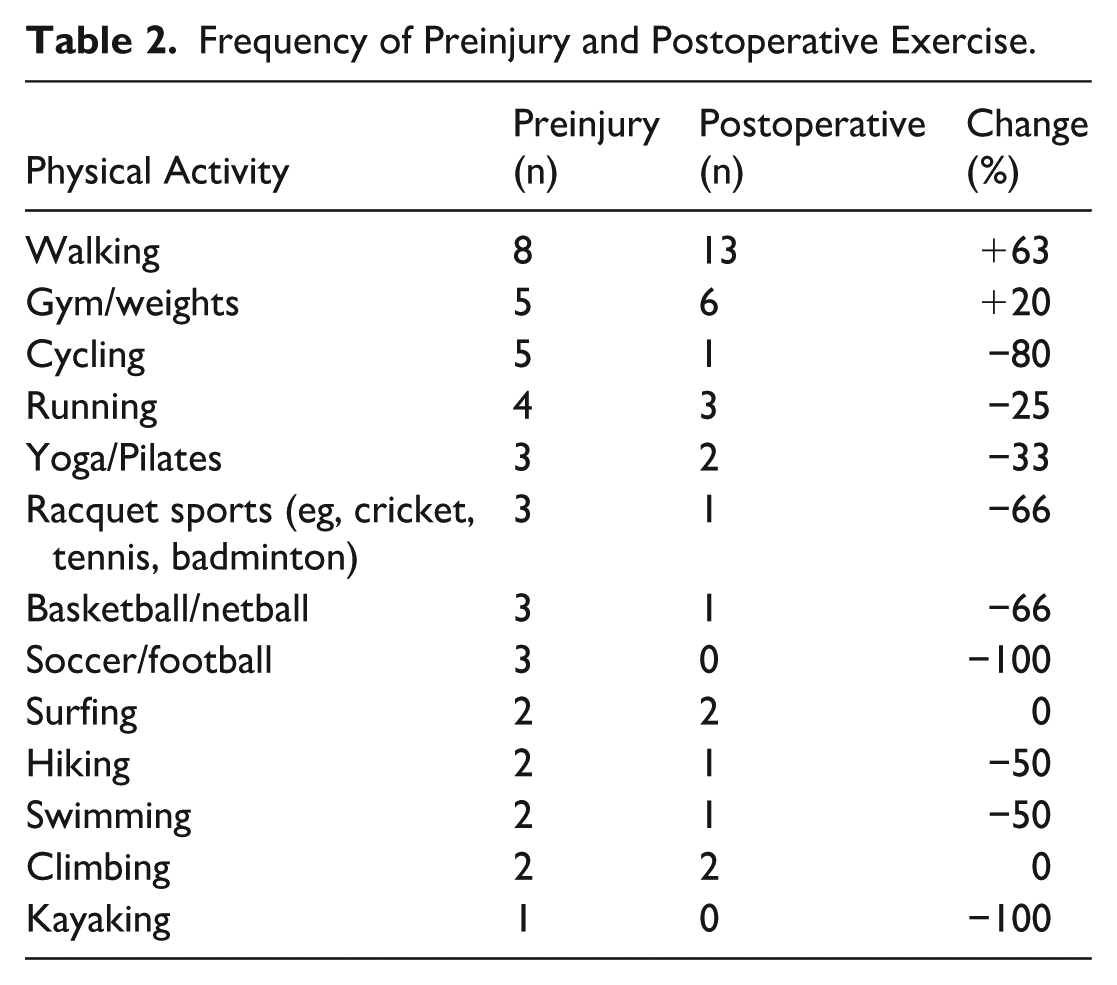
Five patients (25%) noticed no difference in sporting ability compared with their preinjury capacity. Three patients (15%) reported a moderate difference, whereas the remainder of the patients reported a mild difference. Eight patients (40%) reported a sensation of weakness or instability when exercising.
Preoperative visual analogue scale (VAS) scores were 6.2 ± 2.2, improving to 1.6 ± 0.8 (P < .001) postoperatively.
AOFAS Midfoot Score
The mean AOFAS score improved from 32.1 ± 19.9 to 90.6 ± 9.4 postoperatively (P < .001). Using the grading system of the AOFAS scores, 12 injuries (60%) were classified as excellent (AOFAS ≥ 90), 7 (35%) as good (AOFAS 75-89), 1 (5%) as average (AOFAS 50-74) and none as poor (AOFAS ≤ 49). Pain, function, and alignment subscores improved from preoperative levels of 14.5 ± 11.9, 11.1 ± 10.5, and 6.5 ± 6.6 to 33.5 ± 5.9, 42.1 ± 4.6, and 15.0 ± 0 postoperatively, respectively (P < .001).
With the numbers available, no significant differences could be detected between gender, age (cutoff 40 years: Table 3), or time to surgery at cutoff of 2 weeks, consistent with Graef et al 14 (Table 4).
Outcome Scores by Gender and Age. a
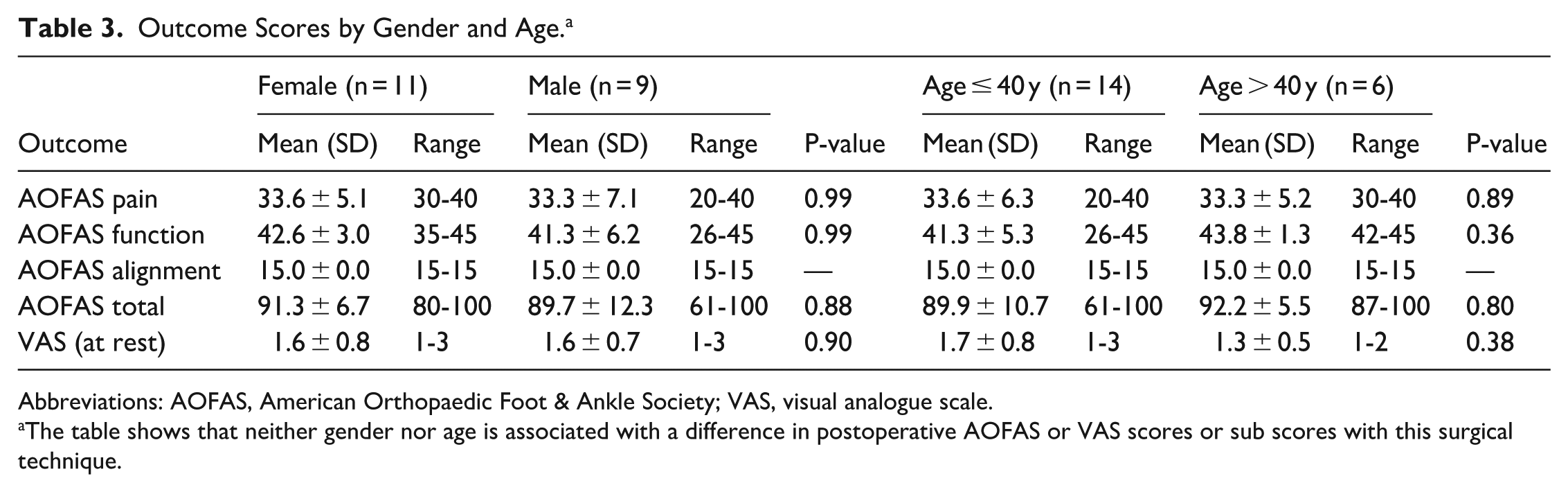
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; VAS, visual analogue scale.
The table shows that neither gender nor age is associated with a difference in postoperative AOFAS or VAS scores or sub scores with this surgical technique.
Outcome Scores by Time to Surgery. a
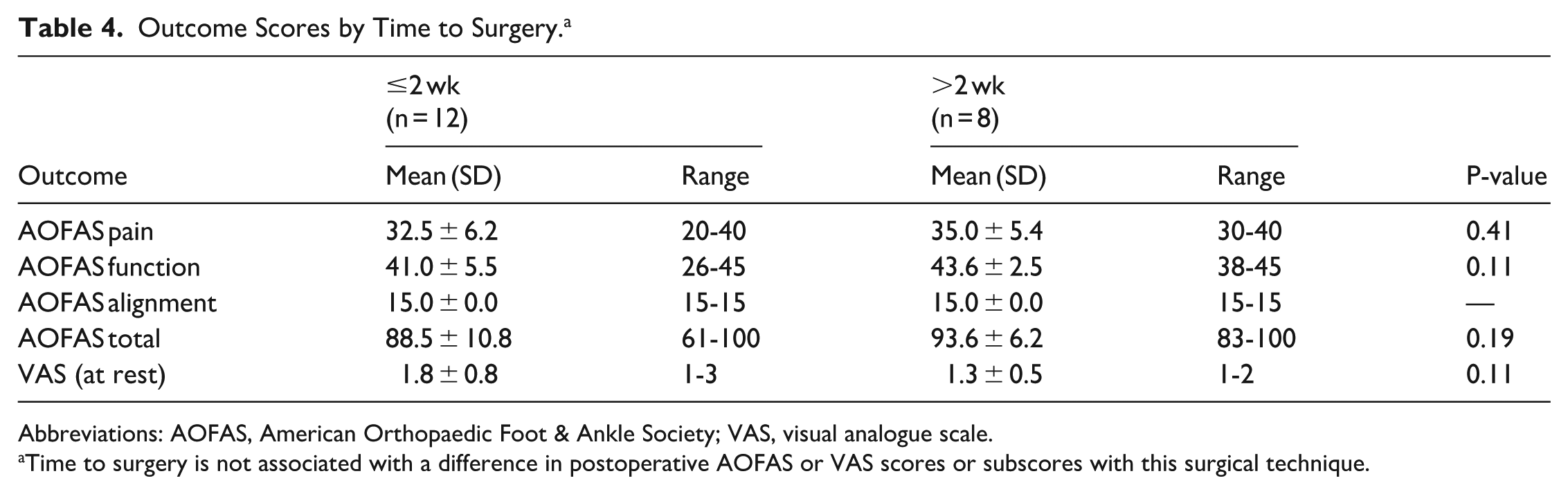
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; VAS, visual analogue scale.
Time to surgery is not associated with a difference in postoperative AOFAS or VAS scores or subscores with this surgical technique.
Complications
We report 1 case of delayed medial wound healing requiring oral antibiotics, which resolved without further surgery. Two patients were prescribed oral antibiotics by their general practitioner for presumed superficial infection; however, there was no objective evidence of infection when assessed by the surgeon at 8 weeks postoperatively. One patient experienced transient regional hypersensitivity, resolving by 6 months.
No cases of malunion, loss of reduction, post-traumatic arthrosis, unplanned revision surgery, secondary arthrodesis, or deep vein thrombosis were observed. No evidence of radiographic diastasis or implant creep was noted before or after routine removal of bridge plates (Figures 4 and 5).
Discussion
Our findings, in a small cohort of patients, suggest that this hybrid technique was associated with good intermediate-term outcomes for patients with primarily ligamentous sports-related Lisfranc injuries.
Lisfranc injuries are a heterogeneous and difficult pathology to treat with potential long-term symptoms including pain, deformity, and loss of function. Although the treatment principles are very similar to that of other fracture-dislocations—anatomical reduction, fixation using absolute or relative stability, respecting soft tissues, and early and safe mobilisation—there has been debate regarding the optimal surgical strategy. Dorsal bridge plating has gained popularity in favour of transarticular screw fixation alone because of its ability to preserve bone stock, bypass articular surfaces of the midfoot, and treat comminuted fractures.2,18,38 Articular bridge plating can be used in combination with transarticular screws, although recent studies have suggested that this does not result in improved outcomes.23,24,28,37 Irrespective of surgical technique, the most important factor that is associated with optimal postoperative outcomes is the quality of reduction.11,15,22
The use of flexible fixation methods in place of a Lisfranc interval screw is a relatively new surgical concept which may offer advantages of less chondral damage, reduced stiffness, preservation of physiological motion, and elimination of the need for transarticular hardware removal. Biomechanical studies show suture tape and endobutton constructs limit C1-M2 diastasis as effectively as screws under physiological loads.1,29 The suture tape construct was tested in cadaveric models by Koroneos et al, 20 who observed that the addition of an inter-cuneiform limb of tape significantly increased failure strength and could sustain higher loads than a screw. They later performed a separate study which concluded that suture tape Lisfranc ligament reinforcement was superior to a single suture button device from C1 to M2. 21 Despite these promising results, only a few case series have been published on suture tape Lisfranc ligament reinforcement in vivo. In some cases, a single suture button construct was used across the C1-M2 interval4,8,9; however, other authors advocated for the use of a second suture limb from C1 to C2. Despite promising clinical results, radiographic diastasis was observed in Cottom et al’s9,10,19 case series at 3-year follow-up.
Hoskins et al 17 reviewed 15 isolated ligamentous Lisfranc injuries treated with a suture tape construct: 8 with a single limb and 7 with inter-cuneiform augmentation. The mean follow-up duration was 7.3 (range 1.4-18.8) months. They reported minimal complications, but the absence of a standardised rehabilitation protocol precluded interpretation of return to function. In comparison, our cohort consisted of 20 mixed ligamentous and low-grade bony Lisfranc injuries with a longer mean follow-up duration of 31.8 (range 12-61) months. Our study utilised a potentially synergistic surgical approach, combining suture tape fixation with articular bridge plating and a standardised non–weight-bearing protocol. This hybrid surgical technique, which has not been widely reported, yielded a postoperative mean AOFAS of 90.6 ± 9.4, comparable to or exceeding other studies using the suture button construct alone, such as Yongfei et al 42 (92.4 ± 4.3) and Cho et al 6 (84.3 ± 2.0). These outcomes may be associated with rigid extra-articular plating, which maintains column length and TMTJ alignment, combined with physiological stabilisation across the Lisfranc interval. However, the small sample size may be a confounding factor.
When comparing outcome measures before and after an arbitrary cutoff of 18 months, AOFAS scores were 88.0 ± 6.9 and 91.6 ± 10.3 (P = .17), respectively, and VAS scores were 1.8 ± 0.8 and 1.5 ± 0.8 (P = .31), respectively. Although statistical significance was not reached, this suggests that patients maintain good outcomes beyond intermediate follow-up, and that function may continue to improve beyond 18 months. This may serve as an important counselling point when providing prognostic information, and discussing recovery time frames.
The AOFAS midfoot score is the most frequently used questionnaire for functional assessment in Lisfranc injuries, although clinical significance is unclear as there is no established minimal clinically important difference (MCID). 8 Philpott et al’s meta-analysis showed postoperative scores in bridge plate fixation were superior to transarticular screw fixation with a 5-point mean difference, although limited by small study numbers. 31 Our postoperative results were superior to the pooled mean of 79.2 ± 8.3 for plate fixation in Philpott et al’s systematic review. The highest mean AOFAS score for bridge plating was reported by Stern and Assal 36 at 85 (78-92); however, they also had the smallest patient cohort (15 participants). It is possible that the incremental benefit in our study relates to the addition of a suture tape construct; however, the small sample size precludes definitive conclusions.
Our return to sport outcomes were comparable to other studies. Ninety-five percent of patients resumed some level of sport at a follow-up duration of 2.7 years with a range of 1-5 years, mirroring Mora et al’s 26 94% at 2.9 years (range, 1.5-5.4 years). Twenty-six percent of our patients reduced participation frequency, which is similar to the one-third noted by Mora et al. Thirty-eight percent of our cohort were asymptomatic and had no restrictions on return to activity, compared with the 27% as reported by Mora et al. The differences in our studies lay in the surgical technique, wherein Mora et al used the combination of articular bridge plating and transarticular Lisfranc screws. This suggests that, despite the modification in surgical protocol, overall results in return to sports and physical activity are similar. Notably, 33% of patients in both studies tended towards lower impact sports or physical activities after 1 year. This suggests that, despite successful surgical stabilisation, Lisfranc injuries remain associated with some morbidity in up to one-third of patients at intermediate-term follow-up.
The infection rate after Lisfranc ORIF has been reported to range between 0% and 15%, 35 with our study mirroring similarly powered reviews such as Kuo et al, 22 who reported a combined superficial and deep infection rate of 8%, and Ly and Coetzee, 25 who reported a 10% infection rate in their cohort of primarily ligamentous Lisfranc injuries.
There are several limitations to our study. The sample size of 20 patients was small, although this remains one of the larger series evaluating this specific technique. Additional limitations include lack of a control group and a relatively short minimum follow-up duration of 1 year, limiting assessment of long-term complications such as arthritis and conversion to arthrodesis. No a priori power analysis was performed; accordingly, null subgroup comparisons (gender, age, and time to surgery) should be interpreted with caution. Additionally, the AOFAS midfoot score, although the most widely used instrument for this injury, has well recognized validity concerns and no established MCID; future studies should incorporate a validated alternative PROM. The retrospective single-surgeon design introduces potential bias. Larger prospective studies and longer follow-up duration are required.
Conclusion
There is debate regarding the optimal surgical fixation method for Lisfranc injuries. Our study provides preliminary evidence that using a combination technique incorporating both articular bridge plating and suture tape Lisfranc ligament reinforcement was associated with restoration of alignment, demonstrated excellent pain and functional scores, and was associated with low complication rates. Our study indicates that this technique has comparable outcomes to similar series assessing transarticular screws or bridge plate-only constructs, with the potential benefit of avoiding iatrogenic injury to the Lisfranc joint and the long-term complications associated with extensive transarticular instrumentation. Further high-powered prospective research, incorporating control groups, would be valuable in confirming both the safety and efficacy of this technique.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261449243 – Supplemental material for Patient-Reported Outcomes Following Lisfranc Fixation via Articular Bridge Plating Combined With the Suture Tape Ligament Reconstruction Technique
Supplemental material, sj-pdf-1-fao-10.1177_24730114261449243 for Patient-Reported Outcomes Following Lisfranc Fixation via Articular Bridge Plating Combined With the Suture Tape Ligament Reconstruction Technique by Matthew Sun, Sophia Padovano, Tanita Botha and Sasha Roshan-Zamir in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
The study was approved by the local ethics committee at St Vincent’s Private Hospital (ID: 23038) and is consistent with the declaration of Helsinki.
Consent to Participate
All patients provided verbal informed consent for this study.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.