
Abstract
Background:
Talus fracture-dislocations with talar body extrusion (TBE) are a rare subtype of talus fracture that have been reported to occur in 1.2% of talus fractures. There is limited evidence on the outcomes of these injuries. The purpose of this study was to characterize injury patterns, operative management, and radiographic and reoperation outcomes of TBE.
Methods:
A retrospective review of talus fractures treated at a level 1 trauma center from 2016 to 2024 was performed. Radiographs and computed tomography scans were screened for TBE. Demographics, injury characteristics, operative details, reoperations, and radiographic complications were recorded. Outcomes were reported descriptively for patients with at least 6 months of follow-up, with a nested subanalysis of those with at least 12 months. Uneventful outcome was defined as no reoperation, no avascular necrosis (AVN) or nonunion, and no greater than grade 2 posttraumatic arthritis (PTA) at final follow-up.
Results:
Among 178 talus fractures, 18 TBEs were identified. Seventeen patients had at least 6 months of follow-up and 15 had at least 12 months. In the 6-month cohort, mean follow-up was 1.72 years; 15 patients (88%) underwent temporizing reduction with external fixation and/or percutaneous fixation, 16 underwent definitive ORIF, and 1 underwent primary TTC fusion. Reoperation occurred in 7 (41%), AVN in 6 (35%), nonunion in 4 (24%), and grade 3 or 4 PTA in 10 (59%); 4 (24%) had an uneventful outcome. In the 12-month subgroup, reoperation occurred in 7 (47%), AVN in 5 (33%), nonunion in 4 (27%), and grade 3 or 4 PTA in 10 (67%); 3 (20%) had an uneventful outcome.
Conclusion:
Complications and reoperations were common after open reduction and internal fixation for TBE, although a minority of patients achieved uneventful radiographic and surgical outcomes. Follow-up stratified reporting showed persistently high complication burden at 12 months, although a small subset maintained uneventful radiographic and surgical outcomes, including 3 of 15 patients with at least 12 months of follow-up.
Level of Evidence:
Level IV, case series.
Introduction
Talus fractures are a relatively rare type of lower extremity fracture that account for approximately 0.1% to 2.5% of all fractures. 1 Talus fracture-dislocations with extrusion of the talar body are a rare subtype that is associated with severe soft tissue injury, disruption of the talar blood supply, and a high risk of complications. 2 Roddy et al 3 reported that only 1.2% of 343 operatively treated talus fractures involved talar body extrusion (TBE). The distinctive blood supply and biomechanical role of the talus predispose these injuries to avascular necrosis (AVN), malunion, nonunion, and posttraumatic arthritis (PTA).1,3 In addition, these injuries are typically caused by high-energy trauma and are commonly accompanied by other injuries that may complicate treatment and recovery.
The broader literature on talus fractures supports urgent reduction, stabilization, and staged fixation in the setting of soft tissue injury. However, because of the low incidence of TBE, optimal management is poorly defined. The literature is limited to small case series that describe high complication rates; however, they lack sufficient sample sizes to support evidence-based treatment algorithms for TBE.2,4 Given this gap in the medical literature, there is a need to better characterize the management and treatment outcomes of TBE. Thorough reporting on complications rates and the failure mechanisms may help guide surgical decision making and help clarify patients’ expectations regarding long-term ankle function following TBE. The purpose of this study was to characterize injury patterns, operative management, and radiographic and reoperation outcomes after talar body extrusion.
Methods
A retrospective review was performed by identifying patients with any talus fracture treated at an academic level 1 trauma center from 2016 through 2024. All radiographs and computed tomography scans of talar fractures were screened for the presence of TBE. Patient demographics and comorbidities were recorded, including Area Deprivation Index (ADI) national rank, a neighborhood-level measure of socioeconomic disadvantage obtained from the Neighborhood Atlas, University of Wisconsin School of Medicine and Public Health, in which higher scores indicate greater deprivation.5,6 Fracture and dislocation patterns were classified with the Hawkins and Sneppen systems when appropriate. Injury characteristics included concomitant orthopaedic injuries, Gustilo-Anderson classification for open fractures, mechanism of injury, polytrauma status (injury severity score >15), and documented arterial injuries. Venous injury, neurologic injury, comminution severity, and bone loss details were not consistently documented and therefore were not analyzed as independent variables.
Operative details were collected, including use of temporizing reduction, external fixation and/or percutaneous fixation, definitive fixation strategy, and surgical approaches. For outcome reporting, patients with at least 6 months of follow-up comprised the primary descriptive cohort, and a nested subanalysis was performed for patients with at least 12 months of follow-up. Reoperation, AVN, nonunion, and PTA were recorded through final follow-up within each cohort, and PTA was graded at final follow-up with the modified Kellgren-Lawrence scale. An uneventful outcome was defined descriptively as no reoperation, no AVN/nonunion, and no more than grade 2 PTA. Patient-reported and functional outcome measures were not consistently available and therefore were not analyzed. Because of the small sample size and the non–mutually exclusive fragment displacement categories, the subgroup analyses were descriptive only and no inferential statistics were performed.
Results
A total of 178 talus fractures were screened, and 18 TBEs were identified. Seventeen patients had at least 6 months of follow-up and constituted the primary outcome cohort; 15 had at least 12 months of follow-up (Table 1). Mean follow-up in the ≥6-month cohort was 1.72 ± 1.02 years. The mechanisms of injury of the 18 TBE patients included 10 from motor vehicle collisions, 4 fall from height, 1 motorcycle collision, 1 fall from standing, and 2 related to other mechanisms. Ten injuries were closed, 12 patients sustained polytrauma, including 1 patient with an ipsilateral pilon fracture and most injuries involved the talar neck (15/17, 88%) (Table 2). Among the neck fractures, 8 were Hawkins III and 7 were Hawkins IV. The 2 talar body fractures were Sneppen types I and V. When the main extruded fragment was evaluated, posterior displacement was most common (8/17, 47%) (Figure 1), followed by medial displacement (4/17, 24%).
Talar Body Extrusion Cohort Characteristics (Patients With ≥6 Months’ Follow-up).

Abbreviation: ISS, injury severity score.
Area Deprivation Index (ADI) is a neighborhood-level measure of socioeconomic disadvantage, with higher scores indicating greater deprivation as compared to other neighborhoods within the United States of America. The mean ADI of this cohort was 51.0 ± 23.8, indicating that the cohort was centered near the national median with broad variability in neighborhood-level socioeconomic disadvantage.
Talar Body Extrusion Injury Characteristics (Patients With ≥6 Months’ Follow-up).

Abbreviation: ORIF, open reduction and internal fixation.
The bone fragment displacement direction is classifying the largest extruded talar body fragment.
Closed reduction was attempted in the emergency department in 7 patients (41%) and was unsuccessful in all cases. All patients underwent urgent operative reduction. Fifteen patients (88%) underwent temporizing stabilization with external fixation and/or percutaneous fixation before definitive treatment. Sixteen patients underwent definitive open reduction and internal fixation, and 1 patient underwent primary hindfoot fusion with a tibiotalocalcaneal nail because the injury was considered nonreconstructable. An anterolateral approach was commonly used, often with an additional incision that was dictated by fracture morphology and fragment displacement direction. One case required an anteromedial exposure with proximal-lateral extension, which was performed to repair the associated posterior tibial arterial injury.
Complications for the ≥6-month cohort and the nested ≥12-month subgroup are summarized in Table 3. In the ≥6-month cohort, 7 patients (41%) underwent reoperation. Six of the 7 reoperations occurred in polytraumatized patients injured in motor vehicle collisions, and 3 reoperated patients had documented ipsilateral lower-extremity injuries. Reoperation courses included hindfoot arthrodesis, hardware removal–based reconstructive procedures, infection-related debridement, and 1 below-knee amputation (Figure 2). The patient who ultimately underwent below-knee amputation had initially undergone primary hindfoot fusion because of anterior tibial and posterior tibial artery injury and a fracture pattern deemed nonreconstructable. Four patients developed nonunion, 3 underwent salvage hindfoot arthrodesis, and 1 was not a surgical candidate because of severe psychiatric comorbidity.
Talar Body Extrusion Clinical and Radiographic Outcomes.
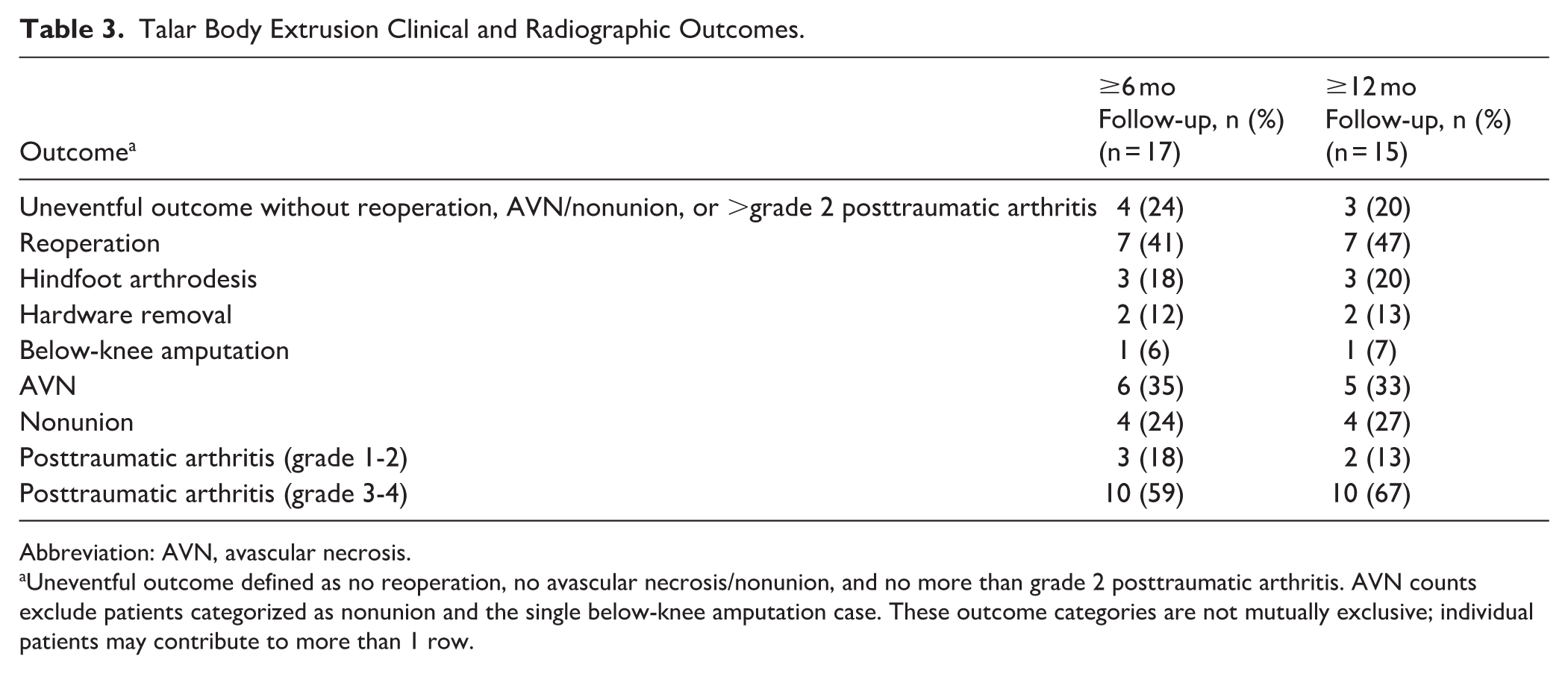
Abbreviation: AVN, avascular necrosis.
Uneventful outcome defined as no reoperation, no avascular necrosis/nonunion, and no more than grade 2 posttraumatic arthritis. AVN counts exclude patients categorized as nonunion and the single below-knee amputation case. These outcome categories are not mutually exclusive; individual patients may contribute to more than 1 row.

Lateral radiograph of the right ankle of a patient with a Hawkins type IV talar neck fracture- dislocation with talar body extrusion.
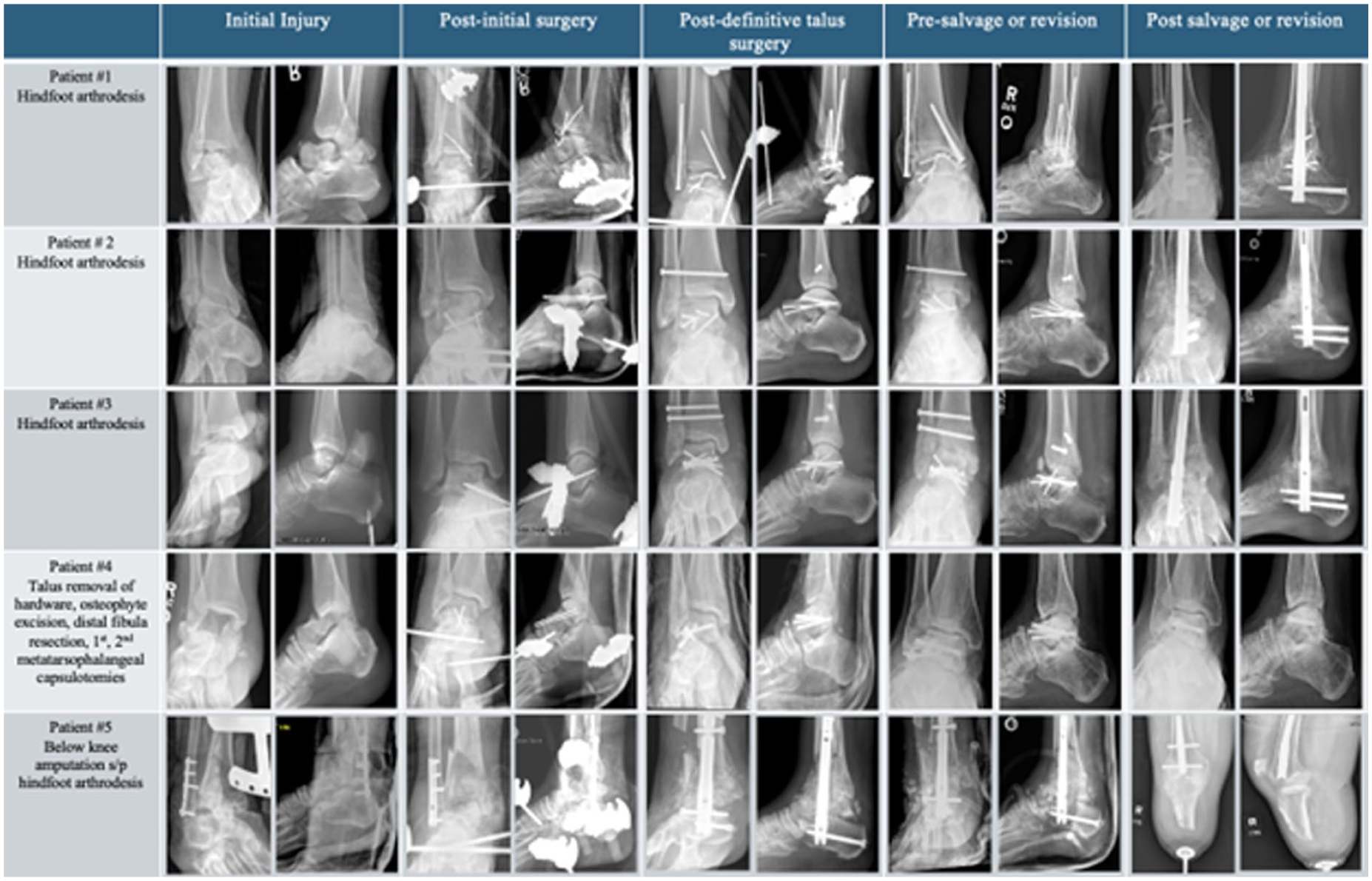
Radiographic timeline from the initial injury to the final outcome for the 5 patients who underwent a salvage procedure.
In the ≥6-month cohort, AVN was noted in 6 patients (35%), nonunion in 4 (24%), grade 1 or 2 PTA in 3 (18%), and grade 3 or 4 PTA in 10 (59%) (Table 3). Ten patients (59%) did not undergo reoperation; nevertheless, 5 of these 10 developed grade 3 or 4 PTA. Four of 17 patients (24%) achieved an uneventful outcome without reoperation, AVN/nonunion, or greater than grade 2 PTA. A descriptive summary of fragment displacement direction and reoperation within the ≥6-month cohort is provided in Table 4. Because displacement groups were not mutually exclusive, these data were summarized descriptively only. Reoperation occurred in 2 of 3 patients (67%) with any lateral displacement, 5 of 12 (42%) with any posterior displacement, and 5 of 14 (36%) with any medial displacement.
Descriptive Analysis of Displacement Direction and Reoperation (Patients With ≥6 Months’ Follow-up). a
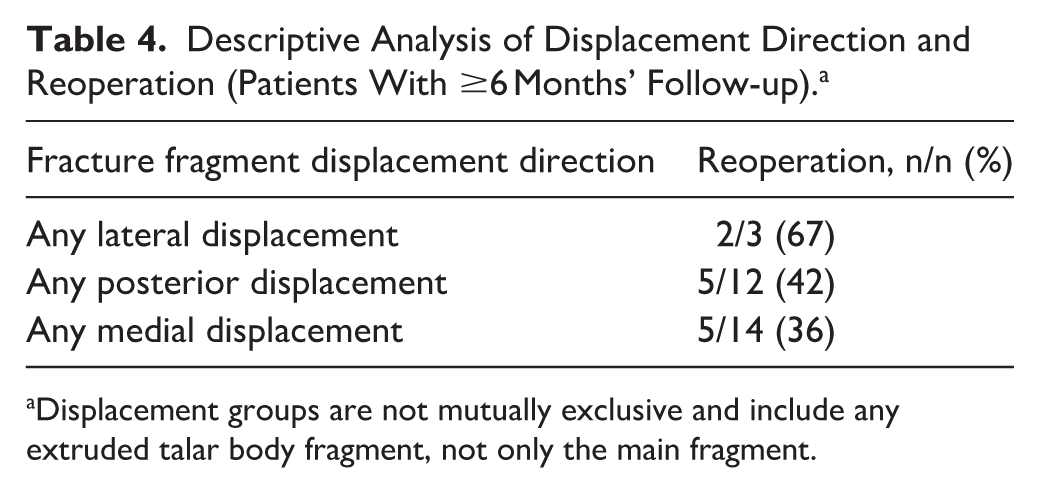
Displacement groups are not mutually exclusive and include any extruded talar body fragment, not only the main fragment.
In the nested subgroup of 15 patients with at least 12 months of follow-up, complication rates remained high: 7 patients (47%) underwent reoperation, 5 (33%) developed AVN, 4 (27%) developed nonunion, and 10 (67%) developed grade 3 or 4 PTA. Three of 15 patients (20%) met the definition of an uneventful outcome. Thus, although favorable longer-term radiographic courses were observed in a small subset, most patients with at least 12 months of follow-up demonstrated substantial radiographic sequelae and/or required additional surgery.
Discussion
The principal finding of this study is that TBE was associated with a high complication burden after operative treatment, even when outcomes were stratified by follow-up duration. In the primary cohort with at least 6 months of follow-up, reoperation was required in 41%, AVN occurred in 35%, nonunion in 24%, and grade 3 or 4 PTA in 59%. In the nested subgroup with at least 12 months of follow-up, these rates remained similarly high, with grade 3 or 4 PTA observed in 67%. Nonetheless, favorable limb-salvage outcomes remained possible in a minority of cases. Using the study’s follow-up-stratified definition of uneventful outcome, 4 of 17 patients (24%) in the ≥6-month cohort and 3 of 15 patients (20%) in the ≥12-month subgroup had no reoperation, no AVN/nonunion, and no more than grade 2 PTA at final follow-up.
These findings are consistent with prior small series describing the severity of this injury. Gupta et al 2 reported major complications in 2 of 5 patients with extruded fracture-dislocations of the talus. Smith et al 4 reported talar collapse in 6 of 8 patients with at least 1 year of radiographic follow-up after talar extrusion injuries treated with reimplantation. Marsh et al 7 similarly described high infection and salvage rates after major open talar injuries. Compared with the broader displaced talar neck and body fracture literature, the present TBE cohort appears to represent the severe end of the spectrum. Leonetti et al 8 reported mean rates of osteonecrosis of 30.2%, subtalar osteoarthritis of 53.2%, and tibiotalar osteoarthritis of 33.7% after surgical treatment of displaced talar fractures, whereas AVN occurred in 35% of the present ≥6-month cohort and grade 3 or 4 PTA was already present in 59% at ≥6 months and 67% at ≥12 months. In addition, Roddy et al 3 reported a 15% rate of salvage surgery at 16 years after operative treatment of talus fractures overall, whereas reoperation occurred in 41% of the present ≥6-month cohort and 47% of the ≥12-month subgroup, emphasizing the substantial early burden associated with TBE. These comparisons suggest that TBE carries a particularly high early burden of radiographic sequelae and secondary procedures relative to talus fractures more broadly.
In the present study, the high rates of reoperation, AVN, nonunion, and advanced PTA likely reflect the severity of soft tissue and vascular injury inherent to TBE. Most injuries in this series occurred after high-energy trauma, and many patients sustained polytrauma or associated ipsilateral lower-extremity injuries, underscoring the complexity of limb salvage in this setting. Even among patients who avoided reoperation, advanced PTA remained common, suggesting that limb preservation and fracture healing were not consistently associated with an uncomplicated longer-term course. Descriptive evaluation of displacement direction was also included because it may help characterize injury morphology in this rare pattern. Although the overlapping fragment-displacement groups and small counts precluded formal comparison, the proportion undergoing reoperation was highest among patients with any lateral displacement. At the same time, the subset of patients who met the study definition of uneventful outcome supports that acceptable radiographic limb-salvage results can still be achieved in a minority of cases.
This study has several important limitations. It is retrospective and includes a small heterogeneous cohort from a single center. Outcome reporting was limited by the rarity of the injury, variable follow-up, and the need to use descriptive nested follow-up strata rather than formal comparative analysis. Functional outcomes and patient-reported outcome measures were not consistently available, so the true clinical impact of the radiographic findings cannot be fully assessed. In addition, venous injury, neurologic injury, comminution severity, and bone loss were not consistently documented, which limits causal interpretation of later arthritis and salvage procedures. Despite these limitations, this series adds to the sparse literature on TBE and, to our knowledge, reports one of the largest cohorts of this rare injury pattern.
Conclusion
Talus fracture-dislocations with extrusion of the talar body had high complication and reoperation rates after operative treatment. Nonetheless, uneventful radiographic and surgical outcomes were observed in a minority of patients, including 3 of 15 patients with at least 12 months of follow-up. Patients should be counseled on the possible sequelae of this injury, but surgical treatment including urgent preliminary reduction and stable internal fixation was associated with a satisfactory radiographic course in select patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261452668 – Supplemental material for Talus Fracture-Dislocations With Talar Body Extrusion Have High Complication Rates, With Uneventful Outcomes in a Minority of Patients After Open Reduction Internal Fixation
Supplemental material, sj-pdf-1-fao-10.1177_24730114261452668 for Talus Fracture-Dislocations With Talar Body Extrusion Have High Complication Rates, With Uneventful Outcomes in a Minority of Patients After Open Reduction Internal Fixation by David Dallas-Orr, Westin Mace, Jacob C. Wilson, Abby Viglione, Shannon Tse, Ellen P. Fitzpatrick, Gillian L.S. Soles, Mark A. Lee, Augustine M. Saiz and Sean T. Campbell in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from University of California Davis Institutional Review Board (ID: 2139637).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Dallas-Orr, MD, MBA, MTM, reports Johnson & Johnson: other professional activities. Ellen P. Fitzpatrick, MD, reports DePuy, A Johnson & Johnson Company: paid consultant. Gillian L.S. Soles, MD, reports Johnson & Johnson: other professional activities. Mark A. Lee, MD, reports Globus Medical, Inc.: other professional activities; AO North America: fiduciary officer; OsteoCentric Technologies, Inc.: stock option; AO Foundation: fiduciary officer; IlluminOss Medical, Inc.: other professional activities; Johnson & Johnson: other professional activities. Augustine M. Saiz, MD, reports AO North America: IP royalties; Stryker: other professional activities; Arthrex: other professional activities; Johnson & Johnson/DePuy Orthopedic: other professional activities; Orthopaedic Research and Education Foundation: IP royalties. Sean T. Campbell, MD, reports NSite medical: stock; OTA: other professional activities; AO North America: IP royalties; AAOS: other professional activities; Smith and Nephew: other professional activities; DePuy Synthes Products LLC: other professional activities; Takeda Pharmaceutical Company: IP royalties. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.