
Abstract
Background:
Isolated lateral malleolus fractures account for a significant proportion of ankle fractures, and complications related to surgical treatment are common. This study aimed to assess the feasibility of conservative treatment with walker boot and immediate weightbearing as tolerated for Weber B / supination-external rotation (SER) lateral malleolus fracture, by comparing stable (SER2) and potentially unstable (SER4a) fractures. The distinction between stable and unstable fractures is crucial to guide treatment decisions.
Methods:
This prospective study included patients with Weber B/SER lateral malleolus fractures who met specific criteria. Fracture stability was assessed via medial clear space (MCS) measurement on weightbearing radiographs and conservative (walker boot and immediate weightbearing as tolerated) or surgical treatment was determined accordingly. Clinical and functional outcomes—including visual analog scale (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) scores, Foot and Ankle Ability Measure (FAAM) scores, and 36-Item Short Form Health Survey (SF-36) scores—were evaluated in outpatient clinic follow-up, with a minimum duration of 12 months.
Results:
Out of 155 identified Weber B fractures with MCS <7 mm, 141 patients completed follow-up: 114 with SER2 and 27 with SER4a fractures. The SER2 group demonstrated excellent outcomes at 12 months (VAS 0.1, AOFAS 98.9, FAAM activities of daily living (ADL)/Sport 99.4/99.6), with 98.2% return to sport, 100% return to work, and 100% return to ADL. The SER4a group demonstrated comparable outcomes at 12 months (VAS 0.0, AOFAS 100, FAAM ADL/Sport 100/100), with full return to sport, work, and ADL. One patient in the SER4a group evolved to nonunion and required surgery during follow-up. With the numbers available, no significant intergroup differences in outcome scores or return to function could be detected.
Conclusion:
This study supports conservative treatment—with walker boot and immediate weightbearing as tolerated—for stable SER2 lateral malleolus fractures, and was associated with reduced need for surgery and lower exposure to surgical complications. It also suggests that potentially unstable SER4a fractures may achieve comparable outcomes under the same conservative protocol. Weightbearing radiographs assessment with MCS measurement appears to be an effective method for guiding treatment decisions in Weber B/SER lateral malleolus fractures.
Level of Evidence:
Level II, therapeutic, prospective cohort study.
Introduction
Isolated lateral malleolus fractures comprise approximately 70% of all ankle fractures. 1 Although these fractures are classically simple and easy to treat, there is a high incidence of complications related to surgical treatment, such as wound dehiscence, infection, hardware prominence requiring removal, and up to 20% superficial peroneal nerve injury.2 -4 Several systematic reviews have demonstrated that the key factor in managing isolated Weber B lateral malleolus fractures resulting from a supination-external rotation (SER) mechanism is stability.5,6 Thus, stable fractures can be treated conservatively, whereas unstable fractures require surgical fixation. 7
We now know that the medial column, consisting of the medial malleolus and the medial ligament complex (deltoid ligament), comprise the key structures responsible for ankle stability. 7
Weber’s classification only assesses the lateral malleolus and, therefore, cannot distinguish stable from unstable fractures in the common type B injuries. The Lauge-Hansen classification relates the mechanism of injury to both medial and lateral structures and thus can differentiate stable and unstable patterns.
SER injuries cause a trans-syndesmotic lateral malleolus fracture (Weber B): SER2. With further external rotation, the injury may progress to SER3 (with posterior malleolus or posterior ligament complex injury), and eventually to SER4 (medial malleolus fracture or deltoid ligament rupture). In Weber B/SER4 lesions, the medial clear space (MCS) is abnormally widened, with various cutoffs values described in the literature ranging from >4 to 5 mm. According to the literature, the MCS is an expression of tibiotalar congruence and an indirect measure of ankle stability.1,8,9
It is therefore imperative to distinguish between SER2 and SER4 (with deltoid ligament injury vs without medial malleolus fracture) to determine the most appropriate treatment based on fracture stability.8 -10 According to the literature, ankle fracture stability can be assessed using gravity stress radiography, manual stress testing, and weightbearing radiographs, with each modality providing complementary information for decision making.11 -13 However, weightbearing radiographs are increasingly recognized as the most reliable method for assessing ankle joint congruence and guiding treatment.8,14 Fractures that remain congruent under weightbearing (MCS < 4 mm) can be safely managed nonoperatively, regardless of stress test results, supporting a shift from the traditional stable/unstable classification to a more functional concept of “congruency under load.”11 -14
The deltoid ligament (medial complex) consists of a superficial layer that resists plantar flexion and external rotation of the talus relative to the tibia, and a deep layer (anterior and posterior tibiotalar ligaments) responsible for overall ankle stability by controlling lateral talar translation.8,9,15
The posterior tibiotalar ligament (PTTL) is described as the strongest and thickest deep ligament. It is loose in plantar flexion and tight in neutral position and with weightbearing; it has been proposed to contribute to resistance against lateral translation of the talus, restoring ankle mortise with normal joint congruence and MCS.8,9,12
When both components (superficial and deep) are intact, the fracture is classified as SER2: MCS is normal on nonweightbearing, weightbearing, and stress radiographs, indicating a stable ankle.10,12
If there is rupture of the superficial deltoid component and/or anterior tibiotalar ligament (ATTL) while the PTTL remains intact, there is no resistance to external rotation and lateral displacement of the talus when the ankle is in plantar flexion (PTTL is loose). However, in neutral position and under load, the PTTL tightens and prevents lateral translation of the talus, restoring the ankle mortise with normal joint congruency, as evidenced by a normal MCS. That is, injuries to the superficial component of the deltoid and/or ATTL but with intact PTTL are classified as SER4a—partially stable fractures. 12
When there is complete rupture of both superficial and deep deltoid components, the MCS is increased in all ankle radiographs, and these fractures are classified as SER4b—unstable fractures. 12
Studies have shown that the best method for distinguishing stable from unstable SER injuries is to obtain weightbearing radiographs at 5, 7, or 10 days after injury.8,12 Gougoulias et al 14 showed that 3.7% of fractures were unstable and required surgical treatment, whereas those considered stable were all treated conservatively and did not subsequently required surgery.
According to the literature, SER2 fractures are considered stable and can be treated conservatively with walker boot, allowing early weightbearing as tolerated.8,9,12,16
SER4a fractures are potentially unstable, because to ensure proper ligament healing (particularly the superficial deltoid and ATTL), the ankle must remain in a neutral position (90°), where the PTTL is tightened. These fractures should be treated conservatively, immobilized with a suropodalic plaster cast in a neutral position. A walker boot has been contraindicated for these injuries, as it allows plantar flexion, leading to laxity of the partially ruptured ligaments.8,9,12 SER4b fractures are generally unstable and usually require surgical fixation.8,9,12 Although isolated Weber B/SER lateral malleolus fractures have classically been treated surgically, recent evidence suggests that about 90% of these fractures reduce under load and behave as stable fractures, 12 allowing for conservative treatment as a safe option and avoiding potential surgical risks and complications.
The aim of this study is to evaluate whether isolated Weber B/SER lateral malleolus fractures that appear to be stable on weightbearing radiographs can be successfully managed conservatively with an early weightbearing protocol, while maintaining ankle congruence after fracture healing. Additionally, we aim to compare clinical and radiographic outcomes between completely stable (SER2) and potentially unstable (SER4a) fractures following conservative treatment protocol.
Material and Methods
This is a prospective study with an 18 month duration, including all patients evaluated in the emergency department of a secondary care hospital and who were subsequently followed up in outpatient consultations at the same institution for isolated Weber B/SER lateral malleolus fractures. Ethical approval was obtained from the local ethics committee. Based on existing evidence, the inclusion criteria were defined as patients aged between 18 and 89 years, with isolated Weber B/SER lateral malleolus fractures and MCS on nonweightbearing radiographs <7 mm. Exclusion criteria included other types of ankle fractures, personal history of ipsilateral or contralateral ankle fracture or surgery as well as hindfoot surgery, previous injury causing limited walking capacity, peripheral neuropathy, inability to give informed consent, noncompliance with a treatment protocol, and communication difficulties in Portuguese. In addition to radiographic assessment, all patients underwent computed tomography in the emergency department to rule out occult fractures of the medial and posterior malleolus. Patients were immobilized with a plaster cast and evaluated in consultation with bilateral single-leg weightbearing radiograph within 10 days of injury. Those with an MCS ≤4 mm underwent the conservative treatment protocol (SER2 or SER4a): walker boot for 5-6 weeks and immediate weightbearing as tolerated.
We classified fractures as SER2 when MCS was <7 mm on nonweightbearing radiographs and ≤4 mm on both nonweightbearing and weightbearing radiographs. SER4a fractures were defined as those with MCS >4 mm and <7 mm on nonweightbearing radiographs, but ≤4 mm on weightbearing radiographs. SER4b fractures were defined by persistent MCS widening (>4 mm) across all radiographic assessments.
Those with an MCS >4 mm (SER4b) were treated surgically and therefore excluded from the study. Follow-up assessments (clinical and radiologic) were conducted at 1, 2, 5, 12 weeks and 6, 12 months, with a minimum follow-up of 12 months. To assess intraobserver reliability in interpreting weightbearing radiographs, the same observer repeated the measurements on 3 separate days, and the mean of these 3 measurements was used in the analysis.
Radiologic outcomes that were assessed included bilateral MCS, fibular shortening, talocrural angle, and fibular lengths. The MCS was measured according to the method described by Murphy et al, 17 defined as the distance between the medial border of the talus and the lateral border of the medial malleolus, measured along a line positioned 5 mm below and parallel to the talar dome (Figure 1). 17 Fibular length was measured using a method comparable to that outlined by Panchbhavi et al, 18 as the distance between a line parallel to the distal tibial articular surface and a second line parallel to the distal tip of the fibula (Figure 2). The talocrural angle was measured in weightbearing radiographs in both ankles, by drawing a perpendicular line downward from the tibial plafond surface, intersected by a line drawn connecting the tips of both malleoli. The talocrural angle was measured in the superomedial quadrant (Figure 3). 19 Fibular shortening was defined in 2 ways: the difference in fibular length between the injured and uninjured side, or a difference of >2° in the talocrural angle between the 2 sides. 20

Illustration of the technique for measuring the medial clear space using mortise view projections on weightbearing radiographs. A point was first marked 5.0 mm below the talar dome. The medial clear space was then measured as the distance between the inner edge of the talus and the outer edge of the medial malleolus along a line parallel to and 5.0 mm beneath the talar dome.

Illustration of the method for measuring the fibular length mortise view projections on weightbearing radiographs. The measurement (A) was taken as the distance between a line drawn parallel to the distal tibial articular surface and another line drawn parallel to the distal tip.

Illustration of the method for measuring the talocrural angle (α) using weightbearing radiographs of both ankles. A perpendicular line was drawn downward from the tibial plafond surface, intersected by a line connecting the tips of both malleoli. The talocrural angle was measured in the superomedial quadrant.
Clinical and functional outcomes included visual analog scale (VAS) for pain, American Orthopaedic Foot & Ankle Society (AOFAS) score, Foot and Ankle Ability Measure (FAAM) score, and 36-Item Short Form Health Survey (SF-36) score, return to sport, return to work, and activities of daily living (ADL).
The data were analyzed using IBM SPSS Statistics, version 29.0. Multiple outcomes were assessed without a prespecified primary outcome. Descriptive statistics were used to characterize the sample: categorical qualitative variables were presented as frequencies and percentages; interval quantitative variables were expressed as means and SDs. To determine the appropriate statistical tests, normality of distribution was assessed. For the large groups, the central limit theorem was applied to justify the use of parametric tests. To compare groups (SER2 and SER4a), the Mann-Whitney U test was used when the smaller group (SER4a) did not follow a normal distribution. The parametric t test for independent samples was used when both groups followed a normal distribution. For associations between categorical qualitative variables, the χ2 test was applied.
To assess differences between assessment times, parametric tests were used: repeated measures analysis of variance (3 or more times) using the least significant difference multiple comparison of means test to evaluate the differences between the various groups, and the t test for paired samples to see the differences between just 2 times (6 months and 12 months of follow-up). Only these parametric tests were used for this purpose, because the distribution of the results was normal in both groups,
Statistical significance was considered at a P value <.05 with a 95% CI.
Results
A total of 155 patients with Weber B fracture with MCS <7 mm on nonweightbearing radiographs were identified. Four were excluded because of a previous malleolar fracture. Of the 151 enrolled, 119 had stable fractures (SER2), 31 had partially unstable fractures (SER4a), and 1 was unstable (SER4b). In the SER2 group, 5 patients were excluded: 3 were lost to follow-up and 2 died during follow-up because of unrelated medical conditions (1 within 6 months and 1 before 12 months). In the SER4a group, 4 patients were excluded: 1 evolved to nonunion and required surgery during follow-up, 1 patient did not comply with the protocol, and 2 patients were surgically treated at another institution. In total, 141 patients completed follow-up: 114 in the SER2 group and 27 in the SER4a group (Figure 4).
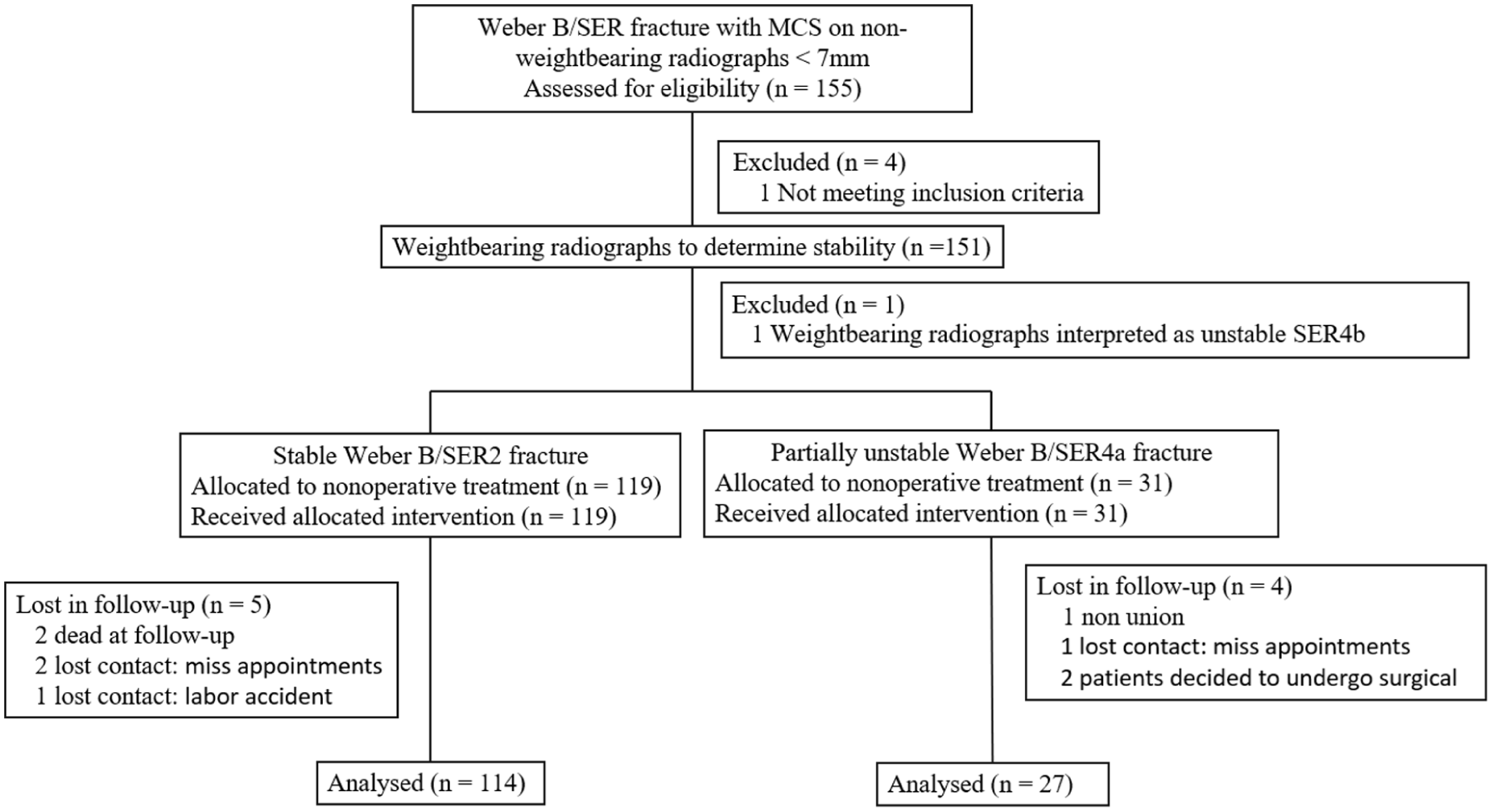
Study diagram.
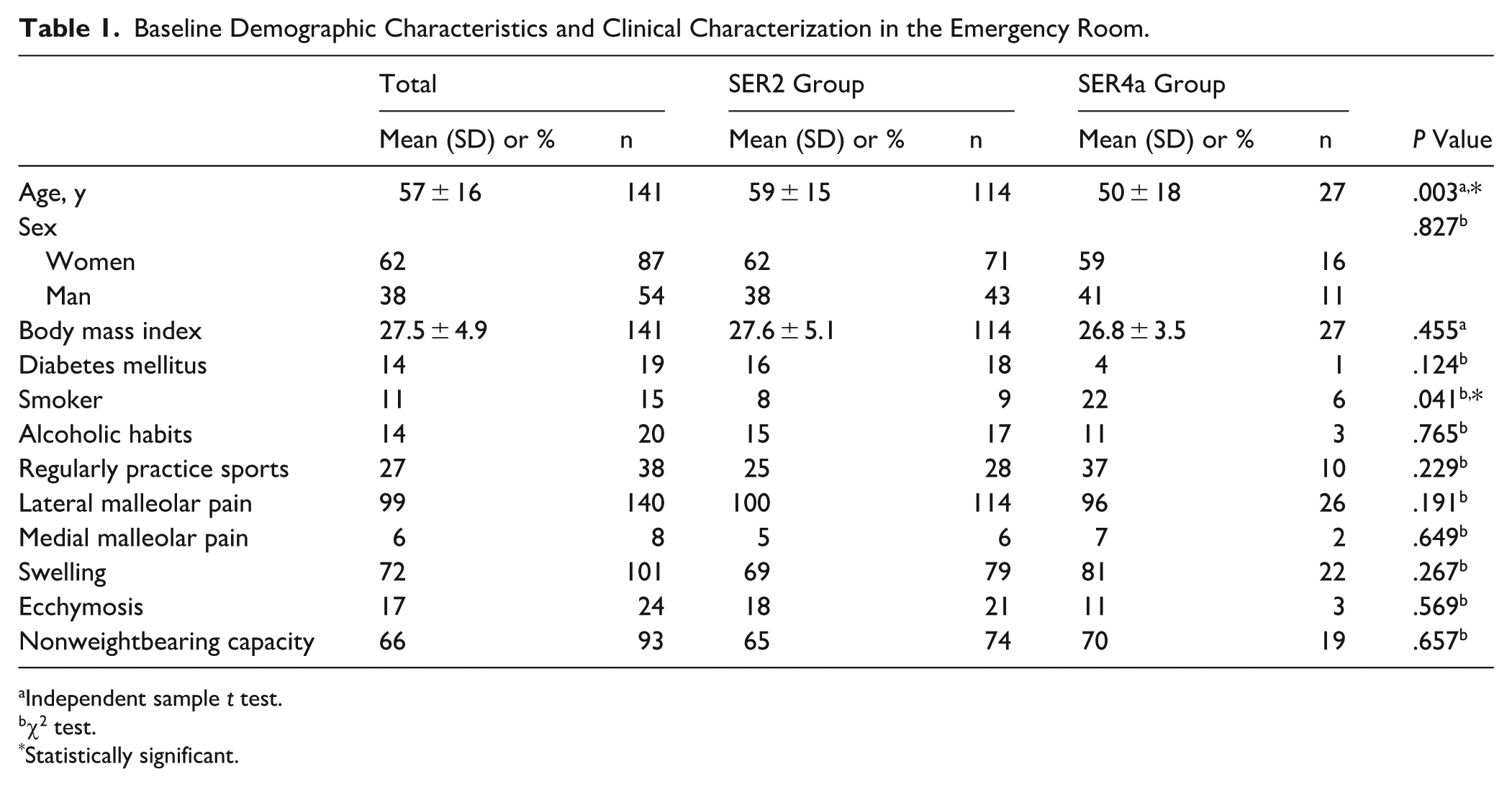
The mean age was 57 ± 16 years (19-89); 62% were women and 38% were men. Among these patients, 27% regularly practiced sports, 11% were smokers, 14% reported alcohol consumption, and 14% had diabetes. The average body mass index was 27.5 ± 4.9 (Table 1). Statistically significant differences were found between the SER2 and SER4a groups only in terms of age (P = 0.003)—SER2 patients were older (59.33 ± 14.56 years) than those in the SER4a group (49.52 ± 17.57 years)—and smoking habits, with a higher percentage in the SER4a group (22%) than in the SER2 group (8%) (Table 1).
Baseline Demographic Characteristics and Clinical Characterization in the Emergency Room.
Independent sample t test.
χ2 test.
Statistically significant.
In the emergency department, 99% of patients reported lateral malleolar pain, 6% reported medial malleolar pain, 72% had swelling, and 66% were unable to bear weight (Table 1). No statistically significant differences were found between groups regarding clinical signs and symptoms (Table 1).
At 6 months of follow-up, the SER2 group had a mean VAS score of 0.7 (0.5-0.9), AOFAS 95.6 (94.2-97.0), FAAM ADL subscale 98.51 (97.4-99.7), FAAM sports subscale 97.7 (96.3-99.1), SF-36 physical functioning 97.9 (96.5-99.3), SF-36 limitations due to physical health 96.7 (94.8-98.6), and SF-36 pain 94.2 (92.4-95.9). At 12 months of follow-up, the SER2 group had a mean VAS score of 0.1 (0.0-0.2), AOFAS 98.9 (98.3-99.5), FAAM ADL subscale 99.4 (98.5-100.4), FAAM sports subscale 99.6 (99.1-100.2), SF-36 physical functioning 99.4 (98.6-100.3), SF-36 limitations due to physical health 99.1 (97.9-100.4), SF-36 pain 98.6 (97.8-99.4) (Supplemental Table 1).
Return to sport at the previous level was observed in 88.6% (101) of cases, return to work in 97.4% (111) of cases, and to ADL in 97.4% (111) at 6 months of follow-up and 98.3% (112) return to sport and 100% (114) return to work and ADL at 12 months of follow-up (Supplemental Table 1).
At 6 months of follow-up, the SER4a group had a mean VAS score of 0.5 (0.1-0.9), AOFAS 97.1 (95.1-99.1), FAAM ADL subscale 99.22 (98.1-100.4), FAAM sports subscale 98.9 (96.9-100.8), SF-36 physical functioning 99.3 (97.7-100.8), SF-36 limitations due to physical health 97.22 (93.0-101.4), and SF-36 pain 95.9 (92.9-98.9). At 12 months of follow-up, the SER4a group had a mean VAS score of 0.0 (0.0-0.0), and all functional scores were 100 at 12 months (Supplemental Table 1). Return to sport at the previous level was observed in 96.3% (26) of cases, return to work in 100% (27) of cases and to ADL in 100% (27) at 6 months of follow-up and 100% (27) return to sport, return to work, and ADL at 12 months of follow-up (Supplemental Table 1).
No statistically significant differences were found between the groups regarding functional scores or return to sport, return to work, and ADL at any time point. (Supplemental Table 1).
When the scores were analyzed at the 2 time points, statistically significant improvements were found in all scores between the 6- and 12-month follow-ups (P < .001) (Table 2). There also was a statistically significant decrease in VAS score (P < .001) (Table 2), and return to sport increased statistically significantly between 6 months (90.1%) and 12 months (98.6%) (Table 2).
Differences Between the Various Moments of Assessment of Functional Outcomes.
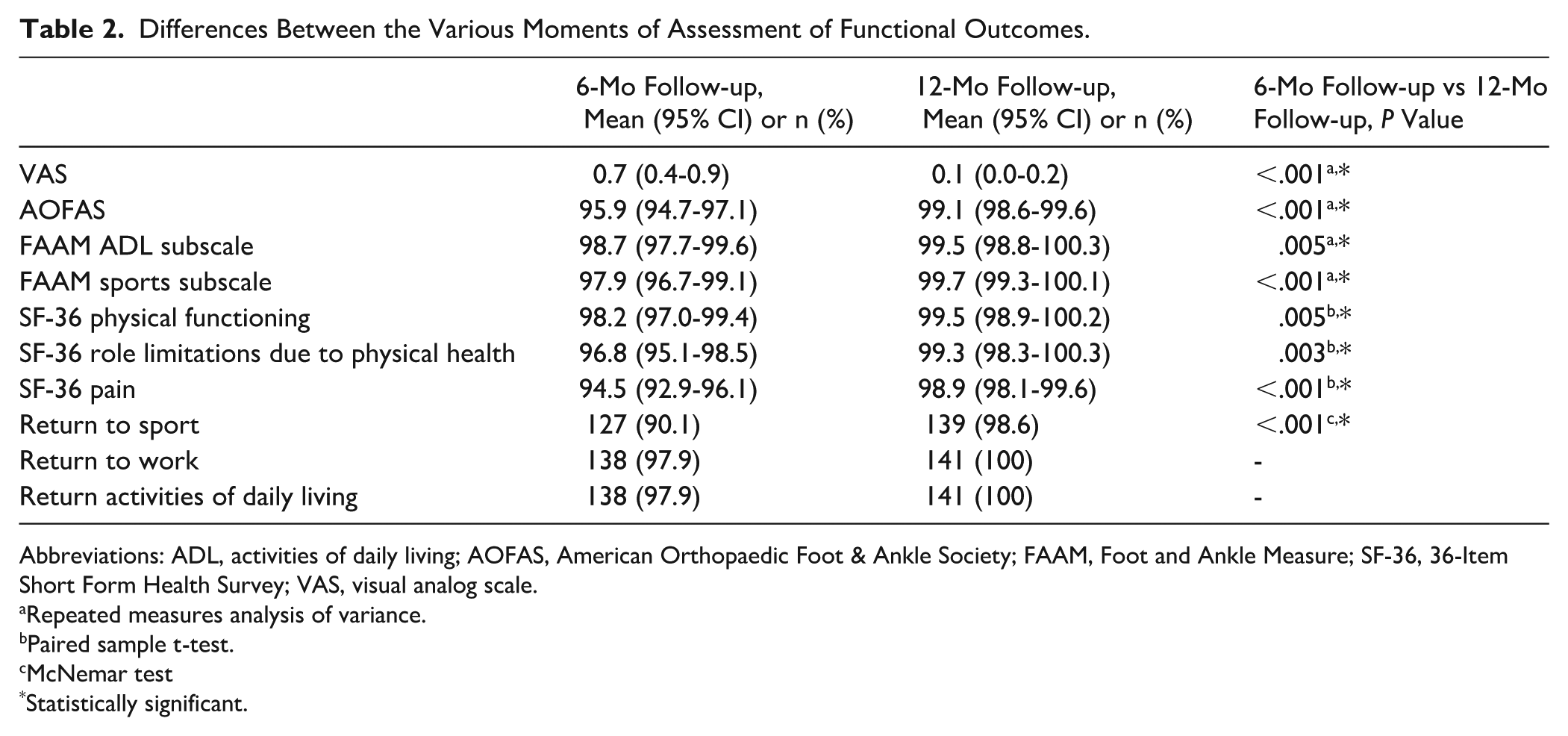
Abbreviations: ADL, activities of daily living; AOFAS, American Orthopaedic Foot & Ankle Society; FAAM, Foot and Ankle Measure; SF-36, 36-Item Short Form Health Survey; VAS, visual analog scale.
Repeated measures analysis of variance.
Paired sample t-test.
McNemar test
Statistically significant.
No statistical correlation was found between fracture type (SER2 and SER4a) in any of functional outcomes (Supplemental Table 2).
Regarding fibular shortening (>2° difference compared to the contralateral side), there was a statistically significant difference between the groups (P < .05), shortening (>2° difference to the contralateral side) had a statistical correlation with type of fracture, that was greater in the SER4a (30%) group than in SER2 (8%) (Table 3).
Differences Between SER2 and SER4a Groups Regarding Radiographic Parameters.
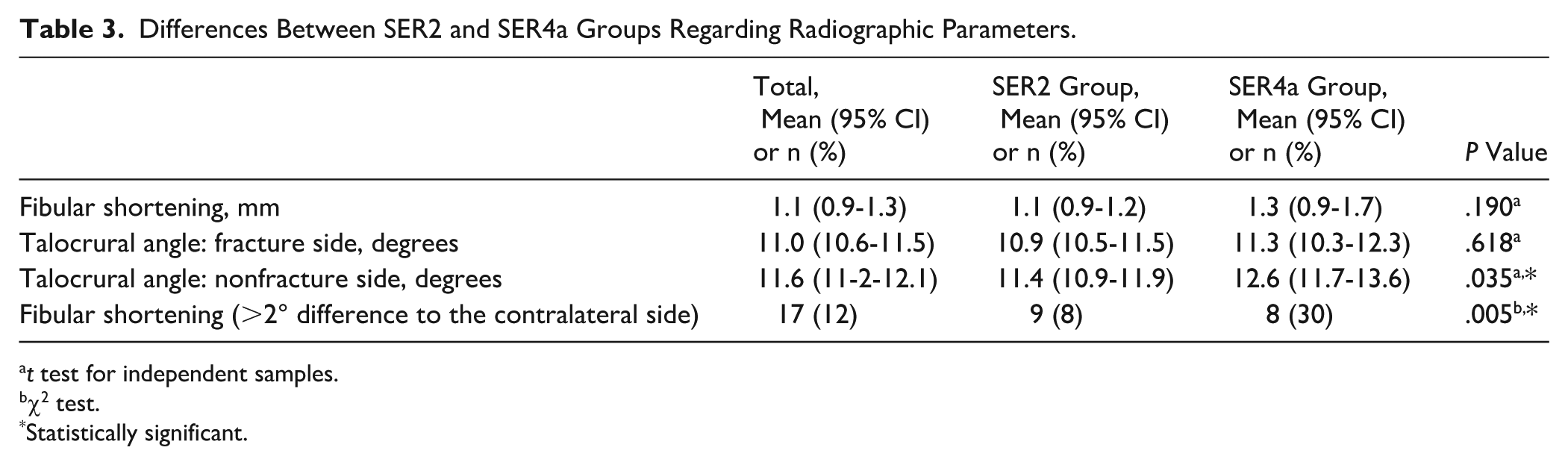
t test for independent samples.
χ2 test.
Statistically significant.
A statistically significant correlation was found between fibular shortening and functional outcomes at 6 months, with a positive correlation between fibular shortening and VAS score, and a negative correlation between fibular shortening and AOFAS score, FAAM ADL subscale, and FAAM sports subscale (P < .05) (Supplemental Table 3). In other words, the greater the fibular shortening, the higher the VAS value and lower values for the other scores. However, with the numbers available, no significant association could be detected between fibular shortening and any functional score evaluation at 12 months.
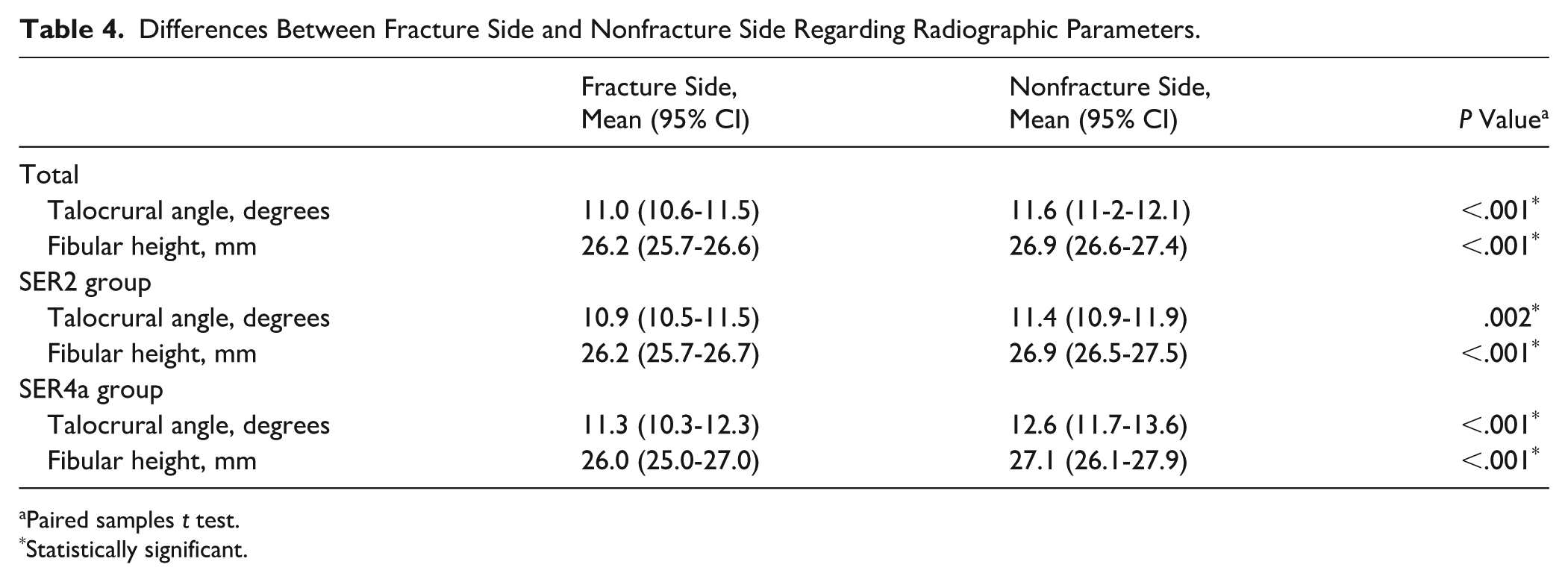
Comparison of the fractured and nonfractured side revealed statistically significant differences in talocrural angle and fibular length, with significantly greater shortening on the fractured side (P < .05) (Table 4).
Differences Between Fracture Side and Nonfracture Side Regarding Radiographic Parameters.
Paired samples t test.
Statistically significant.
Discussion
This study investigated the outcomes of conservative treatment, using a walker boot and immediate weightbearing as tolerated, for isolated Weber B/SER lateral malleolus fractures, specifically comparing stable SER2 fractures and potentially unstable SER4a fractures. Our findings may contribute to the evolving understanding of optimal management strategies for these injuries, particularly in distinguishing the necessity for surgical intervention versus conservative treatment.
In our cohort of 141 patients, all but 1 achieved union with MCS <4 mm on weightbearing radiograph. Only 1 patient in the SER4a group required surgical treatment because of symptomatic nonunion at 6 months.
These findings are consistent with recent high-quality evidence. Gregersen et al 12 demonstrated that Weber B fractures stable on weightbearing radiographs can be safely treated nonoperatively, regardless of gravity stress test results, with no significant differences in outcomes between SER2 and SER4a patterns at 2-year follow-up. Similarly, the CROSSBAT study showed no clinically significant advantage of surgical treatment over conservative management for displaced Weber B fractures, with comparable functional outcomes and higher complication rates in the operative group. 12
Our findings suggest that both SER2 and SER4a fractures can be safely treated with early weightbearing protocols, with maintenance of normal ankle congruence at the 12-month (this means that there were no changes in MCS measurements during that time with any subject) follow-up, as demonstrated by 2 case examples from our cohort (Figure 5).

The figure presents 2 cases of patients with SER4a fractures, demonstrating nonweightbearing radiographs taken in the urgency room with MCS <7 mm and weightbearing radiographs at 10 days and 12 months postinjury with MCS ≤4 mm. MCS, medial clear space.
Patients with stable SER2 fractures reported excellent clinical outcomes at both 6- and 12-month follow-up. The mean VAS score was low (6-mo follow-up [6MF]: 0.7; 12-mo follow-up [12MF]: 0.1), indicating minimal pain. A high AOFAS score (6MF: 95.6; 12MF: 98.9) suggests good function and mobility. The FAAM scores for ADL (6MF: 98.5; 12MF: 99.4) and sports (6MF: 97.7; 12MF: 99.6) reflected excellent functional status. SF-36 scores were generally high, indicating good physical functioning (6MF: 97.9; 12MF: 99.4), minimal limitations due to physical health (6MF: 96.7; 12MF: 99.1), and low pain levels (6MF: 94.2; 12MF: 98.6). Additionally, high rates of return to their previous levels of sport (6MF: 88.6%; 12MF: 98.2%), work (6MF: 97.4%; 12MF: 100%), and ADL (6MF: 97.4%; 12MF: 100%) were also observed. These outcomes highlight the potential of conservative management with walker boot and immediate weightbearing as tolerated to provide satisfactory recovery without the risks associated with surgical procedures.
Our findings support the growing body of evidence that stable SER2 fractures can be effectively managed conservatively, even with early weightbearing as tolerated. This aligns with the current paradigm shift in ankle fracture management, where increasing emphasis is placed on functional stability under load. Evidence from both Gregersen et al 12 and the CROSSBAT trial supports a more conservative approach, even in fractures traditionally considered unstable, provided that joint congruence is maintained.
These fractures tend to be associated with excellent functional outcomes and low complication rates, in line with previous research.8,9,12,13 The conservative approach minimizes the risks associated with surgical interventions, such as infection, hardware prominence, and nerve injuries.3,4
Patients with potentially unstable SER4a fractures also demonstrated excellent outcomes at 6 and 12 months. The mean VAS score was still relatively low (6MF: 0.5; 12MF: 0), indicating considerable improvement in pain. The AOFAS score (6MF: 97.1; 12MF: 100) and FAAM scores for daily living (6MF: 99.2; 12MF: 100) and sports (6MF: 98.9; 12MF: 100) suggest good mobility and high level of functionality. SF-36 scores were mostly high, revealing relatively high physical functioning (6MF: 99.3; 12MF: 100), lower limitations due to physical health (6MF: 97.2; 12MF: 100), and lower pain levels (6MF: 95.9; 12MF: 100). Also, all patients in this group were able to return to work (6MF: 100%; 12MF: 100%), and a significant proportion returned to their previous sport (6MF: 96.3%; 12MF: 100) and ADL levels (6MF: 100%; 12MF: 100%).
The study also highlights the challenges associated with potentially unstable SER4a fractures. These fractures, characterized by the disruption of the superficial component of the deltoid ligament and potential ATTL rupture, can lead to comparable outcomes to SER2, and present good functional outcomes on at least 12 months’ follow-up, suggesting that this type of fracture can be effectively treated conservatively with walker boot and immediate weightbearing as tolerated in line with previous research.8,21
Unlike traditional conservative treatment protocols that recommend immobilization with a plaster cast, we propose the use of an orthotic device as already suggested in a previous study with a shorter follow-up time.8,12,21 This approach improves comfort and mobility for the patient. To date, no evidence has shown higher osteoarthritis rates associated with the treatment of SER4a fractures using this protocol. Long-term follow-up (5-10 years) will be essential to confirm joint preservation and offer valuable new insights.
With the numbers available, no statistically significant differences in functional outcomes could be detected between the SER2 and SER4a fractures at any time point, highlighting that both groups achieved excellent results.
Both groups demonstrated reduced pain from 6 to 12 months, increased functional scores, and improved return to sport, with the majority of the patients returning to sport at 6 months.
There was no correlation between fracture type and any of the functional outcomes, suggesting that neither type of fracture is associated with worse outcomes.
On comparing the fractured with the nonfractured side, statistically significant differences were found regarding the talocrural angle and length of the fibula, showing a significant shortening on the fractured side (Table 4), as we expected.
Importantly, fibular shortening was more common in the SER4a group and was significantly correlated with worse outcomes at 6 months (more pain, lower function).
This may be because these injuries reflect a more advanced stage of the SER mechanism, with greater rotational force at the time of trauma and, consequently, a greater tendency toward transient fibular displacement. Although weightbearing appears to restore tibiotalar congruence, it may not completely eliminate a small degree of residual fibular displacement generated during the initial injury.
However, this correlation was no longer present at 12 months, suggesting that this parameter may not be a reliable predictor of functional recovery in the short term (12-month follow-up).
The study has important clinical implications for the management of Weber B/SER lateral malleolus fractures. It reinforces the idea that stable SER2 fractures may be safely treated with walker boot and early weightbearing as tolerated and was associated with reduced need for surgery and lower exposure to surgical complications. Additionally, it highlights that potentially unstable SER4a fracture, previously considered for surgery and less suitable for walker boot protocols and early weightbearing, may also benefit from this conservative treatment achieving equivalent good functional results, leading to lower health care cost and reduced morbidity.
Our results further support previous literature suggesting that operative treatment may be unnecessary in a substantial proportion of these fractures, without compromising outcomes, and potentially reducing exposure to the well-documented risks associated with surgery.
Limitations
It is essential to acknowledge the limitations of our study. Despite being a prospective study, the overall sample size was relatively small, particularly for the SER4a group. The imbalance in sample size between the 2 groups (SER2 vs SER4a) may have influenced the results and statistical significance. The smaller number of patients in the SER4a group reduces statistical power, increasing the risk of type II error and limiting the ability to detect small but potentially clinically relevant differences between groups. Additionally, unequal group sizes may affect the robustness of comparative analyses and widen CIs, making the estimates less precise. Therefore, the absence of statistically significant differences between groups should be interpreted with caution. This highlights the need for further research with larger and more diverse cohorts to validate and strengthen these findings.
The exclusion of patients who did not comply with the treatment or follow-up protocol represents a potential source of selection bias, possibly favoring better outcomes and limiting the generalizability of the results.
Additionally, the follow-up period of 12 months—although sufficient for assessing short-term functional recovery—does not capture potential long-term complications, such as the development of post-traumatic osteoarthritis. Extending follow-up to 5 or 10 years would provide deeper insights into the implications of the treatment strategy.
Finally, this was a single-center study, which may restrict the generalizability of the results to other health care settings and populations. Multicenter studies are recommended to confirm these findings across different clinical contexts ant patient demographics.
Conclusions
This study demonstrates that weightbearing radiographs with MCS measurement appeared to be an effective method to guide the treatment of stable or unstable Weber B/SER isolated lateral malleolus fracture. In stable fractures (SER2), a conservative treatment protocol using a walker boot and early weightbearing as tolerated results in excellent functional outcomes, while being associated with a lower exposure to the risks related to surgical fixation. Importantly, our findings suggest that potentially unstable fractures (SER4a)—traditionally considered less amenable to conservative care—may also be successfully managed using this same protocol, with outcomes comparable to SER2 fractures.
Our research contributes to the growing body of evidence supporting conservative approaches for stable and potentially unstable fractures. It emphasizes the critical role of weightbearing radiographs in guiding treatment decisions and paves the way for more individualized and less invasive management approaches in these cases.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261450952 – Supplemental material for Conservative Management of Weber B/SER Lateral Malleolus Fractures With Immediate Weightbearing: Outcomes in Stable and Potentially Unstable Patterns
Supplemental material, sj-pdf-1-fao-10.1177_24730114261450952 for Conservative Management of Weber B/SER Lateral Malleolus Fractures With Immediate Weightbearing: Outcomes in Stable and Potentially Unstable Patterns by Raquel Lima Cunha, António Madureira, Pedro Atilano Carvalho, António Miranda, Filipa Oliveira and João Teixeira in Foot & Ankle Orthopaedics
Footnotes
Appendix
Correlation Between Fibular Shortening and Functional Outcomes at Different Assessment Times. a

| 6-Mo Follow-up | 12-Mo Follow-up | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Fibular Shortening, mm | P Value | Fibular Shortening (>2° Difference to the Contralateral Side) | P Value | Fibular Shortening, mm | P Value | Fibular Shortening (>2° Difference to the Contralateral Side) | P Value | ||
| VAS (0-10) | 0.215 | .01* | −0.021 | .809 | 0.031 | .714 | −0.089 | .292 | |
| AOFAS (0%-100%) | −0.194 | .021* | 0.005 | .952 | −0.063 | .455 | 0.11 | .194 | |
| FAAM ADL subscale (0%-100%) | −0.13 | .123 | 0.027 | .754 | 0.028 | .744 | 0.038 | .652 | |
| FAAM sports subscale (0%-100%) | −0.242 | .004* | −0.004 | .962 | 0.041 | .628 | 0.044 | .604 | |
| SF-36 physical functioning (0%-100%) | −0.177 | .036* | 0.002 | .978 | 0.032 | .703 | 0.041 | .626 | |
| SF-36 role limitations due to physical health (0%-100%) | −0.233 | .005* | 0.009 | .915 | 0.04 | .64 | 0.044 | .601 | |
| SF-36 Pain (0%-100%) | −0.167 | .047* | 0.025 | .766 | −0.059 | .486 | 0.103 | .225 | |
Abbreviations: ADL, activities of daily living; AOFAS, American Orthopaedic Foot & Ankle Society; FAAM, Foot and Ankle Measure; SF-36, 36-Item Short Form Health Survey; VAS, visual analog scale.
Pearson correlation test.
Statistically significant.
Ethical Considerations
Ethical approval for this study was obtained from the ethics committee of Centro Hospitalar de Entre o Douro e Vouga.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.